Today, complications often occur during pregnancy and childbirth. Premature placental abruption is very dangerous for the baby and the mother. This complication occurs, according to statistics, in 0.3 – 1.5 cases out of 100. Most cases are recorded in the first trimester. But basically everything ends well if such a complication appears in the early stages of pregnancy.
- Functions of the placenta
- What is placental abruption?
- Causes of detachment
- Classification
- Symptoms
- Severity of the problem
- Treatment
Placental abruption - what is it?
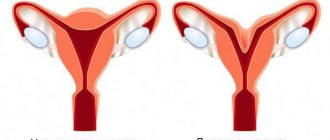
Gynecologists distinguish:
- premature detachment of a normally located placenta (localized on the walls of the uterine body, in its upper parts or at the bottom);
- premature detachment of the placenta located in the area of the uterine pharynx.
Why is the placenta so important?
The process of placenta formation begins in the second week after conception. At this point, the egg is already attached to the uterine wall. Until the 12th week of pregnancy, the placenta is actively growing and forming, after which it reaches a state of maturity.
It is a rather complex structure formed by intertwined vessels of the fetus and mother. Between them there is a hemoplacental barrier - a special protective membrane that prevents the entry of harmful substances from the mother’s body into the fetus’ body, and removes the child’s waste products into the mother’s blood.
The main functions of the placenta include:
- Gas exchange. It is through the placenta that oxygen enters the blood of the fetus. Carbon dioxide is transported in the opposite direction.
- Excretory and nutritious. Through the placenta, the fetus receives nutrients, vitamins and minerals, without which normal development is impossible. Waste products are also excreted through it.
- Protective. The placenta passes the mother's antibodies to the fetus, that is, it has immune properties. It also prevents the occurrence of immune conflict.
- Hormonal. The placenta synthesizes hormones necessary for the normal course of pregnancy: - placental lactogen (prepares the woman’s body to produce milk for prolonged breastfeeding); — human chorionic gonadotropin (supports the functional activity of the placenta, ensures the production of progesterone by the corpus luteum); - prolactin (responsible for milk production); - estrogen (promotes the growth of the uterine lining); - progesterone (prevents new eggs from leaving the ovaries, stimulates the growth of the uterine mucosa); - relaxin, testosterone, serotonin and many other hormones important for the health of a pregnant woman.
Thus, with premature placental abruption, the baby is deprived of oxygen and nutrients. There is also a risk of developing uterine bleeding, which is dangerous to the health of the pregnant woman.
Forms of premature placental abruption
The severity of the symptoms of premature placental abruption depends not only on the area of the separated area, but also on the form of the disease:
- With central abruption, blood accumulates between the placenta and the uterus, and there is no bleeding from the genital tract. The mother's condition deteriorates sharply, her pulse and blood pressure change.
- With marginal detachment, dark red blood is released from the genital tract. The greater the blood loss, the worse the pregnant woman feels.
- In case of detachment with combined bleeding, both external and internal bleeding are diagnosed.
Based on the area of the severed area of the placenta, it is customary to distinguish:
- Complete (total) detachment. Due to the cessation of gas exchange, the child dies and suffocates.
- Partial detachment. This form may have: - a progressive course, when the size of the hematoma increases and the separation of the placenta continues; - non-progressive course, when the vessels of the uterus are thrombosed and the pathological process does not spread further.
It is important to know that a small placental abruption in early pregnancy is safer than a similar-sized abruption in the last trimester. This is explained by the fact that in the first 12 weeks of pregnancy this organ continues to grow and can still compensate for the lost area.
According to the criterion of the size of the detached part of the placenta, in obstetrics there are three degrees of severity of the condition of the mother and fetus:
- mild (up to 20% of the placenta was detached);
- medium (more than 25% of the placenta was detached);
- severe (more than 75% of the entire area of the placenta has been detached).
The meaning and functions of the placenta
The child's place is temporary and is formed during the process of bearing the baby. The placenta is often called the placenta or placenta. When the baby is already born, the processes of detachment of the placenta begin - this is the final stage of delivery. This organ is necessary for continuous communication between the fetus and the maternal body. The baby's place begins to form approximately a couple of weeks after fertilization, and completes formation at approximately 16-18 weeks. It is during this period that the nutrition of the fetus changes from histotrophic to hematotrophic.
During this transition of nutrition, hematoplacental protection is formed, which ensures the performance of placental functions. In general, the functions of this body are reduced to several tasks.
- Nutritious. Maternal blood penetrates into the space between the placental villi and the uterine wall, which contains vitamins and nutritional components and minerals. From there, all these micronutrients penetrate the vascular canals of the placenta, and through them are delivered to the fetal structures.
- Gas exchange. From the mother's bloodstream, oxygen nutrition is supplied to the baby's bloodstream. The gas formed during the baby's breathing penetrates the maternal circulatory system. This is how the placenta performs the fetal respiratory function.
- Hormonal activity. The placenta also performs the work of an endocrine glandular organ, since it produces many hormonal substances that are necessary for the full course of gestation. This includes hCG, which supports placental functions and helps the corpus luteum secrete progesterone. The placenta also produces lactogen, which ensures proper development of the breasts and prepares them for lactation. Also, placental structures contribute to the production of prolactin, estrogens, progesterone, relaxin, serotonin and other hormonal substances important during pregnancy.
- Excretory. During fetal life, metabolites are formed in the form of creatinine, urea or creatine, which are removed through placental structures.
The tissues of the baby's place allow the antibodies of the pregnant woman to pass to the baby, increasing the immune strength of the unformed baby. Usually, the afterbirth prevents the development of immune confrontation between the patient and the fetus. Moreover, the baby’s place regulates and promotes the formation of immune structures in the pregnant woman and the fetus. However, the baby's place will not be able to provide fetal protection from the effects of medications, viral pathogens, alcohol and nicotine components, and drugs.
Why placental abruption occurs - causes of pathology
The causes of premature placental abruption in early and late pregnancy include:
- hypertension (if the pressure remains at 130/90 mm Hg or higher for a long time);
- serious nervous and mental overload,
- mechanical injuries in the uterine area, careless medical manipulations,
- gestosis (edema, high blood pressure, kidney dysfunction),
- chronic diseases of the branches of the vascular bed,
- pathologies of the blood coagulation system (excessive clotting),
- placental insufficiency (uteroplacental blood flow is disrupted at the level of small vessels).
The most common cause of premature placental abruption in later stages is complicated gestosis. During childbirth, the described problem occurs when:
- short umbilical cord of the fetus (a child who has not yet been fully born pulls the placenta with him, and it begins to separate from the walls of the uterus prematurely);
- too sharp reduction in the volume of the uterus;
- illiterate use of uterotonics - drugs that promote uterine contraction.
Signs of placental abruption in early and late pregnancy
Common symptoms of placental abruption:
- increased uterine tone (the muscle layer of the uterus becomes tense);
- weakness, pale skin, dizziness;
- bloody discharge from the genital tract (the volume depends on the size of the separated area);
- lower abdominal pain;
- hypotension;
- increased heart rate;
- changes in heart rate indicators.
If we describe the symptoms of premature placental abruption at different stages of pregnancy, then each trimester is characterized by its own symptoms.
I trimester
In the first trimester arise:
- mild pain;
- placental hematoma.
The process is still treatable, but emergency hospitalization is required.
II trimester
In the second trimester, premature placental abruption manifests itself:
- abdominal pain;
- hematoma;
- high uterine tone and pronounced tension.
There is a high risk of oxygen starvation of the fetus, due to which the child begins to move very actively.
III trimester
In the third trimester of pregnancy, placental abruption occurs most often. Its symptoms are typical:
- severe pain in the lower abdomen;
- bleeding;
- increased fetal activity.
Since the placenta is no longer growing, feto-placental insufficiency quickly develops. But an emergency caesarean section is not always indicated. If the exfoliated area is small, there is a chance of blocking the further spread of the pathological process.
If you notice similar symptoms, consult a doctor immediately. It is easier to prevent a disease than to deal with the consequences.
Diagnosis of premature placental abruption
Diagnosis of placental abruption during pregnancy is not difficult for obstetricians and gynecologists. The doctor takes into account the presence of bleeding, pain, hypoxic suffering of the fetus and hemodynamic disorders.
During a gynecological examination, hypertonicity and asymmetry of the uterus are revealed. On palpation the patient experiences pain.
- Using ultrasound, you can see the exfoliated area and accurately determine its size.
- Dopplerography of uteroplacental blood flow allows to detect disturbances in transplacental hemodynamics.
- The degree of fetal hypoxia is determined using phonocardiography and cardiotocography procedures.
A slight placental abruption can also be detected after childbirth by the characteristic indentation with dark blood clots present on its surface.
Severity of the problem
The complication in question can be of three degrees of severity:
- light
Such a detachment is discovered mainly after childbirth. Pathology can also be detected during gestation by ultrasound. At the same time, the woman feels normal, and the condition of the fetus is also normal. The symptoms described above simply do not exist.
- medium-heavy
This means that the baby's place is behind the uterus by 1/3-1/4 of the total area. In this case, a small amount of blood is released from the vagina. The doctor detects uterine hypertonicity and fetal bradycardia. In this case, the patient may have a stomach ache. Manifestations of hemorrhagic shock gradually intensify.
- heavy
Abdominal pain is characterized as bursting and severe. In this case, the pain appears suddenly, along with dizziness and severe weakness. Some women faint. There may be little or moderate bleeding from the genitals. The doctor notes that the uterus is asymmetrical, dense, and sharp pain occurs on palpation.
The placenta with this form has separated by ½ or more. This is a huge threat to the unborn child. It is urgent to take medical action so that the child does not die in the mother’s belly. There is a rapid increase in the manifestations of DIC syndrome, the patient feels worse and worse and may die.
Treatment of placental abruption in early and late pregnancy
When choosing a treatment regimen for premature placental abruption, obstetricians and gynecologists take into account the following factors:
- the moment when the detachment process began;
- condition of mother and child;
- severity of bleeding;
- volume of blood loss.
Doctors may refuse emergency delivery if the following indicators occur:
- pregnancy is less than 36 weeks;
- detachment occurred in a small area and does not progress further;
- the amount of blood loss is insignificant and discharge from the external genital tract has stopped;
- the pregnant woman feels well and is in the hospital under constant medical supervision;
- no symptoms of fetal hypoxia were identified.
Treatment of non-progressive partial placental abruption
For non-progressive partial placental abruption at up to 36 weeks, a woman is prescribed:
- bed rest;
- antispasmodics;
- hemostatic drugs;
- antianemic drugs;
- tocolytics (medicines that reduce uterine contractility).
Treatment is necessarily carried out under the control of Doppler ultrasound, ultrasound, and coagulogram.
If symptoms of placental abruption progression occur, the question of early delivery arises. If the birth canal is ready (the cervix is softened, sufficient patency of the cervical canal is diagnosed), amniotomy is performed (artificial rupture of the membranes). Childbirth can be natural with constant cardiac monitoring.
Treatment of placental abruption of moderate and severe severity
If moderate or severe premature placental abruption is diagnosed, a cesarean section is performed. This does not take into account the gestational age of the child and his viability. After removing the fetus from the uterus, surgeons completely separate the placenta and remove any clots that have formed. Then the walls of the uterus are examined and the condition of the myometrium is determined. If the changes in the organ are significant, a hysterectomy is performed - surgical removal of the uterus.
Regardless of which method of delivery was chosen by doctors, blood loss is restored, anemia and bleeding disorders are corrected using transfusion or infusion therapy. To exclude the occurrence of uterine bleeding in the postpartum period, the woman in labor is prescribed uterotonic drugs, for example, prostaglandins, oxytocin, methylergometrine.
Surgery to remove the entire uterus is performed to save a woman's life when the uterine wall becomes saturated with blood (Couveler's uterus). Sometimes, instead of removing an organ, ligation of the vessels feeding it is performed, however, this is a very complex operation that is not always possible.
Features of placental abruption in the second trimester
The birth of a healthy baby is the dream of every woman.
Rejection of the placental structures during the period of 12-27 weeks of pregnancy usually implies the presence of a hematoma clearly visible on ultrasound examination, increased tension and tone of the muscles of the uterine body. The development of hypoxic conditions is indicated by a change in the baby’s behavior; the baby begins to behave extremely restlessly, he activates movements to speed up blood flow.
In the second trimester, the specific week in which rejection occurred is of utmost importance. It’s just that placental structures can grow until half of the second trimester (≈20 weeks), so they can still have time to compensate for the lost points of contact with the uterine body. At a later date, experts raise the question of an emergency delivery operation that will help save the baby.
The most dangerous is considered to be detachment in the 3rd trimester, when the placenta has already lost any compensatory capabilities, so it will not be able to restore its activity after detachment. If placental rejection occurs in the later stages of gestation, emergency delivery is necessary for vital indications. If a minor, partial detachment is diagnosed, and the bleeding has stopped safely on its own, then the pregnant woman is placed in a hospital until delivery in order to safely save the baby.
The danger and consequences of premature placental abruption for the fetus and mother
Premature placental abruption can lead to the death of both mother and child, so doctors take this disease very seriously. According to statistics, children die in 15% of cases.
Babies born from a pregnancy complicated by premature detachment very often suffer from various neurological disorders. The reason for this is intrauterine hypoxia. Often repeated pregnancy in women also occurs with detachment.
So, premature placental abruption in early or late pregnancy is dangerous:
- the fact that the fetus begins to suffocate and may die in utero or be born with neurological abnormalities;
- multiple hemorrhages in the uterine wall lead to the development of a condition that gynecologists call Kuveler's uterus (the organ is completely saturated with blood and is subject to amputation, the woman becomes infertile);
- you can never exclude the risk of developing disseminated intravascular coagulation syndrome - a very serious disorder of the blood coagulation system, leading to the formation of intravascular clots and bleeding;
- Hemorrhagic shock may occur (due to large blood loss, the functions of the nervous system, circulatory and respiratory systems are disrupted).
Forecasts
Premature detachment is considered a fairly common factor leading to stillbirth in the last weeks of gestation. About 15% of children die from this pathology. The consequences of premature placenta rejection can be very serious, both for the mother and for the fetus. This condition is threatening and therefore requires mandatory and urgent intervention by an obstetrician-gynecologist. It’s better to take care of prevention in advance to avoid dangerous consequences.
Risk group for the development of premature placental abruption during pregnancy
Most often, premature placental abruption is diagnosed in pregnant women who suffer from high blood pressure. It does not matter whether the symptoms of hypertension made themselves felt before or after conception.
Also at risk for the development of obstetric pathology include:
- black women;
- pregnant women with bleeding disorders;
- patients over 40 years of age;
- women in labor who already have several children;
- women who smoke and drink alcohol;
- drug addicts;
- having abortions.
Prevention of premature placental abruption
In order to avoid premature placental abruption during pregnancy, the following measures must be observed:
- Plan your pregnancy and prepare wisely for it. It is recommended to identify existing gynecological and chronic diseases in advance and treat them.
- Eliminate abortions.
- Register with the antenatal clinic before 12 weeks of pregnancy.
- During pregnancy, regularly visit a gynecologist (standard scheme: in the first trimester - once a month, in the second trimester - once every 2-3 weeks, in the third trimester - once every 7-10 days), do not ignore medical recommendations.
- If there is uterine tone, consult a gynecologist about the advisability of taking tocolytics (drugs that relax the uterus).
- Promptly treat pregnancy complications such as: - placental insufficiency (due to insufficient blood supply to the vital uterus-placenta system, the functioning of the placenta is disrupted); - gestosis (a complication of pregnancy, characterized by the appearance of edema, impaired renal function, high blood pressure); - high blood pressure (this means a persistent, not a single increase).
- Avoid emotional experiences and intense physical activity.
This article is posted for educational purposes only and does not constitute scientific material or professional medical advice.