general characteristics
Erythropoietin is a glycoprotein hormone that causes an increase in the production of red blood cells. In an adult, it is formed mainly in the kidneys, and in the embryonic period, almost completely - in the fetal liver. Erythropoietin is involved in the body's physiological response to anemia and hypoxia. Decreasing the available oxygen in the blood reaching the kidneys increases the production of erythropoietin and increases the rate of formation and differentiation of erythroid cells in the bone marrow. If hypoxia is compensated, erythropoietin levels are usually within normal limits. Chronic obstructive pulmonary diseases, sleep apnea, hemoglobinopathies with increased hemoglobin affinity for oxygen, leading to tissue hypoxia, as well as local renal hypoxia due to renal artery stenosis lead to secondary polycythemia associated with increased erythropoietin levels. In primary polycythemia, associated with uncontrolled erythropoietin-independent production of erythroid cells from stem cells, the level of erythropoietin in the blood is not increased. In case of kidney pathology leading to impaired formation of erythropoietin, a decrease in its level is the main factor in the development of anemia, in case of chronic renal failure, which can be corrected by the administration of erythropoietin. In some cases of kidney pathology (with cystic and tumor lesions), excess production of erythropoietin may be observed, which leads to secondary polycythemia. Reduced levels of erythropoietin are detected in anemia of chronic diseases, chronic infections, autoimmune diseases, rheumatoid arthritis, cancer, and may also be associated with the action of proinflammatory cytokines that inhibit the production of erythropoietin. The correspondence of the actual development of the body to the periods of prepuberty/puberty/postpuberty is determined only by a doctor
What is erythropoietin?
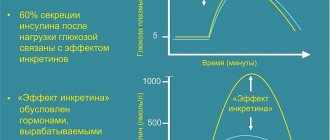
Erythropoietin is a hormone that helps the body maintain optimal oxygen levels. To do this, it stimulates the production of red blood cells or red blood cells.
Red blood cells provide our tissues with oxygen and remove carbon dioxide. When oxygen levels drop, erythropoietin helps replace the loss by increasing the production of red blood cells and hemoglobin. Here's how it happens:
The kidneys have specialized cells that can detect when oxygen levels in the blood are low. If this is the case, the kidneys produce more erythropoietin. The hormone triggers the maturation of hematopoietic stem cells in the bone marrow. These are the precursors of red blood cells, which with the help of erythropoietin turn into full-fledged cells.
Interpretation:
- Anemia, including aplastic; secondary polycythemia (eg, hypoxia at high altitudes, chronic obstructive pulmonary disease, pulmonary fibrosis); erythropoietin-secreting tumors (for example, cerebellar hemangioblastomas, pheochromocytoma, renal tumors); pregnancy; polycystic kidney disease; kidney transplant rejection; moderate bleeding in a healthy person.
- Kidney failure; primary (true) polycythemia; anemia of chronic inflammatory, infectious, oncological diseases.
Sample result (PDF)
Why is erythropoietin deficiency dangerous?
If erythropoietin production is reduced or impaired, blood oxygen levels remain low or will fall further. This is dangerous because it leads to several pathologies, including anemia and hypoxia. When they occur, the body's tissues receive insufficient oxygen and cannot function normally.
Symptoms of anemia:
- fatigue
- dizziness
- dyspnea
- weakness
- headache
- pale skin
- cardiopalmus
A lack of erythropoietin also reduces the body's ability to adapt to changes in altitude and intense physical activity.
Diseases such as AIDS, inflammatory diseases and some types of cancer can lead to low levels of erythropoietin. Lack of oxygen can aggravate these and other chronic diseases.
Mild cases of anemia may not require any treatment, especially if there are no symptoms. However, in more severe cases, iron supplements or erythropoietin-stimulating drugs may be needed. Erythropoietin therapy has been shown to be an effective treatment for anemia in patients with chronic kidney disease, as well as in patients suffering from cancer, HIV, and organ transplants.
Journal "Internal Medicine" 4(10) 2008
Red blood cell transfusion has long been the mainstay of treatment for patients suffering from anemia [34]. However, the shortage of donors and the risk associated with allogeneic blood transfusions (infection with hepatitis B and C viruses, HIV, the risk of allergic reactions, hemosiderosis of organs) required the search for new treatments, one of which was recombinant human erythropoietin (rhEPO).
Erythropoietin (EPO) is a colony-stimulating factor (CSF) that occupies a central position in the regulation of erythropoiesis. It is a glycoprotein cytokine with a molecular weight of 30–34 kDa. Initially, the EPO molecule consists of 193 amino acids, then during metabolism, 27 amino acids and a terminal arginine are removed from the main sequence, and a glycoprotein containing 165 amino acids is secreted into the plasma. The gene regulating the formation of EPO in humans is localized on chromosome 7 in the region 11q–12q [4].
Despite the fact that the bulk of cytokines are hormone-like substances, EPO in its biological action corresponds to true hormones: it is produced mainly in the kidneys (in the peritubular interstitial cells of the cortex) and partially in the liver (10-15%) and has a stimulating effect on bone brain, that is, it acts remotely, unlike other cytokines.
The main function of EPO is to control the proliferation and differentiation of erythroid progenitor cells. At the early stages of development of erythroid cells, starting from pluripotent stem cells, many growth factors (interleukins-3, -6, -11, granulocyte-macrophage colony-stimulating factor (GM-CSF)) are involved in the regulation of erythropoiesis, but for their final differentiation into morphologically recognizable cells - precursors require the additional presence of EPO. It has the most pronounced effect on erythroid colony-forming units and, to a lesser extent, on proerythroblasts, basophilic erythroblasts and normoblasts. EPO has no effect on mature red blood cells, since they do not contain receptors for it [3, 7].
Another important feature of this cytokine is the ability to prevent apoptosis of erythroid progenitor cells at later stages of development by inhibiting their phagocytosis by macrophages.
Lack of endogenous EPO production leads to a sharp decrease in the level of hemoglobin (Hb) and red blood cells in the blood, that is, to the development of so-called erythropoietin deficiency anemia. Until recently, drug correction of such anemia remained impossible due to the lack of an appropriate drug. The difficulties in its creation were due to the fact that EPO is found in the body in very small concentrations, and conventional methods for isolating it from animal tissues are extremely complex and expensive. However, in recent decades, thanks to the development of genetic engineering, it has become possible to produce a highly purified synthetic EPO preparation, rhEPO, which has two main forms: rhEPO-alpha and rhEPO-beta. Both isoforms consist of 165 amino acids, have the same molecular weight and biological activity (100,000 IU per 1 kg of protein). The difference lies in the varying degrees of glycolysis of their molecules. Recently, another form of the drug has appeared - darbepoetin (darbEPO). DarbEPO contains more N-linked carbohydrate chains than plain rhEPO (making it a more stable compound) and has a 3-fold longer half-life [27].
Since 1987, rhEPO has been used as an effective and safe drug for the treatment of nephrogenic anemia in predialysis and dialyzed patients. Currently, the indications for its use 1 have expanded significantly: it has become an alternative to blood transfusions not only in nephrology, but also in oncohematology, surgery, pediatrics and obstetrics for the treatment and prevention of a number of anemias with insufficient production of endogenous EPO.
RhEPO therapy for chronic kidney diseases. Currently, more than 300,000 hemodialysis patients worldwide are treated with rhEPO. The use of this drug for the correction of anemia in chronic renal failure (CRF) is the gold standard.
On average, in 25% of patients with chronic renal failure, anemia is detected even before the development of azotemia. Subsequently, its frequency steadily increases, and when the blood creatinine level is above 0.45 mmol/l, a decrease in Hb level is detected in all patients [7]. It is believed [55] that the main factor in the pathogenesis of anemia in chronic kidney disease is the relative or absolute deficiency of EPO, caused by a decrease in its production by the kidneys and excessive excretion in the urine (with proteinuria), leading to ineffective erythropoiesis. Other factors of such anemia include hemolysis, iron deficiency, increased plasma volume, blood loss, hyperparathyroidism, aluminum intoxication (with hemodialysis), and infections [16].
Numerous studies [6, 17, 36, 46] have shown that the use of rhEPO in patients with chronic renal failure can increase the level of Hb and red blood cells, eliminate transfusion dependence and thereby prevent sensitization to the HLA system and hemosiderosis of internal organs. Thus, in a group of 18 patients with end-stage chronic renal failure [6], changes in blood parameters (Hb, hematocrit, erythrocytes and reticulocytes) were assessed during rhEPO therapy at a dose of 2000 IU 3 times a week. During rhEPO treatment, a gradual increase in the number of reticulocytes was observed: on the 12th day - from 0.2-0.5 to 1.9-2.4%, on the 18th - to 2.0-5.6%. A trend towards an increase in Hb and erythrocytes emerged by the 20th day: the level of Hb increased from 66–83 to 72–83 g/l, erythrocytes - from 2.3–2.8 to 2.5–3.05 T/l. On the 29th day, it was possible to achieve the target Hb level (100 g/l) in 92.6% of patients.
In another study [21], patients on chronic ambulatory peritoneal dialysis received rhEPO subcutaneously twice a week for 12 months. Results showed that at an average weekly dose of 105 IU/kg, the target Hb level (100–120 g/L) was achieved after an average of 11.7 weeks of therapy.
Correction of anemia leads to a significant improvement in the quality of life of dialyzed patients: normalization of appetite, sleep, mood, sexual function and menstrual cycle, increased tolerance to cold and physical activity, and reduction of fatigue [57]. One of the significant positive effects of rhEPO therapy in patients with chronic renal failure is the improvement of cognitive functions of the brain, which is recorded by psychometric tests. A possible mechanism for this effect is an increase in blood Hb concentration, which leads to improved cerebral oxygenation. In addition, as a result of an increase in hematocrit under the influence of rhEPO, cerebral blood flow, increased in dialyzed patients, is normalized, which is accompanied by a decrease in the flow of uremic toxins into the brain and a decrease in intracranial pressure [7].
RhEPO preparations in patients with chronic renal failure are used not only to normalize Hb levels, but also to correct the so-called oxidative stress, the severity of which closely correlates with the severity of anemia [46]. Studies on the treatment of nephrogenic anemia with rhEPO have demonstrated a decrease in the level of lipid peroxidation products in the blood of such patients. By reducing hypoxia and oxidative stress, rhEPO prevents the development of interstitial fibrosis and destruction of renal tubules. In addition, it has a direct protective effect on tubular cells, reducing apoptosis, and also ensures the integrity of the capillary network by affecting the endothelium [46]. Therefore, the use of erythropoiesis-stimulating drugs in patients with kidney disease may slow the progression of chronic renal failure.
Interestingly, rhEPO not only corrects anemia of renal origin, but also modulates platelet function and eliminates platelet serotonin deficiency caused by uremia. Studies have shown [35] that stimulation of erythropoiesis is accompanied by an increase in the number of platelets, an increase in their aggregation ability, a reduction in bleeding time and replenishment of intraplatelet serotonin depots. Thus, by improving hemostasis, rhEPO therapy can reduce the risk of bleeding in dialyzed patients.
RhEPO in oncology and hematology. Anemia due to a decrease in endogenous EPO production occurs both in solid tumors of various localizations and in hematological malignancies, and can be caused by the effects of the disease itself and/or concomitant radiation therapy (RT) or chemotherapy (CT) [37, 38]. Regardless of the cause of anemia, a decrease in the amount of Hb significantly worsens the quality of life of hematological oncology patients and is an unfavorable prognostic sign.
This problem is relevant not only because anemia requires systematic blood transfusions and causes debilitating symptoms such as fatigue and decreased exercise tolerance, but it itself can cause resistance to radiation therapy. Currently, hypoxia is recognized as the main reason for tumor resistance to radiation therapy. Anemia increases hypoxia of tumor tissue and has a negative prognostic value regarding the effectiveness of treatment of malignant neoplasms [41].
Platinum drugs, such as cisplatin and carboplatin, have the most pronounced and long-lasting effect of inhibiting hematopoiesis. These compounds selectively suppress EPO production in the kidneys by reducing the sensitivity of peritubular fibroblasts to hypoxia [6].
According to the results of large studies [19, 22, 31, 33], the use of rhEPO for the treatment of anemia in cancer patients leads to a significant increase in Hb levels, a reduction in the number of allogeneic blood transfusions and an improvement in the quality of life of patients, and can increase the effectiveness of RT and chemotherapy. All studies have demonstrated the presence of a hematopoietic response (achieved Hb level > 120 or an increase in Hb by 20 g/l or more) in more than 60% of treated patients.
It has been established that the degree of hematopoietic response to rhEPO varies widely and depends both on the histological type of tumor and the chemotherapy regimen that the patient receives, as well as on the dose, frequency, route of administration and duration of rhEPO therapy. There is a clear dose-dependent effect of rhEPO. Thus, in 2 studies in which rhEPO was administered at doses of 25-100 IU/kg or 200-300 IU/kg 5 times a week, the response rate was 24 and 85%, respectively, at a dosage of 3000 or 6000 IU 3 times a week - 58 and 79%, respectively [2]. Similar results were obtained in other studies [31].
When studying the pharmacodynamics of rhEPO in a randomized placebo-controlled trial in patients with end-stage hemoblastosis [58], it was noted that at the initial stages of therapy, an increase in the level of Hb and red blood cells is not associated with the administration of rhEPO, but is probably due to blood transfusions. However, already in the early stages of rhEPO therapy, patients experience activation of erythropoiesis, as evidenced by an increase in the concentration of serum EPO (5 times compared to placebo) and an increase in the number of reticulocytes. The erythropoietic response to rhEPO increases markedly from the 2nd–3rd month of drug administration, since activation of the erythroid lineage occurs gradually and reaches a maximum after several weeks of treatment [22, 38].
It is interesting [45] that in patients with chemotherapy-induced anemia there is a direct correlation between the early response to rhEPO (an increase in Hb level by 10 or more g/l in the first 4 weeks of therapy) and its persistence in the future. Patients with an early response showed a durable therapeutic effect: Hb levels were maintained in the range of 110–130 g/l for a longer time (10.1 ± 5.05 weeks) compared with the group where there was no early response.
It has been established [6] that the survival rate of patients who experience a significant increase in Hb levels in response to therapy is significantly higher than that of patients who do not respond to rhEPO administration.
The greatest effectiveness of rhEPO was observed in patients with solid tumors, non-Hodgkin's lymphomas and multiple myeloma, and the lowest in patients with myelodysplastic syndrome (MDS) [22, 25, 38, 43]. In groups of patients with MDS, the best results were obtained with refractory anemia (21.8%) and refractory anemia with an excess of blasts in the transformation stage (22.7%), a less pronounced response to rhEPO is observed with refractory anemia with ring-shaped sideroblasts [2]. In a study by M. Razzano et al. [43] indicate that the initial level of endogenous EPO in patients with MDS is an important factor in predicting the effectiveness of rhEPO therapy: its low concentration in the blood serum (less than 100 mIU/ml) determines a pronounced response to exogenous EPO. Factors such as a normal karyotype and female gender also have a positive prognostic value. There is evidence [37] that the use of rhEPO in combination with GM-CSF can reduce apoptosis of blood cell precursors in the bone marrow and significantly improve the results of treating anemia in MDS. This synergism between rhEPO and GM-CSF is already used in clinical practice, in particular for refractory anemia with ring-shaped sideroblasts.
The effectiveness of rhEPO preparations has been proven in people of various age groups, including geriatric patients and children. Data from randomized trials [9] indicate that when conducting rEPO therapy, there are no significant differences in the effectiveness of treating anemia in elderly patients (≥ 65 years) and younger individuals. During treatment of rhEPO anemia in 3634 geriatric and 3467 younger patients over 16 weeks, there was a significant increase in Hb levels by an average of 20 g/L in patients over 65 years of age and 19 g/L in those under 65 years of age, as well as a reduction in Hb requirements. in blood transfusions and a significant improvement in quality of life. Overall hematopoietic response was 65.4 and 64.7%, respectively. The use of once-weekly and once-every-two-week regimens in patients over 65 years of age showed similar clinical results.
The use of rhEPO is also possible for the treatment of anemia in children with cancer. B. I. Razzouk et al. [44] observed a significant increase in Hb levels, a decrease in the need for blood transfusions and an improvement in quality of life in response to intravenous rhEPO at a dose of 600–900 units/kg for 16 weeks in cancer patients aged 5 to 18 years receiving chemotherapy. However, rhEPO was well tolerated by children and was safe.
The most commonly used dosing regimen for rhEPO in patients with malignancy is its weekly dose of 40,000 units. However, Steensma et al. [54] demonstrated in their study that after administration of rhEPO at an initial dose of 40,000 units. Once a week three times you can switch to the 120,000 unit regime. every 3 weeks. Moreover, the effectiveness of therapy is comparable to the weekly regimen.
Much attention is paid to the issue of timely initiation of rhEPO therapy. A recent meta-analysis of 5 randomized, placebo-controlled trials found that patients who were pre-transfused were two times more likely to subsequently require repeat transfusions during rhEPO therapy. Similar results were obtained in another integrated analysis of 3 Canadian studies with a total of 665 patients receiving rhEPO for anemia. It was shown that the initial Hb level and preliminary blood transfusions were the main predictors of subsequent red blood cell transfusions. In this regard, it is recommended to start rhEPO therapy as early as possible, which can significantly reduce the volume of blood transfusions in patients receiving chemotherapy [42].
Cardioprotective effects of rhEPO . It is known [18, 27] that anemia, which is an important sign of chronic renal failure, is closely correlated with a higher incidence of cardiovascular diseases and mortality from cardiovascular complications. Although the mechanisms linking anemia, chronic kidney disease, and heart failure (HF) are not fully understood, anemia has been reported to be more prevalent among patients with advanced cardiovascular disease and is associated with higher mortality. Some clinicians [18] combine these three conditions into the so-called cardiorenal anemic syndrome. The nature of anemia in it is multifactorial: concomitant chronic renal failure, heart failure-induced ischemia of the red bone marrow, leading to excessive collagen deposition and impaired erythropoiesis, as well as the inhibitory effect of cytokines, in particular tumor necrosis factor alpha, on the production of EPO, the absorption of iron in the intestine and its exit from the depot [1].
Regardless of the causes, prolonged anemia leads to myocardial ischemia, peripheral vasodilation (due to hypoxia-induced increase in nitric oxide activity), increased venous return and cardiac output, chamber dilatation, hypertrophy and hyperfunction of the heart, especially the left ventricle (LV) [8].
In numerous studies [39, 51, 52], correction of anemia with rhEPO combined with oral or intravenous iron has demonstrated improvements in cardiac function, renal function, and overall quality of life. Thus, in one of the randomized studies [52], the administration of rhEPO to patients with congestive HF functional class III–IV, systolic dysfunction and anemia (Hb level 100–115 g/l) led to a significant decrease in HF functional class and the need for diuretics, and an increase in ejection fraction LV, as well as a significant reduction in the number of hospitalizations. Similar data were obtained in other similar studies [12, 51].
In addition, it has been shown [5, 32, 50] that rhEPO not only has a stimulating effect on erythropoiesis, but also prevents LV hypertrophy in patients with predialysis chronic renal failure, and in patients with severe LV dilation leads to a decrease in its mass and size. As Hb levels increase during rhEPO therapy, hyperdynamia and LV myocardial mass decrease [5]. In the randomized multicenter trial CREATE, the purpose of which was to evaluate the effect of early correction of anemia in patients with chronic renal failure on the functional state of the LV myocardium and cardiac complications, it was shown that the use of rhEPO led to a significant decrease in the rate of development of LV hypertrophy and a decrease in cardiovascular mortality [24].
Currently, evidence has been obtained that rhEPO has not only an indirect (by eliminating anemia), but also a direct cardioprotective effect [26]. There is evidence [53] that rhEPO has a number of potentially beneficial effects not only on the myocardium, but also on the vascular endothelium, reducing apoptosis, increasing mitogenetic activity and stimulating angiogenesis.
It has been shown [18] that patients with chronic kidney diseases complicated by HF have low cell resistance to pro-oxidant factors. The resulting oxidative stress and apoptosis play an important role not only in the progression of renal dysfunction, but also in the induction of myocardial damage. Studies have established [29] that the use of rhEPO in the treatment of cardiovascular diseases in chronic renal failure reduces oxidative stress and the severity of apoptosis. These effects of rhEPO are realized using the enzyme heme oxygenase-1, which has powerful antioxidant and anti-apoptotic properties.
In addition, recent studies [29] have demonstrated a striking improvement in the prognosis of patients with acute coronary syndrome (ACS) when included in rhEPO therapy. Receptors for EPO are present in many tissues of the body, including the cardiovascular system. Experiments in the ischemia-reperfusion model [47, 51] demonstrated that rhEPO has a pronounced direct cardioprotective and angiogenic effect, reducing apoptosis of cardiomyocytes and endothelial cells, improving their function and stimulating angiogenesis in the myocardium. The use of rhEPO in ACS helps to limit the area of necrosis, restore the mechanical function of the myocardium and significantly improve the prognosis [29]. In one study [40], pretreatment of myoblasts isolated from rat hearts with rhEPO reduced their apoptosis by 50% and protected them from ischemic damage (at least during 12 h of anoxia). Administration of erythropoietin to experimental animals before inducing myocardial infarction led to a significant decrease in the volume of cardiac muscle necrosis.
Thus, the creation of rhEPO with selective anti-apoptotic properties may become a promising direction in the treatment of heart failure and coronary heart disease.
RhEPO for other pathologies. It is known [49] that the use of combined antiviral therapy with piggylated interferon and ribavirin in patients infected with the hepatitis C virus can cause the development of anemia due to bone marrow suppression and hemolysis. Studies have shown [56] that rhEPO therapy is effective in correcting anemia, improving the quality of life of such patients and allows maintaining adequate dosages of interferon and ribavirin.
There is evidence that the use of rhEPO has a significant, albeit transient, effect on the function of the endocrine glands. Thus, during a 4-month therapy with rhEPO at a dose of 5000 IU 2 times a week in 22 women suffering from rheumatoid arthritis with concomitant anemia and normal renal function, a significant increase in the levels of insulin and atrial natriuretic peptides and a decrease in the concentrations of renin, aldosterone and somatotropin were recorded. A similar effect of rhEPO on the function of the endocrine glands was also detected in patients with chronic renal failure [23].
Darbepoetin. RhEPO, which has been successfully used to treat anemia, requires frequent repeat injections due to its short half-life. DarbEPO does not have this drawback [17, 20].
Clinical trials have shown that darbEPO, like other forms of rhEPO, is effective in correcting anemia in patients with malignancy and dialyzed patients. However, a longer half-life allows it to be administered much less frequently (once every 2 weeks) [20, 28, 48].
However, the results of studies comparing the effectiveness of rhEPO and darbEPO in reducing transfusion dependence were contradictory. Thus, in a multicenter 16-week study [48], the effectiveness of darbEPO and rhEPO in the treatment of chemotherapy-induced anemia in patients with breast cancer was compared. In one group, patients were prescribed darbEPO-alpha at a dose of 200 mg every 2 weeks, in the other - rhEPO-alpha at a dose of 40,000 units. weekly. The results revealed that the average increase in Hb levels was 19 g/L in the darbEPO group and 17 g/L in the rhEPO group, and the levels of hematopoietic response were 88 and 81%, respectively. However, the number of patients who required blood transfusion during therapy differed significantly: in the rhEPO group it was 16% of patients, and in the Darb group it was only 6%.
In another study, AS Case and RP Rocconi [19] examined the need for blood transfusions in gynecological patients with chemotherapy-induced anemia when darbEPO-alpha and rhEPO-alpha were administered in the same dosages. The increase in Hb levels was almost the same (darbEPO - by 25 g/l, rhEPO - by 23 g/l with an initial level of 112 g/l and 113 g/l, respectively). However, there were significant differences in the frequency of blood transfusions: 35% of patients in the group required red blood cell transfusions, while only 19% in the rhEPO group required red blood cell transfusions.
However, in the United States there is a successful program to exchange rhEPO for darbEPO for inpatients undergoing hemodialysis. This has led to less use of erythropoiesis-stimulating drugs and reduced costs to the healthcare system [17].
Resistance to rhEPO. Unfortunately, a certain proportion of patients undergoing rhEPO therapy remain refractory to treatment [37]. RhEPO resistance is defined as the inability to achieve and/or maintain the target Hb level with weekly intravenous (at a dose of 450 IU/kg) or subcutaneous (at a dose of 300 IU/kg) administration of rhEPO for 4–6 months in the presence of adequate iron reserves in the body. [7].
One of the main causes of resistance is functional deficiency of iron, necessary for the formation of Hb and red blood cells [37]. Therefore, patients receiving rhEPO therapy usually require supplemental iron supplementation. Long-term regular intravenous administration of low doses of iron increases the response to rhEPO therapy, minimizes fluctuations in Hb and hematocrit levels, and prevents the re-development of iron deficiency [14]. Thus, additional administration of iron supplements can improve the results of correction of anemia using rhEPO and reduce treatment costs.
In patients with chronic renal failure on dialysis, other causes of low response to rhEPO include uremic pericarditis, vasculitis, indolent abscess paranephritis and other acute and chronic infections. In this case, the systemic inflammatory response caused by exposure to proinflammatory stimuli leads to anorexia and metabolic disorders. This, in turn, leads to the development of hypoalbuminemia, iron sequestration and decreased sensitivity to rhEPO [16].
It should be remembered that one of the causes of rhEPO resistance in dialysis patients, although quite rare, is aluminum intoxication [4, 7]. In this case, anemia may be its first sign, although the specific mechanism of development of this condition is unknown. It has been suggested that aluminum may interfere with the transport of iron bound to transferrin and heme synthesis.
Side effects of rhEPO. The most common complications of rhEPO therapy include pain at subcutaneous injection sites (35.3%) and arterial hypertension (AH) (29%) [10, 11].
The mechanisms underlying the development or progression of hypertension, often observed during rhEPO treatment of nephrogenic anemia, are not fully understood. M. Annuk et al. [11] associate its occurrence and/or progression with the development of endothelial dysfunction induced by rhEPO therapy. Studies have shown that after rhEPO injection, endothelium-dependent vasodilation decreases, which leads to an increase in total peripheral vascular resistance and the development of hypertension, not only in patients with chronic renal failure, but also in healthy people.
Thus, when prescribing rhEPO drugs, regular monitoring of blood pressure is necessary, and patients with chronic renal failure and hypertension require an increase in doses of antihypertensive drugs.
Along with hypertension, thromboembolic complications occupy one of the first places among the side effects of rhEPO therapy [13]. According to 35 randomized studies [15], which included 6769 patients with cancer, rhEPO therapy leads to disruption of the rheological properties of the blood and increases the risk of thrombosis. Therefore, caution must be exercised when using these drugs in combination with thrombogenic chemotherapeutic agents, as well as in cancer patients at high risk of thrombosis and embolism.
Recently, evidence has emerged of the negative effects of rhEPO on the immune system. A study conducted by R. Hannula et al. [30], showed that the drugs
rhEPOs inhibit the functions of cellular immunity in predialysis patients without affecting the humoral component. The negative effect of rhEPO therapy on immunity was a decrease in the absolute number of lymphocytes and their main subclasses, while the level of IgG class and antiviral antibodies remained unchanged. At the same time, suppression of cellular immunity by rhEPO did not correlate with the activity of erythropoiesis.
An extremely rare but severe complication of rhEPO therapy is partial red cell aplasia, caused by an almost complete cessation of red blood cell production as a result of the formation of antibodies to rhEPO [37, 46].
Other undesirable effects may include headache, arthralgia, dizziness, flu-like symptoms, asthenia, nausea, vomiting and diarrhea [7].
To summarize, we note that the scope of clinical application of rhEPO is constantly expanding. The introduction into practice of this highly active and safe drug opens up broad prospects for clinicians in the treatment and prevention of anemia of various origins and makes it possible to alleviate the suffering of many, many patients.
What does excess erythropoietin mean?
Increasing erythropoietin levels causes the bone marrow to produce more red blood cells. Constantly elevated levels of this hormone signal a chronic lack of oxygen in the blood, for example, due to iron deficiency anemia. Also, an increase in erythropoietin levels can be caused by a tumor that secretes the hormone. For example, renal cell carcinoma.
In rare cases, too many red blood cells can cause a condition known as secondary polycythemia. It is associated with a number of serious health risks:
- increased blood viscosity
- less efficient blood supply and oxygen saturation
- high blood pressure in the lungs
- life-threatening blood clots
- stroke
Special instructions for the use of the drug Epovitan™ recombinant human erythropoietin
Before and during treatment with Epovitan, it is necessary to constantly monitor blood pressure levels, using the drug with caution in cases of untreated or insufficiently controlled hypertension (arterial hypertension), in the presence of a history of seizures, epilepsy, and chronic renal failure. Patients at risk of developing thrombosis, with various vascular complications, hematological complications, and with impaired liver function (a decrease in the metabolism of the drug in the liver leads to an acceleration of erythropoiesis) should be under medical supervision. During treatment with the drug during the first 8 weeks of therapy, it is necessary to regularly monitor the platelet count. True erythrocyte aplasia If suspicion of this disease arose after the start of treatment with Epovitan (ineffectiveness of therapy, a monthly decrease in hemoglobin levels by 10–20 g/l, the emergence of an additional need for transfusions), then patients undergo a study of all blood sprouts, establish or exclude typical causes. If the diagnosis of true erythrocyte aplasia is confirmed, treatment with this drug is stopped and treatment methods appropriate to the diagnosis are used. Chronic renal failure In patients with chronic renal failure during treatment with Epovitan, it is necessary to constantly monitor the hemoglobin level at regular intervals until a normal hemoglobin level of 100–120 g/l is achieved with further monitoring; control by the rate of increase in hemoglobin levels per month (10–20 g/l). This control is aimed at preventing the development of hypertension. The effectiveness of treatment with the drug depends on a sufficient level of iron in the body and the absence of deficiency of vitamin B12 and folic acid. When the ferritin level decreases below 100 ng/ml, the dose of iron supplements for adults should be 200-300 mg/day, for children - 100-200 mg/day. In patients with chronic renal failure, it is necessary to regulate dialysis parameters, control the level of electrolytes in the blood serum, and during dialysis - the ratio of an increase in hematocrit level with a corresponding increase in the dose of heparin drugs, since their non-optimal level causes occlusion of the dialysis system. Patients with oncological pathology It is necessary to control the level of hemoglobin (up to 120–130 g/l) and the rate of its growth (increase by 10 g/l for 2 weeks or 20 g/l after 2 weeks), ensuring the optimal level of iron in the body by prescribing iron supplements (200–300 mg/day for adults and 100–200 mg/day for children). Treatment with Epovitan should be started taking into account the possibility of developing thrombotic complications, when comparing the positive effects and the presence of aggravating risk factors. It is necessary to take into account that the appearance of erythropoietin-induced cells after the start of erythropoietin administration in cancer patients is delayed by 2-3 weeks due to the main chemotherapy treatment. This compliance of therapy is especially important for patients requiring transfusion. Treatment of HIV-infected patients requires special monitoring, differential diagnosis in relation to other types of anemia and consideration of probable etiological factors . Adult surgical patients participating in the autologous blood collection program and patients outside of it receiving recombinant human erythropoietin are subject to careful monitoring and examination, taking into account special measures. Before starting treatment, it is necessary to exclude other causes of anemia, take into account the risk of thrombosis, and prescribe appropriate prophylactic antithrombotic therapy. In elderly patients, the high level of complications from the cardiovascular and urinary systems should be taken into account. It is necessary to monitor blood pressure levels and biochemical blood parameters. During pregnancy and lactation Epovitan is used in cases where the effect of therapy for the mother dominates the risk to the fetus. Impact on the ability to drive vehicles and other mechanisms . Epovitan should be used with caution in the initial stages of treatment, taking into account the risk of developing hypertension (arterial hypertension), until the transition to optimal maintenance doses .
What happens if I have too much erythropoietin?
What happens if I have too much erythropoietin?
Excess erythropoietin occurs due to chronic low oxygen levels or due to rare tumors that produce high levels of erythropoietin. This causes a condition known as polycythemia, which is an increased number of red blood cells. For many people, polycythemia does not cause any symptoms. However, there are general and nonspecific symptoms, including weakness, fatigue, headache, itching, joint pain and dizziness.
Is it worth using erythropoietin in sports?
In recent decades, professional athletes have discovered significant benefits from erythropoietin. This hormone significantly increases the absorption of oxygen into tissues, which can increase endurance and performance.
How are athletic achievements and genetics related?
Erythropoietin is part of a group of blood doping products that are prohibited by the Medical Commission of the International Olympic Committee (IOC) and the World Doping Agency. One of the reasons for the ban was the high health risk.
The use of erythropoietin as a doping agent results in abnormally high red blood cell counts. Blood thickening occurs and the risk of serious side effects increases:
- allergic reactions
- blood clots
- flu-like symptoms
- heart attack
- high blood pressure
- pulmonary embolism
- seizures
- stroke
Overdose of Epovitan™ recombinant human erythropoietin, symptoms and treatment
An overdose of the drug does not cause toxic effects. But if the main indicators (hemoglobin, hematocrit) are not adjusted during treatment with recombinant human erythropoietin, then their optimal and maximum permissible values are exceeded. Exceeding the dose of erythropoietin can cause an increase in blood pressure and contribute to the development of hypertensive encephalopathy (in severe cases with convulsions). In the absence of correction for the hematocrit index, polycythemia may develop, to reduce the severity of which phlebotomy is prescribed (to normalize the hematocrit index).
Erythropoetin
Treatment of anemia in patients with chronic renal failure,
P/c or i.v. When administered intravenously, the solution should be administered within 2 minutes; for patients on hemodialysis - through an arteriovenous shunt at the end of the dialysis session. For patients not on hemodialysis, it is preferable to administer the drug subcutaneously to avoid puncture of peripheral veins.
The goal of treatment is to achieve a hematocrit level of 30-35% or eliminate the need for blood transfusion. The weekly increase in hematocrit should not exceed 0.5%. Its level should not exceed 35%. In patients with arterial hypertension, cardiovascular and cerebrovascular diseases, the weekly increase in hematocrit and its target values should be determined individually, depending on the clinical picture. For some patients, the optimal hematocrit is below 30%.
Treatment with Erythropoietin is carried out in 2 stages:
Initial therapy (correction stage). For subcutaneous administration, the initial dose is 20 IU/kg body weight 3 times a week. If the increase in hematocrit is insufficient (less than 0.5% per week), the dose can be increased monthly by 20 IU/kg body weight 3 times a week. The total weekly dose can also be divided into daily administrations in smaller doses or administered in one go.
When administered intravenously, the initial dose is 40 IU/kg body weight 3 times a week. If the hematocrit does not increase sufficiently after a month, the dose can be increased to 80 IU/kg 3 times a week. If there is a need to further increase the dose, it should be increased by 20 IU/kg 3 times a week at monthly intervals. Regardless of the route of administration, the highest dose is no more than 720 IU/kg body weight per week.
Maintenance therapy.
To maintain the hematocrit at 30-35%, the dose should first be reduced by half from the dose in the previous injection. Subsequently, the maintenance dose is selected individually, with an interval of 1-2 weeks. With subcutaneous administration, the weekly dose can be administered once or in 3-7 injections per week.
In children, the dose depends on age (as a rule, the younger the child, the higher doses of epoetin beta he needs). However, since it is not possible to predict individual response, it is advisable to start with the recommended regimen.
Treatment with Erythropoietin is usually lifelong. If necessary, it can be interrupted at any time.
Prevention of anemia in premature newborns.
SC at a dose of 250 IU/kg body weight 3 times a week. Treatment with epoetin beta should begin as early as possible, preferably from the 3rd day of life, and continue for 6 weeks.
Prevention and treatment of anemia in patients with solid tumors.
SC, dividing the weekly dose into 3-7 injections.
For patients with solid tumors receiving platinum chemotherapy, treatment with Erythropoietin is indicated if the hemoglobin level before chemotherapy is not higher than 130 g/l. The initial dose is 450 IU/kg body weight per week. If after 4 weeks the hemoglobin level does not increase sufficiently, the dose should be doubled. The duration of treatment is no more than 3 weeks after the end of chemotherapy.
If during the first cycle of chemotherapy, the hemoglobin level, despite treatment with epoetin beta, decreases by more than 10 g/l, further use of the drug may not be effective.
An increase in hemoglobin by more than 20 g/l per month or to a level above 140 g/l should be avoided. If hemoglobin increases by more than 20 g/l per month, the dose of epoetin beta should be reduced by 50%. If the hemoglobin level exceeds 140 g/l, the drug is discontinued until it decreases to a level of <120 g/l, and then therapy is resumed at half the previous weekly dose.
Treatment of anemia in patients with multiple myeloma, low-grade non-Hodgkin's lymphoma, or chronic lymphocytic leukemia.
Patients with multiple myeloma, low-grade non-Hodgkin's lymphoma, or chronic lymphocytic leukemia usually have a deficiency of endogenous erythropoietin. It is diagnosed by the relationship between the degree of anemia and the insufficient concentration of erythropoietin in the serum.
Relative deficiency of erythropoietin occurs:
| At hemoglobin level, g/l | Serum erythropoietin concentration, IU/ml |
| > 90 <100 | < 100 |
| > 80 < 90 | <180 |
| <80 | <300 |
The above parameters should be determined no earlier than 7 days after the last blood transfusion and the last cycle of cytotoxic chemotherapy.
The drug is administered subcutaneously; The weekly dose can be divided into 3 or 7 injections. The recommended starting dose is 450 IU/kg body weight per week. If after 4 weeks the hemoglobin level increases by at least 10 g/l, treatment is continued at the same dose. If after 4 weeks hemoglobin increases by less than 10 g/l, the dose can be increased to 900 IU/kg body weight per week. If after 8 weeks of treatment the hemoglobin level has not increased by at least 10 r/l, a positive effect is unlikely and the drug should be discontinued.
Clinical studies have shown that in chronic lymphocytic leukemia, the response to epoetin beta therapy occurs 2 weeks later than in patients with multiple myeloma, non-Hodgkin's lymphoma and solid tumors. Treatment should be continued until 4 weeks after the end of chemotherapy.
The highest dose should not exceed 900 IU/kg body weight per week.
If within 4 weeks of treatment the hemoglobin level increases by more than 20 g/l, the dose of Erythropoietin should be reduced by half. If the hemoglobin level exceeds 140 g/l, treatment with the drug should be interrupted until it decreases to <130 g/l, after which therapy is resumed at a dose half the previous weekly dose. Treatment should only be restarted if the most likely cause of the anemia is Erythropoietin deficiency.
Preparing patients for the collection of donor blood for subsequent autohemotransfusion.
IV or SC twice a week for 4 weeks. In cases where the patient's hematocrit (>33%) allows blood sampling, epoetin beta is administered at the end of the procedure. Throughout the course of treatment, the hematocrit should not exceed 48%.
The dose of the drug is determined by the transfusiologist and the surgeon individually, depending on the volume of blood that will be taken from the patient and his erythrocyte reserve. The volume of blood that will be taken from the patient depends on the estimated blood loss, available blood conservation techniques and the general condition of the patient; it must be sufficient to avoid a blood transfusion from another donor. The volume of blood that will be taken from the patient is expressed in units (one unit is equivalent to 180 ml of red blood cells).
The possibility of donation depends mainly on the blood volume of a given patient and the initial hematocrit. Both indicators determine the endogenous erythrocyte reserve, which can be calculated using the following formula:
endogenous erythrocyte reserve = blood volume (ml) x (hematocrit - 33): 100
women: blood volume (ml) = 41 (ml/kg) x body weight (kg) + 1200 (ml)
men: blood volume (ml) = 44 (ml/kg) x body weight (kg) + 1600 (ml) (for body weight >45 kg).
Indications for the use of Erythropoietin and its single dose are determined by nomograms, based on the required volume of donor blood and endogenous erythrocyte reserve.
The highest dose is with intravenous administration no more than 1600 IU/kg body weight per week; with subcutaneous administration - 1200 IU/kg body weight per week.
Erythropoietin[edit | edit code]
Red blood cells.
Scanning microscope Erythropoietin
is a glycoprotein hormone, more precisely a cytokine, the main regulator of erythropoiesis, which stimulates the formation of red blood cells from late progenitor cells and increases the yield of reticulocytes from the bone marrow depending on oxygen consumption. As long as tissue oxygenation is not impaired, the concentration of erythropoietin, as well as the number of circulating red blood cells, remains constant. The production of erythropoietin is regulated at the level of transcription of its gene, and since the only physiological stimulus that increases the number of cells synthesizing erythropoietin is hypoxia, neither the production nor metabolism of erythropoietin depends on its concentration in plasma. In the body of a healthy person there are approximately 2.3 * 10^13 red blood cells, the lifespan of which is on average 120 days. Consequently, the body must constantly renew the pool of red blood cells at a rate of approximately 2.3 cells per second. The erythroid cell differentiation system must be strictly regulated to maintain a constant level of circulating erythrocytes under normal conditions. In addition, this system must be highly sensitive to changes in the amount of oxygen in the body. Currently, a lot of data have been obtained indicating that the key factor that controls the differentiation of erythroid cells is erythropoietin circulating in the blood.
Erythropoietin is an extremely active hormone that exerts its effect in the body in picomolar concentrations. Small fluctuations in its concentration in the blood lead to significant changes in the rate of erythropoiesis, and the normal range of its concentrations ranges from 4 to 26 IU/l. Therefore, until the hemoglobin concentration drops below 105 g/l, the erythropoietin concentration does not go beyond the specified range and it is impossible to detect its increase (unless you know its initial values). Erythrocytosis leads to suppression of erythropoietin production via a negative feedback mechanism. This is due not only to an increase in oxygen delivery to tissues due to an increase in the number of circulating red blood cells, but also to an increase in blood viscosity. For an athlete, this means a decrease in the production of one’s own hormone when exogenous is administered and a violation of the mechanisms regulating the production of red blood cells. Therefore, when using erythropoietin in sports as a doping, an athlete should think about the future fate of red blood cell production in his body.
Doping tests[edit | edit code]
Typically, erythropoietin is detected in urine or blood samples. It is more likely to be detected in blood than in urine. The half-life is 5-9 hours, that is, the probability of detection is significantly reduced after 2-3 days.
Heparin is used as a masking agent[1]. Injection of proteases into the bladder through a catheter is also used.[2]
Physiological role of erythropoietin[edit | edit code]
For a long time, the question of the cells that normally produce erythropoietin remained open. This was primarily due to the lack of direct methods for identifying cells that synthesize the hormone. Cell identification was carried out by indirect methods, including the ability of certain tissue cultures to synthesize the product in vitro. It was believed that the main candidates for the role of EPO-producing cells are glomerular cells, as well as cells of the proximal tubule. Cloning of the erythropoietin gene, as well as the development of in situ hybridization methods, which make it possible to directly identify those cells in which the expression of certain genes occurs, has changed ideas about the nature of the cells that synthesize erythropoietin. Using in situ hybridization, it was shown that the cells in which erythropoietin mRNA is synthesized are not glomerular or tubular. Apparently, the main site of EPO synthesis in the kidneys is interstitial cells or capillary endothelial cells. As already noted, the main factor regulating EPO production is hypoxia. Under hypoxic conditions, the amount of EPO circulating in the plasma increases approximately 1000 times and reaches 5-30 U/ml. Numerous experiments with the isolated kidney have shown that it contains sensors that respond to changes in oxygen concentration.
Back in 1987, J. Schuster and coworkers studied the kinetics of erythropoietin production in response to hypoxia. It was shown that approximately 1 hour after the establishment of hypoxia, the amount of erythropoietin mRNA in the kidney increases, and the mRNA continues to accumulate for 4 hours. When hypoxia is removed, the level of EPO mRNA rapidly decreases. Changes in the amount of plasma and renal erythropoietin, detected using erythropoietin-specific antibodies, occur strictly in parallel with changes in the amount of mRNA with a corresponding lag period. The results obtained in this work indicate that hypoxia stimulates de novo EPO production.
In the laboratory of S. Konry in 1989, the process of induction of EPO synthesis was studied using the method of in situ hybridization on tissue sections of the renal cortex. It was found that under conditions of anemia, EPO production increases significantly, although the intensity of hybridization with EPO mRNA in individual cells remains unchanged. It has been shown that increased EPO production is associated with an increase in the number of cells synthesizing the hormone. As normal hematocrit is restored, the number of erythropoietin-synthesizing cells rapidly decreases, and the kinetics of the change correlates with the kinetics of the decrease in the amount of EPO mRNA and circulating hormone. Histological analysis data indicate that EPO is synthesized by interstitial cells of the renal cortex.
It has been shown that 5 to 15% of plasma erythropoietin in adults is of extrarenal origin. And if in embryos the main place of erythropoietin synthesis is the liver, then in the adult body the liver is also the main organ producing EPO, but extrarenal. This conclusion was confirmed in recent experiments detecting EPO mRNA in various organs. Apparently, a change in the main site of EPO synthesis during ontogenesis is a genetically determined event.
The synthesis of erythropoietin in the body is mediated by a significant number of biochemical cofactors and stimulants. It is assumed that hypoxia leads to a decrease in oxygen levels in specific sensory cells of the kidney, which causes increased production of prostaglandins in glomerular cells. Prostaglandins have been shown to play an important role in stimulating erythropoietin production. Inhibitors of prostaglandin synthesis have a suppressive effect on EPO production during hypoxia. The main contribution to the biosynthesis of prostaglandins during hypoxia appears to be made by the cyclooxygenase system. Hypoxia (as well as the administration of cobalt ions) causes the release of neutral proteases and lysosomal hydrolases in the kidneys, which have also been shown to stimulate EPO production. The release of lysosomal enzymes appears to be associated with an increase in cGMP production. It has been shown that lysosomal enzymes are activated with the participation of protein kinases, which, in turn, are activated by cAMP.
During hypoxia, induction of phospholipase A2 activity is observed, which leads to an increase in the level of arachidonates, which, with the participation of cyclooxygenase, are converted into endoperoxides. It has been noted that hypoxia is the optimal condition for cyclooxygenase activity. The calcium system probably plays an important role in these biochemical events: calcium ions stimulate the activity of phospholipase A and the formation of prostaglandin. Prostanoids, in turn, can induce adenylate cyclase activity and trigger a cascade of biochemical events leading to phosphorylation and activation of hydrolases. What is the role of hydrolases and what is the chain that ultimately leads to increased EPO synthesis remains unclear. Some hormones of the hypothalamic-pituitary system, thyroid hormones and some steroid hormones also have activity that stimulates EPO biosynthesis. A specific inducer of EPO production is cobalt ions, the mechanism of action of which on the EPO biosynthesis system is not yet clear. This system is an attractive experimental model for studying the induction of EPO biosynthesis.
A human erythropoietin molecule, in which the carbohydrate component accounts for 40-50% of the molecular weight (the molecular weight of the glycoprotein is 32-36*10^3 a.m.u., and the calculated molecular weight of the protein part is 18,399*10^3 a.u. e.m.), consists of 193 amino acid residues. The isoelectric point of EPO is low (pH 3.5-4.0), which is due to the presence of sialic acids in the terminal positions of the carbohydrate chains of erythropoietin. Isoelectric focusing of plasma EPO in a polyacryamide gel allows us to identify several fractions that are identical in molecular weight, but differ in the size of their isoelectric points, which indicates heterogeneity in the structure of the carbohydrate part of the hormone. Cleavage of sialic acids by treatment with neuraminidase or by acid hydrolysis leads to loss of hormone stability in vivo, but does not affect its activity in vitro. In four sections, glycosidic residues are attached to the protein chain, which can represent different sugars, so there are several varieties of EPO with the same biological activity, but slightly different in their physicochemical properties.
As a result of analysis of the amino acid sequence of human erythropoietin, three potential N-glycosylation sites were identified, which include the consensus sequence Asn-X-Ser/Thr. In experiments on the treatment of the hormone with N-glycosidase, which specifically cleaves off oligosaccharide chains linked to the aspartic residue by an N-glycosidic bond, the assumption of the presence of three N-glycosylation sites in the EPO molecule was confirmed. As a result of experiments on the treatment of the hormone with O-glycosidase, it was established that it also contains oligosaccharide chains connected to the protein part through O-glycosidic bonds.
The erythropoietin gene (Gene: [07q21/EPO] erythropoietin) consists of five exons and four introns. The gene encodes a protein consisting of 193 amino acid residues. Four types of RNA involved in the interaction with the erythropoietin gene have been identified, and two types are represented in extracts after the introduction of cobalt chloride with a significantly lower copy number than in normal extracts. These data indicate the presence of negative regulatory factors (probably ribonucleoproteins) involved in the regulation of erythropoietin gene expression. The assumption of negative regulation of EPO gene expression was confirmed by Semenza G. and co-workers in 1990, who obtained a series of transgenic mice carrying the coding part of the human EPO gene and various fragments of the S-flanking region. Analysis of gene expression in various transgenes made it possible to identify three regulatory elements of the human erythropoietin gene:
- a positive regulatory element required to induce erythropoietin gene expression in the liver;
- negative regulatory element;
- a regulatory element required for inducible gene expression in the kidney.
It has been experimentally shown that there are two transcription initiation sites of the erythropoietin gene, which carry multiple initiation sites. Under normal conditions, transcription initiation occurs from a limited number of sites located in both regions. When anemia is induced or treated with cobalt chloride, the number of functioning transcription initiation sites in both regions increases. In all cases, the production of erythropoietin is limited by difficulties associated with the isolation and cultivation of cells, the instability of hormone production and, finally, its low concentration in culture fluids.
A fundamentally different approach to obtaining large quantities of highly purified EPO was associated with the use of genetic and cellular engineering methods. An attempt was made to create a bacterial producer of erythropoietin. The protein produced in Escherichia coli is recognized by antibodies against EPO and has a molecular weight approximately corresponding to deglycosylated human EPO. It is known that bacterial cells have a glycosylation system that is fundamentally different from the eukaryotic one. Therefore, it is impossible to obtain correctly glycosylated protein in bacterial cells. In the case of EPO, obtaining a correctly glycosylated glycoprotein is of fundamental importance. Therefore, creating a hormone producer based on bacterial cells is impractical. An effective producer of erythropoietin, biologically active both in vitro and in vivo, can only be obtained from cells of higher animals.
When studying the properties of recombinant EPO, it was shown that the presence of an incomplete carbohydrate component (the molecular weight of erythropoietin synthesized in this system is 23 * 10^3 a.m.u.) does not affect the activity of the hormone in vitro, but significantly reduces its activity in vivo . At the same time, complete cleavage of the carbohydrate part with the help of glycosidases leads to an 80% loss of the biological activity of the hormone in an in vitro test. These data are in conflict with existing ideas that the carbohydrate component of EPO is not strictly necessary for its activity in vitro.
Historical background[edit | edit code]
In 1989, a detailed analysis of the structure of recombinant EPO obtained by transfecting cells from the Chinese hamster ovary into the human EPO genome was carried out. It has been established that two types of EPO (called bi- and tetra-forms) are synthesized in cells, differing in the degree of branching of N-linked carbohydrate chains. The bi-form of EPO, containing a less branched carbohydrate component, differs significantly in biological activity from native erythropoietin, used as a standard: the biological activity of the bi-form of EPO in vivo is 7 times lower, and in vitro - 3 times higher. The biological activity of the tetra form of EPO is very close to that of native EPO. These data indicate an essential role of the structure of the carbohydrate component for the biological activity of erythropoietin in vivo. Apparently, the higher in vitro activity of those forms of erythropoietin that contain an incomplete carbohydrate component is associated with facilitating the interactions of erythropoietin with receptors. At the same time, it appears that it is the carbohydrate component that ensures the stability of the hormone in the body and, accordingly, a high level of biological activity in in vivo tests.
By the mid-1980s, the first recombinant erythropoietin was produced by introducing the human EPO gene (located in humans on the seventh chromosome in the region 11q-12q) into ovarian cells of hamsters. Recombinant human r-EPO, obtained by genetic engineering (Recormon), is identical in amino acid composition to natural human EPO. Recormon provides a flexible and cost-effective method for the effective treatment of anemia combined with a high safety profile and excellent tolerability. Thanks to the use of Recormon, the need for blood transfusions, which today are the most common method of correcting anemia, is significantly reduced. Thus, according to numerous studies, the use of Recormon allows one to restore normal hemoglobin levels and eliminate the need for replacement blood transfusions in cancer patients suffering from anemia. At the same time, there is a significant improvement in the quality of life of these patients; the risk of infection that exists when correcting anemia with the help of blood transfusions during the treatment of viral infectious diseases such as HIV and hepatitis C is significantly reduced. Recormon is available in the form of a convenient device for administering and indicating the drug (syringe pen).
However, there are minor differences in the composition of glycosidic residues, which affect the physicochemical properties of the entire hormone molecule. For example, certain differences have been found in the distribution of electrical charge for certain types of erythropoietin. Erythropoietin preparations are produced by various pharmaceutical companies in five types: alpha, beta, retard (NESP), theta and omega).
Since 1988, alpha-EPO and beta-EPO have been used. When administered subcutaneously, their bioavailability is about 25%, the maximum concentration in the blood is after 12-18 hours, the half-life is up to 24 hours (with intravenous administration - 5-6 hours). Erythropoietin retard (NESP) has been used for the last few years and lasts longer than other EPO drugs. Theta-EPO is considered the most effective and least allergenic today, and has the highest degree of purity. This is due to the fact that it is obtained by genetic engineering in human cells (some unscrupulous athletes and sports doctors believe that this makes it undetectable). In fact, theta EPO is only 99% identical to human. Omega-EPO, which is obtained from hamster kidneys, is the most different from other EPO preparations from human EPO, so it is the easiest to identify. Sold only in Eastern Europe and South America.
Erythropoietin preparations[edit | edit code]
Recombinant biosimilar a-EPO from different manufacturers, even having a positive opinion from the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency, may have different properties, degrees of purity and, most importantly, have different biological activities . When erythropoietin preparations from different manufacturers were analyzed, 5 of the 12 products examined showed significant variations in potency between different batches, and three samples showed unacceptable levels of bacterial endotoxins.
Another study compared 11 EPO products (obtained from eight manufacturers) marketed outside the EU and based on the content, potency and isoform composition of the active substance (erythropoietin). In vitro bioactivity ranged from 71-226%, with 5 samples not meeting specifications. Among the deviations in the isoform composition are the presence of one or more additional acidic and/or basic isoforms, as well as an altered quantitative ratio of various isoforms. Inter-run differences were also identified; Some products did not meet their own specifications, meaning that manufacturers did not provide adequate control over their production processes. The amount of active substance also did not always correspond to the declared quantity. Such deviations from the stated parameters may have important clinical significance, since they may lead to an overdose or, conversely, the administration of a lower dose. The data presented clearly indicate the threat of using recombinant erythropoietins without medical indications.
Application in medicine[edit | edit code]
In medical practice, erythropoietin is used to treat anemia of various origins, including in cancer patients and patients with chronic renal failure. Since, as noted above, the body produces endogenous erythropoietin in the kidneys, patients with chronic renal failure always suffer from anemia. In addition, a decrease in the concentration of EPO in human plasma and, accordingly, in the number of red blood cells, is observed in the following pathological conditions and diseases:
- secondary polycythemia;
- inadequate stimulation of one's own EPO;
- benign kidney diseases (hydronephrosis);
- general tissue hypoxia;
- impaired blood supply to the kidneys
- reduction of oxygen concentration in the environment;
- chronic obstructive pulmonary disease;
- diseases of the cardiovascular system (discharge of blood from right to left);
- abnormalities in the structure of the hemoglobin molecule (sickle cell anemia);
- exposure to carbon oxides on the body due to smoking;
- arteriosclerosis of the renal artery;
- graft rejection;
- aneurysms of the renal vessels.
Before the advent of recombinant erythropoietin, such patients regularly received blood transfusions of both whole blood and red blood cells. However, since 1989, the need for such procedures has disappeared, since they have been replaced by the administration of erythropoietin drugs. In some cases, anemia of other origins is also successfully treated with recombinant EPO. The fact that administration of recombinant EPO induces additional erythropoiesis even with completely intact endogenous EPO levels has been exploited by autologous blood donors. As an alternative to red blood cell transfusion, high-dose EPO therapy appears to be an effective anti-anemic measure as an accompanying therapy in the treatment of chronic polyarthritis, AIDS, some tumors, as well as in a number of surgical interventions. The genesis of hypertension as a side effect during the therapeutic use of recombinant EPO still remains unclear. During hemodialysis patients, erythropoietin preparations are usually administered intravenously. In some cases, the same drug can be administered subcutaneously.
An increase in the number of red blood cells under the influence of erythropoietin, in turn, leads to an increase in the oxygen content per unit volume of blood and, accordingly, to an increase in the oxygen capacity of the blood and the delivery of oxygen to tissues. Ultimately, the body's endurance increases. Similar effects are achieved during training sessions in mid-altitude conditions, when the lack of oxygen in the air causes a state of hypoxia, which stimulates the production of endogenous EPO. Naturally, compared to the use of a recombinant drug, hypoxic training is a physiological mechanism for regulating erythropoiesis and improving the oxygen transport function of hemoglobin, which is actually the purpose of using EPO as a doping.
Due to the effect of erythropoietin on oxygen capacity and oxygen transport in tissues, this substance causes an increase in performance in sports with a predominant manifestation of aerobic endurance. These sports disciplines include all types of athletics running, starting from 800 m, as well as all types of skiing and cycling. In addition, recently information has begun to appear in bodybuilding publications that EPO can replace the widespread use of anabolic steroids. EPO preparations are used in combination with stanazolol, insulin and growth hormone (GH) -
Erythropoietin preparations are well-tolerated pharmacological agents that have virtually no side effects. However, an overdose of EPO and uncontrolled use can lead to an increase in blood viscosity and, consequently, to an increased risk of disorders in the circulatory system, including peripheral vascular thrombosis and pulmonary embolism, which is usually fatal. The risk of these side effects of EPO increases when training in mid-altitude areas, as well as when the body is dehydrated.
However, there is evidence that long-term use of erythropoietin drugs can be dangerous to health, and sometimes even to life. In particular, the use of EPO is associated with constant headaches in athletes, which develop as a result of blood thickening and disruption of its circulation in the brain. In addition, iron metabolism may be disrupted: the body's need for it increases despite the presence of a relatively small reserve in the liver. When exogenous iron is administered, it begins to be deposited in the liver, as a result of which cirrhosis of the liver associated with excess iron appears after 20-25 years.
What affects the production of erythropoietin?
Here's what contributes to decreased oxygen levels in the blood and increased production of erythropoietin:
- high altitude
- hypoxia
- lung diseases
- heart disease
High altitude
At higher altitudes, air pressure is lower, which means there is less oxygen in each breath. The body compensates by increasing the production of erythropoietin and red blood cells to maintain stable oxygen levels in the blood. This response helps combat symptoms of altitude sickness caused by decreased oxygen levels.
☝️When adapting to high altitudes, different people show big differences: some quickly produce more erythropoietin, others much more slowly.
The body's response to high altitude is partly determined by genetics. Populations that have traditionally lived at high altitudes for thousands of years, such as the Himalayan Sherpas, produce more erythropoietin and have, on average, more red blood cells than people living at sea level.
Erythropoietin solution 2000IU/ml 1ml N10 (Alium)
Adverse reactions are listed in accordance with the following gradation: often (>1%,0.1%,0.01%, From the cardiovascular system: in patients with anemia with chronic renal failure, the most common is increased blood pressure (BP) or increased already existing arterial hypertension, especially in the case of a rapid increase in hematocrit. In this case, it is recommended to prescribe drug antihypertensive therapy, if there is no effect, it is recommended to temporarily interrupt therapy with epoetin beta. In some patients (including those with previously normal or low blood pressure), a hypertensive crisis with symptoms of encephalopathy (headaches, confusion, sensory and motor disorders - speech disturbances, gait, even tonic-clonic seizures), requiring emergency medical care and intensive care. Particular attention should be paid to sudden migraine-like pain. In patients with solid Tumors, multiple myeloma, non-Hodgkin's lymphomas or chronic lymphocytic leukemia may rarely cause headaches and increased blood pressure, which can be relieved by prescribing drugs. On the part of the hematopoietic organs: in patients with renal failure and anemia, a dose-dependent increase in the number of platelets (not beyond normal limits and disappearing with continued therapy) may occur, especially after intravenous administration. Thrombocytosis develops very rarely. Due to increased hematocrit, it is often necessary to increase the dose of heparin during hemodialysis. Inadequate heparinization may result in blockage of the dialysis system. Shunt thrombosis may develop, especially in patients with a tendency to hypotension or with complications of an arteriovenous fistula (for example, stenosis, aneurysm, etc.). In such situations, early revision of the shunt and timely prevention of thrombosis (acetylsalicylic acid) are recommended. In most cases, along with an increase in hematocrit, the serum ferritin level decreases. In some cases, in patients with uremia - increased levels of potassium and phosphate in the serum. Some patients with solid tumors, myeloma, non-Hodgkin's lymphoma, or chronic lymphocytic leukemia have decreased serum iron metabolism. Clinical studies have shown that the incidence of thromboembolism in cancer patients treated with Erythropoietin is slightly higher than in the absence of such therapy or when using placebo; however, a clear causal relationship with the drug has not been established. In premature newborns, in most cases there is a decrease in serum ferritin, and there may be a slight increase in the number of platelets, especially at 12-14 days of life. In patients preparing to donate blood for subsequent autotransfusion and receiving epoetin beta, there is an increase in the number of platelets, usually within normal limits, and a higher incidence of thromboembolic complications, although their causal relationship with the use of the drug has not been established. Other: rarely - allergic skin reactions in the form of rash, itching, urticaria or reactions at the injection site. Isolated cases of anaphylactoid reactions have been described. However, in controlled clinical studies, the incidence of hypersensitivity reactions did not increase. In some cases, especially at the beginning of therapy, flu-like symptoms such as fever, chills, headache, pain in the limbs and bones, and malaise were noted. These reactions were mild or moderate and disappeared within a few hours or days.