How to use hyaluronic acid at home
Procedures and cosmetics can be quite expensive, so many women resort to using homemade cosmetics. To do this, you will need to purchase sodium hyaluronate powder at the pharmacy and prepare a solution for external use.
To do this, you need to dilute 2 g of the active substance in 30 ml of warm drinking water. leave to infuse for 40-60 minutes. The finished solution can be used as a cream. It should be applied to previously cleansed skin. Apply any other anti-aging product of similar effect on top.
Introduction
Osteoarthritis (OA) is a joint disease, the main pathogenesis of which is cellular stress and degradation of the extracellular matrix. They arise as a result of macro- or microdamage that activates pathological adaptive recovery reactions, including pro-inflammatory pathways of the immune system [1]. According to estimates by the Federal State Statistics Service of the Russian Federation for 2022, diseases of the musculoskeletal system occupy a significant place in the structure of disability along with cardiovascular diseases and cancer. OA plays an important role among these diseases [2]. Currently, the prevalence of the disease is steadily increasing. OA accounts for 36 million outpatient visits and 750 thousand hospitalizations per year. In developed countries, the economic costs of OA amount to 1.5–2% of GDP per year [3]. Clinical manifestations and progression of OA do not pose a threat to the life of patients, but pain, which is a constant symptom of the disease, and limitation of joint function lead to a marked deterioration in the quality of life, the development of temporary and permanent disability. Against this background, there is a progression of concomitant diseases, which leads to an increased risk of overall mortality. In 2016, the Osteoarthritis Research Society International (OARSI), together with the US Food and Drug Administration (FDA), recognized OA as a serious disease [4]. In Russia, the prevalence of OA is also high and reaches 13%. According to the Russian Ministry of Health, over 5 years (2011–2016) there was an increase in the incidence of OA from 32.3 to 35.7 per 1000 population. In recent years, in the process of studying OA, ideas about its pathogenesis have changed significantly. Currently, OA is considered not as a degenerative disease, but as an inflammatory disease. The diversity and varying degrees of severity of individual pathogenesis links have led to the identification of several OA phenotypes. Changing understanding of the pathogenesis of the disease is also changing approaches to therapy, with an emphasis on personalized treatment.
Recommendations for the management of patients with OA
Currently, OA therapy is regulated by documents developed by professional communities. ESCEO (European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases) has developed guidelines that guide consistent treatment choices for patients with knee OA . They were presented in 2014 [5], and supplemented in 2016 [6]. New recommendations were published in 2022, which take into account the latest evidence on the safety and effectiveness of drugs currently used to treat OA [7]. The developed scheme recommends step-by-step administration of therapy (Fig. 1).
If OA symptoms persist, the use of hyaluronic acid (HA) is indicated, both as monotherapy and in combination with drugs from other groups. Let's take a closer look at the effects of HA.
Contraindications
- oncology (consultation with an oncologist is required);
- endocrine disorders (consultation with an endocrinologist is needed);
- diabetes;
- pregnancy, breastfeeding;
- bleeding disorders;
- taking blood thinning medications;
- exacerbation of chronic diseases;
- increased body temperature;
- herpes;
- cold;
- mental disorders;
- violation of the integrity of the skin;
- skin diseases;
- vascular pathologies;
- heart diseases.
Anti-inflammatory and regenerating mechanisms of action of GCs
The physiological role of HA has been well described by many researchers [8–10]. In general, HA can participate in various cellular processes (cell differentiation, proliferation, etc.) and perform physiological functions (lubrication, hydration balance) [9, 10]. HA has unique rheological properties and is an integral part of articular cartilage; the important role of HA in the functioning of joints, not only healthy ones, but also joints with OA [11], as well as other body tissues, has been well studied [12]. Studying the pharmacological action of GC, E. Maheu [13], GM Campo [14] and J. Jerosch. [15] in their studies proved that GC reduces the activity of proinflammatory mediators that produce neuropeptides released by activated synovial cells. The authors also described the interaction of HA with pain receptors and its analgesic properties.
LW Moreland [10] noted in his study that HA can reduce the mechanosensitivity of pain receptors. GC may also reduce OA pain by reducing the synthesis of prostaglandin E2 and bradykinin.
In OA, synovitis plays an important role in inducing pain, swelling and stiffness [16], and the severity of synovitis correlates with a high risk of progression to knee OA [17]. A study was conducted that showed that GC inhibits the activity of matrix metalloproteinases and aggrecanases, which are at least partially involved in the degradation of OA cartilage as a result of their induction by proinflammatory cytokines such as interleukin-1 (IL-1) [18]. . Therefore, it is hypothesized that GC modifies structural joint damage and the rate of progression of OA in addition to its symptom-modifying effect [19].
Regarding the reparative function of HA, JL Cook et al. [20] suggested that intra-articular administration of GC has a direct effect on chondrocytes or synoviocytes and the production of Transforming growth factor beta (TGF-β), basic fibroblast growth factors (FGF) and insulin-like growth factor (Insulin-β). like growth factor, IGF). Histological data confirmed that HA prevents cartilage degradation and may promote cartilage regeneration. Other authors [14] have also provided evidence that GC treatment mitigates synovial hypertrophy and increases the number of synovial fibroblast-like cells while reducing the number of macrophages, lymphocytes, mast cells and adipocytes. HA, according to them, provides cartilage protection by suppressing the production of proinflammatory cytokines, free radicals and proteolytic enzymes in the synovial fluid.
A large number of clinical studies have found that GC reduces the progression of OA. GC is a slow-acting drug that can be used prophylactically or therapeutically as an anti-inflammatory symptom-modifying drug [20, 21].
Several clinical studies have found that intra-articular HA injections slow joint space narrowing on x-ray and stop the progression of cartilage degeneration on subsequent arthroscopy [22, 23].
Changing lip volume
With the help of injections of drugs containing hyaluronic acid, you can achieve significant changes in appearance. The most popular procedure in aesthetic medicine is changing the volume and shape of the lips.
This service is used not only by young women who want to make their lips more sexy, but by people of all ages who are faced with the following problems:
- purse string wrinkles;
- drooping corners of the mouth;
- disproportion;
- curvature of the lip line.
Using hyaluronic acid, you can change the shape of your cheeks, cheekbones or chin, which makes your facial features more harmonious.
Hyaluronic acid is superior to other drugs for increasing lip volume and has the following advantages:
- naturalness _ After the procedure, the lips become voluminous, but without excessive plumpness, and their contour is clearer;
- facial expressions are not disturbed;
- there are no complications , because hyaluronic acid is as friendly as possible to the body;
- rejuvenation of the skin of the lips occurs due to the stimulating effect on metabolic processes.
Varieties
Types of hyaluronic acid are divided according to several criteria, including molecular weight, filler structure, mechanism of action and method of production. But this classification is more suitable for products used in cosmetology. If we talk about oral medications, they can be classified as accumulative agents, some of which not only replenish the deficiency, but are capable of activating the process of producing one’s own collagen. Depending on how the active substance is extracted, the component of hyaluronic acid tablets can be classified as an element of animal origin or a biosynthesis product. In the first case, the proteins and peptides contained in the drug can lead to an allergic reaction.
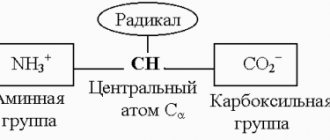
Glycosaminoglycans[edit | edit code]
Formula of chondroitin sulfate, one of the glycosaminoglycans.
Glycosaminoglycans (GAGs) or mucopolysaccharides are unbranched polysaccharide chains built from repeating disaccharide units in which one of the two sugar residues is an amino sugar (N-acetylglucosamine or N-acetylgalactosamine), which in most cases is sulfated. The presence of sulfate or carboxyl groups (or both) on many sugar residues gives glycosaminoglycans a large negative charge. The second sugar is usually an uronic acid (glucuronic or iduronic). There are four main groups of GAGs:
1) Hyaluronate.
2) Chondroitin sulfate and dermatan sulfate.
3) Heparan sulfate and heparin.
4) Keratan sulfate.
GAGs carry a large negative charge, are highly hydrophilic, have a highly elongated conformation, and form gels even at low concentrations. The recruitment of osmotically active cations by GAG causes swelling pressure (matrix turgor), which gives the matrix the ability to resist compressive forces. Because GAGs form porous hydrated gels, they fill most of the available space and provide tissue support while allowing water-soluble molecules to diffuse and cells to migrate.
Preparations with different molecular weights of HA
The effectiveness of HA preparations with different molecular weights is discussed in the literature. Even 20 years ago, KD Brandt et al. analyzed the effectiveness of 3 weekly injections of medium and low molecular weight HA in patients with OA. After 6 months HA with a medium molecular weight provided a more significant reduction in pain on the WOMAC scale (Western Ontario and McMaster Universities Osteoarthritis Index) than low molecular weight HA (by 22.9 ± 1.4 mm and 18.4 ± 1 mm). .5 mm, respectively, p=0.021). Also, in the group that used HA with an average molecular weight, there were significantly more patients who responded to therapy according to the OARSI/OMERACT criteria (Outcome Measures in Rheumatoid Arthritis Clinical Trials, assessment of the outcomes of rheumatoid arthritis in clinical trials), compared with the group receiving low molecular weight GC (73% and 58%, respectively, p=0.001) [24]. Subsequently, the data from this study were repeatedly confirmed [25, 26].
In a randomized, double-blind, controlled trial, more than 400 patients with knee OA received 3-week intra-articular injections of intermediate molecular weight (800–1500 kDa) and lower molecular weight (500–730 kDa) HAs. These injections reduced moderate to severe pain after 6 months. up to 50% of the original values. Joint function improved to the same extent, and on average more than 65% of patients responded to treatment. However, the authors note that treatment with intermediate molecular weight GCs may be more effective than treatment with low molecular weight GCs for symptoms of knee OA over 6 months. with similar safety [27].
Currently, there are many HA preparations that differ in production technology and molecular weight. HA preparations with a molecular weight of 500–800 kDa are most often of animal origin, while in the production of drugs with a higher molecular weight, the method of bacterial fermentation or synthesis is used, which avoids negative consequences. Thus, in a study by RD Altman, it was demonstrated that drugs with low molecular weight of animal origin more often cause adverse events, such as an allergic reaction and reactive synovitis, while HA drugs that underwent bacterial fermentation showed good efficacy and high safety [28] .
In a study by A. Asari et al. [29] demonstrated that HA with a molecular weight of 800 kDa weakly protected against cartilage loss, but the use of HA with a molecular weight of 1900 kDa had a pronounced chondroprotective effect. HA with an average molecular weight (about 2000 kDa) penetrates damaged tissues much more efficiently than high-molecular HA.
The unique viscoelastic properties of HA impart shock-absorbing and lubricating properties to synovial fluid. HA limits the entry of large plasma proteins and cells into the synovial fluid, but facilitates metabolic processes between synovial capillaries and cartilage and other joint tissues. In addition, HA can form a pericellular sheath around cells, interact with proinflammatory mediators, and bind to cellular receptors such as CD44 and RHAMM (receptor for hyaluronate-mediated motility), where it modulates cell proliferation, migration, and expression. genes. It has been shown that all these physicochemical and biological properties of HA depend on its molecular weight. Experimental data indicate that the binding of HA to cellular receptors depends on its molecular size. Low molecular weight HA often produces opposite cellular responses compared to high and medium molecular weight HA. Studies on animal models of OA have shown that HA with an average molecular weight is generally more effective in reducing indicators of synovial inflammation and restoring the rheological properties of synovial fluid (viscoinduction) than HA with a high (more than 3 mDa) molecular weight [30].
In a study by E. Maneiro et al. Chondrocytes were isolated from cartilage obtained from joint replacement surgery in patients with OA and cultured for 24 hours to detect prostaglandin E2 and for 48 hours to measure nitric oxide (NO) levels. After this, they were incubated with HA and stimulated with IL-1 at a concentration of 5 ng/ml. Two HA preparations were used in the study: with a molecular weight of 500–730 kDa and more than 6000 kDa. As a result, a drug with a molecular weight of 500–730 kDa reduced the synthesis of both IL-1-induced NO and prostaglandin E2 by 70% and 45%, respectively, in contrast to GC with a molecular weight of more than 6000 kDa, which did not cause demonstrated similar results [31].
Both low-molecular-weight and medium-molecular-weight hyaluronates have significant efficacy in the treatment of patients with knee OA, as evidenced by the results of a study among patients in Japan [32].
A recent study (2021) evaluated the effects of intra-articular HA administration on the histopathological characteristics of TMJ induced OA cartilage and disc in rabbits. Cartilage and articular disc recovery were demonstrated after 30 days, with medium molecular weight drugs having better effects on joint tissue than high molecular weight drugs. However, after 135 days, regression of joint tissue restoration was observed in both groups, which confirms the need for regular courses of therapy to maintain the obtained effect [33].
When studying the mechanisms of the analgesic effect upon intra-articular administration of GC in a study by S. Gotoh, it was found that GC with a molecular weight of 2–2.5 mDa had a stronger and longer-lasting analgesic effect than GC preparations with a higher molecular weight [34].
Thus, it is important to consider the molecular weight of HA when prescribing drugs for the treatment of OA. According to the above data, the use of Fermatron 1% and Fermatron plus with a molecular weight of HA of 1.9 mDa and 2–2.5 mDa, respectively, maximally corresponds to the basic concept of OA therapy - safety and effectiveness. Their use when administered intra-articularly helps reduce pain with minimal risk of adverse events.
A large number of clinical trials have found that GC is safe and well tolerated by patients with OA when administered intra-articularly [35, 36].
Many randomized clinical trials and meta-analyses have now proven the superiority of GC use in knee OA over placebo and NSAIDs [37]. Some experts believe that intra-articular administration of HA has a more favorable safety profile than the use of NSAIDs [38]. Prescribing GCs can be a good alternative to the latter in the treatment of OA. Particular attention should be paid to prescribing GC drugs to elderly patients and patients with high comorbidity. HA preparations not only help reduce the intensity of pain in OA, but also improve joint function, and the duration of the effect can last up to 6 months. [39–41]. The effectiveness and safety of intra-articular injection of HA have been demonstrated in practice [42].
Duration of GC use and long-term results
Recently, the issues of duration of HA use have been frequently discussed. A. Concoff et al. [43] showed the benefits of repeated courses of GC use. In a meta-analysis of 30 studies, the authors demonstrated a significant significant advantage of repeated courses (2-4 courses) in groups of patients who received intra-articular GCs, compared with groups receiving placebo. Similar data were obtained in a systematic analysis by R. Altman, performed in 2022 [44]. The researchers also noted that repeated intra-articular HA injections were effective and safe. The literature provides evidence that treatment with GC drugs increases the time to endoprosthesis replacement and reduces the need for NSAIDs and opioids. Long-term results of the influence of GC therapy (the need for endoprosthetics) were studied in a retrospective analysis of a database of patients who underwent arthroplasty from 2007 to 2011, 7000 of whom received GC and 19,627 did not receive this drug. The study proved that each subsequent course of HA injections increased the time before endoprosthetics. After 4 or more courses of intra-articular GC administration, the need for endoprosthetics was delayed by approximately 2.2 years [45]. These data indicate a positive effect of GC therapy on the progression of knee OA.
Experience of using HA in Russian practice
A product available on the Russian pharmaceutical market that replaces synovial fluid is Fermatron based on sodium hyaluronate. It is produced by bacterial fermentation, sterilization is carried out using the micromembrane filtration method while maintaining maximum nativeness of the drug, pH stabilization is carried out with a phosphate buffer solution identical to human, and maintains a pH of 7.4. It has an optimal molecular weight of HA - 1.1–2.2 million Da. The entire production cycle - from the synthesis of the active substance to packaging - takes place at the manufacturing plant in the UK. Strict quality control is carried out at each stage of production.
A.S. Mikhailova et al. A comparative study of the effectiveness and safety of HA products with high and medium molecular weight (Fermatron) was conducted. The results of the study showed stable relief of both components of the pain syndrome (pain at rest and movement) in the group receiving GC, which indicates the advantage of this drug in providing an analgesic effect [46].
E.A. Belyaeva and O.S. Avdeeva conducted a retrospective study to study the effect of viscosupplementation therapy with Fermatron GC on the need for knee replacement in 766 patients with OA. It was shown that the differences in the need for endoprosthetics after 1 and 3 courses of therapy are significant in all age groups (p<0.05). These differences are due to a decrease in pain intensity and an increase in the range of motion in the target joint in patients who underwent intra-articular injection of GC [47].
There is a lot of controversy regarding the para-articular administration of HA. When studying the periarticular administration of Fermatron for OA of the knee joints, its effectiveness was proven. Thus, in the study by V.P. Popova et al. There was a significant positive effect with this method of GC administration, which manifested itself in a decrease or complete relief of pain in the knee joints and a significant improvement in joint function. The results obtained were maintained for a long time - on average 6.8±1.4 months. The study authors believe that the effectiveness of intra-articular injection and the effectiveness of periarticular injection are comparable. Thus, periarticular administration of HA-based agents may be a good alternative in the treatment of knee OA, since this method of administration is convenient and quite safe [48].