Relevance
Fluconosole is an antifungal drug that inhibits cytochrome P451 (CYP51) in fungi, which plays a major role in ergosterol synthesis and fungal cell wall formation. In humans, CYP51 is required for the synthesis of cholesterol required for the formation of embryonic tissues.
Fluconazole is often prescribed as first-line therapy during pregnancy to treat fungal infections.
Researchers from Canada assessed the association between low- and high-dose fluconazole use during pregnancy and the risk of spontaneous abortion, major congenital malformations, and stillbirth.
pharmachologic effect
The abstract contains information that the drug acts as an antifungal agent, specifically inhibiting the synthesis of fungal sterols. Belongs to the class of triazole compounds.
There is a specific effect on fungal enzymes that depend on cytochrome P450. The active substance demonstrates activity against a variety of strains of Candida spp. (including effective against visceral candidiasis), Cryptococcus neoformans (including effective against intracranial infections), Trichophytum spp, Microsporum spp. The drug is also active against microorganisms that are causative agents of endemic mycoses: Coccidioides immitis, Hystoplasma capsulatum, Blastomyces dermatitidis.
The drug stops the conversion of fungal cells into lanosterol into ergosterol. Under its influence, the permeability of the cell membrane increases, the process of its growth and replication is inhibited. It is highly selective for cytochrome P450 of fungi, but in the human body it almost does not inhibit these enzymes. Does not demonstrate antiandrogenic activity.
Pharmacological properties of the drug Fluconazole
Antifungal agent of the class of triazole compounds. Fluconazole has a pronounced antifungal effect and specifically inhibits the synthesis of fungal sterols. It has a specific effect on fungal enzymes dependent on cytochrome P450. Active against various strains of Candida spp. (including visceral candidiasis), Cryptococcus neoformans (including intracranial infections), Microsporum spp. and Trichophytum spp. Fluconazole is also active against pathogens of endemic mycoses: Blastomyces dermatitidis, Coccidioides immitis (including intracranial infections), Hystoplasma capsulatum . After oral administration, it is well absorbed from the digestive tract; the concentration in the blood plasma exceeds 90% of the concentration level achieved with intravenous administration. Eating does not affect the absorption of fluconazole. The maximum concentration in blood plasma is achieved 0.5–1.5 hours after oral administration. The half-life of the drug from blood plasma is 30 hours, which allows the drug to be used once a day during a course of treatment with fluconazole and provides a therapeutic effect for vaginal candidiasis after a single dose of the drug. The concentration of the active substance in the blood plasma is directly proportional to the dose taken. 11–12% of fluconazole is bound to plasma proteins. With a single daily dose of fluconazole on days 4–5, a stable concentration in the blood plasma is achieved in 90% of patients. When a loading (twice daily) dose is administered on the 1st day of treatment, the above effect is achieved by the 2nd day of treatment. The pharmacokinetics of fluconazole when administered intravenously is similar to that when administered orally. Fluconazole penetrates well into all body fluids. In the cerebrospinal fluid, the concentration of fluconazole reaches 80% of its concentration in the blood plasma. Fluconazole is excreted from the body in the urine, 80% unchanged. Fluconazole clearance is directly proportional to creatinine clearance.
Pharmacokinetics and pharmacodynamics
Wikipedia indicates that after oral administration, the drug is actively absorbed into the human gastrointestinal tract. In plasma, the concentration of the active substance is more than 90% of the level that is observed if intravenous administration is practiced. The absorption of the substance is not affected by food intake, so it does not matter how you take it, before or after meals. After taking the medicine orally, the highest concentration in the blood occurs after 0.5–1.5 hours. The half-life from the blood is 30 hours. That is, you can take the product once a day. For vaginal candidiasis, a single dose of the drug is sufficient, for which one tablet or another form of the drug is used.
11–12% of the active substance binds to blood plasma proteins. When the drug begins to work depends on the treatment regimen. If you take the medicine once daily, then a stable concentration of the active component in the human blood is observed on the fourth or fifth day (in 90% of people). If on the first day of treatment the patient is given a double daily dose, then this effect is observed already on the second day of treatment.
Penetrates into all fluids in the body. It is excreted from the body through the kidneys, approximately 80% is excreted unchanged.
Pharmacokinetics
After oral administration, fluconazole is well absorbed; food intake does not affect the rate of absorption of fluconazole, its bioavailability is 90%.
The time to reach maximum concentration after oral administration of 150 mg of the drug on an empty stomach is 0.5–1.5 hours, Cmax is 90% of the plasma concentration when administered intravenously at a dose of 2.5–3.5 mg/l. T1/2 of fluconazole is 30 hours. Communication with plasma proteins is 11–12%. Plasma concentration is directly dependent on dose. A 90% level of equilibrium concentration is achieved by the 4th–5th day of treatment with the drug (when taken once a day).
Administration of a loading dose (on the first day), 2 times higher than the usual daily dose, allows one to achieve a concentration level corresponding to 90% of the equilibrium concentration by the second day.
Fluconazole penetrates well into all biological fluids of the body. Concentrations of the active substance in breast milk, joint fluid, saliva, sputum and peritoneal fluid are similar to its levels in plasma. Constant values in vaginal secretions are achieved 8 hours after oral administration and are maintained at this level for at least 24 hours. Fluconazole penetrates well into the cerebrospinal fluid (CSF) - with fungal meningitis, the concentration in the CSF is about 85% of its level in plasma. In sweat fluid, epidermis and stratum corneum (selective accumulation) concentrations exceeding serum levels are achieved. After oral administration of 150 mg on the 7th day, the concentration in the stratum corneum of the skin is 23.4 mcg/g, and 1 week after taking the second dose - 7.1 mcg/g; concentration in nails after 4 months of use at a dose of 150 mg once a week is 4.05 mcg/g in healthy and 1.8 mcg/g in affected nails. The volume of distribution approaches the total water content of the body.
It is an inhibitor of the CYP2C9 isoenzyme in the liver. It is excreted primarily by the kidneys (80% unchanged, 11% in the form of metabolites). Fluconazole clearance is proportional to creatinine clearance. No fluconazole metabolites were detected in peripheral blood.
The pharmacokinetics of fluconazole depends significantly on the functional state of the kidneys, and there is an inverse relationship between the half-life and creatinine clearance. After hemodialysis for 3 hours, the concentration of fluconazole in plasma decreases by 50%.
Indications for use
The following indications for use of the drug are determined:
- infectious diseases caused by candida ( disseminated candidiasis , generalized candidiasis , other forms of invasive candidiasis ;
- candidiasis of the mucous membranes (including the pharynx, oral cavity, esophagus);
- candiduria;
- chronic atrophic and mucocutaneous candidiasis of the oral cavity (develops in people with dentures);
- non-invasive bronchopulmonary infections;
- genital candidiasis ( vaginal candidiasis in acute form and with relapses);
- prevention of recurrent manifestations of vaginal candidiasis (if the disease develops three times a year), candidal balanitis ;
- cryptococcal infection, cryptococcal meningitis;
- onychomycosis;
- dermatomycosis (including mycoses of the body, feet, groin area);
- pityriasis versicolor;
- endemic mycoses deep;
- prevention of the development of fungal infections in people who have undergone cytostatic or radiation therapy.
Currently, the problem of mycotic diseases is acquiring important social significance. The increase in the incidence of mycoses is associated with many factors, primarily with the active use of antibacterial drugs in medical practice, which undoubtedly increases not only the incidence of candidiasis, but also mycoses caused by filamentous fungi. This is also facilitated by the use of cytostatics, corticosteroids and other drugs with immunosuppressive properties. The development of mycosis is promoted by a combination of many reasons associated with the urbanization of modern life of the population [1–4].
The wide distribution of fungi in nature, their constant presence both in the environment and in the body, makes contact and infection of humans inevitable. Particularly alarming is the increase in the number of patients with deep mycoses, which include some mycoses of the ENT organs.
Currently, approximately 100,000 species of microscopic fungi have been identified, of which more than 400 species are capable of causing infections in humans, but about 100 species are of real importance in clinical practice [5].
An analysis of clinical and laboratory studies conducted at the Moscow Scientific and Practical Center of Otorhinolaryngology showed the increasing importance of fungal pathology among general ENT morbidity. So, in 2010-2011. among patients with chronic inflammatory pathology of the ENT organs who applied to the mycology room of the Center’s advisory department, fungal infection was detected in 23% [6].
In this regard, the problem of mycoses of the ENT organs remains relevant, which determined the purpose of this work: to familiarize otorhinolaryngologists with modern principles of diagnosis and treatment of mycoses of the upper respiratory tract and ear, varying in localization and nature of clinical manifestations.
Nosological forms of fungal diseases of the ENT organs are otomycosis, pharyngomycosis, laryngomycosis, fungal infection of the nasal cavity and paranasal sinuses. There are superficial mycoses, which affect the skin, mucous membrane, external auditory canal, pharyngeal cavity, and deep mycoses affecting, for example, the SNP, the postoperative cavity of the middle ear, accompanied by invasion of the fungus not only into the epithelium, but also into surrounding tissues.
According to our data, in recent years, the frequency of detection of pharyngomycosis is 45%, otomycosis - 42%, mycosis of the nasal cavity and SNP - 8%, laryngomycosis -5% among all patients with mycosis of the ENT organs [3, 7].
The proportion of otomycosis among otitis of other etiologies reaches 25.3%, pharyngomycosis in chronic pharyngitis and tonsillitis - 26%. Fungal infection of the larynx in chronic laryngitis reaches 15%; in chronic inflammation of the nose and SNP, the share of the fungal process is 7%.
External fungal otitis, fungal otitis media and fungal infection of the postoperative middle ear cavity occur in 69, 18 and 13% of cases of otomycosis, respectively. The main causative agents of external fungal otitis are molds of the genus Aspergillus
(65%),
Penicillium
(5%), with mycosis of the postoperative cavity the proportion of mold fungi reaches 95%, while with fungal otitis media, yeast-like fungi of the genus
Candida
(79%).
In some cases, fungal diseases of the ears can be caused by fungi of the genera Mucor, Alternaria
, etc. In 17% of cases, we noted a combined infection with
Aspergillus
spp.
and Candida
spp.
in combination with representatives of Staph.
spp and
Pseudomonas
spp.
Infection with two or more species of fungi Aspergillus
spp.
+ Candida
spp.,
Aspergillus
spp.
+ Candida
spp.
+ Alternaria alternata
occurs in 1% of observations.
Candida are the leading pathogens
(97-99% of observations).
In mycosis of the nasal cavity and SNP, mold fungi account for up to 78% of the lesions. The main pathogen is a fungus of the genus Aspergillus
, species -
fumigatus
and
niger
, in some cases, in immunocompromised patients, fungal diseases of SNP can be caused by fungi of the genera
Mucor, Alternaria, Rhizopus, Rhizomucor
, etc.
Basically, all these types of fungi belong to the group of opportunistic fungi and cause disease only under certain conditions that predispose to the development and reproduction of fungi, ensuring their transition from saprophyte to the realization of pathogenic properties.
Among the risk factors for the development of mycoses of the ENT organs, the leading positions are occupied by iatrogenic immunodeficiency states that develop as a result of massive antibiotic therapy, long-term use of glucocorticoid and immunosuppressive drugs for oncological and autoimmune diseases. Mycoses of the ENT organs often accompany severe somatic pathologies, such as HIV infection and AIDS, diabetes mellitus, thyroid dysfunction, agranulocytosis, anemia, bronchial asthma, etc.
The pathogenesis of mycosis consists of adhesion (attachment of the fungus to the surface of the mucous membrane or to the skin), colonization of fungi and their invasive growth. In severe forms of ENT mycosis, the next stage is the generalization of the process: the penetration of fungi into the blood with dissemination and the appearance of secondary foci of mycosis in various organs and tissues. This is especially true for fungi of the genus Aspergillus
spp., the pathogenicity factor of which is their ability to grow at 37 °C, the presence of enzymes (protease, phospholipase), toxins (aflatoxin, fumagillin, etc.), pronounced angioinvasiveness and the ability to evade immune surveillance due to the production of inhibitors of the phagocytic function of macrophages and neutrophils, for example gliotoxin [1, 5].
A factor contributing to the development of otomycosis is, first of all, trauma. When the skin and mucous membrane are damaged, paths are opened for the fungus to penetrate deep into the tissues, and protective reactions at the site of damage are weakened. In addition, the secreted secretion of the injured integumentary epithelium is a good nutrient medium for the proliferation of fungi. Thus, a paradoxical phenomenon has been noted: fungal diseases of the outer ear more often occur in extremely careful people who intensively use cotton swabs and other objects to clean their ears, injuring the skin of the external auditory canal and often causing traumatic invasion of the pathogen. Speaking about the need for proper, gentle removal of excess sulfur, it should be remembered that its presence in a small amount in the ear canal is necessary, since it not only mechanically protects the skin, but also carries out bactericidal and fungicidal functions.
The occurrence of a fungal infection of the outer ear is often preceded by water entering the ear during bathing or removing wax plugs by washing. Long-term local use of glucocorticoid drugs, antibiotics, and antiseptics for otorrhea, which accompanies a purulent-inflammatory process in the middle ear, leads to the development of otomycosis in 20% of cases.
Surgical sanitation of the middle ear in the absence of a positive effect from previous courses of antibacterial therapy, local and physiotherapeutic conservative treatment often entails the development of fungal infection of the postoperative cavity. Perhaps in such cases there is undiagnosed fungal otitis media. Surgical treatment in this case can be performed only after negative repeated mycological studies.
Otomycosis can also develop when working in dusty conditions and in pressure complexes with high pressure and humidity.
Fungal infection of the pharynx and larynx often develops in patients after massive high-dose antibacterial therapy, long-term systemic use at a dose exceeding 0.3 mg/kg/day (in terms of prednisolone) for more than 3 weeks, and local use of inhaled forms of corticosteroids for hormone-dependent bronchial asthma. A stay in the intensive care unit for more than 10 days, accompanied by laryngeal intubation for more than 5 days, significantly increases the risk of developing mycoses. Smoking, the use of removable dentures and their improper treatment contribute to the development of mycosis of the pharynx and larynx.
Mycosis of the nasal cavity as an independent disease is extremely rare, usually due to trauma to the nasal mucosa in HIV-infected people. More often, the fungal process affects the maxillary sinuses after foreign bodies enter them (filling material when filling the canals of the 4th-7th teeth of the upper jaw).
Complaints and clinical manifestations of mycosis of the ENT organs
are determined by the characteristics of vegetation and parasitism of certain types of fungi and are largely determined by the localization of the pathological process.
In all forms of mycotic diseases of the upper respiratory tract and ear, there is a specific discharge in the form of crusts, plaques, thick caseous or liquid secretions, the color, quantity and consistency of which depend on the type of fungus and the phase of its development. The clinical picture, despite the diversity of pathogens, has a number of specific features. Main complaints with mycotic otitis media
- discharge from the ear, formation of “plugs” in the external auditory canal, itching, pain, ear congestion.
Thus, with otomycosis caused by dermatophytes, the skin of the auricle, postauricular area and external auditory canal is mainly affected. Patients are concerned about itching and peeling of the skin of the affected area. In the external auditory canal there is dry discharge in the form of plaque and films. Inflammatory phenomena are not expressed. Accelerated formation of sulfur plugs was noted.
For otomycosis caused by mold fungi ( Aspergillus, Penicillium, Mucor
etc.), the skin of the external auditory canal, the postoperative cavity, and less often the middle ear cavity and the skin of the auricle are affected. The patient experiences severe pain, severe hearing loss, and dizziness. The discharge looks like “wet newspaper.” The symptoms of inflammation are significantly pronounced. After removal of the pathological discharge, granulations are visualized, the skin is damaged and bleeds easily. The disease can occur as necrotizing external otitis with damage to the bones of the skull.
With candidal otomycosis, the middle ear cavity and the skin of the external auditory canal are affected. Upon examination, maceration and infiltration, reminiscent of weeping eczema, are determined. The process often spreads to the skin of the auricle and the area behind the ear. Pain and itching are moderate. Some patients in the acute stage may have complaints of increased body temperature, headache, increased sensitivity of the auricle and postauricular area.
Mycotic otitis media and mycosis of the postoperative cavity are characterized by the following clinical manifestations: hearing loss, noise in the ear, pain, discharge from the ear, periodic itching, congestion and dizziness.
Otomycosis, like other types of specific inflammation, has a chronic course with a subtle onset of the disease, its gradual development and significant duration. The development of a fungal disease is possible at any age; frequent exacerbations and relapses of the disease during treatment are typical.
For fungal infections of the pharynx
patients complain of discomfort in the throat, burning sensation, dryness, rawness, and soreness, which may be more pronounced than with bacterial pharyngitis. Painful symptoms are moderate; when swallowing and eating irritating foods, the pain intensifies. Sometimes patients note irradiation of pain in the submandibular region, on the anterior surface of the neck and in the ear. Depending on the degree of damage, pseudomembranous, hyperplastic, granulomatous and erosive-ulcerative clinical forms of pharyngomycosis are distinguished. Specific signs of the clinical picture of pharyngomycosis are the presence of plaque, swelling of the mucous membrane and pronounced general symptoms of intoxication; frequent (up to 10 times a year) exacerbations are also characteristic.
For fungal infection of the larynx
patients are worried about pain in the throat and on the front surface of the neck, a feeling of “rolling a lump” in the throat and neck, not associated with swallowing, constant hoarseness, rapid fatigue of the voice, and an unproductive cough. On examination, congestive hyperemia of the mucous membrane of the larynx, swelling of the mucous membrane of the vocal folds, and fibrin deposits are characteristic, when removed, the eroded surface is exposed. Often the fungal process is one-sided, which must be differentiated from cancer and tuberculosis.
Fungal infection of the nose and SNP
divided into invasive and non-invasive forms. Invasive forms include acute (fulminant) and chronic forms. Non-invasive ones include fungal body and allergic fungal sinusitis.
Invasive forms of fungal infection of the SNP are extremely unfavorable in predicting the outcome of the disease. The fulminant form of SNP damage is most often caused by fungi belonging to the class Zygomycetes. This form of the disease occurs in patients with severe immunodeficiency, decompensated diabetic ketoacidosis, neutropenia, and burn disease. Zygomycosis is characterized by an extremely severe course and, without active antifungal therapy and early surgical treatment, usually ends in death.
The chronic form occurs as chronic sinusitis with reactive phenomena from surrounding tissues. Accompanied by copious purulent nasal discharge in the morning, severe pain in the projection of the affected SNP.
The fungal body is quite often a “diagnostic finding” when performing a CT scan of the ED and in some patients is asymptomatic.
With allergic fungal sinusitis, in addition to polyps in the nasal cavity and SNP, a thick, viscous secretion is detected in the lumen of the latter.
Lack of awareness among otorhinolaryngologists regarding the diagnosis of fungal infection of the ENT organs is often the reason for their late and/or incorrect diagnosis. This creates difficulties in treatment and leads to a chronic course of the disease.
Diagnosis of fungal disease of ENT organs
, like any infectious disease, is established only on the basis of complex laboratory mycological research methods. A pronounced clinical picture of a disease similar to a fungal infection, no matter how characteristic it may be, is not the basis for making a final diagnosis of mycosis.
Diagnosis of mycosis is carried out in the following areas:
1. Microscopy of pathological discharge.
2. Inoculation of pathological discharge on various elective nutrient media to isolate fungal cultures and their generic and species identification.
3. Determination of the sensitivity of isolated fungi to antifungal drugs.
4. Radiation diagnostics in cases of damage to the nose and special organs.
Sampling of biological material from the ear is carried out using an attic probe or a Volkmann spoon. Pathological discharge from the deep parts of the external auditory canal is placed between two fat-free sterile slides and microscoped at 100, 200 and 400 times magnification.
In the active stage of aspergillosis and mucorosis with abundant formation of mycotic masses with aerial mycelium, we recommend using an operating otorhinolaryngological microscope (otomicroscopic method of express diagnostics) for diagnosis.
If a fungal infection of the pharynx and larynx is suspected, microscopy of scrapings from the mucous membrane of the oral cavity, pharynx, tonsils, taken with a swab to detect elements of the fungus, and seeding of material from the affected areas of the mucous membranes are performed.
The main method for diagnosing mycosis of SNP is culture of aspirate or rinsing water (puncture using a Kulikovsky needle according to the usual method) with mandatory identification of the pathogen. A histological examination of the biopsy material is also carried out.
In addition to microscopy of native material, microscopic examination of preparations stained using the Romanowsky-Giemsa method is performed. The most informative method that reliably identifies the causative agent of the disease is staining the preparation with solutions of calcofluor white, followed by fluorescent microscopy. For mycological diagnosis, pathological material is inoculated on elective media (Saburo, Chapek, wort agar, etc.). Types of yeast-like fungi of the genus Candida
determined by morphological characteristics and the nature of fermentation of sugars. Inoculation of the material is carried out using the standard method [1, 2, 5]. To clarify the diagnosis, in some cases it is necessary to carry out serological, allergological and histological studies [2, 5].
Treatment
You should always start with eliminating the pathogen. Correction of general and local predisposing factors is carried out in parallel or in the second stage.
When treating a patient with mycosis of the ENT organs, it is necessary to take into account all possible conditions under which this disease arose specifically in this patient with a view to their possible elimination. It is necessary to identify and treat diabetes mellitus, blood diseases, gastrointestinal tract, and immune deficiency. The role of allergies in the pathogenesis of the disease should be taken into account, since mushrooms have pronounced allergenic properties, and hyposensitizing therapy should be carried out in parallel with etiotropic therapy.
Selection of rational antifungal therapy for mycosis of ENT organs
presents certain difficulties. On the one hand, a large number of antimycotic drugs expands the possibilities of treating fungal infections that differ in both localization and type of pathogen. On the other hand, it requires the clinician to have increased awareness of the spectrum and characteristics of their action (fungicidal or fungistatic), pharmacokinetics, compatibility with antibacterial drugs, side effects, etc. The ideal treatment is with an antimycotic that has the least toxic and greatest therapeutic effect, which is not always possible, especially in acute forms of fungal disease, when the choice of drug is made empirically, since the pathogenic fungus is not immediately identified and tests can take a long time. Determining the choice of drug are the results of laboratory mycological studies of the sensitivity of fungi isolated from a particular patient to known antifungal drugs.
Fungal disease of the oropharynx - pharyngomycosis is caused mainly by yeast-like fungi of the genus Candida
, which largely determines treatment tactics. Limited acute candidiasis of the tonsils, which developed as a result of antibacterial therapy, usually heals quickly after stopping the administration of antibiotics and performing only local antifungal treatment. However, widespread lesions of the mucous membrane of the oropharynx, with a tendency to chronicity and recurrence, require a long course of treatment using local and general antimycotic therapy. For systemic therapy, a drug from the azole group, fluconazole (mycoflucan), is used orally at a dose of 100-200 mg once a day. Treatment should be continued for another 14 days after clinical improvement. If such treatment is ineffective, itraconazole (200 mg per day orally) or amphotericin B (1 ml 4 times a day orally, or >0.3 mg/kg per day intravenously) is used [1, 8-10].
In the systemic treatment of pharyngomycosis caused by molds, it is advisable to use itraconazole and amphotericin B, which have a fungicidal effect not only on yeast-like fungi, but also on mold fungi of the genera Aspergillus, Mucor, Penicillium
[12].
In addition to systemic treatment, local treatment is also recommended. During treatment, the pharynx after meals should be lubricated with a solution of clotrimazole at a rate of 10 mg 5 times a day, or nystatin tablets should be dissolved/chewed after meals at a dose of 250-500 thousand units 4-5 times a day. For chronic tonsillitis of fungal etiology, courses of washing the lacunae of the tonsils every other day or 1-2 times a week at least 10 times with solutions of antiseptics with antifungal action (miramistin, quinozol, clotrimazole solution) [10, 11].
Drug therapy for mycosis of SNP always accompanies and/or precedes surgical treatment. In the treatment of fungal infections of the nose and SNP, both general and local measures are provided. For invasive forms of fungal infection of the maxillary sinuses, the most effective is a combination of drug antifungal and surgical treatment. To eliminate the Aspergillus infection at this location, surgical treatment is almost always necessary. Surgical intervention consists of performing radical surgery on the affected sinus using the extranasal method with complete removal of all pathologically altered tissues. In the postoperative period, daily rinsing with antiseptics and antimycotics (amphotericin B, miramistin, pimafucin suspension, clotrimazole) is carried out.
In acute toxic forms of invasive aspergillosis of SNP, antifungal therapy is mandatory. Voriconazole or lipid amphotericin B is used [1, 13]. It is possible to use caspofungin and amphotericin B. After stabilization of the process, treatment with itraconazole. The duration of use of antimycotics depends on the clinical picture of the disease and its course, but should continue for at least 14 days after clinical and laboratory cure [1, 2, 9].
For candidiasis of the nose and SNP, it is necessary to combine the use of systemic antifungals with local antifungal drugs. The drug of choice is fluconazole (mycoflucan), which is prescribed once a day at a dose of 50-200 mg. The course of therapy cannot be less than 14 days. If treatment with standard doses of fluconazole is ineffective, it is possible to increase the dosage to 400 mg/day, or prescribe itraconazole 200 mg/day [10].
Patients with allergic fungal sinusitis are advised to undergo surgery to completely remove the polypous mucous membrane and the viscous “rubber-like” contents of the sinus [1, 13]. In the early postoperative period, it is necessary to wash the SNP twice with an aqueous solution of amphotericin B. It is advisable to prescribe topical nasal corticosteroids to prevent relapse no earlier than 20 days after surgery.
Only in case of resistance to other antimycotics, amphotericin B is used for the treatment of candidal lesions of the nose and SNP (intravenous 0.3 mg/kg per day for 3-7 days). Treatment is carried out under the supervision of biochemical studies of liver and kidney function, since amphotericin B has a pronounced nephro- and hepatotoxic effect.
The specificity of the treatment of fungal infection of the larynx is the widespread use of the inhalation method for administering drugs. The effectiveness of the aerosol method for inflammatory diseases of the larynx is determined by the direct effect of the drug on the site of the disease and the higher concentration of the drug at the site of the lesion. With this method of administration, inhalations with the water-soluble sodium salt of nystatin or levorin are effective, especially for candidiasis. Treatment is carried out for 15-20 minutes 1-2 times a day. The initial course of treatment is 12-15 procedures. In case of resistance to other antimycotics, 12-15-day courses of aerosol therapy with amphotericin B are carried out. All patients with laryngomycosis, in addition to inhalation therapy, must undergo systemic therapy with antimycotics. The drug of choice is fluconazole (mycoflucan) once a day at a dose of 100-200 mg, in severe cases - 300 mg/day) [11]. For patients whose fungal disease in the larynx is accompanied by the formation of a large amount of viscous secretion, it is advisable to carry out inhalations with proteolytic enzymes that selectively break down necrotic masses and dilute the viscous exudate for their better removal. For this, inhalations with chemopsin and chemotrypsin (150 mg in 5 ml of saline) can be recommended.
When treating otomycosis, local and systemic drugs are used. For local treatment of mold lesions in the ear, the most effective are naftifine, nitrofungin, terbinafine (exifin), and for candidiasis - clotrimazole, terbinafine (exifin), naftifine. An indispensable condition for local therapy is preliminary thorough cleaning of the ear using endoscopic equipment or an operating microscope. Ear toileting is performed only by a doctor using an attic probe and a padded cotton pad moistened with an antimycotic drug. Thorough toileting of the ear is given special importance, since even a small amount of mycotic masses significantly lengthens the course of treatment until complete recovery.
In case of external fungal otitis, it is necessary to thoroughly clean the anterior inferior part of the external auditory canal. In case of fungal otitis media, mycotic masses are completely removed from the area of perforation of the eardrum. The postoperative cavity of the middle ear is cleaned in the same way - the entire cavity is thoroughly cleaned, especially in the posterior section, behind the spur. Before treatment, if polyps and granulations are present, they are removed or extinguished with a 20% solution of silver nitrate.
Local treatment with antifungal drugs must be carried out for at least 3-4 weeks under mandatory laboratory control (cultures before, during and after the end of the course of treatment). Local treatment is carried out by placing cotton wool moistened with a fungicidal preparation into the ear, which is left for 5-10 minutes 2-4 times a day, depending on the activity of the fungal process.
For systemic therapy of candidal lesions, the most effective is fluconazole (mycoflucan) - 50-200 mg per day for 14 days. For mold mycoses - itraconazole 200 mg/day for 14 days, terbinafine (exifin) - 250 mg/day for 16 days. If necessary, the course of treatment is repeated after 7 days.
The criterion for the effectiveness of treatment is complete clinical cure within a month, confirmed by both the clinical picture and negative results of mycological research [1, 9].
Quite often, with otitis externa, only a local effect on the mycotic focus of infection is carried out, while with fungal otitis media and mycosis of the postoperative cavity, systemic therapy is mandatory.
Since fungal diseases of the upper respiratory tract and ear are prone to recurrence, dynamic follow-up of the patient is necessary for timely implementation of preventive courses of antifungal treatment. Analysis of our own results of treating patients with ENT mycoses using the above drugs allows us to conclude that they are highly effective, accompanied by the elimination of fungi that cause the disease and normalization of the clinical picture [7, 8, 10].
In general, with proper treatment of mycoses of the ENT organs, therapy is quite effective. Unsatisfactory results are largely explained by the lack of awareness of doctors about the clinical manifestations of mycoses, incorrect diagnostic tactics, as a result of which adequate etiotropic treatment is delayed and carried out at a later stage, when the disease has already spread and become chronic.
Contraindications
There are the following contraindications for the use of this medicine:
- manifestation of high sensitivity to fluconazole or to azole compounds, which are similar in chemical structure to fluconazole;
- concurrent use of terfenadine if the patient receives a dose of Fluconazole 400 mg per day or more;
- concomitant use of astemizole or any other drugs that increase the QT interval;
- age up to 4 years.
It should be taken with caution in case of liver failure, also kidney failure, when a rash appears in people suffering from a superficial fungal infection, in potentially pro-arrhythmogenic conditions in people with risk factors (organic heart disease, taking medications that provoke the development of arrhythmia , electrolyte imbalance). How to take Fluconazole in this case, you should definitely ask a specialist.
Side effects
When treated with the drug, the patient may develop the following side effects:
- abdominal pain, diarrhea ;
- headache;
- nausea , flatulence ;
- skin rash;
- hepatotoxic effects;
- anaphylactic reactions.
How to take the medicine when such effects occur, and whether it is worth continuing treatment, should be individually consulted with a doctor.
general description
Fluconazole is an antifungal drug effective against fungus and yeast.
It is commonly used for skin infections, nail bed fungus, and more intense fungal infections including blastomycosis and histoplasmosis. Fluconazole is related to ketoconazole but is able to cross the blood-brain barrier more effectively, making it more successful in treating fungal infections of the central nervous system.
Fluconazole is also effective against ringworm, but is usually used for more serious infections.
Fluconazole has fewer side effects than most other antifungals.
Dosage
The dosage of a medicine for a specific living creature is determined by a veterinarian based on a variety of data - the weight and age of the animal, previous diseases, medications taken and much more.
Do not self-medicate if you do not want to lose your pet! Contact your veterinarian!
How does it work
Fluconazole acts by inhibiting the production of the fungal cell wall. This causes the fungus to become structurally inadequate so that it leaks and dies.
Storage Information
Tablets should be stored in a tightly closed container at room temperature. Oral liquids should be refrigerated and shaken before use.
Missed dose?
Give the dose as soon as possible. If it is almost time for your next dose, skip the missed dose and continue with your regular schedule. Do not give your pet two doses at once.
Side effects and reactions to medications
Fluconazole has been found to be very safe for pets, but has not been studied. The following side effects have been reported in people taking this drug:
- Allergic reaction (difficulty breathing, hives, etc.)
- Vomit
- Diarrhea
- Skin rash
- Loss of appetite
- Dark urine or jaundice due to liver failure
- Pale tongue, gums and nose
Please contact your veterinarian and discontinue use of fluconazole if any of these reactions occur.
Instructions for use of Fluconazole (Method and dosage)
The drug is prescribed for oral administration (Fluconazole Stada capsules, Fluconazole Teva, tablets) or for intravenous administration. There are also other forms of medication, the active ingredient of which is fluconazole - suppositories, ointment.
The solution is infused at a rate not exceeding 10 ml per minute.
Fluconazole tablets, instructions for use
The dosage of the drug depends on the disease and its severity.
Patients with disseminated candidiasis and candidemia are prescribed 400 mg on the first day, then the dose should be reduced to 200 mg. For the treatment of generalized candidiasis, are advised to take 6–12 mg per 1 kg of weight per day.
For patients with oropharyngeal candidiasis , 50 mg to 100 mg of Fluconazole is indicated once a day, the treatment period is 1-2 weeks.
People suffering from atrophic candidiasis of the oral mucosa are advised to take 50 mg once a day. Treatment is combined with the use of local products for the treatment of prostheses. When treating other candidiasis infections of the mucous membranes, 50–100 mg per day is prescribed, the period of therapy is from 14 to 30 days.
In order to prevent the development of relapses of oropharyngeal candidiasis in people with AIDS , 150 mg once a week is indicated. If mucosal candidiasis develops in children, the dose should be taken at the rate of 3 mg of drugs per 1 kg of weight per day. On the first day, you can give your child a double dose.
Patients with cryptococcal infections and cryptococcal meningitis are usually prescribed 200–400 mg of drugs once a day. On the first day, 400 mg of the drug is indicated. The duration of treatment can be from 6 to 8 weeks. Children are prescribed a dose of 6–12 mg per 1 kg of weight per day.
People suffering from infectious skin diseases are recommended to prescribe 150 mg once a week or drink 50 mg of the drug once a day. Treatment should be continued for 2-4 weeks. For men and women with mycosis of the feet , longer therapy is sometimes required - up to 6 weeks.
Patients with pityriasis versicolor are recommended to take 300 mg once a week, the treatment period is 2 weeks. Depending on the intensity of your symptoms, your doctor may prescribe another dose of Fluconazole in the third week. It is possible to use another treatment regimen - 50 mg 1 time per day, the treatment period is two to four weeks.
Patients with onychomycosis are prescribed 150 mg once a week. Therapy should continue until a healthy nail grows in place of the diseased nail.
People suffering from deep endemic mycosis sometimes undergo a long course of treatment with the drug, which can last up to two years. The dose per day is 200–400 mg.
Instructions for the use of fluconazole for thrush stipulate that for vaginal candidiasis, a single dose of the drug is taken, its dose is 150 mg.
As a rule, Fluconazole for thrush is effective after a single dose. But your doctor will tell you more about how to take Fluconazole for thrush after an individual consultation. Before determining how to take any medicine for thrush if you have thrush, the specialist takes into account the causes of the disease and the individual characteristics of its course. For chronic thrush, Fluconazole Teva or other types of the drug are prescribed to prevent relapses at a dose of 150 mg once a month. The product should be used for 4-12 months. For the purpose of prevention, capsules are prescribed in a dose of 50–400 mg once a day, depending on how high the risk of the disease is. For children with thrush, Fluconazole tablets are prescribed at a dose of 3–12 mg of medication per 1 kg of weight per day. How much to drink depends on the severity of the infection.
For balanitis, the treatment regimen for men is as follows: the drug should be taken in a dose of 150 mg once.
Some patients are interested in whether it is possible to take pills or capsules during menstruation. According to experts, you can take Fluconazole at any time, regardless of your monthly cycle. How long it takes for the medicine to help depends on the intensity of the symptoms of the disease.
The use of fluconazole for the treatment of fungal infections in urology
Alyaev Yu.G., Grigoryan V.A., Sultanova E.A., Allenov S.N., Shpot E.V.
Infections caused by yeast-like fungi of the genus Candida (Candida spp.) are the most common of all fungal infections Candida is often the causative agent of nosocomial infections and extremely rarely of community-acquired infections in patients without urinary disorders. The increasing importance of infections caused by fungi of the genus Candida is associated with the widespread use of invasive diagnostic and treatment , immunosuppressive therapy and antimicrobial drugs with a broad spectrum of antibacterial activity [1–4].
Asymptomatic candiduria and candidal cystitis in women
The detection of candida in urine is called candiduria. Candiduria is rarely found in healthy people. Risk factors for candiduria include:
- Diabetes mellitus (DM). In patients with diabetes, the risk of uroinfections caused by fungi increases significantly. Diabetes is a predisposing factor for candiduria, since in patients with glucosuria, the intensity of fungal growth increases, resulting in active colonization of the women’s vagina by fungi of the genus Candida. Additional risk factors include decreased phagocytic activity and nonspecific resistance, as well as urinary retention in patients with a neurogenic bladder [5]. In addition, patients with diabetes are more often subjected to instrumental studies and receive antibacterial drugs.
- Antibacterial therapy. In 30% of healthy individuals, Candida colonizes the mucous membrane of the gastrointestinal tract. However, in patients receiving antibiotics, colonization rates can reach 100% [6]. There is no evidence that the administration of antibiotics directly leads to an increase in the proliferation or virulence of Candida, however, there is evidence indicating that suppression of the endogenous flora by antibiotics leads to Candida colonization of the intestines, genital tract, and urethra [6].
- Bladder catheterization. A catheter inserted into the bladder is the point of entry for microorganisms into the urine collection system. All long-standing catheters are necessarily colonized by flora [7].
- Other risk factors. Other risk factors for candiduria are older age, female gender [8], the use of immunosuppressive drugs, radiation therapy, the installation of intravenous catheters, obstruction of urine outflow, and tuberculosis of the genitourinary system [6].
Asymptomatic candiduria, as a rule, is discovered by chance, is not accompanied by clinical manifestations and does not require treatment , except for the presence of risk factors for generalization of infection .
At urological clinic, we treated asymptomatic candiduria in 15 patients: 9 patients suffered from diabetes (and their blood glucose levels were not sufficiently corrected); 2 patients had recently undergone chemotherapy for breast cancer, 4 patients were diagnosed with severe bladder dysfunction such as detrusor hypotension.
All patients were treated with fluconazole 150 mg orally, once.
As a rule, a single dose of the drug was sufficient to eliminate candiduria. Repeated use of fluconazole was required in only 1 patient suffering from diabetes. The absence of candiduria was confirmed by double bacteriological examination of urine performed at an interval of 2 weeks.
Candidal cystitis, in addition to candiduria, is accompanied by the usual signs of inflammation of the bladder: pain during urination of varying severity, pain in the suprapubic region, frequent urination in small portions, burning in the external genital area, terminal gross hematuria.
At urological clinic we examined 58 of the following patients:
- in 48 of them, cystitis had a mixed etiology (i.e., bacteria of the predominantly intestinal group were sown at a titer of >103 CFU/ml in combination with fungi of the genus Candida at a titer of >104 CFU/ml);
- In 10 patients, bacteriological examination of urine revealed only Candida fungi in a titer of 104 to 108 CFU/ml.
Patients in this latter group received long-term therapy with broad-spectrum antibiotics for chronic recurrent cystitis without sufficient antifungal prophylaxis.
All patients were treated taking into account the sensitivity of the microflora. Patients with cystitis of mixed etiology were prescribed an antibacterial drug in combination with fluconazole :
- antibacterial drug + fluconazole orally 100–200 mg/day. (depending on the Candida titer and duration of antibacterial therapy), 7–14 days.
Patients with candidal cystitis were prescribed fluconazole as monotherapy according to the regimen given above.
It should be noted that the treatment of candiduria turned out to be effective in 100% of cases, which is confirmed by the results of a double bacteriological examination of urine performed at an interval of 2 weeks.
Candidal balanoposthitis and urethritis in men
Candidal balanoposthitis is one of the most common mycotic infections of the penis [9]. In addition to independent damage and development of balanoposthitis, there is a secondary addition of candidiasis infection against the background of already existing balanoposthitis of a different etiology. The clinical picture of balanoposthitis caused by Candida fungi is manifested by the presence of patchy erythema, swelling of the skin, and the appearance of erosive and ulcerative elements, while the pathological process can spread to the skin of the scrotum. Data from microscopic and bacteriological studies allow us to establish the correct diagnosis [9].
One of the routes of infection for candidal balanoposthitis is sexual, but the presence of endocrinopathies (DM, thyroid disease, obesity, etc.), a decrease in the body’s immunological reactivity and other factors are of decisive importance.
The urological clinic has experience in treating 327 patients with candidiasis balanoposthitis.
Depending on the severity of the process, treatment was carried out with local or systemic drugs or a combination of both.
For mild forms of balanoposthitis, along with compliance with hygienic measures, the following was used:
clotrimazole, 1% cream, topically 2–3 times a day, 1–2 weeks. or econazole, cream or powder, topically 2 times a day, 1–2 weeks.
In the presence of risk factors for generalization of infection (for example, in patients with diabetes or patients with immunosuppression), as well as in cases of pronounced inflammatory changes, local therapy was supplemented with drugs for systemic use :
- fluconazole 150 mg orally, once or fluconazole 150 mg orally, on the 1st day, then 50 mg once a day, 7 days. or fluconazole 200 mg orally, on the 1st day, then 100 mg 1 time per day, 4 days.
This therapy was effective in 93–95% of patients, which was confirmed by the results of examination, microscopic and bacteriological examination. In 5–7% of cases, the course of treatment had to be repeated or prolonged.
Often, candidal balanoposthitis is combined with candidal urethritis [9]. In this case, patients experience pain when urinating, frequent urination, cheesy discharge from the urethra, and hyperemia of the urethral sponges.
The diagnosis is made based on the characteristics of the clinical picture and the results of laboratory methods:
- microscopic examination of a native or Gram-stained preparation allows not only to detect the presence of Candida with a predominance of vegetative forms of the fungus (mycelium and budding yeast cells), but also to assess the composition of the urethral microflora (pathogenic and conditionally pathogenic microorganisms) and the severity of the leukocyte reaction;
- Bacteriological examination makes it possible to determine the species of the isolated fungal culture and accompanying microorganisms, as well as to assess drug sensitivity. The growth of fungal colonies >104 CFU/ml is diagnostically significant [9].
In 55 of 327 patients with candidal balanoposthitis, candidal urethritis was also detected.
Treatment in this case necessarily included a systemic antifungal drug:
- fluconazole 150 mg orally on the 1st day, then 50 mg 1 time per day, 7 days. or fluconazole 200 mg orally on the 1st day, then 100 mg 1 time per day, 4 days.
Prevention of fungal infections
Experience in treating urological patients with various inflammatory diseases requiring the prescription of broad-spectrum antibiotics indicates that fluconazole is one of the main and most effective drugs used to prevent fungal superinfection. Depending on the duration of antibacterial therapy, the presence of concomitant diseases (especially diabetes and immunosuppressive conditions), the drug is prescribed once, repeatedly or in prolonged courses:
fluconazole 150 mg orally, once (if necessary, repeat after 1 week, or fluconazole 50 mg orally, 1 time per day, daily or every other day, 7–14 days.
Conclusion
Fluconazole is widely used in urological practice.
The drug has a wide spectrum of action, including most species of Candida, Cryptococcus neoformans, dermatophytes, Malassezia furfur and the “classical” dimorphic pathogens Histoplasma capsulatum, Blastomyces dermatitidis, Paracoccidioides brasiliensis, Coccidioides immitis.
Among the fungi of the genus Candida, the most sensitive to fluconazole are C. albicans, which are the causative agents of most fungal urological infections. Resistance in C. albicans strains rarely develops during treatment.
Fluconazole is soluble in water and is quickly and almost completely absorbed from the gastrointestinal tract. More than 90% of the dose taken orally enters the bloodstream. Simultaneous food intake, as well as gastric acidity, do not affect the absorption of the drug. Peak concentrations are created within 1–2 hours, equilibrium concentrations are achieved by days 4–6 with 1 dose daily. The pharmacokinetic properties of the drug are the same when administered orally or intravenously.
In blood plasma, no more than 12% of the drug is bound to proteins, the main amount is in free form. Therefore, fluconazole penetrates well into all body fluids.
Fluconazole is excreted by the kidneys, mainly in unchanged form. Very high – more than 100 mg/l – concentrations of the drug are created in the urine. Excretion of the drug depends on the glomerular filtration rate. Fluconazole is very poorly metabolized by the liver. The plasma half-life is approximately 30 hours; dosage and duration of therapy do not affect the half-life [10].
Thus, it is obvious that fluconazole can be considered the drug of choice for both the treatment and prevention of fungal infections in the majority of urological patients.
Literature
1. Storfer SP, Medoff G, Fraser VJ et al. Candiduria: retrospective review in hospitalized patients. Infect Dis Clin Pract 1994; 3:23–9.
2. Leu HS, Huang CT. Clearance of funguria with short–course antifungal regimens: a prospective, randomized, controlled study. Clin Infect Dis 1995; 20: 1152–7.
3. Jacobs LG, Skidmore EA, Freeman K et al. Oral fluconazole compared with bladder irrigation with amphotericin B for treatment of fungal urinary tract infections in elderly patients. Clin Infect Dis 1996; 22:30–5.
4. Lundstrom T, Sobel J. Nosocomial Candiduria: A Review. Clin Infect Dis 2001; 32:1602–7.
5. Goeke TM. Infectious complications of diabetes mellitus. In: Grieco MH, ed. Infections in the abnormal host. New York: Yorke Medical Books, 1980; 585–600.
6. Fischer JF, Chew WH, Shadomy S et al. Urinary tract infections due to Candida albicans. Rev Infect Dis 1982; 4: 1107–18.
7. Stamm WE. Catheter–associated urinary tract infections: epidemiology, pathogenesis, and prevention. Am J Med 1991; 91 (suppl. 3B): 65S–71S.
8. Kauffman CA, Vazquez JA, Sobel JD et al. Prospective multicenter surveillance study of funguria in hospitalized patients. Clin Infect Dis 2000; 30:14–8.
9. Rational pharmacotherapy of skin diseases and sexually transmitted infections (edited by A.A. Kubanova and V.I. Kisina). M.: Litterra, 2005.
10. Sergeev A.Yu., Sergeev Yu.V. Fungal infections. Guide for doctors. M.: BINOM-Press, 2003.
Interaction
Before starting treatment, it is important to know not only what Fluconazole in tablets and other forms helps with, but also about the interaction of drugs with other drugs.
When taking Warfarin , the prothrombin time of fluconazole becomes longer.
With simultaneous administration of hypoglycemic oral agents belonging to the group of sulfonylurea derivatives, the half-life of Fluconazole increases. As a result, there is a possibility of hypoglycemia.
With simultaneous administration of phenytoin, a clinically significant increase in phenytoin concentrations is observed.
With simultaneous repeated use of hydrochlorothiazide, an increase in the concentration of fluconazole in the blood is observed. There is no need to change the dosage.
With simultaneous treatment with Rifampicin, AUC decreases by 25%. The half-life is also reduced by 20%. In some cases, the doctor decides to increase its dose.
When treating with Fluconazole, monitoring the concentration of cyclosporine in the blood is recommended.
If the patient simultaneously receives high doses of Theophylline , it is important to consider the possibility of Theophylline overdose.
It is contraindicated to take a dose of more than 400 mg per day in combination with terfenadine .
When taking cisapride , negative side effects from blood vessels and the heart may occur, in particular, paroxysms of ventricular tachycardia .
If Fluconazole and Zidovudine , the patient should be monitored by a doctor, as the side effects of Zidovudine may increase.
If treatment with Astemizole , cisapride , Tacrolimus , Rifabutin , or any other drug that is metabolized by the cytochrome P450 system is simultaneously prescribed, the concentration of these drugs in the blood may increase.
The absorption of Fluconazole is not affected by simultaneous administration of Cimetidine or antacids.
Fluconazole
Single or repeated use of fluconazole at a dose of 50 mg does not affect the metabolism of phenazone (Antipyrin) when used simultaneously.
Concomitant use of fluconazole with the following drugs is contraindicated:
Cisapride: with the simultaneous use of fluconazole and cisapride, adverse reactions from the heart are possible, including ventricular tachysystolic arrhythmia of the “pirouette” type (torsade de pointеs). The use of fluconazole at a dose of 200 mg once a day and cisapride at a dose of 20 mg 4 times a day leads to a marked increase in plasma concentrations of cisapride and an increase in the QT interval on the ECG. Concomitant use of cisapride and fluconazole is contraindicated.
Terfenadine: When azole antifungals are used concomitantly with terfenadine, serious arrhythmias may occur as a result of prolongation of the QT interval. When taking fluconazole at a dose of 200 mg/day, an increase in the QT interval has not been established, however, the use of fluconazole at doses of 400 mg/day and above causes a significant increase in the concentration of terfenadine in the blood plasma. Concomitant use of fluconazole in doses of 400 mg/day or more with terfenadine is contraindicated (see section “Contraindications”). Treatment with fluconazole in doses less than 400 mg/day in combination with terfenadine should be carried out under close monitoring.
Astemizole: simultaneous use of fluconazole with astemizole or other drugs metabolized by the cytochrome P450 system may be accompanied by an increase in serum concentrations of these drugs. Elevated concentrations of astemizole in blood plasma can lead to prolongation of the QT interval and, in some cases, to the development of ventricular tachysystolic arrhythmia of the “pirouette” type (torsade de pointеs). The simultaneous use of astemizole and fluconazole is contraindicated.
Pimozide: Although adequate in vitro or in vivo studies have not been conducted, concomitant use of fluconazole and pimozide may result in inhibition of the metabolism of pimozide. In turn, an increase in plasma concentrations of pimozide can lead to a prolongation of the QT interval and, in some cases, the development of ventricular tachysystolic arrhythmia of the “pirouette” type (torsade de pointеs). The simultaneous use of pimozide and fluconazole is contraindicated.
Quinidine: Although adequate in vitro or in vivo studies have not been conducted, concomitant use of fluconazole and quinidine may also result in inhibition of quinidine metabolism. The use of quinidine is associated with prolongation of the QT interval and, in some cases, with the development of ventricular tachysystolic arrhythmia of the “torsade de pointes” type. The simultaneous use of quinidine and fluconazole is contraindicated.
Erythromycin: Concomitant use of fluconazole and erythromycin potentially leads to an increased risk of cardiotoxicity (QT prolongation, torsade de pointes) and consequently sudden cardiac death. The simultaneous use of fluconazole and erythromycin is contraindicated.
Concomitant use of fluconazole with the following drugs is not recommended:
Halofantrine: Fluconazole may increase plasma concentrations of halofantrine due to inhibition of CYP3A4. When used simultaneously with fluconazole, as well as with other azole antifungal drugs, the development of ventricular tachysystolic arrhythmia of the “pirouette” type is possible, so their combined use is not recommended.
Caution and possible dosage adjustments should be used when the following drugs are used concomitantly with fluconazole:
Drugs that affect fluconazole:
Hydrochlorothiazide: repeated use of hydrochlorothiazide concomitantly with fluconazole leads to an increase in fluconazole plasma concentrations by 40%. An effect of this severity does not require a change in the fluconazole dosage regimen in patients receiving concomitant diuretics, but the doctor should take this into account.
Rifampicin: Concomitant use of fluconazole and rifampicin results in a 25% decrease in AUC and a 20% decrease in fluconazole half-life. In patients concomitantly taking rifampicin, it is necessary to consider the advisability of increasing the dose of fluconazole.
Drugs affected by fluconazole:
Fluconazole is a potent inhibitor of the CYP2C9 isoenzyme and a moderate inhibitor of the CYP3A4 isoenzyme. Fluconazole is also an inhibitor of the CYP2C19 isoenzyme. In addition, in addition to the effects listed below, there is a risk of increased plasma concentrations of other drugs metabolized by the isoenzymes CYP2C9 and CYP2C19 and CYP3A4 when taken simultaneously with fluconazole. In this regard, caution should be exercised when using these drugs simultaneously, and if such combinations are necessary, patients should be under close medical supervision. It should be taken into account that the inhibitory effect of fluconazole persists for 4-5 days after discontinuation of the drug due to the long half-life.
Alfentanil: There is a decrease in clearance and volume of distribution, and an increase in the half-life of alfentanil. This may be due to inhibition of the CYP3A4 isoenzyme by fluconazole. Alfentanil dosage adjustment may be required.
Amitriptyline, nortriptyline: increased effect. Concentrations of 5-nortriptyline and/or S-amitriptyline can be measured at the start of combination therapy with fluconazole and one week after the start of treatment. If necessary, the dose of amitriptyline/nortriptyline should be adjusted.
Amphotericin B: In studies in mice (including immunosuppressed mice), the following results were observed: small additive antifungal effect in systemic infection with C. albicans, no interaction in intracranial infection with Cryptococcus neoformans, and antagonism in systemic infection with A .fumigatus. The clinical significance of these results is unclear.
Anticoagulants: like other antifungal agents (azole derivatives), fluconazole, when used simultaneously with warfarin, increases prothrombin time (by 12%), and therefore bleeding may develop (hematomas, bleeding from the nose and gastrointestinal tract, hematuria, melena). In patients receiving coumarin anticoagulants, prothrombin time must be constantly monitored during therapy and for 8 days after simultaneous use. The advisability of adjusting the warfarin dose should also be assessed.
Benzodiazepines (short-acting): After oral administration of midazolam, fluconazole significantly increases midazolam concentrations and psychomotor effects, and this effect is more pronounced after fluconazole is administered orally than when fluconazole is administered intravenously. If concomitant therapy with benzodiazepines is necessary, patients taking fluconazole should be monitored to assess the appropriateness of an appropriate reduction in the benzodiazepine dose.
When coadministered with a single dose of triazolam, fluconazole increases triazolam AUC by approximately 50%, Cmax by 25-50%, and half-life by 25-50% due to inhibition of triazolam metabolism. Triazolam dose adjustment may be necessary.
Carbamazepine: Fluconazole inhibits the metabolism of carbamazepine and increases the serum concentration of carbamazepine by 30%. The risk of carbamazepine toxicity must be taken into account. The need for carbamazepine dose adjustment based on concentration/effect should be assessed.
Slow calcium channel blockers: Some calcium channel antagonists (nifedipine, isradipine, amlodipine, verapamil and felodipine) are metabolized by the CYP3A4 isoenzyme. Fluconazole increases the systemic exposure of calcium channel antagonists. Monitoring for the development of side effects is recommended.
Cyclophosphamide: with simultaneous use of cyclophosphamide and fluconazole, an increase in serum concentrations of bilirubin and creatinine is observed. This combination is acceptable given the risk of increased bilirubin and creatinine concentrations.
Fentanyl: There has been a report of one death possibly related to the concomitant use of fentanyl and fluconazole. The disturbances are believed to be related to fentanyl intoxication. Fluconazole has been shown to significantly prolong the clearance time of fentanyl. It should be borne in mind that an increase in the concentration of fentanyl can lead to depression of respiratory function.
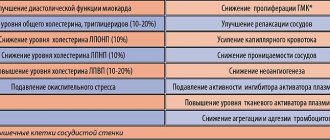
HMG-CoA reductase inhibitors: When fluconazole is used concomitantly with HMG-CoA reductase inhibitors metabolized by the CYP3A4 isoenzyme (such as atorvastatin and simvastatin) or the CYP2D6 isoenzyme (such as fluvastatin), the risk of developing myopathy and rhabdomyolysis increases. If concomitant therapy with these drugs is necessary, patients should be monitored for symptoms of myopathy and rhabdomyolysis. It is necessary to monitor the concentration of creatinine kinase. If there is a significant increase in creatinine kinase concentrations or if myopathy or rhabdomyolysis is diagnosed or suspected, therapy with HMG-CoA reductase inhibitors should be discontinued.
Immunosuppressants (cyclosporine, sirolimus, tacrolimus)
Cyclosporine: In patients with a kidney transplant, the use of fluconazole at a dose of 200 mg/day leads to a slow increase in cyclosporine concentrations. However, with repeated doses of fluconazole at a dose of 100 mg/day, no changes in cyclosporine concentrations were observed in bone marrow recipients. When using fluconazole and cyclosporine simultaneously, it is recommended to monitor the concentration of cyclosporine in the blood.
Sirolimus: increased plasma concentrations of sirolimus, presumably due to inhibition of sirolimus metabolism through inhibition of the CYP3 A4 isoenzyme and P-glycoprotein. This combination can be used with appropriate dose adjustment of sirolimus depending on the effect/concentration.
Tacrolimus: simultaneous use of fluconazole and tacrolimus (orally) leads to an increase in serum concentrations of the latter by 5 times due to inhibition of the metabolism of tacrolimus occurring in the intestine through the CYP3A4 isoenzyme. No significant changes in the pharmacokinetics of the drugs were observed when tacrolimus was administered intravenously. Cases of nephrotoxicity have been described. Patients receiving oral tacrolimus and fluconazole concomitantly should be monitored closely. The dose of tacrolimus should be adjusted depending on the degree of increase in its concentration in the blood.
Losartan: Fluconazole inhibits the metabolism of losartan to its active metabolite (E-31 74), which is responsible for most of the effects associated with angiotensin II receptor antagonism. Regular monitoring of blood pressure is necessary.
Methadone: Fluconazole may increase plasma concentrations of methadone. Methadone dose adjustment may be necessary.
Nonsteroidal anti-inflammatory drugs (NSAIDs): Cmax and AUC of flurbiprofen increased by 23% and 81%, respectively. Similarly, the Cmax and AUC of the pharmacologically active isomer [S-(+)-ibuprofen] increased by 15% and 82%, respectively, when fluconazole was administered simultaneously with racemic ibuprofen (400 mg).
With simultaneous use of fluconazole at a dose of 200 mg/day and celecoxib at a dose of 200 mg, the Cmax and AUC of celecoxib increased by 68% and 134%, respectively. In this combination, it is possible to reduce the dose of celecoxib by half.
Although there are no targeted studies, fluconazole may increase the systemic exposure of other NSAIDs metabolized by CYP2C9 (eg, naproxen, lornoxicam, meloxicam, diclofenac). NSAID dose adjustment may be necessary.
When NSAIDs and fluconazole are used concomitantly, patients should be closely monitored medically to identify and monitor NSAID-related adverse events and toxicities.
Phenytoin: Concomitant use of fluconazole and phenytoin may be accompanied by a clinically significant increase in phenytoin concentrations. If concomitant use of both drugs is necessary, phenytoin concentrations should be monitored and the dose adjusted accordingly to ensure therapeutic serum concentrations.
Prednisone: there is a report of the development of acute adrenal insufficiency in a patient after liver transplantation while fluconazole was discontinued after a three-month course of therapy. Presumably, cessation of fluconazole therapy caused an increase in the activity of the CYP3 A4 isoenzyme, which led to increased metabolism of prednisone. Patients receiving combination therapy with prednisone and fluconazole should be under close medical supervision when discontinuing fluconazole to evaluate the condition of the adrenal cortex.
Rifabutin: Concomitant use of fluconazole and rifabutin can lead to an increase in serum concentrations of the latter by up to 80%. Cases of uveitis have been described with the simultaneous use of fluconazole and rifabutin. Patients receiving rifabutin and fluconazole concomitantly should be monitored closely.
Saquinavir: AUC increases by approximately 50%, Cmax by 55%, clearance of saquinavir decreases by approximately 50% due to inhibition of hepatic metabolism of the CYP3A4 isoenzyme and inhibition of P-glycoprotein. Dose adjustment of saquinavir may be necessary.
Sulfonylureas: Fluconazole, when administered concomitantly, results in an increase in the half-life of oral sulfonylureas (chlorpropamide, glibenclamide, glipizide and tolbutamide). Patients with diabetes mellitus can be prescribed the combined use of fluconazole and oral sulfonylureas, but the possibility of hypoglycemia should be taken into account, in addition, regular monitoring of blood glucose is necessary and, if necessary, dose adjustment of sulfonylureas.
Theophylline: when used simultaneously with fluconazole at a dose of 200 mg for 14 days, the average rate of plasma clearance of theophylline is reduced by 18%. When prescribing fluconazole to patients taking high doses of theophylline or to patients at increased risk of developing theophylline toxicity, monitor for symptoms of theophylline overdose and, if necessary, adjust therapy accordingly.
Vinca alkaloid: Although focused studies are lacking, it is suggested that fluconazole may increase plasma concentrations of vinca alkaloids (e.g., vincristine and vinblastine) and thus lead to neurotoxicity, possibly due to inhibition of CYP3A4.
Vitamin A: There has been a report of one case of central nervous system (CNS) adverse reactions in the form of pseudotumor cerebri with the simultaneous use of all-trans retinoic acid and fluconazole, which disappeared after discontinuation of fluconazole. The use of this combination is possible, but one should remember the possibility of adverse reactions from the central nervous system.
Voriconazole (inhibitor of CYP2C9, CYP2C19 and CYP3A4 isoenzymes): simultaneous use of voriconazole (400 mg 2 times a day on the first day, then 200 mg twice a day for 2.5 days) and fluconazole (400 mg on the first day, then 200 mg per day for 4 days) leads to an increase in voriconazole concentration and AUC by 57% and 79%, respectively. It has been shown that this effect persists when the dose is reduced and/or the frequency of administration of any of the drugs is reduced. Concomitant use of voriconazole and fluconazole is not recommended.
Zidovudine: when used simultaneously with fluconazole, an increase in the Cmax and AUC of zidovudine is observed by 84% and 74%, respectively. This effect is probably due to a decrease in the metabolism of the latter to its main metabolite. Patients receiving this combination should be monitored for side effects of zidovudine. A dose reduction of zidovudine may be required.
Azithromycin: with simultaneous oral use of fluconazole in a single dose of 800 mg with azithromycin in a single dose of 1200 mg, no pronounced pharmacokinetic interaction has been established between both drugs.
Oral contraceptives: with simultaneous use of a combined oral contraceptive with fluconazole at a dose of 50 mg, no significant effect on hormone levels has been established, while with daily administration of 200 mg of fluconazole, the AUC of ethinyl estradiol and levonorgestrel increases by 40% and 24%, respectively, and with 300 mg of fluconazole once weekly administration, the AUCs of ethinyl estradiol and norethindrone increased by 24% and 13%, respectively. Thus, repeated use of fluconazole at the indicated doses is unlikely to affect the effectiveness of the combined oral contraceptive.
Tofacitinib: Tofacitinib exposure is increased when coadministered with drugs that are both moderate CYP3A4 inhibitors and strong CYP2C19 inhibitors (eg, fluconazole). A dose adjustment of tofacitinib may be necessary.
Studies of the interaction of oral forms of fluconazole when taken simultaneously with food, cimetidine, antacids, as well as after total body irradiation in preparation for bone marrow transplantation showed that these factors do not have a clinically significant effect on the absorption of fluconazole.
The listed interactions were established with repeated use of fluconazole; There are no known drug interactions resulting from a single dose of fluconazole. Doctors should note that interactions with other drugs have not been specifically studied, but are possible.
special instructions
If liver dysfunction is observed during treatment, constant monitoring by a physician is important. If signs of liver damage are observed, the medication should be discontinued.
When using the medicine topically for men and women, it should be taken into account that people with AIDS are more likely to develop a variety of skin reactions.
It is necessary to take into account not only how long it takes for Fluconazole to act, but also the fact that if treatment is stopped prematurely, relapses may develop. Therefore, it is important to completely complete the prescribed treatment regimen. It is important to take this into account when using Fluconazole for nail fungus, since reviews for nail fungus indicate that if treatment is stopped prematurely, a relapse of the disease may occur.
Many patients have a question about whether Fluconazole is an antibiotic or not? Please note that this is an antifungal agent, not an antibiotic.
Whether men can take this drug depends on the diagnosis. Fluconazole for men is prescribed for fungal infections; it must be taken exactly as prescribed.
Special instructions for the use of the drug Fluconazole
Patients whose liver function tests are impaired during treatment with fluconazole should be under medical supervision. If clinical signs of liver damage appear, fluconazole should be discontinued. People with AIDS are more likely to develop severe skin reactions when taking many drugs. If a rash, possibly caused by the use of fluconazole, appears in a patient receiving treatment for a superficial fungal infection, the drug should be discontinued. If a rash appears in patients with invasive/systemic fungal infections, their condition should be monitored; if bullous lesions or erythema multiforme develop, fluconazole should be discontinued. The use of fluconazole should be avoided in pregnant women, except in cases of severe and potentially life-threatening fungal infections when the expected benefit to the woman outweighs the potential risk to the fetus. Fluconazole is detected in breast milk at the same concentration as in the blood, so its use during breastfeeding is not recommended.
Fluconazole analogs
Level 4 ATC code matches:
Medoflucon
Vfend
Itracon
Mikosist
Irunin
Mikomax
Orungal
Mycoflucan
Sporagal
Orungamin
Flucostat
Difluzol
Rumicosis
Futsis
Vero-Fluconazole
Kandizol
Kanditral
Itraconazole
Diflazon
Fluconazole analogues are products with a similar active ingredient. The price of analogues depends on the manufacturer and the form of release of the drug. There are a number of analogues of this drug:
- Diflazon
- Diflucan
- Vero-Fluconazole
- Mikomax
- Flucostat
Which is better: Fluconazole or Diflucan?
Often patients compare two drugs with antifungal action - Fluconazole and Diflucan . What is the difference between these medicines? Both drugs are based on the active substance fluconazole. Diflucan is available in tablets of 50 mg, 100 mg, 150 mg, and other forms. But the price of Diflucan is much higher.
Flucostat or Fluconazole - which is better?
Speaking about how Flucostat from Fluconazole, it should be noted that both drugs contain the same active substance. Flucostat is a more expensive medicine. What is the difference between these medications, and which one is best prescribed in a particular case, is determined by a specialist. As a rule, Fluconazole is more often prescribed when prophylaxis is necessary for cancer patients after radiation and chemotherapy.
Fluconazole or Nystatin - which is better?
Nystatin is an antifungal drug, an antibiotic, active against candida bacteria. Under the influence of Nystatin, the permeability of the membrane of fungal cells is disrupted, which contributes to disruption of their growth and reproduction. Which drug is preferred in a particular case depends on the diagnosis and the doctor’s prescription.
Reviews about Fluconazole
Due to the high fungicidal activity of this drug, patient reviews and doctors' reviews of Fluconazole are mostly positive. Patients, leaving reviews about Fluconazole Teva, as well as reviews about Fluconazole Stada on the forums, write that the drug helps to quickly and effectively eliminate the symptoms of fungal diseases. Users mention that the tablets are relatively inexpensive, but at the same time they allow you to completely get rid of nail fungus and other unpleasant diseases. In some cases, it is enough to take Fluconazole 150 mg once to completely overcome the symptoms of the disease.
Very often, women write positive reviews about Fluconazole for thrush . It is noted that the medicine not only relieves thrush, but also helps prevent relapses of the disease.
Fluconazole price, where to buy
The price of Fluconazole tablets depends on the packaging and manufacturer. You can buy Fluconazole in Moscow at prices ranging from 40 to 140 rubles. Capsules 150 mg (1 piece in a package) can be purchased for 140 rubles. Capsules 50 mg can be purchased for 60 rubles (pack of 7 pieces)
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
- Online pharmacies in KazakhstanKazakhstan
ZdravCity
- Fluconazole Sandoz caps.
150 mg Salutas Pharma GmbH, Germany RUB 154 order - Fluconazole caps. 150 mg No. 1Ozon Pharm LLC
39 RUR order
- Fluconazole capsules 150 mg 2 pcs. Ozon LLC
52 RUR order
- Fluconazole-Teva capsules 50 mg 7 pcs. Teva Pharmaceutical Works Private Limited Company
280 rub. order
- Fluconazole-Obl caps. 150 mg 1 pc. JSC Obolenskoe farm. company
39 RUR order
Pharmacy Dialogue
- Fluconazole-Teva capsules 50 mg No. 7Teva
RUR 318 order
- Fluconazole (caps. 50 mg No. 7) Ozon LLC
67 RUR order
- Fluconazole Stada (caps. 150 mg No. 1) Hemofarm LLC
63 RUR order
- Fluconazole-OBL (caps. 150 mg No. 1) Obolenskoye pharmaceutical pred.
35 rub. order
- Fluconazole-Teva (caps. 50 mg No. 7)Teva Pharmaceutical Works Private Co.
RUB 281 order
show more
Pharmacy24
- Fluconazole-Darnitsa 0.15g N2 capsules PrAT" Pharmaceutical company "Darnitsa", Ukraine
28 UAH. order - Fluconazole-KR 50 mg No. 7 capsules PAT"Khimpharmzavod"Chervona Zirka", Kharkov, Ukraine
15 UAH order
- Fluconazole-Darnitsa 150 mg No. 3 capsules PrAT" Pharmaceutical company "Darnitsa", Ukraine
40 UAH order
- Fluconazole 200 mg 100 ml No. 1 solution Eurolife Healthcare Pvt. Ltd., India
83 UAH order
- Fluconazole 100 mg N10 tablets PrAT "Technolog", Uman, Cherkasy region, Ukraine
32 UAH order
PaniPharmacy
- FLUCONAZOL capsule Fluconazole capsules 0.15g No. 2 Ukraine, Zdorovye LLC
33 UAH order
- Fluconazole caps. 150mg №2
31 UAH order
- FLUCONAZOL tablets Fluconazole tablets 150 mg No. 2 Ukraine, Tekhnolog ChAO
29 UAH order
- FLUCONAZOLE capsule Fluconazole forte caps. 200 mg No. 2 Ukraine, Health LLC
47 UAH order
- FLUCONAZOL capsule Fluconazole capsules 0.05g No. 10 Ukraine, Darnitsa ChAO
28 UAH order
show more