Composition and dosage forms
The drug is available in the form of tablets for oral administration: white or cream-colored, biconvex, with a characteristic medicinal odor. Dosage of the active component: 50 and 150 mg.
The active ingredient of the drug is tolperisone hydrochloride, which has a relaxing effect on the fibers of muscle tissue. Each tablet, in addition to the active component, contains auxiliary and formative components:
- lactose;
- lemon acid;
- stearic acid;
- crospovidone.
The drug shell contains: talc, titanium dioxide, polyvinyl chloride and other components.
Mechanism of action of the drug Tolperisone
The drug selectively inhibits the activity of parts of the brain responsible for regulating the motor functions of muscles. It has a central anticholinergic effect, has a slight antispasmodic effect, expands the lumen and reduces vascular tone. Tolperisone does not affect the activity of the peripheral nervous system.
The drug tablets dissolve and are absorbed into the blood in the gastrointestinal tract. Their active component has a bioavailability of about 20%. The effect of the medicine begins 20–30 minutes after administration, reaching a maximum within 1–1.5 hours. The effect lasts 4–5 hours. The medication does not accumulate in the body. All its substances are transformed in the liver. Metabolites are excreted through the kidneys in the urine within 6–8 hours.
Material and methods
A prospective study of complex conservative therapy was conducted in two pools of patients with early stages of coxarthrosis for the period from 2014 to 2022. with a substantive assessment of the articular component of treatment. Conservative treatment of the first comparison group was carried out according to the generally accepted scheme, taking into account the individual characteristics of each patient; in the second observation group, along with NSAIDs and chondroprotectors, the original oral centrally acting muscle relaxant tolperisone (Mydocalm) was used.
Inclusion criteria:
OA of the hip joint of the I, II and early III stages, occurring with periods of very pronounced exacerbation (usually seasonal), persistent synovitis, moderate inflammatory changes in the hemogram (leukocytosis up to 11·109/l without a shift in the leukocyte formula, acceleration of ESR up to 20– 35 mm/h, increase in CRP by 1-3 mg/l).
Exclusion criteria:
To randomize the study, the pools did not include patients with a specific genesis of the pathology (secondary OA), as well as with contraindications (NSAID gastropathy, a history of gastric and duodenal ulcers) or intolerance to physical methods of treatment, or to certain drugs of the complex regimen therapy.
Aceclofenac (Aertal) in the form of tablets at a dose of 200 mg/day in two doses was used as a representative NSAID. The chosen chondroprotectors were a combination of chondroitin sulfate at a dose of 500 mg/day in two doses, glucosamine at a dose of 1500 mg/day in one dose and a 1.5% solution of sodium hyaluronate (30 mg) in the form of sodium salt of hyaluronic acid (double intra-articular injection).
In the modified regimen, a centrally acting muscle relaxant was added to these drugs—oral administration of tolperisone (Mydocalm) at a dose of 150 mg/day in three doses. Mydocalm has a membrane-stabilizing, local anesthetic effect, inhibits the conduction of impulses in primary afferent fibers and motor neurons, which leads to blocking of spinal mono- and polysynaptic reflexes. It also secondarily inhibits the release of mediators by inhibiting the entry of Ca2+ through channels into synapses. In the brain stem, the conduction of excitation along the reticulospinal tract is inhibited. Increases peripheral blood flow regardless of the influence of the central nervous system. A weak antispasmodic and adrenergic blocking effect plays a role in the development of this effect.
The indications for the use of Mydocalm include the treatment of increased tone and muscle spasms accompanying diseases of the musculoskeletal system, including arthrosis of large joints.
The effectiveness of therapy was assessed using clinical, paraclinical and laboratory criteria. Clinically, changes in the range of motion of the diseased joint (amplitude in degrees) and the dynamics of synovitis were determined according to ultrasound data. The dynamics of pain syndrome were assessed using a visual analogue scale (VAS). All criteria were studied before the start of treatment and on the 12th day from the start of therapy. The nonspecific inflammatory process was assessed using ESR and CRP.
As a result, the first comparison group included patients ( n
=36), who were prescribed a standard therapy regimen.
The second (main) group was formed from patients ( n
= 32) who were additionally prescribed Mydocalm (Table 1). As can be seen from the table, in both groups of patients, women aged 55-64 years prevailed with a disease duration of 2 years, the second stage of the degenerative process and a pronounced phase of its exacerbation.
Table 1. General characteristics of the study population of patients (n=68)
For what diseases is Tolperisone indicated?
It is recommended to use the drug in the following conditions:
- increased tone, muscle spasms;
- spastic contractures of the limbs;
- cerebral palsy;
- dysfunction of the spinal cord;
- rigidity, muscle dystonia;
- obliterating sclerosis of the extremities;
- Raynaud's syndrome;
- diabetic angiopathy, thromboangiitis and other manifestations of arterial damage;
- Parkinson's disease;
- acrocyanosis, dysbasia, other painful conditions caused by disorders of vascular innervation;
- disturbances of venous circulation and lymph movement in conditions after thrombosis;
- vascular encephalopathy;
- infantile spastic paralysis;
- trophic ulcers of the lower extremities;
- epilepsy.
The medication is approved for use from the age of 1 year.
Indications
Tolperisone is indicated in a fairly large number of neurological diseases:
- hypertonicity in spinal and cerebral palsy;
- spinal automatism;
- muscle spasms of various origins;
- dystonic phenomena with muscle rigidity;
- obliterating diseases of the vessels of the extremities, including Buerger's disease;
- diabetic angiopathy;
- intermittent angioedema dysbasia;
- postencephalitic parkinsonism;
- Little's disease (a form of cerebral palsy).
When is Tolperisone contraindicated?
It is necessary to refuse treatment with the drug during pregnancy and lactation. There is not enough information about the effect of the active substance on fetal formation. The systemic effect that it causes can affect the condition of both mother and child and cause irreversible disorders.
Other contraindications for use:
- myasthenia gravis;
- individual hypersensitivity to the components of the drug;
Signs of a possible allergic reaction to Tolperisone: bronchospasm, skin itching, urticaria, the appearance of red spots - erythema, anaphylactic shock, Quincke's edema.
Results and discussion
Upon admission, patients in both groups had the following levels of the studied criteria (Tables 2, 3).
Table 2. Clinical indicators of the studied criteria at admission
Table 3. Paraclinical and laboratory indicators of the studied criteria upon admission
As can be seen from table. 2 and 3, no significant, statistically significant differences in the studied criteria were found in the groups of patients.
The dynamics of therapy effectiveness criteria in the comparison group are presented in Fig. 1.
Rice. 1. Dynamics of the studied criteria for the effectiveness of treatment in the comparison group.
In the majority of patients in the comparison group ( n
=34) the increase in the amplitude of flexion, extension and rotation of the hip had a statistically significant increase (11±30;
p
<0.05).
The VAS pain index value decreased by more than 20 mm ( p
<0.01). At the same time, the severity of synovitis and laboratory criteria also had positive dynamics, but did not always have statistical confirmation (Table 4).
Table 4. Dynamics of clinical and laboratory criteria for the effectiveness of therapy in the comparison group
Thus, by the end of observation in this group of patients, all studied criteria had positive dynamics compared to the initial values: the amplitude of hip movements and the severity of pain showed statistically significant changes, and changes in the severity synovitis and laboratory parameters were unreliable.
The changes in the studied data in the main observation group looked somewhat different (Fig. 2).
Rice. 2. Dynamics of the studied criteria for the effectiveness of treatment in the main observation group.
In the main group, the same trends were observed as in the comparison group: most significant and reliable ( p
<0.01) the intensity of the pain syndrome on the VAS scale decreased - minus 33 mm, in addition,
the amplitude of all hip movements increased p The severity of synovitis and laboratory criteria also had positive, statistically insignificant dynamics (Table 5).
Table 5. Dynamics of clinical and laboratory criteria for the effectiveness of therapy in the main group
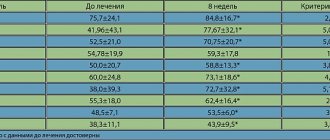
Thus, the differences between the groups consisted primarily in more reliable and pronounced clinical (the amplitude of hip movements increased: 11±30 at p<0.05 in the comparison group and 14± 20 at p
<0.01 in the main group) and subjectively stated paraclinical (pain intensity on the VAS scale decreased by 21 mm in the first group and by 33 mm in the second,
p
<0.01) effects of therapy (Fig. 3, 4).
Rice. 3. Dynamics of the amplitude of hip movements in the control and main groups upon admission and on the 12th day of therapy.
Rice. 4. Dynamics of VAS in the control and main groups upon admission and on the 12th day of therapy.
Side effects of the drug
During treatment with Tolperisone tablets, the following may appear:
- muscle weakness;
- dyspnea;
- increased fatigue;
- dizziness;
- drowsiness during the daytime;
- decreased blood pressure;
- pain in the stomach and abdominal cavity;
- nausea, vomiting.
In the absence of a serious threat to the physical condition, such symptoms do not require discontinuation of the drug.
Use of Tolperisone: instructions
The treatment regimen depends on the characteristics of the painful manifestations. General recommendations:
- 1 tablet with a dosage of 50 mg. 2–3 times a day for adults in the first days of therapy;
- 150 mg each. up to three times a day - if the drug is well tolerated in the subsequent period.
For children under 15 years of age, the dosage is selected taking into account body weight:
- 2–4 mg per 1 kg of weight: children from 1 to 6 years old;
- 5 mg per 1 kg. weight: from 7 to 14 years.
The time of eating does not affect the absorption of the drug.
An overdose of the drug is fraught with respiratory problems, cardiac depression, and vascular collapse. It is important to use it strictly as prescribed by the doctor, after carefully studying the instructions. After taking each dose, monitor changes in physical condition.
Introduction
Osteoarthritis (OA) is a heterogeneous group of diseases of various etiologies with similar biological, morphological, clinical manifestations, which are based on damage to all components of the joint, primarily cartilage, as well as subchondral bone, synovial membrane, ligaments, capsule, periarticular muscles [1] . The disease is an important medical, social and economic problem due to its widespread prevalence (6.43% in the population, correlates with age and reaches maximum values of 13.6% in people over 45 years old), a significant deterioration in the quality of life of patients due to constant pain syndrome, as well as high disability [2].
Despite the high negative significance of this pathology, modern regulatory documents on the provision of specialized care for OA have not been developed. The existing standard of care for patients with coxarthrosis from 2005 is recommended for use in federal specialized medical institutions [3], and the relatively modern standard from 2012 regulates exclusively primary health care provided on an outpatient basis [4]. Both orders include only symptomatic drugs, while etiopathogenetic therapy is not indicated. Therefore, practicing doctors use clinical recommendations and treatment protocols for patients with OA in their work [5]. According to these documents, a generally accepted treatment regimen involves 3 successive stages [6, 7]:
1) non-pharmacological methods: lifestyle changes, excess weight loss, physical exercise, use of orthopedic products, physiotherapeutic and spa treatment;
2) drug therapy: NSAIDs, non-selective COX-2 inhibitors (paracetamol, diclofenac, ibuprofen, ketoprofen, naproxen), moderately selective COX-2 inhibitors (meloxicam, nimesulide, aceclofenac), selective COX-2 inhibitors (celecoxib, etoricoxib), opioid analgesics (tramadol) if NSAIDs are ineffective, intra-articular administration of corticosteroids (methylprednisolone or triamcinolone), chondroprotectors (chondroitin sulfate, glucosamine sulfate, hyaluronic acid derivatives), interleukin 1 inhibitor - diacerein, unsaponifiable compounds of avocado and soy (NSAC) - piaskledin;
3) surgical treatment - endoprosthetics.
The first nonspecific symptoms of OA (pain, limited range of motion) appear even in the absence of radiological changes in the joint and are most likely caused by muscle spasm. However, in most domestic clinical recommendations there is no such class of drugs as centrally acting muscle relaxants, while the Kazakhstan Protocol for the Treatment of OA (2013) contains such drugs [8]. The inclusion of centrally acting muscle relaxants in the complex conservative treatment regimen for OA of large joints, especially in the initial stages of the pathology, seems to be pathogenetically justified and an appropriate addition to the generally accepted treatment regimen.
The purpose of the study was to compare the effectiveness of the generally accepted regimen of conservative drug therapy for hip OA (NSAIDs + chondroprotectors) and a modified regimen (NSAIDs + chondroprotectors + centrally acting muscle relaxant - tolperisone).
special instructions
The therapeutic effect of the drug is enhanced and prolonged when combined with peripheral muscle relaxants, Clonidine, psychoactive and anesthetic agents. Tolperisone reduces the speed of motor skills and mental reactions, affects concentration. During the treatment period, it is necessary to refrain from driving and working with complex mechanisms.
The combination of the drug with alcohol is unacceptable, as it leads to serious intoxication, a sharp decrease in vascular tone, and damage to the central nervous system.