Write a review
Reviews: 0
Manufacturers: Moskhimfarmpreparaty im. N. A. Semashko
Active ingredients
- Azathioprine
Disease class
- Idiopathic thrombocytopenic purpura
- Myasthenia gravis and other neuromuscular junction disorders
- Ulcerative colitis
- Pemphigus [pemphigus]
- Chronic hepatitis, unspecified
- Psoriasis
- Rheumatoid arthritis, unspecified
- Polyarteritis nodosa and related conditions
- Systemic lupus erythematosus
- Dermatopolymyositis
- Nephritic syndrome, unspecified
- Death and rejection of transplanted organ and tissue, unspecified
Clinical and pharmacological group
- Not indicated. See instructions
Pharmacological action
- Immunosuppressive
Pharmacological group
- Immunosuppressants
Use of the drug Azathioprine
The dose is selected individually. To prevent transplant rejection, a loading dose of up to 5 mg/kg body weight is prescribed orally in 2–3 doses for 1–2 months; then switch to maintenance treatment at a dose of 1–4 mg/kg per day orally. For diffuse connective tissue diseases, it is prescribed orally at an average daily dose of 2–2.5 mg/kg; for chronic active hepatitis, the daily oral dose is 1–1.5 mg/kg. For rheumatoid arthritis, lower doses of azathioprine may be effective. The treatment is long-term. When azathioprine is discontinued, the dose should be reduced gradually.
Well-known traditional approaches to the treatment of inflammatory bowel diseases (IBD) - ulcerative colitis (UC) and Crohn's disease (CD) - primarily include first-line drugs: aminosalicylates and corticosteroid hormones, the use of which is aimed at stopping the attack of the disease, inducing remission and maintaining the achieved remission for as long as possible. However, among patients with IBD there are often patients with the so-called. refractory forms of the disease. Refractoriness to treatment includes two concepts: steroid resistance and steroid dependence. Steroid resistance is defined as a lack of response to hormonal therapy within a period of 5 days to 3-4 weeks, depending on the severity of the disease. Steroid dependence implies a response to corticosteroids, but discontinuation or reduction of the drug dose causes reactivation of the inflammatory process in the colon, which forces a return to the original dose of hormones. The critical dose of prednisolone at which recurrent deterioration occurs ranges from 15–30 mg/day. In such patients, the question of the possibility of achieving remission and its maintenance becomes very problematic. Steroid dependence can occur after the first attack of the disease, and with repeated courses of hormonal treatment it becomes more common.
In large cohort studies, Moum V. et al. showed that the cumulative risk of relapse within the first year after diagnosis of UC is 50% [1]. Similar results were obtained at the Mayo Clinic. Thus, Faubion WA et al., having analyzed the results of the first course of steroid therapy in patients with UC, found that only 49% achieved a long-term positive effect of treatment; at the same time, 22% of cases developed steroid dependence, and 29% required colectomy due to resistance to treatment [2]. Mukholm P. noted that 10–15% of patients with IBD develop a continuous course of the disease during treatment with corticosteroids [3]. According to E.A. Belousova, the frequency of refractory forms of IBD in the Russian population is 26% [4].
The lack of effect of conservative therapy is an indication for surgery (colectomy or subtotal resection of the colon), in most cases with the formation of an ileostomy. Since UC mainly affects young able-bodied people, the consequences of such an operation inevitably lead to disability, labor and social maladaptation of patients.
An alternative method of conservative treatment may be an attempt to use reserve drugs - immunosuppressants. Azathioprine (AZA), 6-mercaptopurine (6-MP), methotrexate and cyclosporine A are currently used in the treatment of IBD. AZA and
6-MPs were historically the first immunosuppressants used in the treatment of IBD.
AZA is a purine antimetabolite, due to which it has cytostatic activity. In the body it forms the active metabolite 6-MP. Acts on rapidly proliferating cells, including immunocompetent ones: lymphocytes and macrophages. Since these cells make up the bulk of the inflammatory infiltrate of the colon mucosa in IBD, this appears to be responsible for the immunosuppressive effect. AZA inhibits the synthesis of most inflammatory mediators, suppresses the activity of natural killer cells and, presumably, the production of prostaglandins [5, 6].
The optimal dose of AZA is 2 mg/kg/day, but if necessary it can be increased to 2.5 mg/kg [7, 8]. The effect of the drug develops slowly, improvement can be noticeable no earlier than after 3–4 weeks; to obtain the maximum effect, a period of 4–6 months is required, which is why AZA cannot be used in acute severe situations: it is advisable for the treatment of chronic, sluggish steroid-resistant and steroid-dependent active forms of IBD and to maintain remission [9]. AZA is used as monotherapy or in combination with corticosteroids, which makes it possible to reduce the dose of the latter [7–9].
Clinical researches
AZA has been used in the treatment of refractory forms of IBD since the 1960s. The largest number of works is devoted to the use of AZA in CD. Thus, according to the results of the National Cooperative Crohn's Disease Study (NCCDS), AZA is effective in patients with severe hormone-dependent and hormone-resistant forms [10]. The first part of this study assessed the effectiveness of AZA in patients with active disease (136 patients participated, 36% of whom achieved remission compared with 26% receiving placebo). The second part of the project assessed the effectiveness of AZA in maintaining remission. According to the study results, 40% of patients receiving AZA and 40% of those receiving placebo remained in remission of the disease. In the first part of the protocol, patients received AZA at a dose of 2.5 mg/kg, in the second – 1 mg/kg. The insufficient effect of AZA is explained by the peculiarities of the study design, in particular the fact that before the start of the study, all medications were discontinued in patients, which could affect the effectiveness of AZA, since its effect develops slowly. In the second part, the dose of the drug was clearly underestimated.
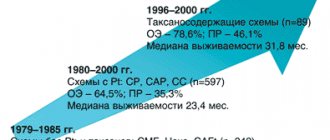
In the 1980s Ewe K. et al. continued to study the use of AZA in patients with CD [11]. Their study included 42 patients who received AZA at a dose of 2.5 mg/kg in combination with prednisolone at an initial dose of 60 mg/day, which was gradually tapered to complete discontinuation over 7 weeks. The duration of the study was 16 weeks. According to its results, the CD activity index (CDAI) while taking AZA decreased by 218 points compared to a decrease of 130 points in patients receiving placebo. The authors found that 76% of patients achieved remission, while in the control group this figure was 38%. In addition, it was noted that the appointment of AZA allowed prednisolone to be discontinued more quickly.
Candy S. et al. in 1995 published the results of two studies on the use of AZA in CD [12]. A total of 63 patients took part, divided into two groups. One of them received AZA in combination with prednisolone, the other received placebo and prednisolone. After 12 weeks, remission was not achieved either in the group of patients receiving AZA or in the placebo group. However, after 15 months of treatment, remission was detected in 15 (42%) people from the group receiving AZA, while in the control group, remission was established in only 2 (7%) patients.
Pearson DC et al. published a paper in 1995 that conducted a meta-analysis of 9 randomized trials on the use of AZA in patients with CD. Based on the results of these studies, the authors conclude that it is advisable to prescribe AZA in patients with hormone-dependent and hormone-resistant forms of CD to reduce the time required to achieve remission and its maintenance [13].
Much less work has been devoted to the use of AZA in patients with UC. So, Hawthorne A.V. et al., who studied this problem, provide the following data [14]. Their study included 67 patients with UC. The first group consisted of patients with remission for 2 months before randomization, the second group consisted of patients who had been receiving AZA for 6 months; they also had remission. Patients in the first group were prescribed a placebo, while the second group continued to take AZA. The study lasted one year. By the end of this period, in the first group, remission was achieved in 35% of patients, in the second - significantly more often - in 59%. Three patients receiving AZA developed side effects that required discontinuation of the drug. The authors note the advisability of long-term administration of AZA in patients with severe refractory forms of UC, but believe that long-term immunosuppression can lead to undesirable effects, including the development of neoplasia.
Connell WR et al., evaluating the use of AZA in patients with UC, also speak out about the risk of developing colon cancer in them [15].
In the domestic literature, only one study demonstrates the effectiveness of AZA in hormonal-dependent forms of IBD. So, Rumyantsev V.G. et al. AZA was prescribed at an initial dose of 50 mg/day, followed by an increase to 2 mg/kg/day, which made it possible to reduce the dose of steroids or completely eliminate them in 60–70% of patients with CD [16].
Despite the general, fairly consistent point of view on the advisability of using AZA in patients with refractory forms of IBD, its significant disadvantages should be taken into account. The drug has a wide range of adverse reactions: dyspeptic symptoms (nausea, vomiting, diarrhea); flu-like syndrome with fever and myalgia; bone marrow suppression with leukopenia, neutropenia (less often with agranulocytosis), thrombocytopenia. Taking AZA may also be accompanied by hepatotoxic reactions in the form of cytolysis and cholestasis, pancreatitis, the development of polyneuritis, alopecia and activation of secondary infection. The drug is believed to increase the risk of malignancy, although many dispute this position. Side effects develop with a frequency of 6–20%. At the beginning of treatment, it is necessary to monitor the level of leukocytes and liver enzymes every 10–14 days, then these studies can be carried out once a month or less often. The slow-onset effect combined with a large number of side reactions is a significant drawback of the drug and significantly limits the possibilities of its use. However, in the absence of side effects, AZA can be used to maintain remission for a long time - up to 2 years at 2 mg/kg/day or at a minimum dose of 50 mg/day (less than 1 mg/kg) without increasing the risk of malignancy [17]. There is a point of view according to which maintenance therapy with AZA should be carried out much longer – up to 5–6 years, without adverse reactions and the threat of malignancy, but this position is very controversial [10, 18].
Currently, AZA is included in many national guidelines and recommendations for the treatment of steroid-resistant and steroid-dependent forms of UC and CD [19, 20].
Own experience of using AZA
Despite significant global experience in the use of AZA for IBD, in Russia the drug is rarely used, mainly in specialized medical clinics. The reasons for this, apparently, should be considered, on the one hand, insufficient knowledge by doctors of the possibilities of treating IBD, and on the other hand, the fear of developing serious side effects. Therefore, in this publication we want to share our own experience of long-term use of AZA in patients with refractory UC.
The purpose of the work was to evaluate the effectiveness of AZA for inducing and maintaining remission in steroid-dependent forms of UC.
Materials and methods
We observed 14 patients with steroid-dependent UC (8 men and 6 women) aged from 32 to 67 years. The duration of the disease was 3–25 years.
The characteristics of patients according to the prevalence of the inflammatory process in the colon and the severity of the course are given in Table. 1.
All patients were diagnosed with UC at one time, confirmed by endoscopic and histological methods. The first attacks of the disease in all patients were severe, and therefore the main method of treatment was the use of corticosteroid hormones. We used oral prednisolone at a rate of 1–1.5 mg/kg or intravenous infusion of methylprednisolone (500 mg per day) for 7–10 days, followed by transfer to oral administration. In addition, antibiotics were prescribed, as well as symptomatic therapy to correct water-protein-electrolyte disturbances and anemia. This course of treatment made it possible to achieve complete clinical and endoscopic remission or significant improvement and, accordingly, gradual withdrawal of steroids. Steroid dependence developed in patients at different times and did not depend on the duration of the disease, gender and age, or the severity of UC. In four patients, steroid dependence developed after the first attack of UC and was manifested by activation of inflammation and relapse of disease symptoms when the dose of prednisolone was reduced to 20–30 mg per day. In the remaining 10 patients, the first exacerbations of the disease were successfully stopped by the above course of treatment. Maintenance therapy in these cases was carried out with 5-ASA drugs. However, after 3–4 attacks of UC and repeated courses of treatment with steroids, these patients also developed steroid dependence: activation of the inflammatory process in the colon occurred when the dose of prednisolone was reduced to 35–40 mg per day; in four cases of moderate UC, only a slight improvement was achieved.
In order to enhance drug therapy against the background of a stable dose of prednisolone or methylprednisolone (30–40 mg/day), AZA was added to therapy at a dose of 2–2.5 mg/kg/day (daily dose – 100–150 mg) in all patients. Clinical symptoms of the disease before the start of AZA treatment corresponded to a moderate course in 12 patients and a severe course in 2 patients.
results
The first signs of improvement in most patients were noted by the end of the 4–5th week of treatment. There was a decrease in the frequency and volume of stool (an average of 2–4 bowel movements), a decrease in blood in the stool, an increase in hemoglobin levels and a normalization of body temperature. Stabilization of the patients' condition allowed us to begin reducing the dose of corticosteroids according to an individual regimen with a stable dose of AZA. Subsequently, AZA was used as monotherapy.
By the end of 4–6 months from the start of treatment, complete clinical and endoscopic remission was achieved in 11 (78.6%) patients. In three (21.4%) patients, AZA was canceled after 6 months due to ineffectiveness. The duration of observation of patients ranged from one year to 5 years (Table 2).
In all 11 patients, while taking AZA, a change in the refractory course of UC was noted. During the entire treatment period, the patients felt well, taking AZA was easily tolerated, and no dyspeptic symptoms were observed. The disease seemed to have acquired a “mild” course with rare mild exacerbations (in 5 out of 11 patients) or without them. During exacerbations, a minimal or moderate degree of process activity was determined endoscopically. The condition of the patients at the time of exacerbation did not require hospital treatment. Therapy during an exacerbation included AZA at the same dose in combination with mesalazine at a dose of 3–4 g/day for 3–4 weeks. No steroid use was required. After achieving clinical and endoscopic remission, patients continued to take AZA, and aminosalicylates were discontinued. Complete labor and social rehabilitation of patients was noted.
During treatment with AZA, regular monitoring of leukocyte and liver enzyme levels was carried out. Blood tests and biochemical tests were examined weekly for the first month, biweekly for the second month, and monthly thereafter. Side effects in the form of leukopenia were noted in 4 (28.6%) patients in the 2-4th month of treatment (blood leukocyte counts decreased to 2.8-3.2 x 109/l), and therefore the dose of the drug was reduced up to 50 mg/day until blood counts normalize, after which it is again increased to the initial dose. Subsequently, no signs of leukopenia were detected in these patients. We did not observe any other side effects.
All patients were under constant observation with regular endoscopic examination (colonoscopy once a year). At least once a year and/or if necessary (in case of complaints not related to the underlying disease), other examinations were performed: chest x-ray, ultrasound of the abdominal organs, endoscopy, etc. Thus, the need for lung x-ray arose in case of prolonged ARVI. The purpose of such careful monitoring was not only to monitor the course of the underlying disease, but also to timely identify complications of long-term immunosuppressive therapy for AZA: inflammatory and neoplastic processes. During the observation period, such complications were not noted in any of the cases.
Conclusion
AZA is an effective immunosuppressive agent for inducing and maintaining remission in refractory forms of UC. Clinical and endoscopic remission after 4–6 months was achieved in 78.6% of patients. Taking AZA made it possible to completely stop using corticosteroids. Against the background of AZA, qualitative changes in the course of UC were noted: a decrease in the frequency and severity of exacerbations, a significant reduction in the duration of exacerbation. AZA was well tolerated by patients. The incidence of side effects was 28.6%. Of the entire range of possible adverse reactions, only reversible leukopenia was noted, which did not cause drug withdrawal. Prescribing AZA requires careful monitoring of peripheral blood parameters and liver function tests, especially in the first months of treatment. In addition, strict clinical and instrumental monitoring is necessary for the timely detection of malignant neoplasms. It is recommended to have a colonoscopy at least once a year.
Side effects of the drug Azathioprine
Possible secondary infections, leukopenia, thrombocytopenia, anemia, development of megaloblastic erythropoiesis and macrocytosis, nausea, vomiting, anorexia, skin rash, arthralgia, myalgia, drug fever, cholestatic hepatitis. Pancreatitis, peptic ulcers, gastrointestinal bleeding, intestinal necrosis and perforation have been reported in transplant recipients. There are isolated reports of side effects such as acute renal failure, hemolytic anemia, acute pulmonary diseases, and meningeal reactions.
Similar drugs:
- Diprospan Solution for injection
- Prednisolone Oral tablets
- Metoject Solution for injection
- Imuran Oral tablets
- Prednisolone Solution for injection
- Diprospan Suspension for injection
- Restasis Eye Drops
- Leflunomide Oral tablets
- Cyclosporin Capsule
- Decadron (Decadron) Solution for injection
** The Drug Directory is intended for informational purposes only. For more complete information, please refer to the manufacturer's instructions. Do not self-medicate; Before starting to use the drug Azathioprine, you should consult a doctor. EUROLAB is not responsible for the consequences caused by the use of information posted on the portal. Any information on the site does not replace medical advice and cannot serve as a guarantee of the positive effect of the drug.
Are you interested in the drug Azathioprine? Do you want to know more detailed information or do you need a doctor's examination? Or do you need an inspection? You can make an appointment with a doctor - the Euro lab is always at your service! The best doctors will examine you, advise you, provide the necessary assistance and make a diagnosis. You can also call a doctor at home . Euro lab clinic is open for you around the clock.
** Attention! The information presented in this medication guide is intended for medical professionals and should not be used as a basis for self-medication. The description of the drug Azathioprine is provided for informational purposes and is not intended for prescribing treatment without the participation of a doctor. Patients need to consult a specialist!
If you are interested in any other drugs and medications, their descriptions and instructions for use, information about the composition and form of release, indications for use and side effects, methods of use, prices and reviews of drugs, or you have any other questions and suggestions - write to us, we will definitely try to help you.