Pharmacological properties of the drug Galantamine
An alkaloid isolated from the tubers of some snowdrop species (Galanthus Woronowi A.Los., Galanthus nivalis var. gracilis) and some closely related plants. Anticholinesterase agent, a strong reversible cholinesterase inhibitor. Facilitates cholinergic transmission, enhancing and prolonging the action of endogenous acetylcholine. Enhances neuromuscular transmission in skeletal muscles, exhibits antagonism towards curare-like non-depolarizing agents. Increases the tone of smooth muscles of internal organs, enhances the secretion of exocrine glands. Causes miosis, reduces intraocular pressure, causes a spasm of accommodation. Penetrates well through the BBB, enhances excitation processes in the cholinergic synapses of the central nervous system.
Galantamine Canon (tablets) 4mg, 8mg, 12mg
The drug Galantamine Canon is indicated for the treatment of mild to moderate dementia of the Alzheimer's type. The effectiveness of galantamine in patients with other types of dementia and other memory disorders has not been established. Also, no positive effect of galantamine use (for 2 years) on slowing down cognitive impairment and slowing down the transition to clinically significant dementia in patients with the syndrome of “mild” cognitive decline (“mild” types of memory impairment that do not meet the criteria for Alzheimer’s type dementia) has been established ). Mortality was significantly higher in the galantamine group than in the placebo group, 14/1026 (1.4%) of patients receiving galantamine and 3/1022 (0.3%) of patients receiving placebo. The causes of death varied. About half of the deaths in the galantamine group were due to various vascular causes (myocardial infarction, stroke and sudden death). The significance of these findings for the treatment of patients with dementia of the Alzheimer's type is unknown. Placebo-controlled studies in patients with dementia of the Alzheimer's type were conducted for 6 months only. In these studies, mortality was not increased in the galantamine group.
Treatment with Galantamine Canon should only be carried out under the supervision of a physician and under the supervision of a person caring for the patient.
Patients with Alzheimer's disease lose weight. Treatment with cholinomimetic drugs, including galantamine, is accompanied by a decrease in body weight, so this indicator should be monitored during therapy.
Like other cholinomimetic drugs, Galantamine Canon should be used with caution in the following diseases:
Diseases of the cardiovascular system
Due to their pharmacological action, cholinomimetic drugs can cause vagotonic effects (for example, bradycardia). It should be used with caution in patients with SSS and other disorders of supraventricular conduction, during simultaneous therapy with drugs that reduce heart rate (digoxin and beta-blockers) and in patients with electrolyte metabolism disorders (hyperkalemia, hypokalemia); in the period after acute myocardial infarction; with newly diagnosed atrial fibrillation; in patients with atrioventricular block II-III degree, unstable angina or chronic heart failure, especially functional class III-IV according to the NYHA classification.
During therapy with Galantamine Canon for dementia of the Alzheimer's type, the risk of developing adverse reactions from the cardiovascular system increases.
Digestive system diseases
In patients with an increased risk of developing erosive and ulcerative lesions of the gastrointestinal tract (for example, a history of gastric and duodenal ulcers, NSAID therapy), it is necessary to monitor the condition in order to early identify the corresponding pathological symptoms. Galantamine Canon is not recommended for use in patients with gastrointestinal obstruction or after recent gastrointestinal surgery.
Nervous system diseases
The use of cholinomimetic drugs may cause convulsions. It should be remembered that seizure activity can be a manifestation of Alzheimer's disease itself. In rare cases, increased cholinergic tone may worsen Parkinson's disease.
Cerebrovascular events have been reported infrequently in patients with dementia of the Alzheimer's type using galantamine. This should be taken into account when prescribing galantamine to patients with cerebrovascular pathology.
Respiratory system diseases
The drug Galantamine Canon should be prescribed with caution to patients with severe asthma, COPD, acute infectious diseases of the lungs (for example, pneumonia).
Kidney and urinary tract diseases
Galantamine Canon is not recommended for use in patients with urinary tract obstruction who have recently undergone bladder surgery.
General anesthesia
Galantamine, which is a cholinomimetic, can enhance the blockade of depolarizing-type neuromuscular transmission (muscle relaxation) caused by general anesthesia (when used as a peripheral muscle relaxant, suxamethonium), especially in cases of pseudocholinesterase deficiency.
If treatment is suddenly stopped (for example, before surgery), withdrawal syndrome does not develop.
The influence of a medicinal product for medical use on the ability to drive vehicles and machinery
The drug Galantamine Canon, like other cholinomimetic drugs, can cause drowsiness and dizziness, which negatively affect the control of transport and other mechanisms, especially in the first weeks after the start of treatment.
Use of the drug Galantamine
For subcutaneous administration, single doses for adults are 2.5–10 mg; for children aged 1-2 years - 0.25-0.5 mg, 3-5 years - 0.5-1 mg, 6-8 years - 0.75-2 mg, 9-11 years - 1.25 -3 mg, 12-14 years old - 1.75-5 mg, 15-16 years old - 2-7 mg, if necessary, the dose can be increased, but strictly individually. For adults, the maximum single dose is 10 mg, the daily dose is 20 mg. Galantamine is administered 1 time, and if necessary 2 times a day. Therapy begins with minimal doses, which are gradually increased; The frequency of use of galantamine in high doses is 3 times a day. The course of treatment lasts up to 50 days, if necessary, 2-3 repeated courses can be carried out with an interval of 1-1.5 months. For intravenous administration, single doses for adults are 10–25 mg; for children aged 1-2 years - 1-2 mg, 3-5 years - 1.5-3 mg, 6-8 years - 2-5 mg, 9-11 years - 3-8 mg, 12-15 years - 5–10 mg. When taken orally, the daily dose is 5–10 mg, the frequency of administration is 3–4 times a day after meals, the duration of treatment is 4–5 weeks.
Galantamine, 8 mg, film-coated tablets, 56 pcs.
The drug Galantamine Canon is indicated for the treatment of mild to moderate dementia of the Alzheimer's type. The effectiveness of galantamine in patients with other types of dementia and other memory disorders has not been established. Also, no positive effect of galantamine use (for 2 years) on slowing down cognitive impairment and slowing down the transition to clinically significant dementia in patients with the syndrome of “mild” cognitive decline (“mild” types of memory impairment that do not meet the criteria for Alzheimer’s type dementia) has been established ). Mortality was significantly higher in the galantamine group than in the placebo group, 14/1026 (1.4%) of patients receiving galantamine and 3/1022 (0.3%) of patients receiving placebo. The causes of death varied. About half of the deaths in the galantamine group were due to various vascular causes (myocardial infarction, stroke and sudden death). The significance of these findings for the treatment of patients with dementia of the Alzheimer's type is unknown. Placebo-controlled studies in patients with dementia of the Alzheimer's type were conducted for 6 months only. In these studies, mortality was not increased in the galantamine group.
Treatment with Galantamine Canon should only be carried out under the supervision of a physician and under the supervision of a person caring for the patient.
Patients with Alzheimer's disease lose weight. Treatment with cholinomimetic drugs, including galantamine, is accompanied by a decrease in body weight, so this indicator should be monitored during therapy.
Like other cholinomimetic drugs, Galantamine Canon should be used with caution in the following diseases:
Diseases of the cardiovascular system
Due to their pharmacological action, cholinomimetic drugs can cause vagotonic effects (for example, bradycardia). It should be used with caution in patients with SSS and other disorders of supraventricular conduction, during simultaneous therapy with drugs that reduce heart rate (digoxin and beta-blockers) and in patients with electrolyte metabolism disorders (hyperkalemia, hypokalemia); in the period after acute myocardial infarction; with newly diagnosed atrial fibrillation; in patients with atrioventricular block II-III degree, unstable angina or chronic heart failure, especially functional class III-IV according to the NYHA classification.
During therapy with Galantamine Canon for dementia of the Alzheimer's type, the risk of developing adverse reactions from the cardiovascular system increases.
Digestive system diseases
In patients with an increased risk of developing erosive and ulcerative lesions of the gastrointestinal tract (for example, a history of gastric and duodenal ulcers, NSAID therapy), it is necessary to monitor the condition in order to early identify the corresponding pathological symptoms. Galantamine Canon is not recommended for use in patients with gastrointestinal obstruction or after recent gastrointestinal surgery.
Nervous system diseases
The use of cholinomimetic drugs may cause convulsions. It should be remembered that seizure activity can be a manifestation of Alzheimer's disease itself. In rare cases, increased cholinergic tone may worsen Parkinson's disease.
Cerebrovascular events have been reported infrequently in patients with dementia of the Alzheimer's type using galantamine. This should be taken into account when prescribing galantamine to patients with cerebrovascular pathology.
Respiratory system diseases
The drug Galantamine Canon should be prescribed with caution to patients with severe asthma, COPD, acute infectious diseases of the lungs (for example, pneumonia).
Kidney and urinary tract diseases
Galantamine Canon is not recommended for use in patients with urinary tract obstruction who have recently undergone bladder surgery.
General anesthesia
Galantamine, which is a cholinomimetic, can enhance the blockade of depolarizing-type neuromuscular transmission (muscle relaxation) caused by general anesthesia (when used as a peripheral muscle relaxant, suxamethonium), especially in cases of pseudocholinesterase deficiency.
If treatment is suddenly stopped (for example, before surgery), withdrawal syndrome does not develop.
The influence of a medicinal product for medical use on the ability to drive vehicles and machinery
The drug Galantamine Canon, like other cholinomimetic drugs, can cause drowsiness and dizziness, which negatively affect the control of transport and other mechanisms, especially in the first weeks after the start of treatment.
PsyAndNeuro.ru
In recent years, several studies have been published on the use of galantamine-memantine combination in Alzheimer's disease (AD). In a two-year randomized controlled trial (RCT) of prodromal AD, the cognitive performance of patients receiving a combination of galantamine and memantine was significantly better than the cognitive performance of those receiving galantamine alone [1].
In a retrospective cohort study, the combination of galantamine-memantine significantly improved cognitive performance compared with the combination of donepezil-memantine in the treatment of AD [2]. In a naturalistic study, patients with dementia with Lewy bodies received galantamine for 6 months. Patients who responded to treatment were then also given memantine. The addition of memantine to galantamine significantly improved cognition and behavior compared with galantamine alone [3].
Despite compelling evidence, the galantamine-memantine combination is still underutilized in clinical practice. In the United States, galantamine and memantine are approved for the treatment of AD. The donepezil-memantine combination is also approved for the treatment of AD, but the galantamine-memantine combination is not.
Galantamine is superior to donepezil because it is a positive allosteric modulator of alpha7-nicotinic acetylcholine receptors and acts as an acetylcholinesterase inhibitor. Finally, in addition to cognitive impairment, psychosis and negative symptoms are often observed in AD. The galantamine-memantine combination can not only improve cognitive function, but also be used against psychosis and negative symptoms.
When analyzing the results of RCTs on the treatment of AD, it must be taken into account that many of them give a negative result due to the fact that patients are often recruited at an advanced stage of the disease. Treatment may be ineffective in late stages of AD because chronic neuroinflammatory processes cause irreversible damage over time. Typically, RCTs involve patients whose plaque burden and degree of neurodegeneration are already quite high, so their disease has probably already become irreversible. Clinical data suggest that treatment of asthma in the early stages is more promising. The best results are achieved in patients at the prodromal stage or in patients with mild cognitive impairment. This situation can be compared with carcinoma in situ and stage 1 or 2 cancer versus stages 3 and 4; in later stages, intervention usually does not produce results.
It is probably often the case that one drug is not enough to stabilize all pathophysiological mechanisms and reduce the symptoms of asthma. Neurodegenerative diseases include many pathologies, so combination treatment seems to be the most rational choice.
At the same time, taking a significant amount of medications by patients with asthma places a serious financial burden on their families. Previously, we published an analysis to find out which memantine is more economically beneficial. In the Russian Federation, 11 manufacturers of memantine are available in pharmacies, of which 6 contain an Indian substance, and 5 – a European one. However, the production of tablets for three of them is localized in the Russian Federation, and only two memantines - Akatinol and Memantal - are entirely produced in Europe. It is noteworthy that the first of them is the original drug, and the second is the only generic with proven therapeutic equivalence.
The combination of galantamine and memantine can be effective not only for asthma, but also for traumatic brain injury, autism and other neuropsychiatric diseases. In 22 patients with AD, memantine improved biomarkers of oxidative stress such as non-protein thiols and 3-nitrotyrosine in the cerebrospinal fluid [4]. Redox reactions mediated by NMDA receptors and their interactions with other molecules may be involved in synaptic dysfunction.
Simultaneous effects on nicotinic and NMDA receptors can be a very successful method for improving the basic parameters of cognitive functions of the brain [5].
Author: Filippov D.S.
Sources:
[1] Peters, O. et al. 2012. A combination of galantamine and memantine modifies cognitive function in subjects with amnestic MCI. J. Nutr. Health Aging 16(6), 544–548
[2] Matsuzono, K. et al. 2015. Combination therapy of cholinesterase inhibitor (donepezil or galantamine) plus memantine in the okayama memantine study. J. Alzheimer's Dis. 45(3), 771–780
[3] Vasenina, EE, Gankina, OA, Levin, OS, 2022. The addition of memantine to galantamine increases treatment efficacy in patients with moderate dementia with Lewy bodies. Zh Nevrol Psikhiatr Im S Korsakova 118 (6. Vyp. 2), 32–36
[4] Valis, M. et al. 2022. The Concentration of Memantine in the Cerebrospinal Fluid of Alzheimer's Disease Patients and Its Consequence to Oxidative Stress Biomarkers. Front. Pharmacol. 10,943
[5] Koola, Maju. (2020). Galantamine-Memantine Combination in the Treatment of Alzheimer's Disease and Beyond. Psychiatry Research. 293.113409.
Galantamine (remenil)
Galantamine is a cholinesterase inhibitor. This drug is used for moderate Alzheimer's disease and some other forms of dementia, for example, with Lewy bodies or vascular dementia. Galantamine increases acetylcholine concentrations through reversible inhibition of the metabolzyme enzyme acetylcholinosterase, which increases the availability of acetylcholine. Insufficiency of cholinergic activity is one of the important links in the pathogenesis of Alzheimer's disease. The drug also modulates the activity of nicotinic receptors and interferes with the process of amyloid deposition. Although galantamine may reduce symptoms of Alzheimer's disease, it does not prevent or stop the progression of this mental disorder. The effect of taking galantamine begins to appear after 2-6 weeks of treatment, and more clearly after several months of therapy. If the effect of the drug is insufficient, then select its appropriate dose, change to another cholyesterase inhibitor or NMDA antagonist (memantine), and joint use with the latter drugs is possible. You should not combine galantamine with drugs that have a sedative effect: opioids, hypnotics, tricyclic antidepressants. When co-administered with SSRIs, the risk of QTc prolongation and syncope increases. Side effects include nausea, vomiting, diarrhea, anorexia, weight loss, and somewhat less frequently: weakness, headache and dizziness. Rare dangerous complications: bradycardia, cardiac arrest due to syncope, convulsive syndrome, increased secretion of gastric juice. The drug is prescribed at a dose of 16-24 mg/day twice a day, starting treatment with 4 mg. twice a day (tablets 4, 8, 12 mg), gradually increasing to 8 mg. twice a day for a month. A month after starting treatment, the dose of the drug can be increased to 12 mg twice a day. Pharmacokinetics: the drug is mainly metabolized through CYP2D6 and 3A4 isoenzymes. Inhibitors of CYP2D6 and 3A4, including ketoconazole, cimetidine, paroxetine and erythromycin, may increase galantamine blood concentrations. Galantamine enhances the effect of anesthetics, which should be kept in mind when premedicating surgical operations. Bradycardia is possible when used together with beta blockers.
Experience of clinical use of Reminyl (galantamine)
The problem of population aging affects doctors of all specialties and especially psychiatrists. The reason for this is the increasing incidence of dementia in older people. Accordingly, the socio-economic burden on society for the treatment and care of this category of patients is increasing. According to an epidemiological study of the mental health of the elderly population of Moscow, Alzheimer's disease (AD) affects 4.5% of residents aged 60 years and older (1).
Table 1. Average total scores of the MMSE, ADAS-Cog, IADL, BEHAVE AD scales before the start of therapy
Figure 1. Dynamics of the average total MMSE score in mild, moderate dementia and for the group as a whole
Table 2. Dynamics of the average difference in the sums of scores of the ADAS-Cog, IADL, BEHAVE-AD scales
Figure 2. Dynamics of the patients’ condition according to the CGL scale
Figure 3. Dynamics of the average total score on the MMSE scale in AD and AD
Figure 4. Dynamics of the average total MMSE indicator in SMD
As is known, dementia is caused mainly by primary neurodegenerative processes, vascular pathology or a mixed vascular-degenerative process. According to the literature, a stroke increases the risk of vascular dementia (VaD) by 4-12 times (9). In our opinion, the current state of psychopharmacotherapy makes it possible not to ignore the decline in cognitive and psychosocial activity associated with the normal aging process.
The common mechanism for the two main types of dementia - Alzheimer's disease (AD) and vascular dementia (VaD) - is cholinergic neurotransmitter deficiency, the involvement of which in the development of dementia in both AD and VOD is now generally accepted, and its compensation with cholinomimetic drugs has become one of the main approaches to the treatment of this disease. It has been proven that an increase in the concentration of central acetylcholine is accompanied by an increase in the processes and number of synaptic contacts (4).
Galantamine (Reminyl) is a selective, competitive, reversible acetylcholinesterase inhibitor that can enhance the effects of acetylcholine through modulation of nicotinic acetylcholinergic receptors (nAChRs). Potentiation of nicotinic receptors makes it possible to enhance the nicotinic response of cholinergic neurons damaged by the degenerative process, but continuing to function. In addition, Reminyl modulates the release of glutamate, dopamine and GABA, thereby reducing the psychological and behavioral symptoms of dementia. As a result of increasing the sensitivity of nAChR (due to the modulating effect of galantamine (Reminyl) on nAChR), the effectiveness of the drug has been proven not only in AD, but also in mixed dementia (MSD) and vascular dementia (VoD).
Purpose
This study was to study the effectiveness and tolerability of Reminyl in clinical practice. We undertook an open, uncontrolled study of the effectiveness and safety of Reminyl in the treatment of AD, AD and SMD.
The objective of the study was to compare the results of therapy depending on the type of dementia, its nosology and severity.
Research methodology
developed jointly with researchers from the Scientific Center for Mental Health (headed by Prof. V.A. Kontseva). According to the study protocol, patients with mild or moderate dementia (according to the Clinical Dementia Rating) (11), AD (according to the NINCDS/ADRDA criteria), AD (according to the NINCDS-AIREN criteria) and “mixed” dementia (MD) (according to the NINCDS criteria) were selected /ADRDA). The study included patients with an MMSE score ranging from 12 to 24 points at the time of the screening visit. The diagnosis took into account clinical laboratory data, including CT or MRI of the head.
Exclusion criteria:
Patients with dementia of other origins - brain tumor, Parkinson's disease, frontotemporal dementia and other brain pathologies, as well as so-called metabolic dementia and pseudodementia were excluded from the study. Patients with severe and/or decompensated somatic pathology were also not included. The simultaneous administration of drugs that affect cognitive function was excluded: acetylcholinesterase inhibitors, NMDA receptor antagonists, peptide drugs, antioxidants, nootropics, antipsychotics and antidepressants with a pronounced anticholinergic effect, as well as those that alter drug absorption or reduce heart rate.
In accordance with the study protocol, patients were treated with Reminil for 3 months at a dose of 8 mg/day. (in 2 doses) in the 1st month of therapy and 16 mg/day. (in 2 doses) over the next 2 months.
Treatment efficacy was analyzed using the following clinical and psychometric scales: MMSE, ADAS-Cog and Activities of Daily Living (IADL), Behavioral Disorder in AD (BEHAVE-AD), and Clinical Global Impression (CGL). In addition, undesirable effects of therapy were recorded in a special table. The MMSE scale was assessed four times: at visit zero and then every month; on other scales - three times: at the “zero” visit, after 1 and 2 months.
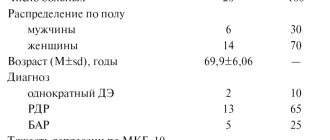
14 patients (7 men and 7 women) participated in the study. 4 of them were diagnosed with late-onset BA, 6 had SD and 4 had SMD. 11 patients had mild and 3 had moderate dementia. The average age of onset of the disease (onset of dementia) was 65.3 ± 6.4 years. The average age of patients at the start of therapy was 71.7 ± 7.8 years. The duration of dementia ranged from 2 to 10 years, on average - 5.8 ± 3.9 g. More than half of the patients (n = 8; 57%) suffered from one or another somatic disease, mainly arterial hypertension, coronary artery disease, cardiosclerosis, and vascular encephalopathy.
All patients completed a three-month course of treatment. SPSS 12 programs were used for statistical data processing.
The dynamics of the MMSE scale data was assessed based on the calculation of its total indicator; analysis of the results of the ADAS Cog, IADL and BEHAVE-AD scales was based on the difference in their total scores between the initial and follow-up assessments (Table 1). In this case, the average indicators of the mentioned scales were calculated by pairwise comparison of their initial value with each of the subsequent ones using the Wilcoxon method. CGL scale data were subjected to frequency (percentage) analysis.
The initial data demonstrate a significant correspondence between the severity of dementia and its assessment according to the MMSE and ADAS-Cog scales, which characterize various parameters of the cognitive functions of patients, as well as the IADL scale, which reveals the degree of adaptation in everyday life. A similar trend, which, however, did not reach the level of statistical significance, was observed according to the BEHAVE-AD scale, which records very heterogeneous symptoms, of which the most common in the patients we examined were mild (within 1-2 points) sleep disturbances (98 %), anxiety and phobias (78.5%), subdepression (64%), individual delusional symptoms (14.2%).
Research results
Figure 1 demonstrates statistically significant positive dynamics in the cognitive functioning of patients, according to the MMSE scale, both for the group as a whole and for mild and moderate dementia by the end of the first month of therapy. Noteworthy is the stabilization of this indicator after two months of therapy in patients with moderate dementia, while in patients with mild dementia a statistically significant increase in this indicator occurred throughout the entire observation period.
Information on the dynamics of the average difference in the total indicators of the ADAS-Сog, IADL and BEHAVE-AD scales is given in Table 2.
According to the ADAS-Cog scale, both in mild and moderate dementia, and in the group as a whole, a statistically significant improvement in the cognitive functions of patients was noted after 2 months of therapy. The rates of this improvement increased by approximately another half by the end of 3 months of therapy. The corresponding indicators of the BEHAVE-AD scale underwent similar dynamics, which indicated a reduction in the productive psychopathological symptoms and behavioral disorders associated with dementia. The IADL scale scores in patients with mild dementia demonstrated a significant improvement in the functional abilities of patients by the 2nd month of therapy, with a slight subsequent improvement by the end of the 3rd month. Whereas in patients with moderate dementia, such a trend was not observed, possibly due to the small number of patients.
According to the CGL scale (Figure 2), there was a varying degree of positive dynamics in the condition of patients in the group as a whole, both after 1 and after 3 months. therapy was observed in 80% of patients. In all types of dementia, minimal improvement prevailed, and there were no cases of worsening of the condition. Marked improvement was observed in only a third of patients with mild dementia by 2 months of therapy. Upon completion of therapy, improvement in overall condition was observed 2 times more often in mild than in moderately severe dementia.
Depending on the diagnostic affiliation of dementia, it was possible to compare the results of therapy only for mild dementia, since almost all cases of AD corresponded to mild dementia. Individuals with AD (n = 3) and AD (n = 4) selected for comparison differed in the age of onset of dementia (74.3 ± 9.8 and 66.5 ± 6.3 years, respectively), as well as in the age of the patients at the start of therapy (79.2 ± 11.5 and 70.75 ± 9.5 years, respectively).
According to the MMSE scale (Figure 3), with approximately the same score at the start of therapy in the AD and SoD groups after 3 months of therapy, the improvement in cognitive functions in SoD turned out to be more pronounced (by about 2.5 points) than in AD. A similar trend was noted according to the ADAS-Cog and IADL scales. The mean BEHAVE-AD total score improved more markedly in AD. However, the small number of observations makes statistical processing of data on the above scales incorrect. After 1 month of therapy, cases with minimal improvement were observed in BA, and cases with moderate improvement dominated in SoD. With SoD, already at this early stage of treatment, approximately 21% of patients showed a pronounced and 9% a moderate improvement.
In the 4 patients with SMD included in the study, the severity of dementia was mild. The average age at the onset of dementia was 64.0 ± 4.9 years, the average age of patients at the start of treatment was 67.75 ± 7.7 years.
Figure 4 demonstrates the positive dynamics of the cognitive functions of patients with SMD according to the MMSE scale; the improvement was almost 5 points compared to the initial assessment. A clear improvement in patients with SMD was also observed in terms of other scales, but it was especially noticeable at the end of therapy.
Adverse events
Moderately severe adverse events were observed in 2 patients (14.2%). In one case, nausea was noted, in the second - headache, difficulty falling asleep when the dose of the drug was increased in the second month of treatment. Reducing the daily dose of the drug (from 16 to 8 mg) led to the disappearance of adverse events and improvement in the patients' condition at the end of therapy, despite the use of a dose of 8 mg/day.
The discussion of the results
Thus, a clinical study of Reminil made it possible to establish its effectiveness in the treatment of the main types of dementia. According to the literature, the drug demonstrates a complex therapeutic effect on various components of dementia: cognitive and psychopathological disorders, behavioral disorders, and maladjustment of patients in everyday life. Significant improvement, according to our data, becomes obvious by the end of the first month of therapy and gradually increases by the time it is completed. Noteworthy is the stabilization of indicators after two months of therapy in patients with moderate dementia. It should be noted that, according to the CGI scale, there was not a single case of deterioration in the condition of patients in general, and some degree of improvement was detected in the majority of patients (80%).
Despite a fairly harmonious reduction in the manifestations of dementia in all its variants, the greatest therapeutic effect in relation to the state of cognitive functions and parameters of the general condition of patients was achieved in mild dementia (MMSE, ADAS-cog and CGI scales). A pronounced improvement was observed only in mild dementia (by the 2nd month of therapy in 1/3 of cases). Upon completion of therapy, improvement in overall condition was observed 2 times more often in mild than in moderately severe dementia.
The reduction of productive psychopathological symptoms and behavioral disorders accompanying dementia, according to the dynamics of the IADL and BEHAVE-AD scales, in patients with mild dementia was significant by the end of 3 months of therapy, while in patients with moderate dementia no such trend was noted.
An assessment of the effectiveness of galantamine therapy in patients with mild dementia in SoD and AD showed that in SoD, indicators of the cognitive sphere and everyday life skills improve more clearly (on the MMSE, ADAS-cog, IDAL scales). The condition of patients in general definitely improved by the second month of treatment with AD, and by the third month of treatment with AD.
In the studied sample of patients, moderately severe adverse events (mainly headache, nausea) were noted in two patients. They occurred when the dose of the drug was increased in the second month of treatment to 16 mg/day and disappeared after returning to the original dose. This makes it advisable to treat dementia even with low doses of the drug in cases where higher doses lead to adverse events.
Thus, this study demonstrated the greater effectiveness of treatment with galantamine SoD compared to BA and its good tolerability.