Sustanon 250[edit | edit code]
Yuzhakov Anton Testosterone description of the drug
Sustanon 250 from Organon Sustanon from Gerth Pharmaceuticals (volume 10ml, 250mg/ml)
Sustanon
(also known as
Sustaretard
,
Sust250
,
Sustamed
,
Tetrasterone
,
Sustaver
,
Sustager
) is a mixture of various testosterone esters, first developed and released by Organon as a means of hormone replacement therapy for insufficient secretion of endogenous testosterone.
Currently, almost all mixtures of testosterone esters are equated to Sustanon, for example, the most popular analogue is Omnadren 250. A large number of drugs are manufactured clandestinely. Duration of action of various testosterone esters
Sustanon includes 4 forms of testosterone:
- 30mg Testosterone propionate
- 60mg Testosterone phenylpropionate
- 60mg Testosterone Isocaproate
- 100mg Testosterone Decanoate
- Oil (usually peanut oil) as a solvent
- Benzyl alcohol - as a preservative and antiseptic
Sustanon 250, produced in bottles, is 100% fake and has nothing in common with the original Sustanon 250 (according to storage conditions, testosterone can only be stored in glass containers, the use of rubber caps is strictly prohibited).
Each form of testosterone that is included in Sustanon has a different absorption rate, which allows you to maintain a constantly high level of anabolic hormones in the blood for a month. There is no need for frequent injections; Sustanon is given only once every three weeks (for medical purposes). Some people believe that Sustanon is a combination course in one bottle, but this is not entirely true, because each component of the drug is converted in the body only into testosterone.
The peak of Sustanon's popularity occurred in the 80s and 90s of the last century, at which time a large number of articles were written about the benefits of the drug. However, it should be remembered that Sustanon was not developed as a drug to increase muscle mass, and its main advantage is ease of use. Sustanon has a higher cost compared to individual testosterone esters (in equivalent quantities), while its anabolic properties do not differ from isolated forms of testosterone, which makes its use in bodybuilding not entirely justified.
Sustanon 250 is absolutely identical to the drug Omnadren 250 (manufactured under license by Jelfa SA - Poland).
Availability in the 90s[edit | edit code]
Material from the book
P. Grunding, M. Bachmann. "Anabolic steroids" 1994[1]
Sustanon is widely available on the black market and is easy to buy. Unfortunately, most of these drugs are more or less well-executed counterfeits. If you are offered ampoules without a paper label, but simply with a stamp, most often in red, these are definitely fakes. Most often, we are talking about Omnadren, where the corresponding inscription has been erased and replaced with the imprint “Sustanon”. Original Sustanon, which is almost exclusively produced, always has a paper label. The original “Susta” is now becoming increasingly difficult to find and is becoming increasingly rare. On the black market, only Portuguese Sustanon 250, Dutch Sustanon 250 and especially Russian, as well as Indian Sustanon 250 are most often found. All three drugs have a paper label on the ampoules.
Recently, on the black market you can increasingly find Russian Sustanon 250, which is produced in Calcutta (India) and is officially intended only for export to Russia. And yet, through Czechoslovakia, large quantities of this original drug Sustanon 250 are smuggled to Germany. It seems to be a high quality drug, because... Those who use it report positive results and good tolerability, so dishonesty in its production is excluded. Russian Sustanon 250 is sold in plastic packaging, on the back of which the name of the drug, the name of the manufacturer and the chemicals contained are written in blue font. The text is written either on silver foil or on white paper. 5 ampoules are arranged together in a row, and each ampoule is also separately packaged. The original Sustanon 250 costs on the black market, judging by experience, 12 - 18 DM per ampoule and it is worth it.
Availability in the 2010s[edit | edit code]
New brands are widely distributed (Sustamed from Balkan, Sust250 from Allchcemasia, Sustaged from Golden Dragon, SUSTANON from SP Laboratories, Sustaject from Neo Labs, Sustaver from Vermodje). Sustanon from Organon is also popular and is produced in branches of different countries: Egypt, Pakistan and Holland. Cost 250 - 370 rubles. for 1 ml. Vials have become a more popular dosage form, while Organon continues to be produced in ampoules.
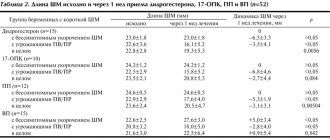
Long-acting forms of testosterone in the treatment of hypogonadism
Definition and classification
Hypogonadism is a clinical syndrome caused by the inability to provide a physiological level of testosterone associated with dysfunction of one of the links of the hypothalamic-pituitary-gonadal (HPG) system with a normal sperm count.
There are primary and secondary testicular failure.
Primary testicular failure is a testicular disease manifested by low testosterone levels, impaired spermatogenesis and increased levels of gonadotropic hormones.
Secondary testicular failure is a disorder at the central level in the hypothalamus and pituitary gland, characterized by low or normal levels of gonadotropins and low testosterone levels.
This classification is important for the choice of treatment tactics, since with secondary hypogonadism, unlike primary, fertility can be restored with appropriate hormonal stimulation. In men with primary testicular failure, childbearing is most often impossible. Further evaluation of patients with secondary hypogonadism reveals pituitary tumors or systemic diseases.
Late-onset hypogonadism is an age-related syndrome characterized by typical clinical symptoms caused by low levels of testosterone in the blood. The presence of late hypogonadism worsens the patient’s quality of life and leads to dysfunction of many organs and systems. This term includes concepts such as andropause, androgen deficiency in old age, partial androgen deficiency in aging men. An age-related decline in testosterone levels is associated with dysfunction of both the testicles and the hypothalamic-pituitary axis. At the same time, testosterone levels decrease with age in men by an average of 1-2 per year, although a lower testosterone concentration compared to the lower limit of normal for a healthy young man is observed only in some elderly patients.
Less commonly, hypogonadism can serve as one of the manifestations of the pathology of the HGG system in men with a mutation of the DAX-1 gene, hemochromatosis, sickle cell anemia, thalassemia, during treatment with glucocorticosteroids, and alcoholism.
Clinical picture of hypogonadism
Diagnosing androgen deficiency in men presents certain difficulties. Clinical symptoms of hypogonadism are nonspecific and depend on age, comorbidities, severity and duration of the disorder, varying sensitivity to androgens, and previous testosterone therapy.
We list the symptoms and signs indicating the presence of androgen deficiency in men.
- Incomplete sexual development, eunuchoidity, aspermia.
- Decreased sexual desire (libido) and activity.
- Decreased frequency of spontaneous erections.
- Feeling of discomfort in the mammary glands, gynecomastia.
- Reduced amount of body hair (axillary and pubic), slow hair growth, particularly on the face.
- Reduced testicles.
- Infertility, absence or low sperm count in semen.
- Decreased height, fractures due to minor injuries, low bone mineral density.
- Reduced muscle mass and strength.
- Hot flashes, increased sweating.
The above clinical symptoms and signs were established based on a study by doctors of a population of patients being treated in the clinic, who are likely to have a more pronounced androgen deficiency; There have been no observations of men with classical androgen deficiency in the general population.
The threshold testosterone concentration below which symptoms of androgen deficiency occur and adverse health effects develop remains unknown and may be age dependent. Moreover, the testosterone concentration at which the drug is effective remains unknown and may vary depending on the individual patient and target organ.
Less specific symptoms and signs that occur with androgen deficiency include the following.
- Decreased energy, motivation, initiative, self-confidence; aggressiveness.
- Feeling sad, depressed, depressed mood.
- Decreased concentration and memory.
- Sleep disturbances, increased drowsiness.
- Mild anemia (normochromic, normocytic, within the range typical for women).
- Decreased physical activity and performance.
Thus, the data available today indicate that there is no clear threshold testosterone level at which lower levels would indicate clinical symptoms of androgen deficiency and which would be a criterion for diagnosing hypogonadism in all patients.
Laboratory diagnostics
Determination of testosterone levels. It should be noted that determination of testosterone levels is indicated only for patients with clinical signs of androgen deficiency. The most important parameters in identifying hypogonadism are total and estimated free testosterone, which is determined by calculating the level of total testosterone and sex hormone binding globulin (SHBG). It is important to determine testosterone between 7 and 11 am, when its level is highest.
It is believed that the minimum testosterone threshold level is not constant and depends on geographical and ethnic factors. However, the minimum level of testosterone at which hormone replacement therapy is not required has now been officially determined. Thus, the lower limit of normal is the level of total testosterone 12 nmol/l (346 ng/dl) and free testosterone 250 pmol/l (72 pg/ml). It was also determined that when the level of total testosterone is 8 nmol/l (231 pg/ml) and free testosterone is 180 pmol/l (52 pg/ml), hormone replacement therapy is indicated. With intermediate testosterone levels and the presence of symptoms of hypogonadism, the indication for hormonal therapy is to exclude other causes of the disease.
It must be remembered that in 30% of cases, a repeat test reveals a normal testosterone level. In addition, 15% of healthy young men may experience a decrease in testosterone levels compared to normal values within 24 hours. Therefore, if a discrepancy between the clinical picture and laboratory diagnostic data is detected, it is better to repeat the tests.
The evaluation of a patient with androgen deficiency should include a general health assessment to rule out systemic diseases, the use of certain medications (eg, opiates or high-dose glucocorticoids) and recreational drugs that affect testosterone production and metabolism, eating disorders and excessive exercise, such as how these conditions may cause a transient decrease in testosterone levels. The diagnosis of androgen deficiency should not be made during the acute phase of a viral respiratory illness.
The following are groups of patients who are often found to have low testosterone levels. All of them are indicated for determination of androgen levels.
Conditions in which it is recommended to determine testosterone levels in the blood:
- Mass formation in the area of the sella turcica, exposure to radiation in the area of the sella turcica or other diseases of the sella area.
- The use of drugs that affect the production and metabolism of testosterone, such as glucocorticoids, ketoconazole and opioids.
- Weight loss during HIV infection.
- End-stage renal failure and hemodialysis.
- Moderate and severe chronic obstructive pulmonary diseases.
- Infertility.
- Osteoporosis or fractures due to minor injuries, especially in young men.
- Diabetes mellitus type 2.
Thus, diagnosing androgen deficiency in certain groups of patients makes it possible to identify patients with diseases that may seem unrelated to androgen deficiency. For them, testosterone therapy is also indicated and may be useful in treating the underlying disease.
Determination of FSH, LH and additional examinations. After identifying androgen deficiency, for the differential diagnosis of primary (testicular) and secondary (hypothalamic-pituitary) hypogonadism, determination of the level of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) in the blood plasma is indicated. In men with primary testicular failure of unknown etiology, we recommend a karyotype study to exclude Klinefelter syndrome. In patients with suspected secondary hypogonadism, additional examinations are necessary to exclude pituitary tumors, hyperprolactinemia, hemochromatosis and other infiltrative processes, obstructive sleep apnea syndrome and genetic disorders associated with gonadotropin deficiency.
Imaging of the pituitary gland is recommended using magnetic resonance imaging (MRI) to exclude tumor, infiltrative processes, severe secondary hypogonadism (plasma testosterone level < 150 ng/dL), panhypopituitarism, persistent hyperprolactinemia, symptoms or signs of tumor compression, such as headaches, visual impairment, visual field defects.
Testosterone stimulates bone formation and prevents bone resorption. Numerous mechanisms underlie this effect of testosterone, including processes regulated by estrogen and androgen receptors.
It is recommended to determine bone density using dual-energy x-ray absorptiometry in men with severe androgen deficiency and with fractures due to minor injuries.
Treatment
The presence of clinical symptoms of hypogonadism and low testosterone levels confirmed by laboratory testing are an indication for hormone replacement therapy. Testosterone preparations can be used either as monotherapy or in combination with other drugs. Testosterone monotherapy may be effective in treating erectile dysfunction in men with hypogonadism. However, treatment with testosterone alone has a more pronounced effect on libido than on erectile function. During testosterone therapy, men with hypogonadism report improved ratings of sexual activity, more frequent thoughts and fantasies related to sex, increased attention to erotic stimuli, and an increase in the frequency and duration of nocturnal erections. There is an improvement in hair growth in some androgen-dependent areas, in addition, with testosterone therapy in healthy men with hypogonadism, muscle mass and strength increase, the volume of adipose tissue decreases, and an increase in bone mineral density is noted.
The use of testosterone improves mood. Uncontrolled studies have shown increased feelings of alertness and well-being after testosterone use. The effects of testosterone on cognitive function have been poorly studied, with some studies finding small effects on visual spatial perception, verbal memory, and fluent speech.
Thus, the use of testosterone is aimed at preserving secondary sexual characteristics in men, improving sexual function, maintaining good health and maintaining bone mineral density, i.e., correcting the main symptoms of hypogonadism.
When prescribing testosterone therapy, one should strive to increase its content to an average level within normal values.
Characteristics of testosterone preparations
Currently, there are various dosage forms of testosterone available that have proven effectiveness and safety. These include drugs for intramuscular administration, subdermal and transdermal use, and tablet forms. To successfully carry out hormone therapy, the doctor must clearly understand the pharmacokinetics of testosterone drugs, although the choice of one form or another of the drug depends on the patient’s preferences.
There is a risk of complications due to testosterone therapy. In this case, rapid withdrawal of the drug's effect may be required, which is only possible with treatment with short-acting forms of testosterone (transdermal, tablet and buccal preparations). Therefore, in late hypogonadism, short-acting drugs have an advantage over deposited forms (intramuscular, subcutaneous).
Preparations for oral use. Testosterone undecanoate (Andriol) is well absorbed when administered orally, but due to rapid breakdown in the liver, it does not adequately maintain sufficient levels of testosterone in the blood. 17-α-alkylated testosterone derivatives (especially methyltestosterone) are resistant to liver enzymes, but their use is currently limited due to proven hepatotoxicity.
Long-acting injectable forms of testosterone: thanks to the effect of esterification, a hydrophobic testosterone molecule was obtained, allowing the drug to prolong its effect. When the oil depot of hydrophobic testosterone is administered intramuscularly, it is slowly released, causing a prolonged effect.
Testosterone enanthate and testosterone cypionate (Testred Cypionate) have similar pharmacokinetic properties. In case of an overdose of these drugs, the levels of estradiol and dihydrotestosterone in the blood may exceed normal values. The usual daily dose of the drugs is 100 mg per week. 200–300 mg of testosterone enanthate is administered every 2–3 weeks. The maximum level of testosterone in the blood is achieved 5 days after administration of the drug, the initial level is achieved after 10–14 days. The advantage of these drugs is the low cost of treatment and the possibility of obtaining high concentrations of testosterone in the blood. Disadvantages include pain at the injection site and the need for frequent visits to the doctor to re-inject the drug.
Currently, a new parenteral form of testosterone undecanoate (Nebido) has been developed, which allows for a long-term, sustainable increase in testosterone levels in the blood. After two introductory doses of 1000 mg of the drug with an interval of 6 weeks, subsequent injections are made every 12 weeks, which allows maintaining normal testosterone levels in the blood in the vast majority of patients with hypogonadism. In some cases, the intervals between injections can be increased to 14 weeks.
Transdermal testosterone preparations. Transdermal forms of testosterone are available in the form of patches and gels. To achieve the best effect, their daily use is recommended. The daily dose of testosterone with this method of administration is 5–10 mg. The advantage of transdermal drugs is the ability to obtain stable testosterone levels throughout the entire duration of action. The most common side effect when using patches is skin irritation at the application site, which is not typical for the gel form. Individual characteristics of skin absorption may require doubling the daily dose.
Recommended testosterone replacement therapy regimens:
- IM administration of 75-100 mg of testosterone enanthate or testosterone cypionate (Testred Cypionate) weekly or 150 to 200 mg every 2 weeks.
- IM administration of Nebido once every 3 months or first 2 times after 6 weeks, then after 12 weeks.
- Application at night of one or two non-genital 5 mg testosterone patches to the skin of the back, thigh or shoulder, away from contact areas.
- Application of 5-10 g/day of gel containing testosterone to those areas of the skin that are covered by clothing.
- Use of buccal bioadhesive tablets at a dose of 30 mg 2 times a day.
This regimen should be considered as recommended for initiating testosterone replacement therapy; then the dose should be adjusted based on data on the concentration of testosterone in the blood plasma of each patient.
Men receiving testosterone supplements should be monitored according to a standard monitoring regimen. This allows side effects of therapy to be identified as early as possible. When monitoring men with hypogonadism receiving testosterone therapy, it is difficult to determine the indications for prostate biopsy. According to systematic reviews, after the initiation of testosterone therapy, PSA levels increased on average by 0.3 ng/ml in young hypogonadal men and by 0.44 ng/ml in older men. An increase in PSA levels after 3-6 months during testosterone therapy in men with androgen deficiency of more than 1.4 ng/ml is not typical. If this indicator is exceeded, you should pay attention to the condition of the prostate gland, perform TRUS; if questionable areas are identified along the periphery of the gland, a prostate biopsy is indicated. If the rate of increase in PSA exceeds 0.4 ng/ml over a period of less than 3 years, a detailed examination should be carried out and the patient should be monitored more closely.
Possible side effects
Undesirable effects that have been proven to be associated with testosterone use are the following:
- erythrocytosis;
- acne and oily skin;
- the appearance of subclinical prostate cancer;
- growth of metastatic prostate cancer;
- decreased sperm production and fertility.
Rare effects, the connection with the use of testosterone is not so obvious:
- gynecomastia;
- baldness (hereditary);
- progression of symptoms of benign prostatic hyperplasia;
- breast tumor growth;
- the appearance or progression of obstructive sleep apnea syndrome.
Specific undesirable effects of various forms of testosterone preparations:
- for tablets for oral use - effect on liver function and cholesterol levels (methyltestosterone);
- for implanted granules - infectious complications, expulsion of implanted granules;
- for intramuscular injections of testosterone enanthate or testosterone cypionate (Testred Cypionate) - fluctuations in mood and libido, pain at the injection sites, severe erythrocytosis (especially in older men);
- for a skin patch - skin reactions at the site of application;
- for skin gel - the potential risk of transferring testosterone to the skin of another person (the patient must be warned about the need to cover the areas of skin to which the gel is applied with clothing and to wash these areas of skin and hands with soap before close contact with another person);
- for buccal tablets - changes in taste sensations, irritation of the gum mucosa.
Risk factors and contraindications. Hormone replacement therapy has been used in women for a long time. Available indications of an increased risk of developing hormone-dependent diseases force us to pay attention to the possible consequences of hormone replacement therapy in men.
Conditions in which the use of testosterone is contraindicated:
- metastatic prostate cancer;
- mammary cancer;
- undiagnosed nodular formations or indurative process in the prostate gland;
- increased PSA levels of unknown etiology;
- erythrocytosis (hematocrit >50%);
- severe symptoms of lower urinary tract obstruction associated with benign prostatic hyperplasia, more than 19 points on the AUA/IPSS scale;
- severe course of heart failure (III and IV functional class).
Testosterone therapy may be associated with an increased risk of serious adverse effects in men for a number of conditions. Metastatic prostate cancer and breast cancer are hormonally dependent tumors, the growth of which can be stimulated by testosterone therapy; Testosterone should not be prescribed to men with these types of tumors. There is an opinion about the possibility of prescribing testosterone replacement therapy on the basis of an individual approach to patients with low testosterone levels after radical prostatectomy in the absence of signs of the disease for two or more years and if it is impossible to detect PSA in the blood, however, due to the lack of randomized trials, such an approach should not be considered as a recommendation for all patients.
The presence of a nodular formation or inducing process in the prostate gland, as well as an increase in PSA levels, sometimes indicate undetected prostate cancer. In addition, testosterone therapy may worsen the condition in men with erythrocytosis, untreated obstructive sleep apnea syndrome, severe symptoms of lower urinary tract obstruction, and severe heart failure.
Open studies in young hypogonadal men have shown a low incidence of side effects with testosterone replacement therapy. Frequent specific side effects of testosterone are increased hematocrit levels, acne, increased skin oiliness, and a feeling of tension in the mammary glands.
Literature
- Andrology. Men's health and dysfunction of the reproductive system / ed. E. Nishlag, G. M. Bere: trans. from English M.: Mia, 2005. 551 p.
- Seftel AD Male hypogonadism. Part I: Epidemiology of Hypogonadism // Int. J. Res. 2005; Sept; 29.
- Madgar I. et al. Prognostic value of the clinical and laboratory evaluation in patients with nonmosaic Klinefelter syndrome who are receiving assisted reproductive therapy // Fertil. Steril. 2002. Jun; 77(6): 1167–1169.
- Cruger D. et al. Birth of a healthy girl ICSI with ejaculated spermatozoa from a man with nonmosaic Klinefelter's syndrome // Hum. Reprod. 2001; Sept; 16(9): 1909–1911.
- Darby E., Anawalt BD Male hypogonadism: an update on diagnosis and treatment // Treat Endocrinol. 2005; 4(5): 293–309.
- Urology / edited by N. A. Lopatkin. M.: Medicine, 1995. 495 p.
- Dreval A.V. Main syndromes in endocrine diseases of the male gonads // Andrology and genital surgery. 2001. No. 2. P. 22-26.
- Dode C., Hardelin JP Kallmann syndrome: fibroblast growth factor: signaling insufficiency? // J. Mol. Med. 2004; Nov; 82(11): 725–734.
- Chen CJ et al. Early diagnosis of Prader-Willi Syndrome in a newborn // Acta Paediatr Taiwan (China. 2004, Mar-Apr; 45(2), 108-10).
- Nebido // Product Monograph, Andrology. August; 2004: 59.
- Christopher B. Cutter, MD Compounded Percutaneous Testosteron Gel: Use And Effects in Hypogonadal Men // J. Am Board Fam Pract. 2001; 14(1): 22-32.
I. A. Danilov, Candidate of Medical Sciences P. A. Shcheplev, Doctor of Medical Sciences, Professor of the KB of the Administration of the President of the Russian Federation, Moscow/p>
Effects of Sustanon[edit | edit code]
Sustanon works just like any other form of testosterone. This means that the main effects of Sustanon are:
- Increase in muscle mass (on average 6 kg per month)[2]
- Anti-catabolic effect
- Increased appetite
- Increased hematopoiesis - an increase in the number of red blood cells in the blood ensures better oxygen transport, thereby increasing endurance.[3]
- Increased libido (while taking Sustanon)
The drug detection time is up to 3 months.
Is testosterone safe? What to expect from taking testosterone?
Currently, men use testosterone pills, gel or injections to restore normal levels of the male hormone. The ongoing pharmaceutical marketing blitz promises that these "low testosterone" treatments will make men feel more alert, energetic, and sexy. However, side effects remain. For example, some older men taking testosterone may face increased heart risks.
Endocrinologist Associate Professor of Medicine Carl Palle of Harvard Medical School believes that "men should be more alert to possible long-term complications."
Signs of Low Testosterone
| MIND • Depression • Decreased self-confidence • Difficulty concentrating • Sleep disturbance Body Decreased muscle and bone mass • Increased body fat • Fatigue • Breast enlargement • Hot flashes Sexual function Decreased sex drive • Decreased spontaneous erections • Difficulty maintaining an erection |
How do men react to testosterone advertising?
Urologist Michael O'Leary believes that “direct-to-consumer marketing is very aggressive. Thousands of people who would never have asked me this before started doing so when they saw the ad: “Are you feeling tired?”
Fatigue alone is not enough to warrant a prescription for testosterone. "General fatigue and malaise are pretty low on my list," says O'Leary. “But if there are significant symptoms, a laboratory test will need to be taken. Most men have normal testosterone levels.”
If a man's testosterone is below the normal range, there is a good chance that the man may take hormone supplements indefinitely. “There is a slight lure of testosterone,” notes endocrinologist Palle. “Men start taking testosterone and they feel better, but then it’s hard to get rid of it. During treatment, the body stops producing testosterone on its own. Men can often feel a big difference when they stop therapy because their body's testosterone production has not yet been achieved."
This wouldn't matter much if we were confident that long-term hormone therapy was safe. But some experts worry that testosterone therapy exposes men to some risks that could be harmful over time.
What are the risks of testosterone therapy?
Relatively few men experience immediate side effects from taking testosterone, such as acne, trouble breathing during sleep, swollen or tender breasts, or swollen ankles. Doctors also watch for high red blood cell counts, which can increase the risk of clotting.
Men taking testosterone long-term appear to have a higher risk of cardiovascular disease, such as heart attacks, strokes, and death from cardiovascular disease. For example, the Testosterone in Older Men study was stopped in 2010 when early results showed that men treated with hormonal drugs had significantly more heart problems. “In older men, the theoretical cardiac side effects become more immediate,” notes Palle.
Some doctors are also concerned that testosterone therapy may stimulate the growth of prostate cancer cells. As with the hypothetical heart risks, the evidence is mixed. But because prostate cancer is so common, doctors tend to be cautious about prescribing testosterone to men who may be at risk.
For men with low blood testosterone levels, the benefits of hormone replacement therapy usually outweigh the potential risks. However, for most other men, this is a shared decision with your doctor. Testosterone gives men the ability to feel better when they're feeling down. But this quick fix may distract attention from unknown long-term dangers. "I can't tell you for sure that it increases your personal risk of heart problems and prostate cancer, or that it doesn't," Palle concludes.
So, keep the risks in mind when considering testosterone therapy. “I often don’t approve of this, especially if the man has health problems.”
Rate your health
- Have you considered other reasons why you may be experiencing fatigue, low sex drive, and other symptoms associated with low testosterone? For example, do you eat healthy? Do you exercise regularly? Are you sleeping well? Consider these factors before moving on to hormone therapy.
- If your sex life isn't what it used to be, have you ruled out relationships or psychological issues that could be contributing to it?
- If erectile dysfunction has you suspecting "low testosterone" as the culprit, consider that cardiovascular disease can also cause erectile dysfunction.
Get an accurate assessment of your health
- Inaccurate or misinterpreted test results can either misdiagnose or miss a case of testosterone deficiency. Testosterone levels should be measured between 7 a.m. and 10 a.m., when they peak. Confirm low readings with a second test on a different day. Determining bioavailable testosterone, or the amount of hormone capable of affecting the body, may require multiple measurements and careful interpretation.
- After starting therapy, check with your doctor periodically to check your testosterone and other laboratory tests to make sure the therapy is not causing problems with your prostate or blood chemistry.
Be aware of unknown risks
- Approach testosterone therapy with caution if you are at high risk for prostate cancer; have severe urinary symptoms from an enlarged prostate; or you have been diagnosed with heart disease, a heart attack.
- Ask your doctor to explain the different side effects for different testosterone formulations, such as gels, patches, and injections. Know what to look for if something goes wrong.
Realistic Expectations from Taking Testosterone
Testosterone therapy is not the fountain of youth. There is no evidence that it will restore you to the level of fitness or sexual function of your youth, prolong life, prevent heart disease or prostate cancer, improve memory or mental acuity.
If erectile function has been a problem, testosterone therapy may not fix it. In fact, it may increase your sex drive, but it won't allow you to act on it. You may also need medication or other therapy to get or maintain an erection.
How to improve your health without drugs?
Sustanon - side effects[edit | edit code]
Like any other form of testosterone, Sustanon is converted into estrogens. For this reason, Sustanon causes side effects such as gynecomastia, edema, female-type fat deposition and inhibition of the production of testosterone. These side effects can be prevented by using antiestrogens, preferably aromatase inhibitors. Selective estrogen receptor modulators (tamoxifen, etc.) are used only during post-cycle therapy.
As a result of a decrease in the production of endogenous testosterone, it is possible to develop such a serious side effect of Sustanon as testicular atrophy. This side effect can be prevented if you do not take a Sustanon course longer than 8 weeks and take antiestrogens. Longer courses require the use of gonadotropin.
In the body, testosterone is converted into dihydrotestosterone, which causes the following side effects: prostate hypertrophy, baldness, acne and others. These are the so-called androgenic side effects of Sustanon.
Also, athletes often report an increase in temperature and a flu-like condition during the course of Sustanon. Like most steroids, Sustanon increases the level of bad cholesterol in the blood (prevented by taking Omega-3 throughout the course).
After injection, infiltrates sometimes form (lumps or “bumps” in the gluteal region or other injection site). As a rule, infiltrates resolve within 2-5 weeks.
“Testosterone is a very insidious hormone”: interview with an endocrinologist
We continue a series of meetings with outstanding domestic doctors. Today - a detailed conversation about our endocrine system in general and the “favorite” male hormone testosterone in particular with the director of the Endocrinology Clinic of the First Moscow State Medical University. Sechenov Valery Fadeev.
We know that endocrinology is about hormones; we often hear “check your thyroid.” On the other hand, many have a rather poor idea of how the activity of the thyroid gland is related to the daily functioning of the body, in particular the male one.
There is a very big difference between the functioning of the female and male endocrine systems, despite the fact that the set of hormones in men and women is the same. The difference is in the quantity and nature of secretion. A significant part of the hormones in the female body is produced cyclically, and in the male body - tonically, that is, continuously, without monthly cyclicity. The human hypothalamic-pituitary system is tuned to such “male” hormone production by the appearance of a certain amount of testosterone during fetal development, from the moment of fertilization to the birth of the child.
I will ask you in particular detail about testosterone, which is of great interest to our readers. But let's start, if possible, with the basics - with the functions of the thyroid gland.
Thyroid hormones are the most ancient in origin; they regulate the most basic functions of the cell. And every cell. More precisely, they regulate the processes of oxidation and oxygen consumption by the cell. Our body can be compared to a stove in which a fire burns. We throw firewood there - what we eat. In order for a fire not to go out, oxygen is needed. There is a damper in the stove, and with its help we can make the flame stronger - by opening it wider, or we can dim it - leaving a small crack, and the fire will smolder. The function of thyroid hormones is to control the valve, or more precisely, the intensity of oxidation, combustion, which results in the formation of heat - the energy that every cell needs.
How did we even know that hormones exist in our body?
Before the concept of “hormone” appeared, we were talking about the so-called humoral factors. Back in the 14th century, the Chinese associated secondary sexual characteristics with them: doctors of that time said that “the beard is an external manifestation of the power of the male seed,” “the beard is related to the kidneys and testicles.” In the middle of the 19th century, the German professor Berthold conducted experiments: a rooster was castrated, as a result of which his secondary sexual characteristic, the comb, regressed. After this, the extract of the removed testes was injected into the cockerels, and the comb was restored. These were the first experiments related to testosterone. The very concept of “hormone” appeared later, at the beginning of the 20th century, and since then its interpretation has undergone numerous transformations.
Endocrinology was formed as a field of medicine dealing only with hormones?
Yes, classical endocrinology concerns seven anatomically distinguished endocrine glands: thyroid, parathyroid, pituitary gland, pancreas, adrenal cortex, testes and ovaries, pineal gland. These are endocrine glands that secrete hormones. Actually, the name “endocrinology” translates as “the science of what is secreted inside” - it studies the chemical substances secreted by these glands into the blood and regulating the functions of many cells.
Explain the interaction between the nervous and endocrine systems.
Comparing the nervous system with the endocrine system is like comparing a telephone and a radio. The nervous system is a telephone: wires-nerves that come from the brain and transmit information to a specific point. The hormonal gland produces information that is distributed through the blood to many people - like a radio that broadcasts from one point, but everyone hears it. That is, the impulse of the endocrine system is a loudspeaker. When there is a failure in the nervous system, only what is activated by this nerve stops working - one muscle: just like if you break a telephone wire, only the telephone will not work. And if the radio station breaks down, no one will hear the message. That is, the pathology of the endocrine system is multisystem - it is a pathology of many structures at once. An example is the hormones of the thyroid gland, which act on almost all cells of our body. In our cell, everything is energy-dependent - all enzyme systems, all their functioning, since every cell contains ATP, adenosine triphosphate - our battery. And the intensity of energy production in it is regulated by thyroid hormones.
Should a young man, who is not worried about anything, visit an endocrinologist one day for a prophylactic visit?
Preventive medicine in general is a rather controversial thing. The popular concept of “the more you examine, the better” is fundamentally wrong. In the modern world, unnecessary examinations can cause no less harm than their absence, including because their interpretation is very difficult. Ultrasound reveals one-millimeter structures in the thyroid gland. And they can make more noise without causing any consequences. We can talk about preventive endocrinology, first of all, in connection with blood sugar levels. If we are talking about an overweight man, it is advisable to control sugar from the age of 20–25 - at least once every few years. This should also be done if the parents were sick with diabetes or had cardiovascular pathology.
Are diseases of the endocrine system inherited?
The tendency is inherited. These are so-called multifactorial diseases - there is a certain predisposition that may or may not be realized. If a person is prone to diabetes, but does not gain excess weight, he may not get sick. That is, environmental factors, in particular food, can contribute to the implementation of the genetic factor. Thirty years ago we called type 2 diabetes age-related, but today it occurs even in children. Unfortunately, we often see diabetes in 25-year-old obese patients. By the way, it is important to say that there is an obvious connection between obesity and decreased testicular function. With severe obesity, testosterone levels decrease. The fact is that adipose tissue is the site of sex hormone exchange; when a man becomes obese, the balance of estrogen and testosterone changes. This leads to suppression of pituitary regulation of the testes and decreased testosterone production.
What do young men usually turn to an endocrinologist for?
In men aged 20–30 years, endocrine pathology occurs relatively infrequently—almost ten times less often than in women. But if a man develops, say, Graves' disease at a young age, then it is much more severe and has a worse prognosis. Why? It is difficult to say, there are no clearly proven explanations. But I repeat once again - at a young age, pathology of the thyroid gland in men is rare. The greatest problem is the decline in its functions, which occurs in men after 40 years of age. The symptoms of this disorder are very nonspecific: we can talk about, let’s say, an incomprehensibly bad state of health - a general loss of strength, lethargy, fatigue, decreased muscle tone, potency, libido, erectile dysfunction, that is, some non-specificity that could potentially be the background or a trail of any disease. In a hospital sample, as we call it, if a patient comes to the doctor and there is a set of these factors without an obvious concomitant disease, and even more so if it is present, it is better to check the function of the thyroid gland.
What methods are used for this today?
Blood is taken from a vein and one indicator is determined - TSH, thyroid-stimulating hormone of the pituitary gland. Its level allows you to more than accurately assess the functioning of the thyroid gland. Problems with this hormone are more common in women, but it is not uncommon for men either.
It turns out that from the point of view of the hormonal system, men are more protected by nature?
Yes, but they live on average twenty years less. In fact, a woman is protected by nature - and from the position of the endocrine system too. She still has the task of reproduction, while the biological significance of a man who has performed the copulatory function is practically complete.
If you remember the copulatory function, let's talk about testosterone, which worries everyone so much.
Testosterone is a very interesting hormone, one might say, insidious. This is the 21st century, and there is still no understanding of how to accurately determine it - all methods have flaws. Hormone levels are measured using immunometric methods, that is, using antibodies. Testosterone is a steroid hormone, very small in structure; the size of the antibody is a certain number of times larger. That is, the number of testosterone is a very delicate matter. It must be able to interpret it depending on the situation, in combination with other hormones, with gonadotropins - hormones of the anterior pituitary gland. Therefore, the prevailing opinion that if you were given a huge amount of testosterone in a laboratory, then you are a superman is wrong. In general, this is part of the myth that endocrinology is some kind of attachment to a hormonal laboratory: we sit here, send everyone for hormonal studies, get a number, and make a diagnosis. Absolute nonsense.
What is the main task of endocrinology?
This is a clinical discipline, the same as, say, cardiology. And the interpretation of laboratory tests is often at the last stage of our reasoning. The cardiologist also has an echocardiogram: it can be completely fine, but the person has a whole bunch of problems. The same can be said with regard to hormones: if the diagnosis could be made by numbers, I would not be needed here. You can assign a laboratory assistant to make diagnoses and write prescriptions directly on the hormonal test results form.
Let's trace the life process of testosterone in the context of the maturation of the male body.
Let's. We will omit puberty and early development - there are very complex, I would even say, ornate processes in the relationship between the hormones of the adrenal cortex and the testicles, which is hardly interesting to your readers. By the age of 20, testosterone production levels reach peak values, and from the age of 30, slowly, slowly, differently for everyone, but in general, quite naturally, they begin to decline. Testosterone is produced in the testicles, but it is a deep misconception to consider it a hormone created by nature only for erection. Erectile function can be completely normal even with low testosterone, but sex drive, desire, libido - call it what you want - will most likely be reduced. Testosterone is an anabolic steroid for the male body; it does almost everything that distinguishes a man from a woman; it contributes to the development of not only the reproductive system, but also the muscular system, the brain, and even the production of red blood cells. Without it, a man turns into a eunuch - a thin voice, lack of hair growth, flabby muscle system, obesity, tummy. But at the age of your readers, testosterone deficiency is quite rare. If you take one hundred percent of men aged 20–30 years with erectile dysfunction, then probably 90–95 percent have a psychogenic problem. After all, erectile function has many components, first of all, the brain; the system is very complex. And most often it fails due to various kinds of violations: childhood fears, complexes, neuroses, personality disorders, relationships between partners, that’s all. But the real testosterone deficiency, rather, looks towards the age of “50 plus”. And this is where a lot of speculation arises on this very topic.
Pharma machinations?
Partly yes. In part, the lobby of those involved in erectile dysfunction is inflating this topic. Both abroad and here we have “specialists” who are ready to pin testosterone deficiency on literally everyone, blaming almost all male diseases, including obesity, for this deficiency. Almost diabetes is treated with testosterone. After all, what is a deficit? The figure is below normal. And this concept is very relative, especially for hormones. This is the case when the word “norm” must be put in large quotation marks. There is no norm, there is a reference, and this is a statistical concept: they took, relatively speaking, one hundred healthy men aged 20–30 years, looked at testosterone, calculated the average, removed the Gaussian dome and got two numbers.
At the same time, there are characteristics of the population: racial, regional, age...
That's it, age. And here you can speculate endlessly. He moved the reading frame and said: “You have a deficit...”
"…take a pill".
Yes, “take a pill.” Firstly, there are not many studies that have studied the use of testosterone in older men, and secondly, they are not as long-lasting. Some of them had positive results, some had negative results in terms of cardiovascular risk.
So does artificially increasing testosterone levels entail a risk of cardiac problems?
I can’t give a definite answer. But research results in this sense are contradictory. There is a figure that clearly shows testosterone deficiency, then its administration has positive consequences. But if we take the “gray” zone, as we call it, when someone considers this value to be a deficit and others do not, here this assignment most often does not lead to any results. After all, hormones are part of a large integrated system within a person. Man, unfortunately, is mortal, and no one can do anything about it yet. A person ages, and all his systems age, including the endocrine system, integrally adapting to a particular age. And if at the age of 60 you begin to artificially make yourself 18 with the help of pills, you cause a conflict of systems. It’s not for nothing that the Old Testament says: “No one puts new wine into old wineskins; otherwise the new wine will burst the skins and flow out on its own, and the skins will be lost.” You see, a hormone is a systemically acting active element. If you introduced testosterone into the systemic circulation, it affected not only your penis: it affected the brain, the heart, the blood vessels, the liver - everything! This means that the consequences can also be systemic.
And unpredictable?
Well, if someone wants to experiment and is ready, as in “Egyptian Nights,” to get some kind of stroke during one sexual act, that’s his choice. But in any case, you shouldn’t do this at 20–30 years old. If you have sexual problems at this age, don’t immediately blame low testosterone. Yes, this happens, but extremely rarely, and then it is a serious violation. But often in such a situation they grasp at borderline results, when prescribing testosterone is simply a convenient solution for the doctor.
Why is such an appointment dangerous?
There is an aspect in which the male body is more delicate than the female - I'm talking about the production of sperm. External administration of testosterone suppresses it. In general, as soon as a person has even a severe runny nose with fever, spermatogenesis will be suppressed for some time. Nature has arranged it this way: a sick male should not fertilize females. You don’t even need a runny nose: let’s say a man is exhausted at work, is nervous, doesn’t get enough sleep at night - in this situation he will have low testosterone simply due to a general loss of strength. Even at a young age. We experimented in our clinic: we looked at testosterone in patients with diabetes during hospitalization, and then two weeks after he had been with us. First of all, the man got enough sleep. Secondly, we have put some general indicators in order. And after two weeks his testosterone is already normal! A single determination of testosterone cannot be trusted at all. And when they begin to evaluate the spermogram of a man who is sick with some kind of chronic disease, uncompensated, this is also absurd. The first thing you need to do is cure him. Bring it back to normal, and then evaluate the functioning of the reproductive system. Or he's on a drinking binge...
This is also an interesting topic - alcohol and male hormonal levels. Does whiskey actually lower blood sugar?
Any ethanol, any ethyl alcohol potentially blocks the production of glucose by the liver, and for some time can actually reduce sugar levels. But I don’t recommend treating diabetes with alcohol—it doesn’t matter whether it’s whiskey, vodka or tequila.
But what about the cherished 40 milligrams per day, which are allowed even by cardiologists?
40 milligrams is possible - of course, provided that the person is ready to stop there. Alcohol is a universal tranquilizer, and in the modern world it also plays a positive role, helping a person in a state of chronic stress to relieve this stress. Chronic stress, by the way, also has a bad effect on sexual function. So no one is against alcohol in small quantities to reduce stress. But in large cases, it only causes harm, disrupts erection and ejaculation. You ask about the connection with the functions of the thyroid gland - alcohol does not directly affect it. And on sexual function - only negatively.
Are you talking about fertility?
Exactly. In chronic alcoholics, testicular function is completely impaired. Against the background of intoxication, testosterone production decreases and spermatogenesis is disrupted, this has been proven. And if we are talking about fertility, today there are practically no medications that affect spermatogenesis. This is such a subtle and complex process that we have not yet learned how to interfere with it. In a woman, you can stimulate ovulation in order to obtain an egg, but if a man’s spermatogenic epithelium is affected, there are no treatment methods.
What exactly negatively affects the function of this epithelium?
The epithelium produces sperm. And many factors influence this process, including your own testosterone. The cells that produce it in the testicle are nearby and influence each other: Sertoli cells, Leydig cells, which form the spermatogenic epithelium, are connected in local regulation. Plus, testosterone production and sperm production in the testicle are influenced by pituitary hormones. So this epithelium is quite sensitive to toxic influences.
To anyone, not just alcohol?
Of course. Here is a simple example: let’s say, God forbid, if we are talking about malignant tumors for which chemotherapy is prescribed, practically the first thing that suffers is the spermatogenic epithelium. Because dividing cells are killed. So, sperm cryopreservation is recommended for young patients before prescribing antitumor chemotherapy.
Let's continue our endocrinological educational program. What is important to know about the work of the pituitary gland and hypothalamus?
We are talking, rather, about the work of the hypothalamic-pituitary system. The nuclei of the hypothalamus are the nuclei of the nervous system that produce humoral factors. These are, as a rule, very small molecules consisting of several amino acids, which enter the pituitary gland through very short vessels and there stimulate the production of pituitary hormones. The pituitary gland is such a conductor, a key regulatory structure of many elements of the endocrine system. This means that sexual function, the functioning of the thyroid gland, adrenal glands, the production of prolactin, the production of growth hormone and a number of other factors depend on it.
Including metabolism?
You know, endocrinologists get a little stupefied when they hear the expressions “metabolism is disturbed” or, say, “hormonal levels.” Human life is all about metabolism, and everything is involved in it, including eyes, teeth, hair, ears and nails.
Let's not fall into a stupor, let's return to the hypothalamus.
The hypothalamus interacts between the nervous and endocrine systems. These systems are interconnected, they function together. But, returning to the beginning of the conversation, nervous systems are a quick regulation, like a phone call: an impulse came and the muscles instantly contracted. The humoral system, including the production of hormones, is a slower basal regulation that carries out fundamental life processes. Here we must remember the evolution, the development of the animal world: it all started not with nerves, but with the fact that there was some kind of plasma in which certain substances circulated.
I sense echoes of an old interdisciplinary debate here...
No no. The nervous system, of course, is also important. We just talked a lot today, for example, about fertility, about sexual function. This is not a simple muscle contraction, it is a complex process extended over time, which is regulated precisely by the relationship of hormones. There's no way a nerve can run from the brain to the testicle and promote sperm production, you know? That would be too cool. And the hypothalamus is precisely responsible for the integrative interaction of nervous influences.
How does the male endocrine system respond to physical activity and the fuel with which these activities are artificially fueled? I'm talking about sports nutrition.
If you are already over 30, then you probably go to the gym for health, and not in order to turn yourself into a cabinet of muscles and seduce girls. At 18 years old, you can, of course, think that a woman needs your muscle mass, but in principle this is absolute stupidity and in 99% of cases it will not work. If you set yourself the task of seducing as many women as possible, you need to spend more effort on developing your brain. And in the gym - think about blood vessels, muscles and some kind of harmony. Now to the question of sports nutrition and energy drinks. I have a very negative attitude towards them. I don’t want to scare anyone, but I had to witness fatal myocardial dystrophy while taking a large number of energy drinks. As for hormones and, in particular, testosterone, unfortunately, I’m afraid that you and I will no longer be able to break the stereotypes that have developed in these gyms. We cannot explain that dabbling with testosterone will lead to the fact that by the time such a guy meets his one and only, he will have nothing left of his spermatogenic epithelium. I myself visit a fitness club and often find myself witnessing conversations between young people on, let’s say, medical topics. What I hear is not just wild - I don’t even have enough words to describe it: “Now I’m on androgens, then I dry out, then I add triiodothyronine...” It should be noted that most often people talk about these topics with, let’s say, not very high intellectual bar.
What does he add?
Triiodothyronine is a thyroid hormone. And then, with the appearance of an absolute expert, but with errors in basic concepts, such a person begins to give recommendations to another person. At the same time, we are talking about very serious hormonal drugs... A real panopticon, and with a health risk. As for consuming large amounts of proteins, this is first of all non-physiological; it puts a lot of stress on the kidneys. I have a lot of patients who are former serious athletes and those who served in special forces. During their physical activity, taking some medications and special nutrition is not entertainment, not a way to seduce a girl, but part of the hardest work with hyperstress. So, as a rule, these people have a whole bunch of endocrine and cardiovascular diseases. With age, many of them acquire obesity, hypertension, and diabetes.
Please tell us about anti-aging endocrinology, about age-related hormone therapy, which is fashionable today.
Due to the development in recent years of the anti-aging industry, most professional endocrinological associations have been forced to publish regulatory documents on hormone therapy: clinical recommendations for the treatment of hypothyroidism, hypogonadism, and growth hormone deficiency. Our professional position is clear: hormone therapy is indicated only and exclusively in situations of hormone deficiency. But there is a powerful anti-aging lobby, non-professional paramedical and other marginal associations. I attended their conferences: from the point of view of professional endocrinologist clinicians, what happens there sometimes looks outlandish. Self-indulgence in our sphere, as in any other sphere, ends badly. Growth hormone, for example, which is used for rejuvenation, is a growth factor; cells multiply from it, which means we can easily grow a tumor for ourselves. The danger is that the anti-aging industry is in an uncontrolled field: they do not need statistics, they do not need prospective studies, they live outside of medical ideology.
That is, starting to rejuvenate with the help of hormone therapy is, in general, a serious risk.
You need to rejuvenate when you are young. Our regulatory system is too complex for the introduction of one or another element into it to trigger any processes in the opposite direction. Today we have listed the classical hormones, but in addition to them there are about two hundred more, and they all participate in the functioning of the body. “Hormon,” by the way, does not come from the word “harmony,” as many people think, but from the word hormao — “put into action.” And all these actions should be, let’s say, proportional to each other. I repeat: the hormone acts on many structures at once, it enters the systemic bloodstream and reaches all cells. We have identified one of its functions, but there are a dozen more that we do not know about. For example, a nerve has one function - innervation of muscles, and a hormone is something more complex. Periodically, one of its effects pops up, and it begins: “This is the hormone of so-and-so.” Almost every hormone was at one time called the hormone of youth. There are episodes of their popularity: sometimes testosterone is popular in our country, sometimes prolactin, sometimes thyroxine. Then suddenly dehydroepiandrosterone is declared the hormone of youth - this is an androgen of the adrenal glands: at one time in the USA it could be bought at any pharmacy without any prescription.
In general, what should a young man do to preserve his endocrine system?
To begin with, surprisingly, remember a simple thing: salt must contain iodine. When your wife or girlfriend goes to the store, ask her not to waste money on various Japanese and Himalayan frills, but to buy our domestic salt, where it says “iodized” on the pack. Its effectiveness has been absolutely proven - it solves the problem of iodine deficiency, prevents the development of goiter and brings many other benefits. This is even more important for women, but men also need to ensure that they get enough iodine into their bodies. This is relative to the thyroid gland. As for diabetes mellitus, it is clear that the disease is associated with a hereditary predisposition, but we must remember its direct connection with excess weight: the stomach not only interferes with tying shoelaces, but also affects our general condition and cardiovascular system. Next is sexual function. A man is given spermatogenic epithelium, one for life, and he must take care of it. The quality of sperm at 20 years old and at 60 differs greatly: it reflects everything that befalls us - from the head and nerves to the environment, not to mention any intoxication, especially chronic ones. So, as you can see, I cannot recommend anything that goes beyond the concept of a healthy lifestyle, although this term smacks of something archaic. Physical activity is needed, and it is highly desirable - without the use of various stimulants. When you're twenty, it seems like you can cram any crap into yourself. But a dozen or two years pass, and we understand that life is not endless. And here the results of all our youthful experiments fall upon us... Do your humble servant know how much he studied before he began to introduce something into the patients’ bodies? To prescribe the hormone, I completed six years of university, two years of residency, graduate school, defended several dissertations, and believe me, I am still checking, rechecking and weighing everything. I never prescribe hormones at the patient’s first visit; I suggest that patients be examined over time and only then do I make a decision. And when boys in fitness clubs start playing around with hormones, it’s crazy. In my opinion, a certain inferiority is manifested here, male complexes, which they try to compensate for by pumping up muscles. So in this sense, I would recommend starting with thinking about what's going on in your head, not what's going on with your testosterone.
Publication link: MensHealth
Sustanon course[edit | edit code]
- The Sustanon course is recommended only for men to gain muscle mass, without any contraindications to the use of anabolic steroids.
- The Sustanon course lasts up to 10 weeks. For longer durations, administration of gonadotropin is required.
- Injections of the drug are performed once a week at a dose of 250-500 mg intramuscularly (it is advisable to inject Sustanon into the gluteal muscles).
- From the second week of the course, start taking aromatase inhibitors under the supervision of estrogen tests (usually using Anastrozole 0.5 mg every other day). Stop taking AIs 1 to 2 weeks after your last injection.
- 3 weeks after the last injection, post-cycle therapy with tamoxifen begins, testosterone boosters are taken for 3-4 weeks to restore the production of your own testosterone.
- For maximum effectiveness of the course, take a sports nutrition complex to gain muscle mass and follow a diet to gain muscle mass.
- Be sure to consult with a specialist before starting to take Sustanon.
Combined courses
Sustanon can be combined with drugs such as:
Nandrolone - for gaining muscle mass. Winstrol - for drying and relief.
Combination allows you to reduce the frequency of side effects and improve the effectiveness of the course. Read more: Combined courses of steroids
Sustanon-250 solution for injection, oil. 1ml amp 1 piece
Pharmacological group:
Androgen.
ATX code: G03BA03 Pharmacodynamics:
Testosterone is the main endogenous hormone indispensable for the normal growth and development of male genital organs and male secondary sexual characteristics. Throughout life in adult men, testosterone is essential for the functioning of the testicles and related structures, as well as for the maintenance of libido, well-being, erectile potency and the function of the prostate and seminal vesicles.
Treatment of hypogonadal men with Sustanon®-250 leads to a clinically significant increase in plasma concentrations of testosterone, dihydrotestosterone, estradiol and androstenedione, as well as a decrease in the level of SHBG (sex hormone binding globulin); Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels are restored to normal levels. Treatment with Sustanon®-250 leads to a decrease in the symptoms of testosterone deficiency. In addition, bone mineral density and muscle mass increase; in obese patients, body weight decreases. During the treatment process, sexual functions are normalized, including erectile function and libido. When using the drug, serum concentrations of HDL (high-density lipoprotein), LDL (low-density lipoprotein) and triglycerides decrease, hemoglobin concentrations and hematocrit increase, while there is no clinically significant change in the level of liver enzymes and PSA (prostate-specific antigen). The drug may cause an increase in the size of the prostate gland, but no functional changes are observed. In hypogonadal men with diabetes, the use of androgens improves insulin sensitivity and/or reduces plasma glucose concentrations.
In boys with delayed growth and puberty, the use of androgens accelerates growth and stimulates the development of secondary sexual characteristics.
Treatment of transsexual women with androgens, like the drug Sustanon®-250, promotes masculinization.
Pharmacokinetics:
Sustanon®-250 contains a number of testosterone esters with varying durations of action. These esters, once in the circulating blood, are immediately hydrolyzed into the natural hormone testosterone.
A single dose of Sustanon®-250 leads to an increase in total testosterone in plasma, the maximum concentration of which reaches approximately 70 nmol/l (Cmax) and is observed approximately 24-48 hours (tmax) after administration. In men, testosterone levels return to the lower limit of normal after approximately 21 days.
Distribution In vitro tests show a high degree of nonspecific binding to plasma proteins of testosterone (more than 97%) and to SHBG (see abbreviation above).
Metabolism Testosterone is naturally metabolized to dihydrotestosterone and estriol.
Excretion Excreted mainly in urine in the form of etiocholanolone and androsterone conjugates.