Autism spectrum disorders (ASD) are a group of disintegrative mental development disorders characterized by a lack of ability for social interaction, communication, and stereotypical behavior, leading to social maladaptation. According to modern epidemiological data, the prevalence of ASD is about 1% in the pediatric population [1–3]. The ratio of the incidence of autistic disorders in boys and girls is 4:1 [4].
Today, there is no generally accepted concept of the etiology of ASD in the world, but it is assumed that genetic factors play a large role in the etiology and pathogenesis of this disorder. Thus, L. Kanner back in 1943 [5] declared the hereditary nature of autism based on observations of family members of children with autism who also had autistic traits. S. Sandin et al. [6] showed that having a sibling with ASD increases the risk of developing this disorder by more than 10 times; half-brother or half-sister with autism - more than 3 times; cousin or sister - 2 times.
In accordance with genetic hypotheses, ASD is considered as a result of structural changes in the genome at various levels: nucleotide substitutions in genes, changes in the number of gene copies, changes in the number of chromosomes in individual cells [4]. It is also believed that an important factor that increases the risk of developing autism is the age of the parents. Population analysis by A. Reichenberg et al. [7], showed that the father’s advanced age has a significant impact on the likelihood of developing ASD in children: the risk of having a child with ASD in fathers over 40 years of age is 5.75 times greater than in fathers under 30 years of age. Perinatal pathology also has a significant impact on the development of ASD. Thus, a low value of the newborn’s Apgar score (less than 7 points) may be a predictor of the occurrence of ASD [8]. In addition, an increased risk of developing ASD is associated with preterm birth (before 35 weeks) and fetal hypoxia [9, 10]. According to V.E. Kagan [11], the frequency of detection of organic neurological symptoms in children with autism ranges from 50 to 84%.
Autism is characterized by the presence of a “triad” of disorders: 1) lack of social interaction (detachment, rejection, poor eye contact, lack of adequate reactions to the emotions of other people); 2) lack of mutual communication; 3) stereotypical regressive forms of behavior [4]. The theory of mind [12], which implies the ability to draw conclusions about the mental state of another individual that is the cause of his actions, can be applied to this disorder.
Receptive and expressive speech in ASD develops with a delay [4]. In early childhood there is no gesticulation, humming and babbling. In expressive speech, the first words (in the form of echolalia, repetitions of the last and first syllables of words) appear in the 2-4th year of life. Patients pronounce them melodiously, sometimes clearly, sometimes blurred. The vocabulary is replenished slowly, after 3-5 years short cliche phrases are noted, egocentric speech predominates.
A characteristic symptom of autism is also impaired coordination of movements. Thus, S. Berkeley et al. [13] and S. Cassidy et al. [14] noted frequent manifestations of dyspraxia in this pathology. Ch. Nyokiktjen [15] wrote that many autistic people have difficulty handling objects and tools. C. Gillberg [16] proposed the concept of DAMP (deficit of attention, motor control, perception), connecting pathogenetic links that play a role in the development of a number of disorders, including ASD. Attention deficit in such cases is combined with impaired coordination of movements.
The integrated use of drug and non-drug treatment methods (defectological, psychological, pedagogical, neuropsychological correction, psychotherapeutic, social work with the patient and his family) is one of the fundamental principles of the supervision of autistic disorders in children [4].
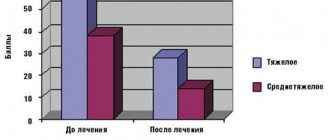
The presence of cognitive impairment in ASD leads to the need to use nootropic drugs. In studies carried out by M.G. Radziwill and V.M. Bashina [17], showed a positive effect of using Cerebrolysin in the correction of behavioral disorders and cognitive dysfunction in children with autism.
The purpose of this study is to evaluate the clinical and neurophysiological changes that occur in children with different types of ASD while taking the drug Cerebrolysin.
pharmachologic effect
Cerebrolysin contains low molecular weight biologically active neuropeptides that penetrate the BBB and directly enter nerve cells.
The drug has an organ-specific multimodal effect on the brain, i.e. provides metabolic regulation, neuroprotection, functional neuromodulation and neurotrophic activity. Metabolic regulation:
The drug Cerebrolysin increases the efficiency of aerobic energy metabolism of the brain, improves intracellular protein synthesis in the developing and aging brain.
Neuroprotection:
the drug protects neurons from the damaging effects of lactic acidosis, prevents the formation of free radicals, increases survival and prevents the death of neurons under conditions of hypoxia and ischemia, and reduces the damaging neurotoxic effect of excitatory amino acids (glutamate).
Neurotrophic activity:
Cerebrolysin is the only nootropic peptidergic drug with proven neurotrophic activity similar to the action of natural neuronal growth factors (NGF), but manifested under conditions of peripheral administration.
Functional neuromodulation:
The drug has a positive effect in cases of cognitive impairment on memory processes.
Dosage
The drug is used parenterally. The dose and duration of use depend on the nature and severity of the disease, as well as the age of the patient. A single administration of the drug in a dose of up to 50 ml is possible, but a course of treatment is more preferable.
The recommended course of treatment is daily injections for 10-20 days.
| Indication | Dose |
| Acute conditions (ischemic stroke, traumatic brain injury, complications of neurosurgical operations) | from 10 ml to 50 ml |
| In the residual period of cerebral stroke and traumatic injury to the brain and spinal cord | from 5 ml to 50 ml |
| Psychoorganic syndrome and depression | from 5 ml to 30 ml |
| Alzheimer's disease, dementia of vascular and combined Alzheimer's-vascular origin | from 5 ml to 30 ml |
| In neuropediatric practice | 0.1-0.2 ml/kg body weight |
To increase the effectiveness of treatment, repeated courses can be carried out as long as the patient's condition improves as a result of treatment. After the first course, the frequency of injections can be reduced to 2 or 3 times a week.
Cerebrolysin is used parenterally in the form of intramuscular injections (up to 5 ml) and intravenous injections (up to 10 ml). The drug in a dose of 10 ml to 50 ml is recommended to be administered only through slow intravenous infusions after dilution with standard solutions for infusion. The duration of infusions ranges from 15 to 60 minutes.
E.A. Morozova
Department of Child Neurology, Kazan State Medical Academy
It is necessary to recognize the sad fact that today the importance of child neurology as a specialty is largely underestimated by global health care. At the same time, we are talking about many millions of children who need the help of a pediatric neurologist in prescribing adequate therapy from the first years, months, and often even minutes of life. Neurological problems of adolescents are no less significant. They are very diverse, and most often have to be considered from the perspective of childhood illnesses. The famous phrase “We all come from childhood” fully applies to the practice of a pediatric neurologist. In the structure of many neurological diseases of children in the first years of life and adolescents, the main share falls on perinatal pathology of the central nervous system, a term that, being very general, does not give an idea of the topic of the neurological problems that have arisen. However, this is a more acceptable diagnosis than the illogical and outdated “cerebral palsy,” which does not reflect either the time of onset of symptoms, the level of damage, or the developed clinical picture in a particular patient. It is known that the perinatal period combines the third trimester of pregnancy, intranatal and early postnatal periods. Symptoms that occur during this time, whether they are caused by intrauterine infection, birth damage to cerebral or spinal structures, or prematurity, one way or another, arise as a result of ischemia and hypoxia of the brain and (or) spinal cord. Therefore, a pediatric neurologist most often deals with pathogenetic therapy, which includes vasodilators and nootropic drugs. This is basic therapy, the timely administration of which helps to normalize blood flow in the affected vascular system, prevent neuroapoptosis and stimulate the sprouting of neurons in the ischemic area. In recent years, the use of drugs that affect the metabolism and plasticity processes of nervous tissue is considered the most promising direction in the treatment of ischemic damage to the central nervous system, post-traumatic changes, demyelinating diseases, etc. Therefore, it is no coincidence that the attention of doctors of various specialties is attracted to nootropic drugs. They entered pediatric practice more than 20 years ago. The name of the nootropics has Greek roots: “noos” - thinking, mind; "tropos" - aspiration. Thus, the World Health Organization has decided to consider nootropic drugs to be drugs that have an activating effect on memory, learning and mental activity, as well as increasing the brain’s resistance to adverse effects. According to their chemical structure, nootropics represent a heterogeneous group of drugs:
1. Pyrrolidone derivatives (piracetam). 2. Derivatives of gamma-aminobutyric acid – GABA (phenibut, pantogam). 3. Neuropeptides and their analogues (Cerebrolysin, Semax). 4. Pyridoxine derivatives (encephabol). 5. Cerebrovascular drugs (vinpocetine). 6. Multicomponent drugs (instenon, actovegin).
Many studies have proven good tolerability of nootropic drugs for neurological pathology in patients of various age groups. One of the most famous nootropics is a drug belonging to the group of neuropeptides – Cerebrolysin. It has a number of unique properties that allow it to be used in a wide range of neurological pathologies. Scientific facts prove the high effectiveness of this drug in neuropediatrics. Having been on the pharmaceutical market for more than 30 years, Cerebrolysin was largely used for neurological pathology in adults, at the same time, many of its properties forced pediatricians, child neurologists and child psychiatrists to turn to assessing the indications and effectiveness of the drug in children. Cerebrolysin (Ebewe Pharma, Austria) is a hydrolyzate of pig brain matter. The active fraction is represented by oligopeptides, the weight of which does not exceed 10 thousand daltons. Low molecular weight biologically active neuropeptides have the ability to penetrate the blood-brain barrier and reach neurons. The effectiveness of Cerebrolysin (CR) in a wide range of neurological pathologies is explained by at least two circumstances: the polyvalent composition of the drug itself, including a set of amino acids and functionally significant peptides; the likelihood of the influence of these components on the links leading to the launch of neuroapoptosis and the ability to prevent the development of negative biochemical reactions at different stages of the pathological process. Direct evidence of the most important mechanism of action of CR, anti-apoptotic, was obtained in 2001. Apoptosis is a biochemical mechanism of “programmed” destruction of certain populations of nerve cells. In a normal cell, the mechanisms of apoptosis are under regulated genetic control, since programmed cell death is a biologically necessary process of tissue transformation. However, under conditions of ischemia, hypoxia, and intoxication, the expression of genes that abnormally trigger neuroapoptosis reactions is induced. It is generally accepted that the cascade of apoptotic processes can be provoked either by a direct effect on the cell genome (viruses), or through mediators (glutamate, interleukins), or by reasons associated with cell ischemia, its damage, or toxic effects. Since apoptosis has reversible stages, pharmacology is considering many options for intervening in its regulation, and, accordingly, modifying neurodegenerative processes. Thus, the therapeutic effectiveness of CR is associated with the correction of destruction processes in damaged brain tissue. The antioxidant effect of CR was demonstrated in rats with hippocampal damage. The drug significantly reduced the activity of enzymes that trigger oxidative stress after just a week of administration. The positive neurotrophic effect on the metabolism and function of the neuron of the amino acids and peptides that constitute the CR was found in experimental studies and consists of more rapid maturation of nerve structures in ontogenesis, their restoration after anoxia and an increase in learning ability. It was found that under the influence of CR in tissue culture, neurons form the same dense network as when neuronal growth factors were added to the culture, which suggested a similar effect of CR. Thus, literature data confirm the multimodal action of Cerebrolysin, associated with its effect on energy metabolism, neuroprotection and neurotrophic functions. Numerous clinical and psychological studies have established an improvement in the neurological status and higher mental functions in patients with vascular pathology of the brain, traumatic brain injury, Huntington's chorea, Friedreich's disease, Alzheimer's disease, Parkinson's syndrome, hyperactive disorders with attention deficit, dyslexia and many others. At the pediatric neurology clinic, we conducted a study of the therapeutic effectiveness of Cerebrolysin (Ebewe Pharma, Austria) in perinatal pathology of the central nervous system, in children with consequences of traumatic brain injury and in hyperactive disorders with attention deficit. Perinatal pathology of the central nervous system combines a variety of symptoms that develop depending on the involvement of cerebral or spinal structures in the process. Most often, these disorders are a consequence of ischemic processes with the development of subsequent hypoxia. They become obvious already in the first hours or days of the child’s life and require the appointment of adequate therapy in the maternity hospital. At the same time, less severe pathology, often being missed in the early stages, attracts the attention of parents and doctors at a later age, when difficulties arise with coordination of movements, formation of speech, perception, and attention. We often observe patients who, already at the age of 3 years, complain of headaches, “become quiet, try to lie down, stop playing.” We conducted a comprehensive examination of 35 children aged 3 to 7 years (20 boys and 15 girls) with the above-described complaints. The examination included a thorough medical history, including complaints and perinatal history, neurological examination, additional research methods (ultrasound of cerebral vessels, REG, craniography, spondylography of the cervical spine, EEG). Criteria for inclusion in the study:
• age from 3 to 7 years; • complicated perinatal history; • neurological symptoms detected in the first year of life; • a similar list of complaints (headaches, delayed speech development; • increased fatigue, awkwardness when performing precise movements); • absence of somatic pathology; • reliable vascular disorders detected during additional research; • absence of epileptic seizures; • parental consent to participate in the study.
The control group included 20 children who met all the criteria of the patients of the first group. In the first group, children received Cerebrolysin 0.1 ml/kg in the morning for 20 days intramuscularly daily and basic therapy: vasodilators, B vitamins, electrophoresis of antispasmodics on the cervical spine using the transverse technique, massage. The dose of Cerebrolysin was increased gradually: in the first two days, 0.5 ml, on days 3-4, 1.0 ml, from the fifth day - 2.0 ml. Children in the control group were prescribed basic therapy and glutamic acid for 20 days. Three months later, a similar course of treatment was repeated for both the study patients and the children in the control group. Treatment results were assessed individually 3 and 6 months after the start of the examination. The criteria for a positive effect were regression of complaints and positive dynamics in neurological status with partial regression of focal symptoms, as well as improvement in cerebral blood flow. In the group of children who received Cerebrolysin, in addition to basic therapy, a positive effect was achieved in 88% of cases, in the remaining 12% it was insignificant. Moreover, parents noted a decrease in the severity and frequency of headaches, a decrease in fatigue, and an improvement in speech after the first course of treatment. Complete disappearance of headaches and significant improvement in other indicators were detected in 65% of patients. This figure seems to us to be very high and indicates the great effectiveness of treatment. It should be noted that the treatment effectiveness rates in the control group were also quite high (considering that the vascular therapy necessary for such a pathology was carried out), but lower than in the first group. A decrease in the main complaints and an improvement in the neurological status was noted in 53% of children. In no case did we observe a deterioration in the patients' condition during treatment. Every practicing neurologist in his daily work is faced with the consequences of traumatic brain injury. This is one of the leading causes of disability among children. According to foreign authors, the number of cases of TBI among children under the age of 14 years is 180 per 100 thousand population. Closed TBI occurs most often in childhood, 80% of which are mild, and 20% are moderate and severe TBI. In each case, mechanical energy affects the developing brain, which is very significant even in mild TBI. It has been proven that the most common long-term consequences of traumatic brain injury, even if we are talking about a concussion, include headaches, which appear in at least 35% of children 3-6 months after the injury. Children complain of increased fatigue and difficulties in school learning. A complex of neurological disorders that occur some time after a concussion is commonly called post-concussion syndrome. Among the pathogenetic mechanisms of its occurrence, of course, disturbances of cerebral blood flow, developing as a regional ischemic process, play a large role. An interesting study was carried out by Berchi-Roche, which proved that with any mechanism of TBI, a concussion occurs in the cervical spine, followed by circulatory disorders in the radiculo-medullary branches of the vertebral arteries. Due to malnutrition of the intervertebral discs, some time after TBI, a degenerative process manifests itself in the area of the discs of the cervical spine. In other words, the whole complex of complaints characteristic of cervical osteochondrosis is formed, and children are no exception. Timely administration of adequate therapy for TBI can prevent the development of serious neurological symptoms. Basic drugs are those that have the functions of activating blood flow and neuroprotection. A number of studies have proven the high effectiveness of Cerebrolysin in treating the consequences of closed TBI in children. We found it interesting to conduct such a study, given the large number of patients with the described problems being treated in the neurological department for older children at the pediatric neurology clinic. We examined 30 children aged 7 to 12 years who had suffered a concussion. All children were hospitalized for the purpose of treating the consequences of a traumatic brain injury, which was more than 6 months old. up to 4 years. These patients made up the first group and underwent treatment with Cerebrolysin. The second group (30 people) was examined as a control group. Criteria for inclusion in the study:
• age from 7 to 12 years; • duration of TBI from 6 months. up to 4 years; • diagnosis of concussion in the acute period of injury; • uncomplicated pre- and perinatal background; • absence of somatic pathology; • absence of epileptic seizures; • parental consent to participate in the study.
In the first group, children received Cerebrolysin daily in the morning at a dose of 2.0 ml intramuscularly for 20 days and basic therapy, including vascular drugs, B vitamins, and dehydration. The dose of Cerebrolysin was increased gradually, reaching the therapeutic dose from the fifth day. Children in the control group were not prescribed Cerebrolysin. They received basic therapy. Upon admission, children underwent a detailed neurological examination with analysis of complaints and neurological status, assessment of the function of attention (using a proofreading test) and memory (using a 10-word memorization test), ultrasound of cerebral vessels, and REG. The main complaints at the time of admission to the hospital were frequent headaches and neck pain, increased fatigue, irritability, impaired attention and memory, and difficulty falling asleep. Already after 2 weeks of treatment, children in both the first and second groups showed regression of their main complaints. By the end of treatment, significant changes could be noted in both groups of patients. Headaches disappeared in children receiving Cerebrolysin in 95% of cases, and in the second group - in 65%. The treatment was equally successful in relation to the phenomena of cerebroasthenia, sleep disorders and neurotic symptoms. These complaints disappeared almost completely in the first group of patients and in more than half of the cases in the second. Cerebrolysin therapy led to a significant reduction in complaints of impaired attention, memory and motor disinhibition, while basic therapy had virtually no effect on such consequences of TBI. In the group of children receiving Cerebrolysin, both the correction test and the memory test scores significantly improved. In the control group, the changes turned out to be significantly small. Cerebrovascular insufficiency, according to ultrasound and REG data, was detected to varying degrees in all patients upon admission. In the group of children receiving Cerebrolysin, by the end of treatment, cerebral blood flow indicators significantly (on average, 50%) improved. In children of the control group, the phenomena of cerebrovascular insufficiency also decreased, but in percentage terms less significant - 20%. Upon admission, children of the first and second groups showed the same type of EEG changes in the form of alpha rhythm irregularity, diffuse increase in slow-wave activity, a large number of bilaterally synchronous bursts of oscillation groups, and local paroxysmal activity. The results of the EEG assessment before and after treatment revealed that the positive dynamics of the EEG pattern was greater in the group of children receiving Cerebrolysin. It manifested itself in the normalization of the alpha rhythm and a decrease in the level of paroxysmalness. Thus, the results of our study confirmed the positive effect of Cerebrolysin on the course of recovery processes in the consequences of traumatic brain injury in children. It took decades for doctors of many specialties to be united by the big problem of cognitive disintegration and hyperactivity in children and adults. For many years, patients with similar disorders turned to neurologists, psychiatrists and psychologists, but mostly to no avail. One of the most common diagnoses in such cases was minimal brain dysfunction (MCD), which did not explain either the etiology or pathogenesis of the disease. In MMD, it is believed that there is a delay in the rate of development of certain brain systems that control speech, attention, memory, perception and many other functions. MMD also includes motor disorders - dyspraxia (according to ICD-10). At the same time, a violation of praxis and difficulty in producing movement, from the point of view of classical neurology, is a consequence of damage to various cortical centers. It is difficult to explain from the perspective of classical neurology such manifestations of “immaturity” in children as dysgraphia, dyslexia and dyscalculia. In other words, from our point of view, under the general name MMD hides a diverse focal, often perinatal, pathology of the nervous system. The increase in the number of patients with changes in cognitive function and inhibition processes in recent years has required the joint efforts of doctors and charities. A syndromic name for the disease has emerged - attention deficit hyperactivity disorder (ADHD). Such a diagnosis symbolizes the lack of clear ideas about its origin and pathogenesis today, although genetic, biochemical, and MRI studies have been carried out in the last decade. The main question remains: is this a disease or a syndrome that has an underlying cause? No less important is whose problem is this – neurologists or psychiatrists? There is no doubt that ADHD is a real disorder. According to foreign epidemiological studies, the frequency of ADHD among children of preschool and school age is growing and today ranges from 4.0 to 9.5%, with a predominance among boys. Patients with ADHD can be divided into groups with confirmed hereditary and acquired forms. In most cases, significant neurochemical and morphological (according to neuroimaging) changes in the brain have been proven. In the pediatric neurology clinic, we are faced with numerous problems of cognitive impairment that change both the quality of life of patients and the possibilities of their social adaptation. Some cognitive disorders develop simultaneously with hyperactivity and attention deficit. These patients seemed interesting to us for a long time, since only the complex of complaints that united them was uniform, and the background against which the complaints arose and developed was different. We examined 50 patients with ADHD aged 7 to 14 years. The diagnosis was based on ICD-10 and the American Psychiatric Association classification, which is recommended by WHO (1994). Exclusion criteria from the study included children with somatic pathology, mental illness, and patients with intellectual disabilities. The control group included 25 children using the same selection criteria. Patients in both groups had normal intelligence. Parents made similar complaints about learning difficulties due to distractibility, inability to concentrate for more than 10-15 minutes, decreased memory, perception, and hyperactivity. In 75% (!) of children in both groups, the perinatal background was burdened: an unfavorable course of pregnancy, complications during childbirth and neurological symptoms during the first year of life, which served as a reason for treatment and observation by a neurologist. Symptoms of obsessive movement neurosis were identified in 23% of patients, mainly in the form of tic hyperkinesis. 12% of the parents of the subjects were under 2 years of age. 35% of children in both groups consulted neurologists due to frequent headaches of moderate intensity. The neurological status revealed mild coordination disorders, peripheral cervical insufficiency syndrome, and pyramidal insufficiency. All children underwent a correction test and a test of directed attention. To assess the effectiveness of treatment, all patients with ADHD were examined before treatment and 2 weeks after its completion. Children in the first group were prescribed Cerebrolysin daily intramuscularly, once a day in the morning. The dose of the drug was gradually increased over 5-6 days from 0.5 ml to 2.0-3.0 ml. Patients of the second group were prescribed B vitamins, glutamic acid, and elcarnitine. Treatment was carried out for 3 weeks. During the repeated (after treatment) study, positive dynamics were assessed by questioning parents, assessing the neurological status and performing tests for concentration. It turned out that in the group of children receiving Cerebrolysin, significant improvement was detected in 65% of cases, while in the control group - in 18%. Parents noted a longer concentration of attention, when by the end of treatment the child was able to work throughout the entire lesson (40 minutes), was significantly less distracted, memory became better, behavior characteristics became “more manageable,” and he received fewer criticisms at school. A neurological examination revealed improvements in motor skills and coordination, as well as tests for concentration and performing complex tasks. Adverse reactions were noted in 3% of cases in the form of difficulty falling asleep and were associated with a violation of the drug administration regimen (in the afternoon). Thus, our study confirms the positive effect of Cerebrolysin in the treatment of such a complex and multifaceted pathology as ADHD. In general, we can say that both doctors and pharmacologists have long ceased to experience unreasonable euphoria over the extraordinary newly discovered effects of certain drugs - it is known that in medicine, unfortunately, there is no panacea for any disease. The history of medicine knows many cases of grave disappointments and many consequences of insufficiently scientifically confirmed enthusiasm for medicinal substances. But in cases of a convincing positive effect of a drug obtained through repeated studies, we can talk about a small victory, another step towards a cure. Cerebrolysin is one of these drugs today.
Recommended reading 1. Collection of reports of the IV international symposium “Cerebrolysin: pharmacological effects and place in clinical practice.” M.: 2002. 2. Diagnosis and treatment of cognitive and behavioral disorders in children. The use of Cerebrolysin in their complex correction. Methodological manual for doctors. N.N. Zavadenko et al. M.: RGMU. 2005; 89. 3. Attention deficit hyperactivity disorder (ADHD): etiology, pathogenesis, clinical picture, course, prognosis, therapy, organization of care. Expert report. Russia. 2007. 4. Your naughty child (translation from English). St. Petersburg: Peter, 2004-218.
Side effects
The frequency of adverse reactions was determined in accordance with WHO recommendations: very often: (≥1/10); often: (from ≥1/100 to <1/10); uncommon (from ≥1/1000 to <1/100); rare (from ≥1/10,000 to <1/1000); very rare, including isolated reports (<1/10,000).
From the immune system:
very rarely - increased individual sensitivity, allergic reactions.
Mental disorders:
rarely - the expected activation effect is accompanied by agitation, manifested by aggressive behavior, confusion, and insomnia.
From the nervous system:
rarely - too rapid administration of the drug can lead to dizziness; very rarely - isolated cases of generalized epilepsy and one case of seizures were associated with Cerebrolysin.
From the cardiovascular system:
very rarely - too rapid administration of the drug can lead to increased heart rate and arrhythmia.
From the digestive system:
very rarely - dyspepsia, diarrhea, constipation, nausea, vomiting; rarely - loss of appetite.
For the skin and subcutaneous tissues:
very rarely - skin reactions; rarely - with excessively rapid administration, a feeling of heat, sweating, and itching may occur.
General disorders and disorders at the injection site:
very rarely - redness, itching, burning at the injection site, pain in the neck, head and limbs, fever, mild back pain, shortness of breath, chills, collapsing state.
One study reported an association between rare use (>1/10,000 to <1/1,000) with hyperventilation, hypertension, hypotension, fatigue, tremor, possible depression, apathy and/or somnolence, and flu-like symptoms. (cold, cough, respiratory tract infections).
Since Cerebrolysin is used mainly in elderly patients, the above symptoms of diseases are typical for this age group and often also occur without taking the drug.
It should be noted that some undesirable effects (excitement, arterial hypertension, arterial hypotension, lethargy, tremor, depression, apathy, dizziness, headache, shortness of breath, diarrhea, nausea) were identified during clinical studies and occurred equally in patients treated with Cerebrolysin and in patients in the placebo group.
If any of the side effects indicated in the instructions are aggravated or any other side effects not specified in the instructions are noted, the patient should inform the attending physician.
Notification in case of suspected side effects
It is important to report side effects after drug approval to ensure ongoing monitoring of the drug's risk-benefit profile. Healthcare professionals are asked to report all cases of adverse reactions observed with the drug through national adverse reaction reporting systems and/or to the company's representative office.
Reviews
On the forums you can find a variety of opinions about the drug. Most of the positive reviews are related to the therapy of children and the solution of problems with developmental delays, speech, the consequences of birth injuries and pathologies of the central nervous system. The greatest progress in treatment was observed when procedures began for children before the first year of life.
Adult patients respond less cordially to the medication after the first therapeutic course. The question is related to inattention: the manufacturer initially indicated in the instructions that the best results occur after several repeated approaches.
Drug interactions
Taking into account the pharmacological profile of the drug Cerebrolysin, special attention should be paid to possible additive effects when co-administered with antidepressants or MAO inhibitors. In such cases, it is recommended to reduce the dose of the antidepressant. The use of Cerebrolysin in high doses (30-40 ml) in combination with MAO inhibitors in high doses can cause an increase in blood pressure.
Cerebrolysin and balanced solutions of amino acids should not be mixed in the same solution for infusion.
Cerebrolysin is incompatible with solutions containing lipids and with solutions that change the pH of the medium (5.0-8.0).
special instructions
If injections are performed too quickly, a feeling of heat, sweating, and dizziness may occur. Therefore, the drug should be administered slowly.
The compatibility of the drug has been tested and confirmed (within 24 hours at room temperature and light) with the following standard solutions for infusion: 0.9% sodium chloride solution, Ringer's solution, 5% dextrose (glucose) solution.
The simultaneous use of Cerebrolysin with vitamins and drugs that improve cardiac circulation is allowed, but these drugs should not be mixed in the same syringe with Cerebrolysin.
Only clear Cerebrolysin solution should be used and only once.
Impact on the ability to drive vehicles and operate machinery
Clinical studies have shown that Cerebrolysin does not affect the ability to drive vehicles and use machinery.
Analogs
If unusual reactions to the medication occur, a substitute is used. The list of analogues in ampoules is presented:
- Amylonosar, Bravinton, Vinpocetine;
- Cavinton, Cortexin, Piracetam;
- Lucetam, Nootropil, Piracetam Bufus;
- Piracetam-Vial, Picamilon, Cerakson;
- Cerebrolysate, Escotropil, Vinpotropil;
- Cellex, Thiocetam.
Cheap substitutes for Cerebrolysin include Nootropil, Glycine, Isten, etc.
Release form, composition and packaging
Injection
yellowish-brown, transparent.
| 1 ml | |
| Cerebrolysin concentrate (a complex of peptides* obtained from pig brain) | 215.2 mg |
* molecular weight not more than 10,000 daltons.
Excipients:
sodium hydroxide, water d/i.
- 1 ml - brown glass ampoules (10) - contour cell packaging (1) - cardboard packs.
- 2 ml - brown glass ampoules (10) - contour cell packaging (1) - cardboard packs.
- 5 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 10 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 20 ml - brown glass ampoules (5) - contour cell packaging (1) - cardboard packs.
- 30 ml - brown glass bottles (1) - cardboard packs.
- 30 ml - brown glass bottles (5) - cardboard packs.