Diclofenac, 75 mg/3 ml, solution for intramuscular administration, 3 ml, 5 pcs.
Damage to the gastrointestinal tract
When using diclofenac, phenomena such as bleeding or ulceration/perforation of the gastrointestinal tract, in some cases fatal, were observed. These events may occur at any time when using drugs in patients with or without previous symptoms and a history of serious gastrointestinal diseases. In elderly patients
such complications can have serious consequences. If patients receiving Diclofenac develop bleeding or ulceration of the gastrointestinal tract, the drug should be discontinued.
To reduce the risk of gastrointestinal toxicity in patients with gastrointestinal ulcers, especially complicated by a history of bleeding or perforation, as well as in elderly patients
the drug should be used in the minimum effective dose.
Patients at increased risk of developing gastrointestinal complications, as well as patients receiving therapy with low doses of acetylsalicylic acid (Aspirin), should take gastroprotectors (proton pump inhibitors or misoprostol) or other medications to reduce the risk of unwanted effects on the gastrointestinal tract. Patients with a history of gastrointestinal lesions, especially the elderly, should report all abdominal symptoms to the doctor.
Patients with bronchial asthma
Exacerbation of bronchial asthma (NSAID intolerance/NSAID-induced asthma), angioedema and urticaria are most often observed in patients with bronchial asthma, seasonal allergic rhinitis, nasal polyps, chronic obstructive pulmonary disease or chronic respiratory tract infections (especially those associated with allergic rhinitis-like symptoms). In this group of patients, as well as in patients with allergies to other drugs (rash, itching or urticaria), special caution should be observed when using Diclofenac (preparedness for resuscitation measures).
Skin reactions
Serious dermatological reactions such as exfoliative dermatitis, Stevens-Johnson syndrome, toxic epidermal necrolysis, in some cases fatal, have been reported very rarely with the use of diclofenac. The highest risk and incidence of severe dermatological reactions were observed in the first month of treatment with diclofenac. If patients receiving Diclofenac develop the first signs of skin rash, damage to the mucous membranes or other symptoms of hypersensitivity, the drug should be discontinued. In rare cases, in patients who are not allergic to diclofenac, anaphylactic/anaphylactoid reactions may develop when using Diclofenac.
Effects on the liver
Since during the period of use of the drug Diclofenac there may be an increase in the activity of one or more liver enzymes, during long-term therapy with the drug, monitoring of liver function is indicated as a precautionary measure. If liver dysfunction persists and progresses or signs of liver disease or other symptoms (for example, eosinophilia, rash, etc.) occur, the drug should be discontinued. It should be borne in mind that hepatitis during the use of the drug Diclofenac can develop without prodromal phenomena.
Effects on the kidneys
During therapy with Diclofenac, it is recommended to monitor renal function in patients with hypertension, impaired cardiac or renal function, the elderly, patients receiving diuretics or other drugs that affect renal function, as well as in patients with a significant decrease in circulating blood plasma volume of any etiology , for example, in the period before and after major surgical interventions. After cessation of drug therapy, normalization of renal function indicators to initial values is usually observed.
Impact on the cardiovascular system
Therapy with NSAIDs, including diclofenac, particularly long-term and high-dose therapy, may be associated with a small increased risk of serious cardiovascular thrombotic events (including myocardial infarction and stroke).
In patients with diseases of the cardiovascular system and a high risk of developing diseases of the cardiovascular system (for example, with arterial hypertension, hyperlipidemia, diabetes mellitus, smokers), the drug should be used with extreme caution, at the lowest effective dose for the shortest possible duration of treatment, since the risk of thrombotic complications increases with increasing dose and duration of treatment. With long-term therapy (more than 4 weeks), the daily dose of diclofenac in such patients should not exceed 100 mg. The effectiveness of treatment and the patient's need for symptomatic therapy should be periodically assessed, especially in cases where its duration is more than 4 weeks. The patient should be instructed to immediately seek medical attention if the first symptoms of thrombotic disorders (eg, chest pain, shortness of breath, weakness, speech disturbances) appear.
Impact on the hematopoietic system
Diclofenac may temporarily inhibit platelet aggregation. Therefore, in patients with hemostasis disorders, it is necessary to carefully monitor relevant laboratory parameters. With long-term use of the drug Diclofenac, it is recommended to conduct regular clinical tests of peripheral blood.
Masking signs of an infectious process
The anti-inflammatory effect of Diclofenac may complicate the diagnosis of infectious processes.
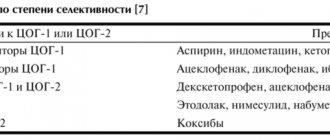
Use simultaneously with other NSAIDs
Diclofenac should not be used concomitantly with other NSAIDs, including selective COX-2 inhibitors, due to the risk of increased adverse events.
Impact on the ability to perform potentially hazardous activities that require special attention and quick reactions (driving vehicles, working with moving mechanisms, etc.)
Patients who experience visual disturbances, dizziness, drowsiness, vertigo or other central nervous system disorders while taking diclofenac should not drive or operate machinery.
Compound
In Diclofenac 5% gel, the active substance - diclofenac sodium - is included in a concentration of 50 mg/g, in 1% - in a concentration of 10 mg/g.
Excipients: isopropyl alcohol, benzyl alcohol, carbomer 940, sodium metabisulfite, polysorbate 80, triethanolamine, purified water. Composition of Diclofenac ointment: Diclofenac sodium (10 or 20 mg/g), propylene glycol, dimethyl sulfoxide, macrogol 400 and 1500.
Composition of Diclofenac injections: Diclofenac sodium (25 mg/ml), sodium metabisulfite, mannitol (E421), benzyl alcohol, sodium hydroxide, propylene glycol, water for injection.
Diclofenac rectal suppositories contain 50 or 100 mg of Diclofenac sodium and solid fat.
Composition of enteric-coated tablets: 25 or 50 mg Diclofenac sodium, disubstituted calcium phosphate, starch, magnesium stearate, polyvinylpyrolidone K30, purified talc, cellulose acetate, indoresin, diethyl phthalate, carmoisin varnish, titanium dioxide, Ponceau 4R varnish, red and yellow iron oxide .
Composition of tablets in p/o: 25 mg Diclofenac sodium, milk sugar, sucrose, povidone, stearic acid, potato starch. Shell: castor oil, cellacephate, titanium dioxide, tropeo-lin O dyes and azorubin.
Composition of retard tablets: 100 mg Diclofenac sodium, hypromellose, hyaetellose, Kollidon SR, sodium alginate, MCC, magnesium stearate. Shell: collicut MAE 100 R, povidone, talc, propylene glycol, titanium dioxide, iron oxide yellow and red.
Composition of eye drops: Diclofenac sodium (1 mg/ml), sodium chloride and dihydrogen phosphate dihydrate, propylene glycol, sodium hydroxide, hydrogen phosphate dodecahydrate and disodium edetate, water for injection.
Diclofenac with alcohol - compatible or not?
Diclofenac and alcohol are incompatible.
Consequences of alcohol with NSAIDs
Drinking alcohol during treatment with NSAIDs can cause:
- deterioration of liver function;
- reducing the effectiveness of the drug;
- development of unpredictable complications and adverse reactions;
- hypertension and, as a consequence, increased congestion in the circulatory system and intoxication of the body.
Injections and alcohol are not compatible, since the injection form of the drug stimulates the activity of the central nervous system, and alcohol, on the contrary, inhibits it. As a result, quite serious neurological disorders are possible.
Pharmacodynamics and pharmacokinetics
The NSAID Diclofenac is a derivative of phenylacetic acid . Its mechanism of action is based on the ability to suppress the biosynthesis of Pg (prostaglandins) - biologically active lipids that are mediators of fever, pain and inflammation.
Like other NSAIDs, it prevents platelet .
The drug is quickly and completely absorbed; food slows down absorption for 1-4 hours (reducing Cmax by 40%). Cmax when taken orally is observed after 2-3 hours. Changes in this indicator are dose-dependent.
The pharmacokinetic profile does not change with repeated administration. If the recommendations for use are followed, it does not accumulate in the body.
Bioavailability – 50%. It is more than 99% bound to plasma proteins (mainly bound to albumin ). Penetrates into the synovium and breast milk.
Half of the dose taken is metabolized during the “first passage” through the liver. The process is based on single or multiple hydroxylation and conjugation with glucuronic acid. Plasma T1/2 - 1-2 hours.
60% of the dose is excreted by the kidneys in the form of metabolic products, less than 1% in its pure form, the rest of the administered drug is excreted in bile.
Interaction
Simultaneous use with:
- lithium preparations , phenytoin or digoxin - helps to increase the plasma concentration of these drugs;
- antihypertensive drugs and diuretics - reduces the effectiveness of these drugs;
- potassium-sparing diuretics - leads to hyperkalemia ;
- GCS or other NSAIDs - causes adverse reactions from the gastrointestinal tract;
- acetylsalicylic acid - helps reduce the serum concentration of diclofenac;
- cyclosporine - increases the nephrotoxic effect of the latter;
- antidiabetic drugs - can provoke hyper- or hypoglycemia ;
- methotrexate - can lead to increased concentrations and increased toxicity of the latter;
- anticoagulants - requires regular monitoring of hemocoagulation .
If indicated, eye drops can be combined with other ophthalmic agents that contain corticosteroids (at least a 5-minute break must be maintained between instillations).
Side effects of Diclofenac
When taken orally, the following side effects are possible: dyspepsia, erosive and ulcerative lesions of the digestive canal, perforation of its walls, gastric and intestinal bleeding, increased drowsiness, dizziness, hypersensitivity reactions, irritability.
After using the drops the following are noted:
- burning sensation;
- corneal clouding;
- impaired clarity of perception (immediately after instillation);
- iritis;
- hypersensitivity reactions.
Side effects of injections
Intramuscular injections of Diclofenac may be accompanied by a burning sensation at the injection site, abscess, and necrosis of adipose tissue.
Diclofenac during pregnancy and breastfeeding
All dosage forms during pregnancy are used in exceptional cases, taking into account the benefit/risk ratio.
Like other NSAIDs, in the 3rd trimester the drug can cause a lack of uterine contraction in a woman in labor and/or premature closure of the ductus arteriosus in a newborn.
The medicine can penetrate not only into milk, but also through the placental barrier, even when using dosage forms for external therapy. Thus, even the use of gel and ointment during pregnancy can disrupt the development of the fetus.
The drug affects fertility, so it is not recommended for women who are planning a pregnancy, as well as for women who have problems with fertilization.
Overdose
An overdose can cause central nervous system disorders and digestive disorders. The first ones most often manifest themselves:
- dizziness and headaches;
- increased excitability;
- clouding of consciousness;
- phenomena of hyperventilation with increased convulsive readiness.
Disorders of the digestive system are manifested by: nausea, abdominal pain, vomiting, gastrointestinal bleeding.
In severe poisoning, liver damage, acute renal failure, respiratory depression, and hypotension are possible.
The drug does not have an antidote. Special measures, such as hemoperfusion , dialysis or forced diuresis , do not guarantee the removal of the drug due to its almost complete binding to plasma proteins and intensive metabolism.
Due to the low systemic absorption of the gel/ointment, overdose is considered unlikely. Accidental ingestion of the gel or ointment may cause systemic adverse reactions.
The patient is prescribed gastric lavage, vomiting is stimulated, and an enterosorbent . Therapy is symptomatic.