Methotrexate
Patients should be clearly informed that the drug should not be used daily, but once a week .
Patients receiving Methotrexate therapy should be closely monitored to ensure that signs of potential toxicity and adverse reactions are identified and assessed promptly.
Methotrexate should only be prescribed by a medical specialist with sufficient knowledge and experience in antimetabolic therapy.
Due to the possible development of severe or even fatal adverse reactions, patients should be fully informed by their physician about the possible risks and recommended safety measures.
The use of the drug in children under 3 years of age is not recommended due to insufficient data on the effectiveness and safety of treatment in this group of patients.
Recommended examinations and safety measures
Before starting or resuming treatment with methotrexate, a complete clinical blood test should be performed with a count of blood cells, including a platelet count; biochemical blood test with determination of liver enzyme activity, bilirubin concentration, serum albumin; chest x-ray, kidney function test. If necessary, diagnostic measures are taken to assess the activity of tuberculosis infection and viral hepatitis.
During treatment (at least once a month in the first six months of treatment, then at least once every three months), it is necessary to carry out the studies described below.
If the dose of methotrexate is increased, the frequency of examinations should be increased.
1. Examination of the oral mucosa and pharynx to assess the condition of the mucous membrane (stomatitis, pharyngitis).
2. Detailed clinical blood test with counting of blood cells, including determination of platelet count. Suppression of hematopoiesis caused by methotrexate can occur suddenly, including when the drug is used in small doses. In any case of a significant decrease in the number of leukocytes or platelets, it is necessary to immediately interrupt treatment with methotrexate and carry out adequate supportive therapy. Patients should be advised to report any signs and symptoms of possible infections.
Patients concomitantly using drugs that inhibit hematopoiesis (for example, leflunomide) should be carefully monitored with monitoring of blood counts, including platelet counts.
3. Liver function tests: Particular attention should be paid to identifying possible toxic effects on the liver. Treatment should not be started or should be interrupted if, during appropriate examinations or liver biopsy, abnormal liver function is detected that was present before the start of treatment or developed during treatment. Typically, disorders that develop during treatment return to normal within two weeks after interruption of methotrexate therapy, after which, at the discretion of the attending physician, treatment can be resumed.
When methotrexate is used for rheumatological indications, there is no obvious need for liver biopsy to monitor liver toxicity.
The advisability of performing a liver biopsy in patients with psoriasis is associated with the issue of the effectiveness of routine chemical analyzes of liver parameters or studies of type III collagen propeptide for identifying and assessing hepatotoxicity. Appropriate assessment should be carried out individually for each case, differentiating patients depending on the presence or absence of risk factors, such as a history of excessive alcohol consumption, persistent elevation of liver enzymes, history of liver disease, hereditary predisposition to liver disease, diabetes mellitus, obesity, history of use of hepatotoxic drugs or drugs that affect hematopoiesis, long-term previous use of methotrexate, or use of methotrexate in a cumulative dose of 1.5 g or more.
Control of “liver” enzymes in the blood serum: in 13 - 20% of patients, a transient 2-3-fold excess of normal transaminase values was reported. In the case of a persistent increase in liver enzyme activity, dose reduction or discontinuation of treatment should be considered.
Due to the possible toxic effects of the drug on the liver, patients during treatment with methotrexate, unless clearly necessary, should refrain from the simultaneous use of other hepatotoxic drugs; Alcohol consumption should also be avoided or at least significantly reduced.
In patients using other hepatotoxic drugs or drugs that inhibit hematopoiesis (for example, leflunomide), the activity of liver enzymes should be carefully monitored.
4. It is necessary to monitor kidney function by performing functional tests and urine analysis.
Since methotrexate is excreted primarily by the kidneys, in the case of insufficient renal function, an increase in the plasma concentration of methotrexate should be expected, which can lead to severe unwanted side effects.
In cases of possible decline in renal function (for example, in elderly patients), control examinations should be performed more frequently. This also applies to cases of simultaneous administration of drugs that affect the elimination of methotrexate, drugs that can lead to kidney damage (for example, NSAIDs), or drugs that can affect hematopoiesis.
Dehydration may also increase the toxicity of methotrexate.
5. Examination of the respiratory system: special attention should be paid to symptoms of deterioration in lung function, and appropriate tests should be carried out if necessary. Symptoms of respiratory system damage (especially dry nonproductive cough), nonspecific pneumonitis that occur during methotrexate therapy may indicate a potentially dangerous disease and require interruption of treatment and immediate thorough examination to make a diagnosis. Acute or chronic interstitial pneumonitis may develop, often accompanied by eosinophilia; associated deaths have been reported. Clinical symptoms of methotrexate-induced lung injury are varied, but typical signs are fever, cough, difficulty breathing, and hypoxemia. An X-ray examination of the chest is necessary to exclude the presence of infiltrates or infection.
In case of lung disease, rapid diagnosis and discontinuation of treatment are necessary.
The development of respiratory diseases caused by the use of methotrexate is possible at any dose of the drug used.
If the dose of methotrexate is increased, the frequency of examinations should be increased!
Methotrexate affects the immune system and, as a result, may impair the response to vaccination and affect the results of immunological tests. Particular caution is required when using the drug in patients with chronic infectious diseases outside periods of exacerbation (Herpes zoster, tuberculosis, hepatitis B or C) due to the possibility of exacerbation of the disease.
Refusal from immunization is required.
Malignant lymphomas may occur in patients using low doses of methotrexate; in these cases, treatment should be discontinued. In the absence of signs of spontaneous regression of lymphoma, cytotoxic therapy is necessary. Rare cases of acute megaloblastic pancytopenia have been reported when folic acid antagonists (such as trimethoprim/sulfamethoxazole) were co-administered with methotrexate.
The use of methotrexate increases the likelihood of developing dermatitis and skin burns under the influence of solar irradiation and UV irradiation.
In patients with psoriasis, an exacerbation of the disease may occur as a result of UV irradiation during treatment with methotrexate (photosensitivity reaction).
In patients with an additional volume of distribution (presence of pleural effusion, ascites), the elimination of methotrexate is slowed down. In such patients, particularly careful monitoring of toxicity, dose reduction, and in some cases, discontinuation of methotrexate treatment is required. Before starting therapy with Methotrexate, effusion from the pleural or abdominal cavity should be drained.
If diarrhea and ulcerative stomatitis occur, methotrexate therapy must be interrupted, since in such cases the development of hemorrhagic enteritis and death as a result of interstitial perforation are possible.
Vitamin supplements and other products containing folic acid, folinic acid or their derivatives may reduce the effectiveness of methotrexate.
In patients with psoriasis, methotrexate should be used only in cases of severe, persistent, disabling forms of the disease that are difficult to treat with other treatment regimens, and only after confirmation of the diagnosis by biopsy and/or after consultation with a dermatologist.
The drug contains less than 1 mmol of sodium per dose, i.e. practically free of sodium, which is important for patients on a sodium diet.
Before prescribing the drug, women need to make sure that they are not pregnant, since methotrexate is embryotoxic and can cause abortions and fetal defects. Methotrexate affects spermatogenesis and oogenesis, which may lead to decreased fertility during treatment. These effects are reversible after discontinuation of therapy.
Patients of childbearing potential of both sexes should use reliable contraception during treatment with methotrexate and for at least 6 months after its completion.
Patients of childbearing potential and their partners should be properly informed of the possible risks to fertility and pregnancy associated with the use of methotrexate.
Pharmacodynamics and pharmacokinetics
The maximum concentration in the blood of Methotrexate occurs after 30-60 minutes. In patients with leukemia, there may be fluctuations of up to 3 hours.
In blood plasma it binds to albumin. When taken simultaneously with salicylates, chloramphenicols, sulfonamides, tetracyclines, phenytoin, competitive substitution may occur.
Methotrexate does not penetrate the blood-brain barrier; for this it must be administered intrathecally.
The half-life of Methotrexate is about 6-7 hours, in the case of high doses it increases to 17 hours. It is excreted mainly (90%) by the kidneys during the day. About 10% is excreted in bile.
In case of severe renal impairment, excretion is prolonged.
Methotrexate can accumulate in the liver, kidneys and spleen as metabolic products.
Methotrexate price, where to buy
You can buy Methotrexate Ebewe Austria in Moscow for an average of 1,100 rubles. in ampoules. The price in tablets is about 2000 rubles. for 50 tab. dose of 5 mg and 3000 rub. for a dosage of 10 mg.
The price in Ukraine of the drug depends on the volume and quantity in the package and ranges from 200 to 800 UAH.
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
- Online pharmacies in KazakhstanKazakhstan
LuxPharma* special offer
- Methotrexate Ebewe (Austria) 5 mg 50 pcs
1980 rub. order - Methotrexate Ebewe (Austria) 10mg 50pcs
2900 rub. order
- Methotrexate Ebewe (Austria) 2.5 mg No. 50
1850 rub. order
ZdravCity
- Methotrexate tablets p.p.o. 2.5 mg 50 pcs. Ozone LLC
RUB 284 order
- Methotrexate-SZ tablets p.p.o. 2.5 mg 50 pcs. Northern Star JSC
RUB 198 order
- Methotrexate-Kelun-Kazpharm solution for injection 10mg/ml 1mlKelun-Kazpharm Limited Liability Partnership
RUB 837 order
- Methotrexate-Kelun-Kazpharm solution for injection 10mg/ml 2mlKelun-Kazpharm Limited Liability Partnership
RUB 1,051 order
Pharmacy Dialogue
- Methotrexate-SZ (tab.p.pl/vol. 2.5 mg No. 50 (blister)) Northern Star JSC
RUB 218 order
- Methotrexate (tablet p/o 2.5 mg No. 50) Ozon LLC
RUB 265 order
- Methotrexate-Ebewe injection solution syringe 10mg/ml 1ml No. 1 + automatic protection needleEBEWE Pharma
RUR 752 order
- Methotrexate-Ebewe (solution d/in. syringe 10 mg/ml 2 ml No. 1)EBEWE Pharma
RUB 1,037 order
- Methotrexate-Ebewe (injection solution 10 mg/ml 1.5 ml No. 1 + auto-protected needle) EBEWE Pharma
RUR 886 order
show more
Pharmacy24
- Methotrexate Ebewe 10 mg No. 50 tablets EBEVE Pharma Ges.m.b.H.Nfg.KG, Austria/Haupt Pharma Amareg GmbH (“in bulk”), Germany
801 UAH.order - Methotrexate Ebewe 5 mg No. 50 tablets EBEVE Pharma Ges.m.b.H.Nfg.KG, Austria/Haupt Pharma Amareg GmbH (“in bulk”), Nimeczina
612 UAH. order
- Methotrexate-TEVA 100 mg/ml 10 ml solution
662 UAH. order
- Methotrexate-TEVA 25 mg/ml 2ml solution for injection
123 UAH order
- Methotrexate Ebewe 2.5 mg No. 50 tablets EBEVE Pharma Ges.m.b.H.Nfg.KG, Austria/Haupt Pharma Amareg GmbH (“in bulk”), Nimeczina
335 UAH. order
PaniPharmacy
- METHOTREXATE tablets Methotrexate Ebeve tablets. 2.5 mg No. 50 Austria, Ebewe Pharma
359 UAH. order
- METHOTREXATE tablets Methotrexate Orion tablets. 2.5 mg No. 100 Finland, Orion
349 UAH order
- METHOTREXATE bottle Methotrexate solution for injection 100 mg/ml bottle 10 ml No. 1 Netherlands, Pharmachemie
721 UAH. order
- METHOTREXATE tablets Methotrexate Orion tablets. 2.5 mg No. 30 Finland, Orion
173 UAH order
- METHOTREXATE tablets Methotrexate Ebeve tablets. 10 mg No. 50 Austria, Ebewe Pharma
834 UAH. order
show more
Instructions for use of Methotrexate (Method and dosage)
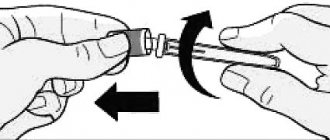
It is possible to administer Methotrexate Ebeve intramuscularly, intraarterially, intravenously or intrathecally. The tablets are not chewed, take before meals.
The instructions for Methotrexate warn that the selection of doses and treatment regimens for each specific pathology should be carried out strictly in accordance with special literature.
In the case of trophoblastic tumors, up to 30 mg is administered intramuscularly daily for a course of 5 days. Courses are repeated after 1 week until a dose of 400 mg is reached.
Lymphomas and leukemia require intravenous administration of 200-500 mg per m2 once a month.
Neuroleukemia: administered intrathecally 1 – 2 times every 7 days at a dose of 12 mg per m2.
Children are prescribed the following doses:
- under 1 year 6 mg;
- age 1 year – 8 mg;
- up to 2 years use 10 mg;
- over 3 years old, 12 mg is administered.
Methotrexate for rheumatoid arthritis is prescribed starting with a dose of 7.5 mg, once a week. According to indications, the dose is increased, but not more than 20 mg per week.
For psoriasis, a dose of up to 25 mg per week is prescribed, intramuscularly or intravenously.
For mycosis fungoides, administer 50 mg per week once or in 2 doses, intramuscularly.
Indications for use
- trophoblast tumors;
- neuroleukemia;
- non-Hodgkin's lymphoma , incl. lymphosarcoma ;
- acute leukemia (myeloblastic and lymphoblastic);
- osteogenic soft tissue sarcoma;
- skin cancer , lung cancer , breast cancer , squamous cell cancer, genital cancer (male and female), bladder cancer, esophageal cancer , kidney cancer, medulloblastoma, retinoblastoma;
- severe stages of mycosis , psoriasis ;
- arthritis , systemic lupus erythematosus, dermatomyositis , ankylosing spondylitis .