Pulmonologist
Prokhina
Maria Egorovna
Experience 39 years
Pulmonologist
Make an appointment
Pulmonary sarcoidosis (benign granulomatosis) is a disease that affects various tissues of the body. But most often it manifests itself in the respiratory organs. With this disease, granulomas form in the lungs, as well as in the trachea, bronchi and lymph nodes.
The danger of sarcoidosis is that granulomas gradually grow, merge, then resolve and leave behind scar tissue. This greatly affects the functioning of organs - in particular the lungs - which cannot fully perform their functions. With superficial ventilation, the respiratory function is disrupted - and this, as is known, entails a load on all internal organs, because the blood cannot supply oxygen to different systems of the body.
The disease is not contagious (unlike tuberculosis) and does not pose any danger to others.
What is sarcoidosis?
Sarcoidosis (ICD-10 code: D86)
- one of the autoimmune (the immune system attacks its own tissues) interstitial lung diseases of unknown origin and unknown pathogen.
A characteristic feature of sarcoidosis is the formation of small inflammatory nodules, lymph nodes, otherwise known as granulomas, in various organs. These are structures consisting of accumulating abnormally stimulated cells of the immune system - macrophages and lymphocytes. Most often it affects young people aged 20 to 40 years, regardless of gender.
Pulmonary sarcoidosis
Pathogenesis
With pulmonary sarcoidosis, first of all, changes such as lymphocytic alveolitis appear. It is thought to be triggered by alveolar macrophages and T-helper cells, which release cytokines. In some cases, oligoclonal local expansion of T lymphocytes occurs. For the subsequent development of granuloma, alveolitis is required.
Sarcoidosis is considered a granulomatosis that is mediated by an intense cellular immune response at the site of disease activity. Granulomas can form in different organs:
- leather
- lungs
- liver
- lymph nodes
- spleen
Causes of the disease
The causes of sarcoidosis remain to be elucidated. Scientists suspect that the immune system's reaction to an unidentified antigen is responsible for the development of the disease. It is a molecule in the body that is detected by certain cells of the immune system. An antigen can also stimulate the production of antibodies against itself. Genetic predisposition and a family history of the disease are also important in the development of sarcoidosis. The risk of developing sarcoidosis in relatives of the patient is four times higher.
Infection is a potential cause of sarcoidosis. It is also suspected that mycobacteria, which cause tuberculosis, and various types of viruses are involved in the development of the disease. Other possible causes: prolonged contact with organic dust, solvents, mold, pesticides, or working with metal and stone.
Symptoms of sarcoidosis
Pulmonary sarcoidosis can have different symptoms for everyone. Most develop systemic symptoms such as easy fatigue, night sweats, decreased exercise intolerance, and weakness. There is also a decrease in appetite, weight loss and a high temperature (usually a slight increase, although it can reach 40 degrees Celsius). Other symptoms of sarcoidosis are related to the involvement of certain organs in the disease process.
Pulmonary sarcoidosis symptoms
What is the prevention of sarcoidosis?
Prevention of sarcoidosis has not been developed, since its cause is not clear. But Immunostimulants, including those of plant origin, inducers of endogenous interferon, sets of antigens of various bacteria are potentially dangerous as triggers of sarcoidosis.
Diet – avoid large amounts of calcium and vitamin D. Do not use multivitamin complexes containing calcium.
Mode – physical training and limiting exposure to ultraviolet radiation are recommended.
The main thing I would like to advise you to do is to learn to cope with stress, enjoy life, communicate with friends and family in order not to get sarcoidosis. In many countries, for example, in Germany, after a diagnosis of sarcoidosis is made, the patient is first of all referred to a psychologist.
What organs are affected by sarcoidosis?
It can affect most organs of the body. Most often (in more than 90% of patients), sarcoidosis affects the lungs and lymph nodes located in the cavities of the lungs. This manifests itself in the form of shortness of breath, low saturation, cough and chest pain when moving or at rest. Sarcoidosis causes pain in the joints - most often in the knees, ankles and elbows. It can cause enlargement and pain in the spleen and liver, as well as swollen lymph nodes at the back of the head.
Cutaneous sarcoidosis is a fairly common manifestation of this disease. Its characteristic features are the appearance of erythema nodosum - large, painful, red inflammatory infiltrates, most often on the anterior surface of the leg. Others: papular changes, small subcutaneous nodules, ulcers, discoloration and alopecia. The disease also affects the heart and can cause fluid to form in the pericardial sac, causing rhythm and conduction problems.
The eyes are another organ that can be affected by sarcoidosis. Anterior uveitis appears, causing redness and pain. There are problems with vision, a feeling of “sand under the eyelids,” that is, dry eyes. The parotid glands, large glands that produce saliva, are also affected, causing them to become swollen and painful. Less commonly, sarcoidosis causes inflammation of the nerves, leading to paralysis and dysfunction. This is manifested by pain, decreased sensitivity and muscle strength. In some patients, sarcoidosis has an acute onset. Fever, joint pain, erythema nodosum and bilateral lymphadenopathy of the lung cavities occur. This set of symptoms is called Löfgren's syndrome.
Skin lesions in sarcoidosis can be specific or nonspecific (erythema nodosum), and the course of the disease can be acute or chronic. In approximately 40% of cases when visiting a dermatologist, there is no damage to internal organs.
Erythema nodosum
Erythema nodosum is the most common nonspecific manifestation of acute or subacute sarcoidosis. It is a hypersensitivity reaction to unknown substances and exhibits the same symptoms as erythema nodosum in the presence of bacterial, fungal and other infectious or chemically induced antigens. It may be accompanied by fever and arthralgia.
Löfgren's syndrome
Erythema nodosum in combination with bilateral hilar lymphadenopathy and arthralgia is known as Lofgren's syndrome, which usually regresses spontaneously. Occurs mainly in young women,
Maculopapular sarcoidosis
| Patchy sarcoidosis | Hypopigmental sarcoidosis | Small nodular sarcoidosis |
| Large nodular sarcoidosis | Ring sarcoidosis | Lichenoid sarcoidosis |
| Livedo sarcoidosis |
- Patchy sarcoidosis
is a rare variant characterized by a rash of erythematous spots, located either isolated or merging with each other. - Hypopigmented sarcoidosis
appears as well-demarcated, round or oval patches, mainly on the extremities. In the center of some lesions, erythematous papules can be observed, giving them the appearance of a “fried egg”. - Fine nodular sarcoidosis
is characterized by a rash of papules ranging in size from a pinhead to a pea, hemispherical or flattened, slightly elevated above the skin level, with a smooth surface, the color of which gradually changes from pale pink with a yellowish tint to violet, brown or brownish-red. With subsequent regression, the papules become flattened, sink in the center, and become covered with telangiectasias and thin pityriasis scales. After their regression, temporary pigmented or superficial white scars remain. Diascopy reveals tiny brownish-yellow specks or a solid brownish color. The number varies from a few pieces to thousands. The rashes recur and can occasionally ulcerate. - Large nodular sarcoidosis
(focal) is characterized by papules or nodules, flat or hemispherical, 0.5-3 cm in diameter, clearly demarcated from the surrounding healthy skin. Their consistency is dense or soft, the color ranges from bluish-pink to reddish-brown and violet-brown, the surface is smooth. Frequent localization is the face, neck, upper limbs. Their number varies from one to several dozen. When diascopy of the nodes, small yellow-brown spots (specks of dust) are revealed, reminiscent of the picture of apple jelly in tuberculous lupus, but less transparent. The nodes regress from the center, where multiple telangiectasias are formed. Rarely, partial ulceration of the nodes is observed. Temporary pigmentation remains at the site of the nodes, less often superficial cicatricial atrophy - Ring-shaped sarcoidosis
is a clinical variant of small-nodular sarcoidosis with a ring-shaped arrangement. It is characterized by densely elastic pink-red papules with a diameter of up to 5 mm, forming rings consisting of a peripheral ridge of small nodules and a rash-free center, which can become depigmented or scarred. With diascopy, the elements turn pale , instead of red, an uneven yellowish tint appears. Annular lesions of cutaneous sarcoidosis often occur on the forehead, face, and neck. Ulceration is rare. The lesions may resemble granuloma annulare but differ histologically. The diffuse papular form can also acquire an annular form. There are no subjective sensations - Lichenoid sarcoidosis
is more common in children and accounts for 1-2% of cases of cutaneous sarcoidosis. Characterized by multiple flat papules 1-3 mm in diameter, red or flesh-colored, localized in the trunk, limbs and face. Resembles lichen planus, but Wickham's grid is absent - Livedo (reticuloform sarcoidosis)
is a rare variant of the disease, most identified cases are registered in Japanese women. It is often combined with damage to the eyes and central nervous system.
Nodular plaque sarcoidosis
| Nodular sarcoidosis | Plaque sarcoidosis | Broca's angiolupoid sarcoidosis - Pautrier |
| Erythrodermic sarcoidosis |
- Nodular sarcoidosis
manifests itself as one or several sharply limited hemispherical nodes, medium in size, the size of a walnut, dense consistency, brownish or brownish-bluish in color. Diascopy reveals yellowish-brown spots. The elements are most often localized on the face and lower extremities. After existing for months or years, the nodes gradually resolve completely, often leaving scar atrophy. - Plaque (diffuse-infiltrative) sarcoidosis
is characterized by a rash of vaguely demarcated violet-pink or bluish-brown smooth infiltrated plaques with a diameter of 5-6 cm, of dense consistency, slightly protruding above the skin level. The elements are most often localized on the face, in the area of the cheeks and nose, on the upper extremities, including on the back of the fingers. Diascopy reveals a yellowish-brown color. - Broca's angiolupoid - Pautrier
has recently been considered as a telangiectatic variant of Beck's sarcoid. The frequency is 8% of all forms of cutaneous sarcoidosis, more often observed in women. The skin lesion is represented by a single, soft, slightly raised, limited, round or oval plaque with a diameter of 2-3 cm with a smooth surface, bluish-red with a yellowish tint or reddish-brown with pronounced liquid tint. This shade depends on the presence of telangiectasia on the surface of the node, which changes the normal grayish-yellow color revealed by diascopy. Frequent localization is the lateral surface of the nose, closer to the corner of the eye, the inner edge of the eyebrow or on adjacent areas of the cheeks. There are no subjective sensations. The tendency of the angiolupoid to resolve is extremely small. - Erythrodermic sarcoidosis
- characterized by the fusion of infiltrated erythematous plaques into large lesions. In some cases, significant desquamation is observed.
Besnier-Tennesson's lupus pernio (Lupus pernio)
| It is characterized by the appearance in the area of the nose, cheeks, ears, chin, forehead and back of the hands of infiltrative foci of a soft consistency, lilac-reddish, sometimes violet-reddish in color with fairly clear boundaries. The surface is smooth, shiny, with dilated sebaceous follicles and a noticeable vascular pattern. There is no peeling, no atrophy or scarring is observed. Diascopy reveals small yellowish spots. In place of the resolved process, atrophy usually remains. The disease may worsen during the cold season. This form is more common in women with a frequency of 5-8% of all cases of cutaneous sarcoidosis. In most cases, patients have lesions of the lungs, bones, joints, and enlarged lymph nodes. In this regard, it is necessary to carefully examine the lungs (hilar adenopathy and parenchymal changes in 90% of patients with systemic sarcoidosis), the musculoskeletal system (Jungling's osteitis), and the eyes (uveitis of the anterior and/or posterior segment of the eye). Youngling's cystoid osteitis occurs in 10-15% of patients in the form of round or oval-shaped foci of rarefaction of bone tissue in the phalanges of the fingers and toes, less often in the bones of the skull, vertebrae, and long tubular bones. The fingers may acquire a spindle-shaped shape, and ulcers with flaccid granulations and bloody-purulent discharge appear on the skin. Lesions on the face when they spread to the sinuses of the nose cause their destruction. |
Subcutaneous sarcoidosis Daria–Roussi
| Subcutaneous sarcoidosis | Sarcoid dactylitis |
It is characterized by the formation of subcutaneous nodes with a diameter of up to 3 cm or more, located in the subcutaneous fatty tissue, usually few and painless. When merging, large plaque infiltrates with a bumpy, uneven surface are formed. The skin in the lesions is dull pink or flesh-colored, sometimes in the form of an “orange peel.” The nodes are localized mainly on the lateral surfaces of the torso, abdomen and thighs. Increasing in size, they become welded together with the skin, but almost never ulcerate, in contrast to the nodes of indurative tuberculosis of the skin. Occurs in 1.4-6% of patients with systemic sarcoidosis and in 12% with cutaneous sarcoidosis.
Sarkidous dactylitis
characterized by the appearance of painless subcutaneous nodes in the area of the fingers, often the hands, resembling swelling.
Scar sarcoidosis
| Scar sarcoidosis | Sarcoidosis on a tattoo |
It is characterized by a rash of reddish translucent nodules that appear in scars after surgery, trauma, venipuncture and some diseases (acne, herpes zoster). It accounts for 9% of all forms of cutaneous sarcoidosis. Frequent localization is the knees and elbows.
Sarcoidosis on a tattoo
- a variant of the scar form that occurs after tattooing. It must be distinguished from a reaction to a foreign body (applied pigment)
Ulcerative sarcoidosis
| Typically occurs in papulo-nodular or atrophic lesions, often on the legs. Frequency is 1.1–4.8% of cases with cutaneous sarcoidosis, more often in black women and Japanese. Healing occurs with the formation of rough scars. |
Warty (verrucous) sarcoidosis
| It is characterized by clearly defined plaques or nodules with verrucous growths and layering of thick crusts on the surface, localized mainly on the lower extremities. |
Psoriasiform sarcoidosis
| It is registered with a frequency of 0.9% of all forms of cutaneous sarcoidosis. It is characterized by clearly defined flat erythematous plaques with a scaly surface localized mainly in the area of the knees and elbows. |
Ichthyosiform sarcoidosis
| It appears as sticky, tightly adjacent to the skin, polygonal scales measuring 0.1 - 1 cm, grayish or brown in color in the area of the lower extremities, forming merging lesions. More often found in people of the Negroid race. |
Morphea-like sarcoidosis
| Morphea-like sarcoidosis | Linear morphea-like sarcoidosis |
Morphea-like (scleroderma-like) sarcoidosis appears as round atrophic plaques or linear lesions resembling scleroderma lesions.
Sarcoidosis of the scalp
| Sarcoidosis of the scalp | Scarring alopecia in sarcoidosis |
Sarcoidosis sometimes affects the scalp. Initially, changes appear in the form of small nodules or papules, after the fusion of which plaques are formed. In place of the resolved elements, scar atrophy remains, which has no specific differences from similar alopecia of other etiologies. The diagnosis of sarcoidosis of the scalp may be suspected in the presence of skin or systemic changes specific to sarcoidosis.
Sarcoidosis of the eye
| Ocular sarcoidosis is observed in 25% of patients; lesions can be observed in any part of the eye. Most often, granulomatous uveitis is detected, which can be acute or chronic. Acute uveitis often occurs in young people in the form of bilateral iritis and iridocyclitis. Chronic uveitis is more common in women and can sometimes cause glaucoma, cataracts and blindness. It is also possible to develop retinochoroiditis, dry conjunctivitis, and calcium deposition. Typical papules in the eyelid area and conjunctiva are characteristic. The combination of iridocyclitis, hyperfunction of the parathyroid glands and facial paralysis is known as Heerfordt syndrome. |
Sarkidosis of the mucous membranes
| Sarcoidosis of the mucous membranes can be isolated, but more often it is combined with sarcoidosis of the skin. The mucous membranes of the upper respiratory tract are most often affected in lupus pernio. The mucous membranes of the nasopharynx, larynx and nasal bones are involved in the process. The first signs of nasal damage are difficulty in nasal breathing and purulent rhinitis; then perforation of the nasal septum, nasal deformation, narrowing of the nasal passages and obstruction of the upper respiratory tract develop. On the oral mucosa, lesions in the form of nodules are most often localized on the gums, tonsils, soft and hard palate, and cheeks. |
Sarcoidosis of the nails
| A rare form, characterized by pronounced subungual hyperkeratosis and onychodystrophy. |
Systemic manifestations
- Pulmonary sarcoidosis is observed in 50% of patients with sarcoidosis. Most often in these cases, there is an enlargement of the mediastinal lymph nodes, which can be isolated (stage I) or combined with multiple foci of sarcoidosis of the pulmonary tissue (stage II). In the third, late stage, large confluent foci of sarcoidosis and pronounced fibrosis of the lung tissue develop in the lungs. In 70% of patients, mediastinal lymphadenopathy is asymptomatic.
- Musculoskeletal system: In 25-30% of cases, joints are affected, in 70% of patients, arthralgia is the first symptom of the disease, they often appear before the onset of erythema nodosum, with chronic disease, the joints are swollen, sensitive and painful. Multiple cysts on the distal phalanges, identified by radiography, are called osteitis cystica.
- In 30% of patients with sarcoidosis, peripheral lymph nodes are enlarged, in 5-40% of cases - hepatosplenomegaly.
- Sarcoidosis can affect any part of the heart, most often the myocardium (granulomatous myocarditis). Heart damage is detected intravitally in only 5% of patients with sarcoidosis, and at autopsy - in 27%.
- Sarcoidosis can occur in any part of the central nervous system; if in these cases mumps develops, then they speak of Mikulicz syndrome.
- Hypercalcemia and hypercalciuria can be observed at any stage of sarcoidosis. The frequency of hypercalcemia varies widely (from 2% to 40%). Persistent hypercalcemia is clinically manifested by polyuria, nocturia or polydipsia in the absence of hypertension. Nephrocalcinosis and renal failure may develop. Hypercalcemia is a feature of systemic sarcoidosis.
Sarcoidosis in children
Sarcoidosis often occurs in children of all ages. Maculopapular skin rashes, uveitis, hilar lymphadenopathy and arthritis are characteristic signs of sarcoidosis in children. Joint changes and lung damage can be severe, persistent and recurrent.
Sarcoid reactions
Sarcoid reactions are the formation of sarcoid-type epithelioid cell granulomas in various organs and tissues, which can be diffuse or localized.
Diffuse sarcoid reactions
may occur with certain chronic infections or when various chemicals enter the body. Sarcoid reactions in these cases have the following features: they appear in those organs that are normally affected by sarcoidosis, or in places of absorption or accumulation of relevant chemicals. The clinical picture of such reactions has a strong resemblance to systemic sarcoidosis. Diffuse reactions most often occur with tuberculosis, leprosy, syphilis, brucellosis, some mycoses and viral diseases. Crohn's disease may have a clinical picture similar to sarcoidosis. Diffuse sarcoid reactions may be caused by beryllium or silicon dioxide (“quartz dust”). Berylliosis is, as a rule, an occupational disease of people involved in the production of neon lamps and ceramic products. The cause of the disease is inhalation of dust containing beryllium or its entry into damaged skin. Sarcoid granulomas in berylliosis most often appear in the lungs and skin. Silicosis (an occupational disease of miners, foundries, potters, etc.), whose work involves prolonged inhalation of small particles of crystalline silicon dioxide, may have a clinical-morphological picture similar to sarcoidosis.
Localized sarcoid reactions
represent the formation in tissues of limited groups of epithelioid cell granulomas in response to foreign bodies of various origins, as well as to infiltrative processes, mainly malignant tumors. A large number of foreign substances and substances that enter the skin can cause the development of granulomas, which have histological similarities to sarcoidosis.
- Silicon contained in dirt, sand, gravel and glass, including car windows, can get into areas of skin injury. In these places, papules appear, and histological examination of them reveals sarcoid granulomas in the dermis. . In silicon granulomas, giant Pirogov-Langhans cells and a foreign body are detected, in which there are clear colorless granules. To identify them, it is necessary to use polarized light. The detection of these silicon particles, however, does not rule out sarcoidosis.
- Granulomatous inflammation of the skin can occur in response to pigment introduced into the skin during a tattoo. The lesions are usually limited to the tattoo sites. There are two morphological types of tattoo pigment granulomas: the foreign body type and the sarcoid type. The latter type consists of clusters of epithelioid histiocytes and giant cells surrounded by a slight round cell infiltrate. Histiocytes and giant cells contain pigment. True systemic sarcoidosis with damage to the mediastinal lymph nodes can occur in the tattoo area. It is possible that these cases are a systemic sarcoid reaction to tattooing rather than capcoidosis. If cutaneous sarcoid reactions to a tattoo are detected, the patient should be evaluated for systemic sarcoidosis. Other granulomas that can complicate tattooing are tuberculosis and leprosy.
- Zirconium, contained in deodorants and other cosmetics and dermatological preparations, can cause sarcoid reactions in sensitized people. Histologically, the skin lesions are identical to sarcoidosis. To verify the diagnosis, it is advisable to examine the preparations in polarized light.
- Sodium bisulfate eye drops cause pigmented papules around the eyes, histologically represented by sarcoid granulomas, the giant cells of which contain pigment.
- Sarcoid granulomas can occur at sites where interferons beta-1b and alpha-2 are injected.
- Sarcoid granulomas on beryllium, zinc, acrylic and nylon threads, sea urchin needles, cactus, and ears of cereal plants are often observed.
- Foreign body granulomas may occur at sites of ruptured cysts or hair follicles (keratin reaction)
- Sarcoid skin reactions can develop with long-term treatment of dermatoses on the face with corticosteroid ointments, acne vulgaris and microtraumas.
- Sarcoid reactions sometimes occur in the lungs and skin of people who use polyvinyl pyrrolidine hair sprays (thesaurosis).
- The morphological picture of sarcoidosis can occur in some skin diseases of unknown origin (granulomatous cheilitis, miliary disseminated lupus of the face, etc.).
Course of sarcoidosis
The course of sarcoidosis depends on the degree of systemic damage. The most severe manifestations are pulmonary fibrosis and eye damage. However, abnormalities expressed to varying degrees can be found in all affected organs, as well as in the nervous and musculoskeletal systems.
Symptoms common to oncology
Sarcoidosis, due to its often nonspecific and alarming symptoms, can lead to suspicion of cancer.
Both cancer and sarcoidosis contribute to the occurrence of night sweats. The same goes for other symptoms such as weight loss, fatigue, cough and chest pain. Imaging tests, such as an X-ray of the lungs, may also show changes that are similar to both conditions—enlarged lymph nodes in the lung and mediastinum, as well as consolidation in the lung. All this can worry a patient who often starts looking for information on the Internet (for example, on a medical forum) - is sarcoidosis cancer? It should be frankly recognized that these are two significantly different diseases.
Sarcoidosis results from a disorder of the immune system of unknown origin and is an interstitial lung disease. On the other hand, lung cancer has a genetic basis (genetic mutation), and uncontrolled division of cancer cells occurs. Therefore, it should be emphasized once again that sarcoidosis is not a cancer, but a disease that belongs to a spectrum of disorders of the immune system response.
Classification
There is currently no universal classification of sarcoidosis. The division of intrathoracic sarcoidosis was developed quite a long time ago, in 1994. The following stages are identified:
- bilateral mediastinal lymphadenopathy and parenchymal infiltration in the form of infiltration
- bilateral mediastinal lymphadenopathy
- widespread interstitial fibrosis and bullous transformation
- parenchymal infiltration in the form of dissemination
The Central Research Institute of Tuberculosis of the Russian Academy of Medical Sciences, together with Hungarian specialists, divided sarcoidosis as follows:
- C. intrathoracic lymph nodes
- S.v.l.u. and lungs
- C. respiratory organs, combined with lesions of other organs
- S. lungs
- generalized S. with damage to the respiratory system
Diagnosis of the disease
The disease is diagnosed based on symptoms and additional tests. Due to its often nonspecific symptoms, sarcoidosis can go undetected for a long time.
A cough and fever may indicate a bacterial or viral infection, such as that caused by coronavirus. Blood tests often show anemia and high levels of calcium in the blood.
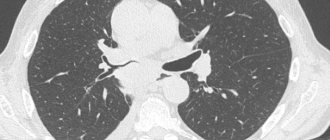
The main tests that are very helpful in diagnosis are X-rays and computed tomography (CT) scans of the chest. They allow visualization of changes in the lung parenchyma, lung tumors, enlarged lymph nodes and compactions in the organ cavities. Other tests used are lymph node and lung biopsies. Pathological analysis of samples of the bronchial mucosa also helps in making a diagnosis. Sometimes a bronchoscopy is performed and fluid is collected from the bronchi. An ophthalmological examination is recommended for every patient.
Sarcoidosis - treatment
Glucocorticosteroids are the main medications used in the treatment of sarcoidosis. However, their use can be abandoned if the disease is mild. However, when lung function deteriorates, or if the heart or brain is affected by disease, their use becomes necessary.
For ocular sarcoidosis, steroids are used in the form of eye drops. If there is no response to the above therapy, immunosuppressants such as methotrexate are administered.
Severe disease may be an indication for the use of biological therapy that uses antibodies. Long-term progressive sarcoidosis with severe respiratory failure is treated with lung transplantation.