Appendicitis is a disease that manifests itself in the form of an inflammatory process that is localized in the appendix of the cecum - in the appendix. This disease is widespread in Russia. Appendicitis is one of the most common abdominal diseases. The only solution to this problem is surgery. The advanced form of the disease is dangerous due to the threat of rupture of the appendix, which can cause the death of the patient. What are the causes of appendicitis?
Where is the appendix located?
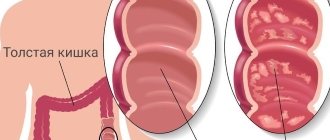
The appendix is an extension of the cecum
Its lower part descends to the pelvis. It can also be located behind the cecum. The organ is small in size: on average, 7-9 cm, its diameter is 0.5-1 cm. A small flap fold separates it from the cecum, preventing intestinal contents from entering the appendix.
Thanks to this, the appendix cavity remains clean. This organ also plays a role in digestion, being a kind of incubator for beneficial bacteria. Not all mammals have this organ.
For example, the cat family does not have this appendage. But rodents have it, for example, rabbits and guinea pigs. Human relatives according to the biological classification - monkeys - also have an appendix. Herbivores have a developed appendix.
How does appendicitis hurt?
Maximum pain during inflammation of the appendix occurs in the area where it is located, that is, slightly to the right of the umbilical cord. The pain of the appendix, raised closer to the liver, is not difficult to confuse with the pain of the liver itself. If the appendix is lowered to the pelvis, then its pain is masked as an ovarian pathology; in men, as an inflammation of the bladder. When the appendix is located posteriorly, the pain is localized in the lower back and felt in the groin.
Pain appears unexpectedly, without any particular reason. The inflammatory process can begin with mild or tolerable pain, followed by an increase, or it can immediately manifest itself with acute stabbing pain, which will be acute and unbearable as long as living nerve endings are sensitive. Therefore, when the appendix is inflamed, you cannot calm down if the pain subsides. On the contrary, the patient must be urgently hospitalized.
Appendicitis is also characterized by other symptoms: general malaise, nausea, and even single vomiting appear. Lost appetite. The temperature rises to 37.2-37.7o C and may be accompanied by chills. A light coating appears on the tongue. The heart rate increases to 90-100 beats per minute.
Reasons for the development of pathology
There are several causes of appendicitis
Although appendicitis is a disease that is fairly easy to treat, the exact cause of its occurrence is currently unknown. There are several main factors that can cause the development of appendicitis:
- mechanical
- vascular
- infectious
- immunological
- endocrine
Each of these factors must be considered separately.
Mechanical factor
It manifests itself in the form of blockage of the appendix, due to which the development of appendicitis begins. Obstruction of the appendix leads to the fact that the microflora it contains cannot leave the appendix, resulting in the development of an inflammatory process. Blockage of the appendix can be caused by:
Signs of peritonitis
Since, in case of untimely provision of medical care to the patient, perforation of the appendix and penetration of its contents into the peritoneum, leading to peritonitis, may occur, you should be aware that with peritonitis, the general condition of the patient sharply worsens. The eyes become sunken, the facial features become sharp. The patient begins to show anxiety, the heart rate increases sharply to 120 beats per minute. The pain spreads throughout the abdomen.
Acute appendicitis
In surgery, there is no disease more famous than acute appendicitis, but at the same time, in most cases, its recognition is difficult. This is due, on the one hand, to the fact that appendicitis, especially in the early stages of the disease, often does not have characteristic clinical manifestations, and on the other hand, to the fact that the doctor observing the patient has limited time to recognize the disease and choose treatment tactics. The latter circumstance excludes the use of any complex instrumental (except ultrasound) and laboratory techniques, therefore the diagnosis of acute appendicitis is based almost exclusively on data from questioning and physical examination.
History and general examination play an extremely important role in the diagnosis of acute appendicitis. The onset of pain in the epigastric region or throughout the abdomen with a gradual shift to the right iliac region (Kocher-Volkovich symptom) is characteristic of acute appendicitis and is rarely found in other diseases. Equally characteristic of appendicitis is scanty one- or two-time vomiting, which usually occurs in patients at home before admission to the surgical hospital.
An objective examination should first of all assess the general condition. It suffers little in case of catarrhal and phlegmonous appendicitis, but in its gangrenous form, despite the optimistic mood of the patient, it is possible to identify pallor, immobility, dry coated tongue, tachycardia and other signs of a systemic inflammatory reaction. The general condition suffers even more with perforated appendicitis. The patient is usually pale, indifferent, and sometimes groans in pain. Facial features are sharpened, knees are often brought to the stomach, pulse is significantly increased, blood pressure is lowered.
Examination of the abdomen in the catarrhal form of acute appendicitis does not reveal any features, but in the phlegmonous form it is possible to find some lag in the right iliac region during breathing. In the gangrenous form, this lag becomes easily noticeable, and in perforated appendicitis, the entire right half of the abdomen does not participate in breathing.
Palpation of the abdomen should be carried out carefully, otherwise incorrect data may be obtained due to the active resistance of the patient. First, superficial palpation is performed, which begins from the left iliac region, then, gradually moving to the right, a zone of hyperesthesia and local tension of the abdominal muscles in the right iliac region are identified.
After this, methodical deep palpation is performed according to Obraztsov-Strazhesko, which also begins with the left lower abdomen, and then, through deep step-by-step palpation, tenderness is detected in the right iliac region. With empyema of the appendix in thin people, it is possible to palpate the thickened appendix in the form of an elongated, mobile, painful formation. It should be remembered that deep palpation in destructive forms of appendicitis is often impossible due to pronounced pain and muscle tension.
By palpation, the symptoms of Voskresensky, Shchetkin-Blumberg, Rovzing, Sitkovsky, Bartomier-Mikhelson are first determined, and then the Obraztsov symptom. We must not forget about palpation of the right lumbar region, which can be crucial for recognizing the retrocecal form of acute appendicitis. In this case, soreness, muscle tension and the Shchetkin-Blumberg symptom will be determined accordingly in this zone.
Vaginal and rectal examinations are strictly required. Their value lies in the fact that they provide direct palpation of the lowest floor of the abdominal cavity. If the appendix is located in the pelvis or if there is an accumulation of purulent effusion here, these studies will reveal significant pain in the area of the posterior vaginal vault or the anterior wall of the rectum, as well as the characteristic fluid discharge. In addition, vaginal examination can play a decisive role in the differential diagnosis between acute appendicitis and inflammation of the uterine appendages.
The minimum tests required to establish a diagnosis of acute appendicitis include measuring body temperature and determining the leukocyte reaction. The temperature, as a rule, is elevated in any form of acute appendicitis, but it rarely exceeds 38 ° C. Only with a developing appendiceal abscess or diffuse peritonitis can the body temperature reach or exceed 39 ° C.
Leukocytosis is characteristic of all stages of acute appendicitis. We described the dynamics of its changes when covering the clinical forms of the disease. It is only necessary to add that in the diagnosis of acute appendicitis, leukocytosis has no independent significance, since it is also observed in other inflammatory diseases, and with the development of gangrene of the appendix, it may not be present at all. Much more important is the assessment of the white blood formula, in particular the presence or absence of a neutrophil shift: an increase in the content of young forms (band neutrophils, myelocytes and promyelocytes) to the detriment of the content of mature (segmented) neutrophils. With the rapid development of the destructive-inflammatory process, the total number of leukocytes can even be reduced (and sometimes significantly!), while young forms of neutrophils predominate in the white blood formula. This so-called leukocytosis of consumption reflects the extreme degree of strain on the hematopoietic system, when it is not able to fully provide the body’s needs during inflammation with the proper number of neutrophils. Therefore, in itself, a general decrease in the number of leukocytes in the peripheral blood against the background of a pronounced clinical picture of acute appendicitis cannot serve as a sign of the subsidence of the inflammatory process. Only an assessment of changes in the leukocyte formula can create a true idea of the positive or negative dynamics during an attack of acute appendicitis.
The diagnosis of acute appendicitis with a typical localization of the appendix is most difficult during the first hours of the disease, i.e. in the stage of “catarrhal” inflammation, since during this period the symptoms are nonspecific: the general condition of the patient suffers little, there are no symptoms of peritoneal irritation, etc. That is why With the catarrhal form of acute appendicitis, the largest number of diagnostic errors occurs. At best, this leads to unnecessary removal of the appendix. However, careful assessment of the history and physical examination, as well as the use of laparoscopy, greatly reduce the incidence of misdiagnosis and thus eliminate unnecessary appendectomies.
In the initial stage of the disease, when there are no signs of a destructive process and the diagnosis of acute appendicitis is in doubt, dynamic monitoring of the patient until clear manifestations of the disease appears. During this period, special studies can be carried out to facilitate the differential diagnosis: chromocystoscopy, excretory urography, laparoscopy, ultrasound scanning of the abdominal cavity.
Differential diagnosis
Acute appendicitis must be differentiated from almost all acute diseases of the abdominal cavity and retroperitoneal space. This, on the one hand, is facilitated by the extreme variability in the location of the appendix, and on the other hand, by the frequent absence of specific symptoms of the disease.
In the initial stage, when the pain does not yet have a clear localization in the right iliac region, but is observed mainly in the epigastric or mesogastric region, it is most often necessary to differentiate acute appendicitis from acute gastroenteritis, acute pancreatitis, and much less often from perforation of a stomach and duodenal ulcer.
Acute gastroenteritis, unlike acute appendicitis, begins with fairly severe cramping pain in the upper and middle parts of the abdomen. When questioned
The patient is almost always able to identify the provoking factor in the form of a change in diet, for example, taking a large amount of fatty and spicy foods, alcohol, etc. Almost simultaneously with cramping pain, repeated vomiting occurs, first of the food eaten, and then of bile. With significant damage to the gastric mucosa, vomiting mixed with fresh blood may occur. After a few hours, frequent loose stools often appear against the background of cramping pain.
During an objective examination of the abdomen, attention is drawn to the absence of localized pain, symptoms of peritoneal irritation and symptoms characteristic of acute appendicitis: Rovzing, Sitkovsky, Obraztsov, etc. During auscultation of the abdomen, increased peristalsis is heard. Digital rectal examination reveals the presence of liquid stool mixed with mucus, the absence of overhang and pain in the anterior wall of the rectum. Body temperature is usually normal or subfebrile. Leukocytosis increases moderately, band shift is absent or slightly expressed.
Acute pancreatitis, unlike acute appendicitis, begins with sharp pain, often of a girdling nature, in the upper abdomen. The pain often radiates to the back and is accompanied by repeated vomiting of bile, which does not bring relief.
In the initial stage of acute pancreatitis, patients behave restlessly, then, as intoxication increases, they become lethargic and adynamic; with a rapidly progressing disease, collapse may occur. The skin is pale, sometimes with some acrocyanosis, the pulse is significantly increased, while the temperature, at least during the first hours of the disease, remains normal.
During an objective examination of the abdomen, attention is drawn to the discrepancy between the severity of the general condition and the relatively unexpressed pain in the epigastric region. In the right iliac region there is most often no pain at all. Only in the late stages of acute pancreatitis, as the effusion spreads from the omental bursa and the right hypochondrium towards the right lateral canal and the iliac region, symptoms simulating acute appendicitis may appear. Meanwhile, in this case, the history of the disease, the presence of maximum pain in the epigastric region and symptoms characteristic of acute pancreatitis (absence of pulsation of the abdominal aorta in the epigastrium, the presence of painful resistance of the abdominal wall slightly above the navel and pain in the left costovertebral angle) will help to establish true diagnosis.
In difficult cases of differential diagnosis, laboratory assessment of the content of amylase (diastase) in the blood and urine is of great help. In particular, if the amylase content in the urine exceeds 128 units. (according to Wolgemut), then if there is doubt about the diagnosis, this fact indicates rather in favor of acute pancreatitis.
A perforated ulcer of the stomach or duodenum has such a characteristic clinical picture that it is almost difficult to mistake this complication of a peptic ulcer for acute appendicitis. The presence of the classic triad (gastric history, dagger pain in the epigastric region, widespread muscle tension), as a rule, allows you to immediately establish an accurate diagnosis. In addition, when an ulcer is perforated, vomiting is very rare and the disappearance of hepatic dullness is often detected - a symptom pathognomonic for perforation of a hollow organ.
Diagnostic doubts arise only in cases of covered perforation of the ulcer, when the stomach contents that have entered the abdominal cavity and the resulting effusion gradually descend into the right iliac fossa, where they are retained. Accordingly, the pain shifts: it subsides in the epigastric region after covering the perforation and, conversely, arises in the right iliac region as gastric contents penetrate into it. Such a false Kocher-Volkovich symptom can contribute to an incorrect conclusion about the presence of acute appendicitis and lead to an error in surgical tactics. The error is all the more possible because in the described situation, muscle tension and other symptoms of peritoneal irritation are clearly visible in the right iliac region: Shchetkin-Blumberg, Voskresensky, etc. Based on this, in this case, the assessment of the immediate and long-term history of the disease becomes extremely important. Long-term gastric discomfort or direct indications of a previous peptic ulcer, the onset of an acute disease not with dull, but with very sharp pain in the epigastric region, and the absence of vomiting do not indicate acute appendicitis. Doubts can be completely resolved by percussion or x-ray detection of free gas in the abdominal cavity.
Unfortunately, in a number of cases of covered perforation of an ulcer, simulating acute appendicitis, it is not possible to avoid a diagnostic error and a true diagnosis becomes possible only during surgery.
With an unusual localization of the appendix (under the liver, near the urinary tract, in the small pelvis), there is a need for a differential diagnosis between acute cholecystitis, urological and gynecological diseases.
Acute cholecystitis, unlike acute appendicitis, most often begins not with dull, but with very sharp pain in the right hypochondrium with typical irradiation to the right shoulder and scapula. This initial stage of acute cholecystitis, known as biliary (hepatic) colic, is often accompanied by repeated vomiting of food and bile.
When questioning the patient, as a rule, it turns out that such attacks of pain occurred more than once and their appearance was associated with a change in the usual diet: taking large amounts of fatty foods, smoked foods, and alcohol. Sometimes a history can establish the presence of transient jaundice that occurs shortly after an attack of pain. These anamnestic indications indicate acute cholecystitis.
When examining the abdomen, it should be taken into account that in the case of a high position of the appendix, maximum pain and muscle tension are localized in the lateral parts of the right hypochondrium, while with cholecystitis these signs are revealed more medially. In acute cholecystitis, it is often possible to palpate an enlarged and sharply painful gallbladder.
Body temperature in acute cholecystitis is significantly higher than in acute appendicitis in all stages of the disease, although in general the destructive process in acute cholecystitis develops more slowly than in appendicitis. As a rule, there is no significant difference in the dynamics of leukocytosis in both cases.
Valuable information can be obtained from ultrasound examination. It allows you to clearly visualize the gallbladder and detect signs typical of its inflammation (increase in the volume of the bladder, the thickness of its walls, layering of the walls, etc.). At the same time, hopes for ultrasound verification of the diagnosis of acute appendicitis are unjustifiably exaggerated, although this sometimes fails.
Right-sided renal colic, as a rule, begins not with dull, but with extremely sharp pain in the right lumbar or right iliac region. Often, against the background of pain, vomiting occurs, which is of a reflex nature. Pain in typical cases radiates to the right thigh, perineum, genitals and is accompanied by dysuric disorders in the form of frequent and painful urination. It should be noted that dysuric phenomena can also be observed in acute appendicitis if the inflamed appendix is in close proximity to the right kidney, ureter or bladder, but in this case they are less pronounced. In the differential diagnosis, an extremely important role is played by the anamnesis: as is known, with appendicitis there is never very severe paroxysmal pain with the irradiation described above. In addition, despite strong subjective pain, during a physical examination of a patient with renal colic, it is not possible to detect either intense pain in the abdomen or symptoms of peritoneal irritation.
Doubts can be resolved after a laboratory urine test and, if possible, urgent emergency urography or chromocystoscopy. Sometimes even macroscopically it is possible to note the intense red color of urine (macrohematuria), not to mention the fact that microscopy of urinary sediment almost always reveals an excess content of fresh red blood cells (microhematuria). Detection of a violation of the passage of urine in one of the ureters, established by urography or chromocystoscopy, in the presence of the pain syndrome described above, serves as a pathognomonic sign of renal colic. Sometimes routine radiography of the urinary tract helps to resolve diagnostic doubts, in which it is possible to notice the shadow of a radiopaque stone. An ultrasound examination brings some clarity to the diagnosis, revealing in a number of patients stones in the projection of the right ureter and an increase in the size of the right kidney.
Right-sided pyelitis (pyelonephritis) in relation to the differential diagnosis with acute appendicitis is a more difficult task than renal colic. The disease, as a rule, begins subacutely with dull arching pain in the lumboiliac or mesogastric region. Vomiting and dysuria are often absent at the onset of the disease. Only after 1-2 days does the body temperature rise sharply (up to 39°C and above). Of course, in this case, the medical history plays an important role, since pyelitis is most often a consequence of impaired urination as a result of urolithiasis, pregnancy, prostate adenoma, etc.
Even in the presence of obvious signs of purulent intoxication, it will not be possible to detect sharp pain on palpation of the abdomen and symptoms of peritoneal irritation. At the same time, it should be noted that with pyelitis, pain in the mesogastric region, iliac region and a positive psoas-symptom of Obraztsov is often determined.
As with renal colic, urine testing plays an important role in the differential diagnosis of pyelitis and acute appendicitis, which can reveal pyuria. Survey and contrast urography for pyelitis are less important than for renal colic, although they often reveal unilateral or bilateral pyelectasis in the patient, which can also be determined by ultrasound.
Features of the differential diagnosis of acute appendicitis and gynecological pathology are presented in Chapter XVIII.
Clinical manifestations of other acute but rare diseases of the abdominal organs: terminal ileitis (Crohn's disease) in its initial stage, Meckel's diverticulitis , etc. do not have any characteristic differences from the signs of acute appendicitis, therefore the correct diagnosis is most often established only during operations.
A great help in difficult cases of differential diagnosis in acute pathology of the abdominal organs is laparoscopy, which is becoming increasingly widespread in surgical hospitals. Laparoscopic examination should be carried out in the operating room in such a way that, if necessary, emergency surgery, including laparoscopic appendectomy, can be started immediately. From the same point of view, it is advisable to perform laparoscopy under general anesthesia.
The differential diagnosis between acute appendicitis and right-sided pyelitis in the second half of pregnancy presents certain difficulties, since the diseases have many similar features: mild pain, high localization of pain, and the presence of vomiting. As for the dysuric phenomena inherent in pyelitis, they can also be observed in acute appendicitis due to the close proximity of the appendix and the right kidney in late pregnancy.
An objective examination of the abdomen indicates the presence of highly localized tenderness, and since the ileocecal angle is located behind the sharply enlarged uterus, symptoms of peritoneal irritation may not be detected for a long time.
Only the onset of the disease is significantly different: it is known that appendicitis always begins with pain, followed by an increase in body temperature and vomiting, while with pyelitis the disease most often begins with severe chills, vomiting, an increase in temperature, and only after this does pain occur. With a careful objective examination, it is possible to notice that the maximum pain in the case of pyelitis in pregnant women is closer to the lumbar region, while in case of appendicitis it is detected in the area of the lateral and anterior wall of the abdomen. Palpation of the abdomen with the patient on the left side can help in correct orientation; in this case, due to some displacement of the uterus to the left, it is possible to palpate the area of the vermiform appendix and the right kidney in more detail. It is also important to examine urine (necessarily taken with a catheter!), which can detect the presence of pyuria as a sign of purulent pyelonephritis, as well as an ultrasound examination that reveals changes in the pyelocaliceal system of the right kidney. However, if doubts remain, it is better for the patient to undergo surgery rather than undergo conservative treatment with the risk of developing appendiceal peritonitis. In pregnant women, surgical tactics should be more active than in other categories of patients.
With regard to pain relief in pregnant women, the rule remains the same as outside pregnancy: for any form of acute appendicitis, general anesthesia should be preferred.
As a surgical approach for an undoubted diagnosis in the first half of pregnancy, the Volkovich-Dyakonov incision is used. In the second half of pregnancy, this access may be inadequate, so it is modified according to the principle: the longer the pregnancy, the higher the incision. Thus, in the last weeks of pregnancy, the incision is made above the ilium due to a significant upward displacement of the cecum and appendix. It is advisable to expand the Volkovich-Dyakonov incision by incising the edge of the sheath of the right rectus abdominis muscle.
Surgical tactics for any form of appendicitis in pregnant women do not differ from the generally accepted principles of its treatment. In other words, the features of the surgical technique and methods of drainage of the abdominal cavity, adopted for various forms of acute appendicitis, fully retain their significance here. It is only necessary to exercise maximum caution when manipulating near an enlarged uterus, since trauma to it can be a direct cause of miscarriage or premature birth. For the same reasons, abdominal tamponade is carried out according to the strictest indications: 1) if it is impossible to achieve reliable hemostasis in the abdominal cavity; 2) when opening a circumscribed periappendiceal abscess.
In the postoperative period, in addition to conventional therapy, it is necessary to prescribe treatment aimed at preventing premature termination of pregnancy. Strict bed rest is prescribed, administration of a 25% solution of magnesium sulfate 5-10 ml 2 times a day intramuscularly, administration of tocopherol acetate at a dose of 100-150 mg per day as an injection of a 10% oil solution 1 ml 1 time. In the absence of laboratory monitoring of hormonal levels, the prescription of hormonal drugs (progesterone, etc.) should be avoided, since in some cases an overdose can have the opposite effect. The administration of proserin and hypertonic sodium chloride solution as agents that promote uterine contraction is strictly contraindicated. For the same reason, hypertensive enemas should not be used.
In pregnant women, the most difficult task is the treatment of diffuse peritonitis. Mortality from this complication remains very high and, according to various authors, is 23-55% for the mother and 40-92% for the fetus, with the highest mortality observed in late pregnancy. Unfavorable results of treatment of diffuse purulent peritonitis in pregnant women gave rise to extreme radicalism in surgical tactics. It was considered necessary to perform the following volume of surgical intervention: immediately after opening the abdominal cavity, perform a cesarean section, then supravaginal amputation of the uterus, then appendectomy, toilet and drainage of the abdominal cavity. Currently, thanks to the availability of powerful antibacterial agents, in most such cases it is possible not to resort to a cesarean section, much less subsequent amputation of the uterus. It must be emphasized that the question of the volume and nature of intervention for destructive appendicitis against the background of long periods of pregnancy should be resolved together with an obstetrician-gynecologist, with his direct participation in surgical intervention. Briefly, the principle of modern surgical tactics can be formulated as follows: maximum activity in relation to peritonitis, maximum conservatism in relation to pregnancy.
In modern conditions, with diffuse appendicular peritonitis in pregnant women, a median laparotomy, evacuation of pus, appendectomy, abdominal toilet, and drainage are installed under general anesthesia. The surgical wound is sutured tightly. In case of full-term or almost full-term pregnancy (36-40 weeks), due to the inevitability of childbirth against the background of peritonitis, the operation begins with a cesarean section, then after suturing the uterus and peritonization of the suture, an appendectomy and all further manipulations associated with the treatment of peritonitis are performed.
The urgent need for amputation of the uterus arises only when it is destructively damaged, which is occasionally observed in conditions of diffuse purulent peritonitis. It should also be taken into account that with diffuse purulent peritonitis, the contractility of the uterus is significantly reduced. In this regard, sometimes after a cesarean section there is a danger of atonic bleeding, the only way to combat which is immediate amputation of the uterus.
Acute appendicitis during childbirth deserves special attention In the literature, there are conflicting opinions about when in such cases it is necessary to perform an appendectomy: before or after delivery, whether to allow childbirth to proceed naturally, or to perform a cesarean section and appendectomy at the same time. In this regard, it should be noted that surgical tactics for appendicitis during childbirth depend both on the course of labor and on the clinical form of acute appendicitis. So, if childbirth proceeds normally with the clinical picture of catarrhal and phlegmonous appendicitis, then it is necessary to promote the fastest natural delivery and then perform an appendectomy. If, against the background of the normal course of labor, there is a clinical picture of gangrenous or perforated appendicitis, then it is necessary to temporarily stop the contractile activity of the uterus, perform an appendectomy and then again stimulate labor. In conditions of pathological childbirth, it is necessary to perform a simultaneous cesarean section and appendectomy for any clinical form of acute appendicitis.
Regardless of the timing of delivery, the patient must be transferred to the surgical department for appendectomy and subsequent postoperative management, where she must be observed by both a surgeon and a gynecologist.
Acute appendicitis in children is much less common than in adults. The vast majority of cases occur over the age of 5 years. The rarity of acute appendicitis before the age of 5 is explained by the fact that the appendix has a funnel-shaped shape, which facilitates good emptying of the appendix, and also by the fact that the lymphoid apparatus of the appendix is still poorly developed during this period of life.
Acute appendicitis in children occurs more violently than in adults. This is due to the child’s body’s insufficient resistance to infection, weak plastic properties of the child’s peritoneum, and insufficient development of the omentum, which does not reach the appendix and thus does not participate in the creation of a delimiting barrier.
The pain that arises in the abdomen is often cramping in nature and does not have the clear dynamics that are characteristic of acute appendicitis in adults. It should be noted that children under 10 years of age, as a rule, cannot accurately localize pain, which makes it difficult to recognize the disease. Vomiting in children is most often repeated, stools do not tend to be delayed, and in young children they even become more frequent. The posture of a sick child is characteristic. He lies on his right side or on his back, bringing his legs to his stomach and placing his hand on the right iliac region, protecting it from examination by a doctor. With careful palpation, it is often possible to identify hyperesthesia, muscle tension and the area of greatest pain. Even in the first hours of the disease, symptoms of Shchetkin-Blumberg, Voskresensky, Bartomier-Mikhelson are pronounced.
The temperature from the very beginning of the disease is significantly higher than in adults, often reaching and exceeding 38°C. The number of leukocytes is also increased, but it rarely exceeds 20x109/l along with the existing neutrophil shift.
In the differential diagnosis of acute appendicitis in children, the following diseases deserve attention: pleuropneumonia, acute gastroenteritis, dysentery, hemorrhagic vasculitis (Henoch-Schönlein disease).
When differentiating pleuropneumonia , it must be taken into account that this disease is characterized not only by pain spreading towards the abdomen, but also by cough, sometimes with transient cyanosis of the lips, wings of the nose and shortness of breath. It should be recalled that in children the normal ratio of breathing to pulse is 1:4, and if
the ratio becomes 1:3 or 1:2, then this rather speaks in favor of acute pneumonia. With pleuropneumonia, you can also listen to rales and pleural friction sounds on the corresponding side of the chest.
When differentiating gastroenteritis , it must be taken into account that this disease begins, as a rule, not with abdominal pain, but with vomiting and the appearance of characteristic repeated watery stools; pain, unlike acute appendicitis, comes later. In addition, with gastroenteritis they have a pronounced cramp-like character, often followed by the urge to stool. The temperature in this disease is elevated, as in appendicitis, but the number of leukocytes is normal or even slightly reduced, and the neutrophil shift is not pronounced.
The need to differentiate acute appendicitis from dysentery occurs most often in the younger age group. Here, first of all, the anamnesis plays a role, in particular, indications that a similar disease appeared in several children at once, especially in children's groups. The pain in dysentery is clearly cramping in nature and is localized mainly in the left half of the abdomen; repeated loose stools are often accompanied by blood. Maximum palpation pain is determined in the lower abdomen on the left; symptoms of peritoneal irritation, with rare exceptions, are not detected. Body temperature during dysentery is often high (38.0-39.0 ° C), the number of leukocytes can be increased without a significant neutrophil shift.
To exclude hemorrhagic vasculitis , take into account that abdominal pain in this disease is caused by multiple small subserous hemorrhages and does not have a clear localization. In addition, a careful examination of the skin allows us to identify the presence or residual effects of hemorrhagic exanthema in symmetrical areas of the torso, limbs, and buttock areas. You should also pay attention to the mucous membrane of the cheeks and sublingual space, where it is possible to detect the presence of small submucosal hemorrhages even before the appearance of a rash on the skin. The abdominal wall is not tense during the examination, but the Shchetkin-Blumberg symptom is most often pronounced, the abdomen is distended and uniformly painful. A rectal examination may reveal bloody intestinal contents. Body temperature sometimes reaches 38°C and higher, the number of leukocytes is also most often increased without a significant neutrophil shift.
In case of significant difficulties in the differential diagnosis, if there are no symptoms of peritoneal irritation, dynamic observation of the child for 6-12 hours is acceptable.
At the same time, it should be remembered that appendicitis in children occurs much more violently than in adults, and often within the first day of the disease destruction of the appendix develops. Based on this, surgical tactics in children should generally be more active than in adults.
All this fully applies to appendicular infiltrate, which in children often forms already on the 2nd day of the disease. Since in children the appendix is relatively long, and the omentum, on the contrary, is short and the peritoneum does not have sufficient plastic properties, the resulting infiltrate is “fragile” and cannot serve as a reliable obstacle to the spread of infection throughout the abdominal cavity. In this regard, the operation is indicated even with a forming (palpable) appendiceal infiltrate, especially since isolating the appendix from loosely fused organs is not particularly difficult.
Appendectomy in children is always performed under general anesthesia. The Volkovich-Dyakonov incision is used as an operative access, with the exception of cases of diffuse purulent peritonitis, when a lower-median laparotomy is indicated.
In most cases, appendectomy in children is not technically difficult due to the absence of adhesions.
Signs of appendicitis in children
Symptoms of appendicitis are quite characteristic
If an adult can explain where, what and how it hurts, then with a child everything is much more complicated. And the younger the child, the more difficult it is to conduct an anamnesis. He cannot explain either the nature of the pain or its location. The child just hurts everything.
But, having heard that they are leaving him in the hospital and that something will be cut out, the baby may unexpectedly “get well.” Don't flatter yourself. The child does not understand that his deception may cost him his life. He wants to return to his usual life, and be closer to his mother, to his family, to everything that promises him warmth and security.
He may begin to be capricious and throw a tantrum demanding to be taken home. Explain to him that the subsided pain is the death of the nerve endings that should feel pain, and that if he does not listen to the doctor, he may die. Try to be with your child at these moments.
Diagnosis by named symptoms
The symptoms of appendicitis according to the authors who discovered them and proposed to take them into account to identify appendicitis and its differential diagnosis with other diseases remain valid to this day. They are checked by surgeons even with the availability of ultrasound and laboratory tests. In such cases, a conservative approach, taking into account the experience accumulated over the years, is justified.
The Shchetkin-Blumberg sign is checked for any suspicion of peritoneal involvement
The methods only emphasize that once upon a time doctors could only rely on themselves, their knowledge and observations. Here are several symptoms that, according to the authors, indicate acute appendicitis.
- Shchetkin-Blumberg - you need to lightly and gradually press on the abdominal wall, then sharply withdraw your hand; peritoneal inflammation is characterized by pain when the pressure is relieved, and not during palpation.
- Voskresensky - being to the right of the patient, the doctor should pull his shirt by the bottom edge with his left hand, and with his right hand make a sharp sliding movement along the tissue above the abdomen from top to bottom, stopping in the iliac fossa. A positive symptom is manifested by increased pain when the sliding stops.
- Rovzinga - when pressing with one hand on the left on the area of the descending colon with the other - a short push is made, while in patients with appendicitis pain appears on the right.
- Razdolsky - the author used percussion of the abdomen, the method gave a positive result in increasing pain over the projection of the appendix.
- Ortner-Sitkovsky - the patient is asked to turn on his left side, while he experiences nagging pain in the right side.
- Obraztsova - increased pain on palpation in the right lateral area against the background of a raised leg straightened at the knee.
- Mikhelson - helps in diagnosing inflammation of the appendix in pregnant women, the author noticed increased pain when the woman was positioned on the right side, due to the pressure of the enlarged uterus on the inflammatory focus.
- Pasternatsky - tapping the lumbar region causes pain in the abdomen, is used not only in the diagnosis of kidney diseases, but also to identify the retroperitoneal position of the inflamed appendix.
- Volkovich - the author pointed out that in patients with chronic appendicitis, the abdomen looks sunken in the right lateral and subcostal region due to a softer abdominal wall.
- Lanza - a painful point characteristic of the disease is determined, mentally you need to connect the protruding upper ends of the iliac bones with a line, the point lies at the junction of the outer and middle third on the right.
Obraztsov's symptom helps in differential diagnosis