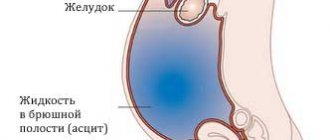
Ascites (accumulation of fluid in the abdominal cavity) is detected in 50% of patients in the early stages of cancer and in almost all patients in whom the cancer process is at the last stage.
The Oncology Clinic of the Yusupov Hospital is equipped with the latest diagnostic equipment from the world's leading manufacturers, with the help of which oncologists identify the early stages of oncological pathology. Chemotherapists, radiologists, and oncologists treat patients with ascites in accordance with international standards of medical care. At the same time, doctors take an individual approach to choosing a treatment method for each patient.
Reasons for development
Ascites is a serious complication of stomach and colon cancer, colorectal cancer, malignant tumors of the pancreas, and oncological pathology of the mammary glands, ovaries and uterus. When a large volume of fluid accumulates in the abdominal cavity, intra-abdominal pressure increases, and the diaphragm moves into the chest cavity. This leads to disruption of the heart and lungs. There is a violation of blood circulation in the vessels.
In the presence of ascites, the patient's body loses a large amount of protein. Metabolism is disrupted, heart failure and other imbalances in the internal environment of the body develop, which worsen the course of the underlying disease.
There is always a small amount of fluid in the abdominal cavity of a healthy person. It prevents the sheets of peritoneum from sticking together. The produced intra-abdominal fluid is reabsorbed by the peritoneum.
With the development of cancer, the normal functioning of the body is disrupted. The secretory, resorptive and barrier functions of the peritoneal layers fail. In this case, either excess fluid production or disruption of its absorption processes may be observed. As a result, a large volume of exudate accumulates in the abdominal cavity. It can reach twenty liters.
The main reason for damage to the peritoneum by malignant cells is its close contact with organs that are affected by a cancerous tumor. Ascites in the presence of oncological pathology develops under the influence of the following factors:
- A large accumulation of blood and lymphatic vessels in the peritoneum through which cancer cells spread;
- Tight fit of the folds of the peritoneum to each other, which contributes to the rapid spread of malignant cells to adjacent tissues;
- Germination of a cancerous tumor through the peritoneal tissue;
- Transfer of atypical cells to peritoneal tissue during surgery.
Chemotherapy may be the cause of ascites. The accumulation of fluid in the peritoneum occurs due to cancer intoxication. If the liver is affected by a primary cancerous tumor, metastases of malignant cells from tumors of a different location, the outflow of blood through its venous system is disrupted, and portal hypertension develops - an increase in pressure inside the portal vein. The lumen of the venous vessels increases, plasma sweats from them and accumulates in the abdominal cavity.
The cause of ascites may be peritoneal carcinomatosis. In the presence of a cancerous tumor of the abdominal organs, atypical cells settle on the parietal and visceral sheets of the peritoneum. They block the resorptive function, as a result of which the lymphatic vessels do not cope well with the intended load, and lymph outflow is impaired. Free fluid gradually accumulates in the abdominal cavity. This is the mechanism of development of carcinomatous ascites.
Make an appointment
Causes
The largest percentage of ascites is caused by liver pathology, mainly cirrhosis. Of 100 patients suffering from ascites, 80 were diagnosed with end-stage cirrhosis with liver failure. The second most common etiological cause is malignant diseases - no more than 15% of all, and 5% are caused by heart disease and other non-tumor nosologies.
In cancer, the leading cause of effusion is peritoneal metastases or peritoneal carcinomatosis.
The largest cohort of patients with ascites are those suffering from ovarian cancer, which is due to the high incidence - more than 14 thousand annually and the latent course of the malignant process. At the time of detection of the tumor, two out of three patients have metastases in the abdominal cavity with concomitant ascites, however, tumor damage to the peritoneum does not transfer the process to stage 4, unlike the vast majority of malignant processes in other organs. Due to the complexity of differentiating tumor processes within the abdominal cavity, the commonality of diagnosis and treatment, ovarian cancer was even combined with primary peritoneal cancer.
With carcinoma of the stomach or pancreas, ascites at the time of cancer detection is found in 30–40% of patients; in the terminal stage of the disease, effusion in varying quantities is found in almost all patients. Excessive synthesis of fluid is caused by several mechanisms, in addition to carcinomatosis: the “liver” component in the form of metastases in the liver itself and the lymph nodes of its gates, increased thrombus formation and impaired blood rheology.
For colon cancer, effusion is not typical - the frequency is no more than 10%, many times inferior to metastasis to the liver, lungs and lymph nodes.
Hepatocellular carcinoma can be complicated by ascites of cirrhotic origin; its share is minimal in the overall structure of malignant processes complicated by effusions.
Peritoneal mesothelioma is usually accompanied by effusion, but the disease is extremely rare.
The total number of Russians suffering from ascites is unknown, because statistics do not take into account the frequency of symptoms of a malignant disease.
Stages of severity
There are three stages of abdominal hydrops depending on the amount of accumulated fluid:
- Initial stage - up to one and a half liters of fluid accumulates in the abdominal cavity;
- Moderate ascites - manifested by an increase in the size of the abdomen, edema of the lower extremities. The patient is concerned about severe shortness of breath, heaviness in the abdomen, heartburn, constipation;
- Severe dropsy - from 5 to 20 liters of fluid accumulates in the abdominal cavity. The skin on the abdomen tightens and becomes smooth. Patients experience heart failure and respiratory failure. When the fluid becomes infected, ascites-peritonitis (inflammation of the peritoneal layers) develops.
Symptoms
The main manifestation of ascites is a significant increase in size and pathological bloating of the abdomen. Signs of abdominal dropsy can increase rapidly or over several months. Ascites is manifested by the following clinical symptoms:
- Feeling of fullness in the abdominal cavity;
- Pain in the abdomen and pelvis;
- Increased gas formation (flatulence);
- Belching;
- Heartburn;
- Digestive disorders.
Visually, the patient’s abdomen enlarges, in a horizontal position it hangs down and begins to “blur” on the sides. The navel gradually protrudes more and more, and blood vessels are visible on the stretched skin. As ascites develops, it becomes difficult for the patient to bend over and shortness of breath appears.
Doctors at the Oncology Clinic evaluate the clinical manifestations of the disease and carry out a differential diagnosis of cancer with other diseases, the manifestation of which is ascites.
How is tense ascites formed?
The accumulation of ascitic fluid is extended over time, the organs have time to adapt to changes in intraperitoneal pressure, so effusion is detected by an enlarged abdomen and symptoms of impaired hemodynamics and functions of internal organs.
The International Ascites Society (IAS) has identified three degrees of severity of effusion without taking into account the severity of clinical manifestations and prognosis, only based on the presence of fluid and the method of its detection:
- Grade 1 - effusion is found during ultrasound of the abdominal cavity, because the volume of fluid is minimal and does not affect the patient’s condition, a “diagnostic finding.”
- 2nd degree - the presence of exudate is indicated by the appearance of the patient, whose abdomen is evenly enlarged, they say “froglike”, the volume is measured in liters, in this severity ascites can no longer but affect the patient’s well-being.
- Grade 3 - intense ascites, clinical manifestations are pronounced and the patient’s condition is serious.
Ascites to the maximum degree of tension goes through all stages, their duration is individual. The volume of metastatic lesions of the peritoneum does not correlate with the rate of formation and volume of effusion: microscopic tumor nodules are capable of synthesizing liters of exudate in a week, while tumor deposits in mesothelioma increasing the thickness of the peritoneum to several centimeters lead to an effusion of less than one to two liters over a very long observation period.
On the other hand, a massive cancerous lesion in a limited volume of the abdominal cavity can simulate tense ascites with an exudate of 3–5 liters. In most cases, with tense ascites, there is more than 10 liters of fluid in the cavity.
Get a treatment program
Diagnostics
Doctors identify ascites during an examination of the patient. Oncologists at the Yusupov Hospital conduct a comprehensive examination of patients, which allows them to identify the cause of fluid accumulation in the abdominal cavity. One of the most reliable diagnostic methods is ultrasound. During the procedure, the doctor not only clearly sees the liquid, but also calculates its volume.
In case of ascites, oncologists necessarily perform laparocentesis. After puncturing the anterior abdominal wall, the doctor aspirates fluid from the abdominal cavity and sends it to the laboratory for testing. Computed tomography radiology scans are used to determine the presence of malignant tumors in the liver that cause portal hypertension.
Magnetic resonance imaging makes it possible to determine the amount of accumulated fluid and its location.
Complications
Complications of ascites can be both short-term and long-term.
Often, ascites is combined with a non-tumor effusion into the pleural cavity, usually on the right side. After removal of ascites, pleurisy regresses on its own.
Airless areas in the lower parts of the lungs - atelectasis are straightened out when the domes of the diaphragm are lowered immediately after paracentesis, but sometimes medications are required to suppress sluggish inflammation.
High intra-abdominal pressure causes expansion of the diaphragmatic opening with the formation of a hernia and reflux of gastric contents into the esophagus. A chronic burn of the mucous membrane is complicated by inflammation - esophagitis with the formation of erosions . The inflammation can be controlled with medications and dietary nutrition, the hiatal hernia does not regress, and you will have to adhere to the rules throughout your life: do not overeat, do not lie down after eating, do not abuse spicy and sour foods.
Ascites provokes the formation of hernias of the abdominal wall and inguinal canal, which is facilitated by muscle atrophy against the background of a malignant process.
A severe complication is spontaneous peritonitis due to microscopic disturbances of the intestinal wall and decreased immunity against the background of changes in the intestinal microflora.
Treatment
Drug therapy for ascites is not carried out due to low effectiveness. Aldosterone antagonists and diuretics normalize water-salt metabolism and prevent excess secretion of peritoneal fluid. Oncologists at the Yusupov Hospital offer palliative surgery to patients with ascites in the late stages of cancer:
- Omentohepatophrenopexy;
- Deperitonization;
- Installation of a peritoneovenous shunt.
Doctors at the Oncology Clinic carry out traditional or intracavitary chemotherapy for ascites - after removing the fluid, a chemotherapy drug is injected into the abdominal cavity. Laparocentesis is performed to remove fluid. The procedure is not performed if the following contraindications are present:
- Adhesive process inside the abdominal cavity;
- Severe flatulence;
- Perforation of the intestinal walls;
- Purulent infectious processes.
Laparocentesis is prescribed in cases where taking diuretics does not lead to a positive result. The procedure is also indicated for resistant ascites.
Laparocentesis is carried out in several stages using local anesthesia:
- the patient is in a sitting position, the doctor treats the subsequent puncture site with an antiseptic and administers painkillers;
- An incision is made in the abdominal wall along the linea alba at a distance of 2-3 centimeters below the navel;
- The puncture itself is performed using a trocar using rotational movements. A special flexible tube is attached to the trocar, through which excess fluid is removed from the body. The fluid is pumped out quite slowly, and the doctor constantly monitors the patient’s condition. As the exudate is removed, the nurse tightens the patient's abdomen with a sheet to slowly reduce the pressure in the abdominal cavity;
- After the fluid is pumped out, a sterile bandage is applied to the wound.
Using laparocentesis, up to 10 liters of fluid can be removed from the patient’s body. In this case, it may be necessary to administer albumin and other drugs to prevent the development of renal failure.
If necessary, temporary catheters can be installed in the abdominal cavity, through which excess fluid will gradually be removed. It should be noted that the use of catheters can lead to a decrease in blood pressure and the formation of adhesions.
There are also contraindications to laparocentesis. Among them:
- pronounced flatulence;
- adhesive disease of the abdominal organs;
- stage of recovery after surgery on a ventral hernia.
Diuretics are prescribed to patients with developing ascites in cancer over a long course. Such drugs as Furosemide, Diacarb and Veroshpiron are effective.
When taking diuretics, medications containing potassium must also be prescribed. Otherwise, there is a high probability of developing disturbances in water and electrolyte metabolism.
Dietary nutrition primarily involves reducing the amount of salt consumed, which retains fluid in the body. It is also important to limit the amount of fluid you drink. It is recommended to include more foods containing potassium in your diet.
After removal of fluid from the abdominal cavity, patients are provided with a balanced and high-calorie diet. This allows you to meet the body's needs for proteins, carbohydrates, vitamins and minerals. Fat consumption is reduced.
Ascites: what is it and how to treat it
Contents ASCITS
REMOVAL OF ASCITES
FEARS AND MISCONCEPTIONS
There is always fluid present in the abdominal cavity of a healthy person. Normally it is no more than 150 ml. Up to 1.5 liters are produced per day, but it is absorbed and does not accumulate. However, with some diseases, the amount of fluid increases - it begins to be produced in excess, or it stops being absorbed.
Together with surgeon Alina Pribytkova, we understand what ascites is and how it is treated.
ASCITS
What is ascites?
Ascites is an accumulation of free fluid in the abdominal cavity. The reasons may be different: most often it is oncology, chronic heart failure, cirrhosis of the liver or kidney disease.
In oncology, the development of ascites most often provokes metastatic damage to the peritoneum, which causes excess fluid production and/or impairs its reabsorption.
There is another cause of ascites in cirrhosis. Normally, the liver synthesizes proteins that help retain fluid inside the vessel. When the liver is damaged, this function suffers, and fluid leaks through the walls of blood vessels more easily.
In chronic heart failure, blood stagnates in the systemic circulation, increased pressure occurs in the vessels and fluid from them leaks into the abdominal cavity. Also, with this pathology, sodium retention occurs in the body, which also contributes to the development of edema.
Kidney disease causes excessive excretion of proteins in the urine (proteinuria). The loss of protein leads to the fact that the liquid part of the blood is not retained in the vessels and leaks through their walls.
Important Ascites indicates deterioration and progression of the disease. In the early stages of the disease, fluid will not accumulate in the abdominal cavity. This happens only in the later stages of the disease, when the body's ability to compensate has been exhausted.
What types of ascites are there?
Ascites is divided into non-tense and tense.
Small or moderate ascites (non-tense) is a condition when fluid has already accumulated inside the abdominal cavity, but this is not enough to prescribe a procedure for removing ascites: there are no signs of tension, the abdominal wall is soft, pliable during palpation - “pressed”. In this case, surgical evacuation of fluid (laparocentesis) is not used due to the high risk of injuring internal organs, since with non-stressed ascites the distance between the internal organs and the anterior abdominal wall is not enough for manipulation due to the small layer of fluid between them.
With intense ascites, the abdomen becomes greatly enlarged, the skin is tightly stretched, shiny, and the navel may protrude, as during pregnancy. When palpating the anterior abdominal wall, great resistance is felt, which is created due to fluid pressure from the inside.
In quantitative terms, ascites becomes tense when fluid accumulates approximately over 7 liters, but all people are different: physique, parameters, body constitution, size of the abdominal cavity. Therefore, doctors do not focus on the volume of fluid: they perform an ultrasound of the abdominal cavity, examine and palpate the abdomen.
In a person with short stature and asthenic physique, ascites can be tense and with the accumulation of 5 liters of fluid. At the same time, in a tall person with a hypersthenic physique, 10 liters of free fluid may not give signs of tense ascites.
Webinar: Organizing therapeutic nutrition for a seriously ill patient How to organize therapeutic nutrition, what to prepare, what and where to feed, so that the food brings not only benefits, but also pleasure Workshop of CareOlga Kotelnikova
Care
Characteristic symptoms appear with tense ascites: a large belly with a protruding navel, like in pregnant women, a feeling of fullness in the abdomen and pressure on the stomach, nagging pain in the abdomen, shortness of breath, problems with eating due to the pressure of fluid on the stomach - belching, nausea or even vomiting, restriction of physical activity. The accumulation of fluid leads to increased intra-abdominal pressure and pushing of the diaphragm into the chest cavity. As a result, the respiratory movements of the lungs are significantly limited (up to the development of respiratory failure), the activity of the heart is disrupted, and the resistance to blood flow in the abdominal organs increases, the functions of which are also impaired. With long-term ascites, the outflow of lymph from the lower extremities and abdominal organs is disrupted, and swelling of the lower extremities occurs. People note a significant increase in general weakness.
Should we sound the alarm? When?
Ascites does not occur overnight; fluid accumulates gradually. A person may not even notice it and think that he is gaining weight. Usually, suspicions arise when specific symptoms occur: an enlarged abdomen, a feeling of fullness in the abdomen and pressure on the stomach, nagging pain in the abdomen, shortness of breath, belching, nausea or even vomiting, limitation of physical activity, swelling of the lower extremities, general weakness.
If a person notices signs of ascites, you need to see a doctor and do an ultrasound of the abdominal cavity: then the doctor will give recommendations and tell you whether the ascites needs to be removed surgically.
If a person is regularly observed by a doctor, then ascites can be detected during routine instrumental examinations (ultrasound, CT), during examination. If necessary, the doctor will prescribe additional examinations and give recommendations.
REMOVAL OF ASCITES
How is ascites removed?
To treat mild ascites, diuretics can be prescribed, which are most effective in cases of ascites resulting from chronic heart failure or cirrhosis of the liver. However, it should be remembered that there are refractory ascites, that is, resistant to diuretic therapy, when the use of medications does not have a positive effect. With prolonged, uncontrolled use of diuretics, the patient develops water and electrolyte disturbances, dehydration, and a drop in blood pressure. With ascites of an oncological nature, diuretics are most often ineffective.
For tense ascites, doctors perform laparocentesis: under local anesthesia, a puncture of the anterior abdominal wall is performed and the fluid is evacuated.
The frequency of the procedure depends on how quickly the fluid accumulates, on the existing pathology and the degree of its progression. For some, tense ascites may recur within a few months, for others within a week/month.
For ascites, the cause of which is chronic heart failure or cirrhosis of the liver, diuretics are also prescribed after surgical removal of the fluid, if the person’s condition allows.
How is the procedure done?
If there is a clinical picture of tense ascites, an ultrasound of the abdominal cavity is performed to assess the level of free fluid and determine the safest point for puncture of the anterior abdominal wall.
They talk with the person: they explain to him the principle of the planned manipulation, the possible risks, as with any invasive intervention. After which, if he agrees to the manipulation, the person signs an informed consent to the intervention. If a person is legally capable, he must sign the document himself; if not, then this is done by his official representative.
The area of the planned puncture of the anterior abdominal wall is treated with an antiseptic solution and then anesthetized layer by layer with a 5-10 ml syringe with a local anesthetic solution (lidocaine, novocaine - if the patient is allergic to these drugs, tell the doctor!). At the same time, the location of the needle is monitored - when it enters the abdominal cavity, ascitic fluid appears in the syringe.
Then, using a long hollow needle - or a special instrument - a stylet with a trocar, depending on the equipment chosen for the manipulation - the doctor pierces the anterior abdominal wall at a previously designated point and penetrates the abdominal cavity, receiving a flow of fluid through the needle. A plastic catheter is passed through the needle into the abdominal cavity, and the needle itself is removed. The plastic catheter is sutured to the skin to prevent it from moving or falling out. Through the catheter, the outflow of fluid goes into a vacuum bag attached to it (for better outflow, the bag should be below the level of the bed - on the floor or attached to the side of the bed).
The most favorable is fractional removal of fluid - 3-4 liters per day, as this will help avoid a sharp drop in pressure inside the abdominal cavity.
Skin care products for a sick person: how to choose? We help you understand the variety of foams, dry shampoos, creams and lotions for hygiene, including in special cases - with bedsores, an established stoma, urinary and fecal incontinence Evgeniya RezvanCar Care Workshop
Care
The drainage is in the abdominal cavity for several days, since it is fixed to the skin with a suture - you can turn, eat, move, the tube will not go anywhere. The puncture site must be treated with an antiseptic once a day and covered with an aseptic bandage. Usually, drainage does not cause pain; on the first evening after the puncture, there may be a slight pain in the area of the puncture of the abdominal wall, then, if there is no planned pain therapy, you can take a painkiller from the NSAID group (if there are no contraindications). But the drainage tube can touch the peritoneum, which lines the anterior abdominal wall from the inside and internal organs, and this in turn can cause discomfort.
After removing the ascites, the drainage from the abdominal cavity is removed. A suture may be placed over the punctured area to prevent any remaining fluid from leaking out. It is impossible to remove everything “dry”, since residual fluid remains in the pelvic cavity and between the intestinal loops, and its accumulation does not stop after laparocentesis. If a suture was not applied, then after a while the tissues “stick together” and the liquid stops leaking.
If a suture was placed after removing the drainage, then it must be treated with an antiseptic solution, the dressings should be changed once a day, healing usually occurs in 7-10 days. If a suture was not applied, the principle of care is the same, the difference is that in the first day or two after removal of the drainage, there may be a need to change the dressing more often due to slight leakage of fluid.
There are ascites that are difficult to evacuate: the liquid may have a gel-like nature, a heterogeneous structure, which can clog the drainage, or in rare cases, the liquid may not flow through the drainage at all due to its excessive viscosity. If the drain is blocked, the doctor will flush it with sterile saline to restore drainage.
Patient N., 56 years old. Diagnosis: Ovarian cancer, disease progression, peritoneal carcinomatosis, tense ascites. According to ultrasound, ascites is gel-like in nature, with a volume of about 10 liters. A decision was made to perform laparocentesis. As a result of the manipulation, practically no liquid flows through the installed plastic catheter due to an excessively thick jelly-like consistency that cannot be actively aspirated (that is, removed by attaching a syringe to the catheter). Next, a repeat laparocentesis was performed using a large-diameter trocar (hollow metal tube), with which it was possible to evacuate no more than 3 liters of secretion. The patient was recommended symptomatic therapy; further attempts to evacuate secretions are inappropriate due to the risk of complications.
The laparocentesis procedure is not very long, in typical cases it takes no more than 15-20 minutes. There are technically complex cases that require more time: if a person has excessively developed subcutaneous fat, there have been surgeries on the abdominal organs in the past, massive growth of metastases in the peritoneum, the presence of voluminous tumors in the abdominal cavity. In such cases, puncture can be performed directly under ultrasound guidance.
Is it possible to carry out the procedure at home? Can I go home immediately after the procedure?
Removal of ascites is a surgical intervention; it is not performed at home, like any other surgical operation: there is no necessary equipment, conditions, and sterility cannot be ensured.
It will also not be possible to go home with drainage, since it is a foreign body. It must be removed at a medical facility. At home, if the drainage is handled incorrectly, it can become dislodged/fall out, which can lead to infection. It is not recommended to remove ascites “in one day”; it is better to do it gradually, over several days, since the immediate removal of a large amount of fluid can provoke a sharp drop in pressure inside the abdominal cavity, which will entail a drop in a person’s systemic blood pressure and a deterioration in general well-being.
Are there any contraindications to the procedure? When can doctors refuse to perform a procedure?
The procedure is not performed when the ascites is not tense or is not tense enough, since in these cases internal organs can be damaged. With mild ascites, there are no painful symptoms, which is the reason to perform laparocentesis. It must be remembered that evacuation of fluid does not cure the disease, but only alleviates the painful manifestations that arise when there is a large accumulation of fluid.
Evacuation of fluid is not carried out if a person is in extremely serious condition, in other words, when the life prognosis is calculated in hours or days, and this means a complete depletion of the body’s compensatory forces. And the loss of protein, electrolytes, a decrease in intra-abdominal pressure with general hypotension (which is always present in the last days and hours of life) can only worsen the patient’s condition; after the manipulation he may not experience relief, and the stress of the intervention will add additional painful sensations to the already extremely serious condition. And we remember that the manipulation is invasive in nature, that is, like any surgical intervention, it can have a number of complications.
The procedure may be refused when a critical accumulation of fluid coincides with the transition to the terminal stage of the disease. Of course, the fluid can be evacuated: technically this is possible for almost any patient's condition, but the person's general condition will continue to get worse as the underlying disease progresses, and the fluid, even during the evacuation process, can quickly accumulate again. As mentioned above, it must be remembered that laparocentesis does not cure the disease, but only alleviates the painful manifestations that occur with a large accumulation of fluid, and it is necessary to compare the expected benefits of the manipulation and the existing risks of causing additional discomfort to the person at the end of life.
For example, according to abdominal ultrasound, the volume of ascites is 8 liters. The doctor puts in a drainage, but the fluid accumulates every day. A person gets 8 liters, 10 liters, 12 liters removed - so a week passes, and the drainage is still standing. He does not experience relief from the manipulation, and the drainage located in the abdominal cavity causes discomfort and complicates the care of the patient.
We already know that when ascitic fluid is removed, a person loses valuable substances - proteins and electrolytes. The protein concentration in serous ascitic fluid is usually relatively low, but with massive ascites, its total loss can be significant, especially with frequent repeated removal of large amounts of fluid, and the loss of protein is combined with the loss of salts, which leads to the development of severe protein and electrolyte deficiency.
Frequent laparocentesis or fractional pumping of fluid from the abdominal cavity over a long period of time will do more harm than good, so transition to the terminal stage of the disease is a contraindication to the procedure.
When it cannot be cured: 7 questions about palliative care Why palliative care is needed, whether it is necessary to register and what to do if a person or his relatives insist on continuing treatment Editorial Board "Vera" Foundation
About palliative care
Laparocentesis is not performed if:
- blood clotting is impaired (the risk of bleeding increases);
- decreased platelet levels (especially after chemotherapy);
- a pronounced adhesive process has been diagnosed (dense connective tissue (cords, adhesions) is formed in the abdominal cavity after inflammatory processes, injuries or surgical interventions, which “solder” the internal organs in the peritoneum, lining the anterior abdominal wall from the inside) - this is a risk of injury to the internal organs;
- peritoneal carcinomatosis was diagnosed, when the abdominal cavity is so affected by metastases that a safe area for puncture is not visualized, which is also fraught with injury or bleeding;
- a person has an unfavorable life prognosis (days, hours).
FEARS AND MISCONCEPTIONS
Is it possible to die from ascites or from the procedure for its removal?
Ascites, like the procedure for removing fluid from the abdominal cavity, cannot cause death. Ascites is not an independent disease, but usually acts as a symptom of one or another serious disorder in the body.
It should be remembered that with laparocentesis, as with any surgical intervention, even in the absence of contraindications, there is a low risk of complications.
Can ascites occur due to medications? Chemotherapy?
Drugs and chemotherapy cannot cause ascites.
Important: People with ascites are advised to evacuate it before chemotherapy to increase effectiveness.
To prevent fluid from accumulating, should you drink less water?
It is necessary to maintain a water-drinking regime, drink as needed. Refusal to drink can worsen the general condition and provoke the appearance of additional painful symptoms against the background of dehydration.
What happens if ascites is not removed?
Fluid in tense ascites does not mechanically damage internal organs, but can put pressure on the stomach, intestines, diaphragm, lymphatic system and disrupt their functions. This can cause breathing problems, constipation, nausea, vomiting, hiccups, belching, heartburn, loss of appetite, swelling of the lower extremities, even lymphorrhea (“sweating” of fluid through the skin). Against the background of the underlying disease, pain may intensify, and a feeling of tension and fullness in the abdominal cavity may appear.
It happens that with a very large accumulation of fluid in the abdominal cavity (20 liters or more), the pressure on the tissue is so high that the fluid begins to find “weak spots” in the abdominal wall and seep through them (scars after operations and even the navel).
Can internal organs be damaged during the procedure?
With mild ascites, there is a high probability of damaging internal organs, so in this case laparocentesis is contraindicated. If there is a significant amount of fluid and signs of tension, the risk of injury is minimal. Complications are possible with any operation, but with the correct indications and taking into account all contraindications, in the vast majority of cases laparocentesis occurs without complications or injuries.
Can drainage damage internal organs?
Changing the position and turning a bedridden patient Care specialist Olga Vygovskaya shows how to correctly turn a bedridden patient Olga Vygovskaya
Care
The drainage tube is soft, it will not damage the internal organs, but it can touch the peritoneum lining the anterior abdominal wall from the inside and internal organs, and this in turn can cause discomfort.
Is it possible to lie on your stomach with ascites? Is the blow dangerous?
Lying on the stomach for a person with tense ascites is extremely uncomfortable, but this is not prohibited. Most often, a person takes a position on his side. Any blows to the stomach in everyday life are also not dangerous: it is a liquid, it “flows around” the internal organs. Blows of excessive force are equally dangerous for internal organs, regardless of the presence of fluid in the abdominal cavity.
Are emergency operations performed for ascites?
If, for urgent reasons, a person with ascites suddenly finds himself on the operating table, this is not a contraindication to emergency surgery; surgeons simultaneously remove free fluid; all operating rooms are equipped with electric aspirators.
The material was prepared using a grant from the President of the Russian Federation provided by the Presidential Grants Foundation.
We would like to thank the volunteers of the Vera Hospice Fund for their assistance in preparing the material.
Stock image used from Depositphotos.
Non-cancerous ascites
Ascites is a consequence of various disorders that occur in the body. Treatment tactics depend on the pathological process that caused the accumulation of fluid in the abdominal cavity:
- To treat acute heart failure, cardiologists at the Yusupov Hospital prescribe metabolites, beta blockers, and ACE inhibitors to patients;
- For infectious and toxic liver lesions, therapy with hepatoprotectors is carried out;
- If ascites has developed due to low protein levels in the blood, albumin infusions are performed;
- Ascites that develops as a result of peritoneal tuberculosis is treated with anti-tuberculosis drugs.
To remove fluid from the body, patients with ascites are prescribed diuretics. The main method of eliminating ascites is to remove accumulated fluid by puncturing the abdominal wall, followed by installing drainage. For persistent ascites, peritoneal fluid is reinfused after filtration. A peritoneovenous shunt for abdominal ascites ensures the flow of fluid into the general bloodstream. To do this, surgeons form a structure with a valve, through which fluid from the abdominal cavity enters the superior vena cava system during inhalation.
Omentohepatophrenopexy for abdominal ascites is performed to reduce pressure in the venous system. The surgeon sutures the omentum to the diaphragm and liver. Then, during breathing movements, the veins are unloaded from blood. As a result, the release of fluid through the vascular wall into the abdominal cavity decreases. As a result of deperitonization (excision of areas of the peritoneum), additional outflow pathways for peritoneal fluid are created.
Symptoms of tense ascites
Tense ascites is a huge belly, uniform and smooth, the navel protrudes outward. In the supine position, the abdomen flattens somewhat, but it is difficult for the patient to lie down—cardiopulmonary failure increases. The patient cannot move; he sits, leaning on his arms with his torso tilted forward, facilitating the breathing movements of the chest.
The patient's face is puffy, the skin is pale and moist, the nasolabial triangle and lips are bluish.
Grade 3 ascites significantly worsens the patient’s condition due to compression of internal organs and displacement of the diaphragm separating the chest and abdominal cavities.
The organs of the mediastinum and the heart change their location, and symptoms of impaired cardiac activity and breathing come to the fore: severe weakness, shortness of breath at rest, palpitations and various arrhythmias, weak pulsation of blood vessels in the periphery and decreased blood pressure, swelling of the legs.
All patients have pronounced congestion in the lungs; in some patients, ascites is combined with effusion into the pleural cavity of a non-tumor nature. With high intra-abdominal pressure, the diaphragm moves the lungs upward, the lower lobes are compressed and lose their airiness - atelectasis is formed. Against the background of swelling of the lung tissue and atelectasis, the bacterial microflora is activated, which manifests itself as sluggish pneumonitis with fever and cough.
As a rule, the appearance of fluid in the abdomen is manifested by an increase in waist circumference, which is combined with a decrease in body weight, so the scales show the same kilograms as before. In fact, the body loses weight, and the person loses weight. The increasing pressure of fluid in the abdominal cavity literally flattens the stomach, reducing its size, causing gastric contents to reflux into the esophagus, which is manifested by constant heartburn and loss of appetite. With intense ascites, the patient can neither drink nor eat - everything is thrown out by the compressed esophagus and stomach. The stool is unstable - constipation alternates with liquid feces, flatulence and seething.
As fluid accumulates, the pain changes localization, its intensity is low, and they mainly complain of heaviness in the lower back.
Stressed ascites is a life-threatening condition, so action must be taken immediately.
Forecast
Ascites in cancer significantly worsens the general well-being of the patient. As a rule, such a complication occurs in the later stages of oncology, in which the survival prognosis depends on the nature of the tumor itself and its distribution throughout the body.
Life expectancy with ascites depends on the following factors:
- Functioning of the kidneys and liver;
- Activities of the cardiovascular system;
- The effectiveness of therapy for the underlying disease.
The development of ascites can be prevented by an experienced doctor observing the patient. Doctors at the Yusupov Hospital have extensive experience in dealing with various types of cancer. Qualified medical personnel and the latest equipment allow for accurate diagnosis and high-quality, effective treatment in accordance with European standards.
Prevention
Prevention of ascites - early detection of a malignant tumor and adequate therapy, regular monitoring after radical treatment of cancer. Ascites can develop many years after treatment for a malignant tumor; high-tech imaging technologies help to detect effusion in a timely manner.
Despite the apparent simplicity and rapid effectiveness of laparocentesis, the treatment of ascites is an extremely complex problem that Euroonco specialists have been successfully solving for many years.
Book a consultation 24 hours a day
+7+7+78
Bibliography
1. Eramishantsev A.K., Lebezev V.M., Musin R.A. Surgical treatment of resistant ascites in patients with portal hypertension // Surgery. - 2003 - No. 4 2. Ivashkin V.T., Mayevskaya M.V./ Treatment of complications of liver cirrhosis: guidelines for doctors //- M.: Litterra. — 2011 — 64 p. 3. Bosch J., Berzigotti A., Garcia-Pagan JC, Abraldes JG /The management of portal hypertension: rational basis, available treatment and future options // J. Hepatol. — 2008 — Vol. 48 - P. 68–93. 4. European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis // J. Hepatol. 2010 Vol. 53 No. 3 P. 5. Lin CH, Shih FY, Ma MH, et al. /Should bleeding tendency deter abdominal paracentesis?// Dig Liver Dis 2005; 37. 6. Pentheroudakis G., Pavlidis N. /Serous papillary peritoneal carcinoma: unknown primary tumor, ovarian cancer counterpart or a distinct entity? A systematic review // Crit Rev Oncol Hematol; 2009, Nov 6.