Features of the composition and pharmacological action of Dexalgin
The components of one tablet are presented:
- dexketoprofen trometamol;
- corn starch;
- glycerol palmitostearate;
- microcrystalline cellulose;
- titanium dioxide;
- propylene glycol;
- sodium carboxymethyl starch;
- hypromellose;
- Macragol 600.
The injection solution contains a similar active ingredient, additional components are sodium chloride and hydroxide, ethanol, and purified water.
The medicine is included in the subgroup of NSAIDs; half an hour after use, a decrease in pain and temperature is noted. The drug has an anti-inflammatory effect. The maximum concentration of Dexalgin when taken orally occurs after 40 minutes, the half-life by the kidneys does not exceed 2 hours. With MK injections it is achieved after 10 minutes.
Dexalgin®
Dexalgin® should not be mixed in the same syringe with a solution of dopamine, promethazine, pentazocine, pethidine or hydroxyzine (a precipitate will form).
Dexalgin® can be mixed in one syringe with a solution of heparin, lidocaine, morphine and theophylline.
Dexalgin® - diluted solution for infusion should not be mixed with promethazine or pentazocine.
Dexalgin® - diluted solution for infusion is compatible with the following injection solutions: dopamine, heparin, hydroxyzine, lidocaine, morphine, pethidine and theophylline.
When storing Dexalgin® - diluted solutions for infusion in plastic containers or when using infusion systems made from ethyl vinyl acetate, cellulose propionate, low-density polyethylene or polyvinyl chloride, absorption of the active substance by the listed materials does not occur.
The following interactions are common to all NSAIDs.
Undesirable combinations
With other NSAIDs, including salicylates in high doses (more than 3 g/day):
simultaneous administration of several NSAIDs due to the synergistic effect increases the risk of gastrointestinal bleeding and ulcers.
With oral anticoagulants, heparin in doses exceeding prophylactic doses, and ticlopidine
: increased risk of bleeding due to inhibition of platelet aggregation and damage to the mucous membrane of the gastrointestinal tract.
With lithium preparations:
NSAIDs increase the level of lithium in the blood, up to toxic levels, and therefore this indicator must be monitored when prescribing, changing the dose and after discontinuation of NSAIDs.
With methotrexate in high doses (15 mg/week or more)
: increased hematological toxicity of methotrexate due to a decrease in its renal clearance during NSAID therapy.
With hydantoins and sulfonamide drugs:
the risk of increased toxic effects of these drugs.
Combinations requiring caution
With diuretics, angiotensin-converting enzyme inhibitors:
NSAID therapy is associated with a risk of acute renal failure in dehydrated patients (decreased glomerular filtration due to decreased prostaglandin synthesis). NSAIDs may reduce the hypotensive effect of some drugs. When coadministered with diuretics, ensure that the patient's fluid balance is adequate and monitor renal function before prescribing NSAIDs.
With methotrexate in low doses (less than 15 mg/week):
increased hematological toxicity of methotrexate due to a decrease in its renal clearance during NSAID therapy. It is necessary to conduct weekly blood cell counts during the first weeks of concomitant therapy. In the presence of even mild renal dysfunction, as well as in elderly people, careful medical supervision is necessary.
With pentoxifylline:
increased risk of bleeding. Intensive clinical monitoring and frequent checking of bleeding time (blood clotting time) is necessary.
With zidovudine
: Risk of increased toxicity to red blood cells due to effects on reticulocytes, with the development of severe anemia one week after administration of NSAIDs. It is necessary to count all blood cells and reticulocytes 1-2 weeks after starting NSAID therapy.
With sulfa drugs:
NSAIDs may enhance the hypoglycemic effect of sulfonylureas due to their displacement from sites of binding to plasma proteins.
With low molecular weight heparin preparations:
increased risk of bleeding.
Combinations to consider
With β-blockers:
NSAIDs may reduce the hypotensive effect of beta-blockers due to inhibition of prostaglandin synthesis.
With cyclosporine and tacrolimus:
NSAIDs may increase nephrotoxicity, which is mediated by the action of renal prostaglandins. During concomitant therapy, renal function should be monitored.
With thrombolytics
: increased risk of bleeding.
With probenecid:
Plasma concentrations of NSAIDs may increase, which may be due to an inhibitory effect on renal tubular secretion and/or conjugation with glucuronic acid, requiring NSAID dose adjustment.
With cardiac glycosides:
NSAIDs may lead to increased plasma concentrations of glycosides.
With mifepristone:
Due to the theoretical risk of changes in the effectiveness of mifepristone under the influence of prostaglandin synthesis inhibitors, NSAIDs should not be prescribed earlier than 8-12 days after discontinuation of mifepristone.
With ciprofloxacin:
Data obtained from experimental studies in animals indicate a high risk of convulsions when NSAIDs are prescribed during therapy with high doses of ciprofloxacin.
Contraindications and indications for Dexalgin therapy
The instructions recommend using tablets to relieve pain caused by:
- surgical interventions - in the postoperative period;
- radiculitis, algodismenorrhea;
- menstruation, dental diseases;
- neuralgia, sciatica;
- arthrosis, rheumatoid arthritis;
- osteochondrosis, spondyloarthritis;
- proliferation of metastases in bone tissue.
The solution in injections is prescribed when it is impossible to take Dexalgin orally - after injuries, operations, and with renal colic.
The drug is contraindicated in patients:
- with individual intolerance to the component composition;
- pathologies of the gastrointestinal tract, heart, liver and kidneys;
- bronchial asthma;
- undergoing anticoagulant therapy.
Dexalgin is not prescribed to minors, during pregnancy and breastfeeding.
Dexalgin, ampoules 25 mg/ml 2 ml, 5 pcs.
Manufacturer
Berlin-Chemie/Menarini, Germany
Compound
Active ingredients:
dexketoprofen trometamol 36.9 mg (73.8 mg), which corresponds to the content of dexketoprofen 25 mg (50 mg).
Excipients:
ethanol 96% - 200 mg,
sodium chloride - 8 mg,
sodium hydroxide - up to pH 7.4,
water for d/i - up to 2 ml
pharmachologic effect
Pharmacodynamics
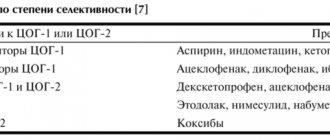
Non-steroidal anti-inflammatory drug (NSAID). It has analgesic, anti-inflammatory and antipyretic effects. The mechanism of action is associated with inhibition of prostaglandin synthesis at the level of COX-1 and COX-2.
The analgesic effect occurs 30 minutes after parenteral administration. The duration of the analgesic effect after administration at a dose of 50 mg is 4-8 hours.
When combined with the opioid analgesics dexketoprofen, trometamol significantly (up to 30-45%) reduces the need for opioids.
Pharmacokinetics
Suction
After intramuscular administration of dexketoprofen trometamol, Cmax in the blood serum is achieved on average after 20 minutes (10-45 minutes). AUC after a single dose of 25-50 mg is proportional to the dose, both with IM and IV administration. The corresponding pharmacokinetic parameters are similar after single and repeated intramuscular or intravenous administration, indicating the absence of drug accumulation.
Distribution
Dexketoprofen trometamol is characterized by a high level of binding to plasma proteins (99%). The average Vd value is less than 0.25 l/kg, the half-life of distribution is about 0.35 hours.
Removal
The main route of elimination of dexketoprofen is its conjugation with glucuronic acid followed by excretion by the kidneys. T1/2 of dexketoprofen trometamol is about 1-2.7 hours.
Pharmacokinetics in special clinical situations
In elderly people, there is an increase in the duration of T1/2 (both after a single and after repeated IM or IV administration) on average up to 48% and a decrease in the overall clearance of the drug.
Indications
- relief of pain syndrome of various origins (including postoperative pain, pain with bone metastases, post-traumatic pain, pain with renal colic, algodismenorrhea, sciatica, sciatica, myalgia, neuralgia, toothache);
- symptomatic treatment of acute and chronic inflammatory, inflammatory-degenerative and metabolic diseases of the musculoskeletal system (including rheumatoid arthritis, spondyloarthritis, arthrosis, osteochondrosis).
Use during pregnancy and breastfeeding
The use of Dexalgin® during pregnancy and lactation is contraindicated.
Contraindications
- hypersensitivity to dexketoprofen or other NSAIDs or to any of the excipients included in the drug.
- peptic ulcer of the stomach and duodenum;
- history of gastrointestinal bleeding, other active bleeding (including suspected intracranial bleeding), anticoagulant therapy;
- gastrointestinal diseases (Crohn's disease, ulcerative colitis);
- severe liver dysfunction (10-15 points on the Child-Pugh scale);
- severe renal dysfunction (creatinine clearance <50 ml/min);
- bronchial asthma (including history);
- severe heart failure;
- treatment of pain syndrome during coronary artery bypass grafting;
- bleeding diathesis or other coagulation disorders;
- childhood.
Contraindicated for epidural, intrathecal or intrathecal administration due to the ethanol contained in the drug.
With caution: the drug should be used if there is a history of allergic conditions; disorders of the hematopoietic system; for SLE or mixed connective tissue diseases; simultaneously with other medications; in case of predisposition to hypovolemia; with ischemic heart disease; in elderly patients (over 65 years old).
Side effects
Frequency of side effects:
- often (1-10%);
- uncommon (0.1-1%) rare (0.01-0.1%);
- very rare (less than 0.01%, including individual reports).
From the hematopoietic system: rarely - anemia; very rarely - neutropenia, thrombocytopenia.
From the side of the central nervous system: infrequently - headache, dizziness, insomnia, drowsiness; rarely - paresthesia.
From the senses: infrequently - blurred vision; rarely - tinnitus.
From the cardiovascular system: infrequently - arterial hypotension, feeling of heat, hyperemia of the skin; rarely - extrasystole, tachycardia, arterial hypertension, peripheral edema, superficial thrombophlebitis.
From the respiratory system: rarely - bradypnea; very rarely - bronchospasm, dyspnea.
From the digestive system: often - nausea, vomiting; uncommon - abdominal pain, dyspepsia, diarrhea, constipation, hematemesis, dry mouth; rarely - erosive and ulcerative lesions of the gastrointestinal tract, including bleeding and perforation, anorexia, increased activity of liver enzymes, jaundice; very rarely - pancreatic damage, liver damage.
From the urinary system: rarely - polyuria, renal colic; very rarely - nephritis or nephrotic syndrome.
From the reproductive system: rarely - in women - menstrual irregularities, in men - dysfunction of the prostate gland.
From the musculoskeletal system: rarely - muscle spasm, difficulty moving in the joints.
Dermatological reactions: sometimes - dermatitis, rash, sweating; rarely - acne; very rarely – photosensitivity.
Allergic reactions: rarely - urticaria; very rarely - severe skin reactions (Stevens-Johnson syndrome, Lyell's syndrome), angioedema, allergic dermatitis.
Metabolic disorders: rarely - hyperglycemia, hypoglycemia, hypertriglyceridemia.
From laboratory parameters: rarely - ketonuria, proteinuria.
Local and general reactions: often - pain at the injection site; uncommon - inflammatory reaction, hematoma, hemorrhage at the injection site, feeling of heat, chills, fatigue; rarely - back pain, fainting, fever; very rarely - anaphylactic shock, facial swelling.
Other: aseptic meningitis, occurring mainly in patients with systemic lupus erythematosus or mixed connective tissue diseases, hematological disorders (purpura, aplastic and hemolytic anemia, rarely - agranulocytosis and bone marrow hypoplasia).
Interaction
The following drug interactions are typical for all NSAIDs, including Dexalgin®.
Undesirable combinations
The simultaneous administration of several NSAIDs, including salicylates in high doses (more than 3 g/day) increases the risk of gastrointestinal bleeding and ulcers due to the synergistic action.
When used simultaneously with oral anticoagulants, heparin in doses exceeding prophylactic doses, and ticlopidine, the risk of bleeding increases due to inhibition of platelet aggregation and damage to the gastrointestinal mucosa.
NSAIDs increase the concentration of lithium in the blood plasma, up to toxic levels, and therefore this indicator must be monitored when prescribing, changing the dose and after discontinuation of NSAIDs.
When used with methotrexate in high doses (15 mg/week or more), the hematological toxicity of methotrexate increases due to a decrease in its renal clearance during NSAID therapy.
When used simultaneously with hydantoins and sulfonamide drugs, there is a risk of increased toxic effects of these drugs.
Combinations requiring caution
If simultaneous use with diuretics and ACE inhibitors is necessary, it should be taken into account that NSAID therapy is associated with the risk of developing acute renal failure in patients with dehydration (decreased glomerular filtration due to inhibition of prostaglandin synthesis). NSAIDs may reduce the hypotensive effect of some drugs. When coadministered with diuretics, ensure that the patient's fluid balance is adequate and monitor renal function before prescribing NSAIDs.
When used simultaneously with methotrexate in low doses (less than 15 mg/week), the hematological toxicity of methotrexate may increase due to a decrease in its renal clearance during NSAID therapy. Blood cell counts should be monitored weekly during the first weeks of concomitant therapy. In the presence of even mild renal dysfunction, as well as in elderly people, careful medical supervision is necessary.
When used simultaneously with pentoxifylline, the risk of bleeding increases. Intensive clinical monitoring and frequent monitoring of bleeding time (blood clotting time) is necessary.
When used concomitantly with zidovudine, there is a risk of increased toxicity to red blood cells due to effects on reticulocytes, with the development of severe anemia one week after administration of NSAIDs. It is necessary to control all blood cells and reticulocytes after 1-2 weeks. after starting NSAID therapy.
It is possible that the hypoglycemic effect of sulfonylurea derivatives may be enhanced due to its displacement from sites of binding to plasma proteins under the influence of NSAIDs.
When used simultaneously with low molecular weight heparin drugs, the risk of bleeding increases.
Combinations to consider
NSAIDs may reduce the hypotensive effect of beta-blockers due to inhibition of prostaglandin synthesis.
When used concomitantly with cyclosporine and tacrolimus, NSAIDs may increase nephrotoxicity, which is mediated by the action of renal prostaglandins. During combination therapy, it is necessary to monitor renal function.
When prescribed simultaneously with thrombolytics, the risk of bleeding increases.
When used concomitantly with probenecid, plasma concentrations of NSAIDs may increase, which may be due to inhibition of renal secretion and/or conjugation with glucuronic acid. This requires NSAID dose adjustment.
NSAIDs can cause an increase in the concentration of cardiac glycosides in the blood plasma.
Due to the theoretical risk of changes in the effectiveness of mifepristone under the influence of prostaglandin synthesis inhibitors, NSAIDs should not be prescribed earlier than 8-12 days after discontinuation of mifepristone.
Data obtained from experimental studies in animals indicate a high risk of developing convulsions when NSAIDs are prescribed during therapy with high doses of ciprofloxacin.
Pharmaceutical interactions
Dexalgin® should not be mixed in the same syringe with a solution of dopamine, promethazine, pentazocine, pethidine or hydroxyzine (a precipitate will form).
Dexalgin® can be mixed in one syringe with a solution of heparin, lidocaine, morphine and theophylline.
A diluted solution of Dexalgin® for infusion should not be mixed with promethazine or pentazocine.
A diluted solution of Dexalgin® for infusion is compatible with the following injection solutions: dopamine, heparin, hydroxyzine, lidocaine, morphine, pethidine and theophylline.
When diluted solutions of Dexalgin® for infusion are stored in plastic containers or when using infusion systems made from ethyl vinyl acetate, cellulose propionate, low-density polyethylene or polyvinyl chloride, absorption of the active substance by the listed materials does not occur.
How to take, course of administration and dosage
Dexalgin® is intended for intravenous and intramuscular administration.
Recommended dose for adults: 50 mg every 8-12 hours. If necessary, the drug can be re-administered at 6-hour intervals. The daily dose is 150 mg.
In elderly patients and patients with impaired liver and/or kidney function, therapy with Dexalgin® should be started with lower doses; the daily dose is 50 mg.
Dexalgin® is intended for short-term (no more than 2 days) use during acute pain syndrome. In the future, it is possible to transfer the patient to analgesics for oral administration.
Rules for the preparation and administration of solutions
The contents of one ampoule (2 ml) are slowly injected deep intramuscularly.
The contents of one ampoule (2 ml) are administered by slow intravenous injection lasting at least 15 seconds.
The contents of one ampoule (2 ml) are diluted in 30-100 ml of physiological solution, glucose solution or Ringer's solution (lactate). The solution should be prepared under aseptic conditions and always protected from exposure to daylight. The diluted solution (must be transparent) is administered by slow intravenous infusion over 10-30 minutes.
Overdose
Symptoms:
nausea, anorexia, abdominal pain, headache, dizziness, disorientation, insomnia.
Treatment:
symptomatic therapy; if necessary - gastric lavage, dialysis.
Special instructions
In patients with disorders of the digestive system or a history of gastrointestinal diseases, constant monitoring is required. If gastrointestinal bleeding or ulcerative lesions occur, therapy with Dexalgin® should be discontinued.
Because All NSAIDs can inhibit platelet aggregation and increase bleeding time due to slowing prostaglandin synthesis; controlled clinical studies have studied the simultaneous administration of dexketoprofen trometamol and low molecular weight heparin preparations in prophylactic doses in the postoperative period. No effect on coagulation parameters was observed. However, when prescribing Dexalgin® with other drugs that affect blood clotting, careful medical monitoring is required. Like other NSAIDs, Dexalgin® can lead to increased levels of creatinine and nitrogen in the blood plasma.
Like other prostaglandin synthesis inhibitors, Dexalgin® may have side effects on the urinary system, which can lead to the development of glomerulonephritis, interstitial nephritis, papillary necrosis, nephrotic syndrome and acute renal failure.
During therapy with Dexalgin®, as with other NSAIDs, a slight transient increase in some liver parameters, as well as a significant increase in the level of AST and ALT in the blood serum, may be observed. At the same time, monitoring of liver and kidney functions is necessary in elderly patients. In case of a significant increase in the corresponding indicators, Dexalgin® should be discontinued.
Like other NSAIDs, dexketoprofen trometamol may mask the symptoms of infectious diseases. In case of symptoms of a bacterial infection or deterioration of health during therapy with Dexalgin®, the patient should inform the doctor.
Each ampoule of Dexalgin® contains 200 mg of ethanol.
Impact on the ability to drive vehicles and other mechanisms that require increased concentration
Due to possible dizziness and drowsiness during treatment with Dexalgin®, the ability to concentrate and the speed of psychomotor reactions may decrease.
Release form
Injection
Storage conditions
In a place protected from light, at a temperature not exceeding 25 °C
Best before date
5 years
Active substance
Dexketoprofen
Conditions for dispensing from pharmacies
On prescription
Dosage form
solution for injections and infusions
Purpose
For adults as prescribed by a doctor
Indications
Radiculitis, Lumbago, Sciatica, Osteochondrosis, Arthritis, Trigeminal neuralgia, Arthrosis, Rheumatoid arthritis
Information in the State Register of Medicines
Go
Barcode and weight
Barcode: 4013054014660 Weight: 0.035 kg
Adverse reactions
During therapeutic procedures, non-standard effects may occur, manifested by:
- vomiting with nausea, high blood pressure;
- tachycardia, nettle fever, chills;
- redness, skin rashes, dermatitis;
- anemic and fainting states, cephalalgia;
- sleep disturbances, digestive disorders, bleeding.
Dexalgin tablets can cause discomfort in the epigastric area and heartburn. The injection solution causes pain and local temperature increase in the injection area, hematomas and inflammation.
The medicine must not be mixed with alcoholic beverages. Violation of the rules can provoke severe intoxication with clinical symptoms of poisoning.
Dexalgin
The following drug interactions are typical for all NSAIDs, including Dexalgin®.
Undesirable combinations
The simultaneous administration of several NSAIDs, including salicylates in high doses (more than 3 g / day), increases the risk of gastrointestinal bleeding and ulcers due to the synergy of action.
When used simultaneously with oral anticoagulants, heparin in doses exceeding prophylactic doses, and ticlopidine, the risk of bleeding increases due to inhibition of platelet aggregation and damage to the gastrointestinal mucosa.
NSAIDs increase the concentration of lithium in the blood plasma, up to toxic levels, and therefore this indicator must be monitored when prescribing, changing the dose and after discontinuation of NSAIDs.
When used with methotrexate in high doses (15 mg/week or more), the hematological toxicity of methotrexate increases due to a decrease in its renal clearance during NSAID therapy.
When used simultaneously with hydantoins and sulfonamide drugs, there is a risk of increased toxic effects of these drugs.
Combinations requiring caution
If simultaneous use with diuretics and ACE inhibitors is necessary, it should be taken into account that NSAID therapy is associated with the risk of developing acute renal failure in patients with dehydration (decreased glomerular filtration due to inhibition of prostaglandin synthesis). NSAIDs may reduce the hypotensive effect of some drugs. When coadministered with diuretics, ensure that the patient's fluid balance is adequate and monitor renal function before prescribing NSAIDs.
When used simultaneously with methotrexate in low doses (less than 15 mg/week), the hematological toxicity of methotrexate may increase due to a decrease in its renal clearance during NSAID therapy. Blood cell counts should be monitored weekly during the first weeks of concomitant therapy. In the presence of even mild renal dysfunction, as well as in elderly people, careful medical supervision is necessary.
When used simultaneously with pentoxifylline, the risk of bleeding increases. Intensive clinical monitoring and frequent monitoring of bleeding time (blood clotting time) is necessary.
When used concomitantly with zidovudine, there is a risk of increased toxicity to red blood cells due to effects on reticulocytes, with the development of severe anemia one week after administration of NSAIDs. It is necessary to control all blood cells and reticulocytes after 1-2 weeks. after starting NSAID therapy.
It is possible that the hypoglycemic effect of sulfonylurea derivatives may be enhanced due to its displacement from sites of binding to plasma proteins under the influence of NSAIDs.
When used simultaneously with low molecular weight heparin drugs, the risk of bleeding increases.
Combinations to consider
NSAIDs may reduce the hypotensive effect of beta-blockers due to inhibition of prostaglandin synthesis.
When used concomitantly with cyclosporine and tacrolimus, NSAIDs may increase nephrotoxicity, which is mediated by the action of renal prostaglandins. During combination therapy, it is necessary to monitor renal function.
When prescribed simultaneously with thrombolytics, the risk of bleeding increases.
When used concomitantly with probenecid, plasma concentrations of NSAIDs may increase, which may be due to inhibition of renal secretion and/or conjugation with glucuronic acid. This requires NSAID dose adjustment.
NSAIDs can cause an increase in the concentration of cardiac glycosides in the blood plasma.
Due to the theoretical risk of changes in the effectiveness of mifepristone under the influence of prostaglandin synthesis inhibitors, NSAIDs should not be prescribed earlier than 8-12 days after discontinuation of mifepristone.
Data obtained from experimental studies in animals indicate a high risk of developing convulsions when NSAIDs are prescribed during therapy with high doses of ciprofloxacin.
Pharmaceutical interactions
Dexalgin® should not be mixed in the same syringe with a solution of dopamine, promethazine, pentazocine, pethidine or hydroxyzine (a precipitate will form).
Dexalgin® can be mixed in one syringe with a solution of heparin, lidocaine, morphine and theophylline.
A diluted solution of Dexalgin® for infusion should not be mixed with promethazine or pentazocine.
A diluted solution of Dexalgin® for infusion is compatible with the following injection solutions: dopamine, heparin, hydroxyzine, lidocaine, morphine, pethidine and theophylline.
When diluted solutions of Dexalgin® for infusion are stored in plastic containers or when using infusion systems made from ethyl vinyl acetate, cellulose propionate, low-density polyethylene or polyvinyl chloride, absorption of the active substance by the listed materials does not occur.
The nuances of taking Dexalgin
The instructions draw attention to the following rules for using tablets:
- the dosage is calculated by the doctor individually;
- a single dose is 0.5-2 tablets (25 mg each), procedures are performed 2-6 times a day;
- the maximum daily volume of medication cannot exceed 3 tablets;
- The duration of therapy is 5 days.
The injection solution is prescribed according to a specific scheme:
- intramuscular administration - 2 ml slowly, every 8-12 hours, 50 mg, daily dosage does not exceed 0.15 g, treatment lasts for 2 days;
- intravenous – carried out according to the dosages of intramuscular treatment, the medication is administered for about 15 seconds;
- drip – 2 ml of the drug is diluted in 100 ml of physiological solution, the dropper is placed for 15-30 minutes.
Accidentally taking an excess amount of medication provokes sleep disturbances, problems with orientation in space, cephalgia, and nausea. In case of intoxication, symptomatic therapy is used.
DEXALGIN 25
Interaction
The following interactions are common to all NSAIDs.
Undesirable combinations
With other NSAIDs, including salicylates in high doses (more than 3 g/day):
simultaneous use of several NSAIDs due to the synergistic effect increases the risk of gastrointestinal bleeding and ulcers.
With anticoagulants
: Dexketoprofen, like other NSAIDs, may enhance the effect of anticoagulants such as warfarin due to high plasma protein binding, inhibition of platelet aggregation and damage to the gastrointestinal mucosa. If simultaneous use is necessary, careful monitoring of the patient's condition and regular monitoring of laboratory parameters is necessary.
With heparin:
with simultaneous use, the risk of bleeding increases (due to inhibition of platelet aggregation and damaging effects on the mucous membrane of the gastrointestinal tract). If simultaneous use is necessary, careful monitoring of the patient's condition and regular monitoring of laboratory parameters is necessary.
With glucocorticosteroids:
with simultaneous use, the risk of ulcerative lesions of the gastrointestinal tract and bleeding increases.
With lithium preparations:
NSAIDs increase the concentration of lithium in the blood plasma up to toxic levels, and therefore this indicator must be monitored when used simultaneously with dexketoprofen, changing the dosage, and also after discontinuation of NSAIDs.
With methotrexate in high doses (15 mg/week or more):
it is possible to increase the hematological toxicity of methotrexate due to a decrease in its renal clearance when used simultaneously with NSAIDs.
With hydantoins and sulfonamides:
their toxic effect may be enhanced.
Combinations
requiring caution
With diuretics, angiotensin-converting enzyme (ACE) inhibitors, aminoglycoside antibiotics, angiotensin II :
simultaneous use with NSAIDs is associated with a risk of developing acute renal failure in dehydrated patients (decreased glomerular filtration rate due to decreased synthesis of prostaglandins). When used concomitantly, NSAIDs may reduce the antihypertensive effect of some drugs. When using dexketoprofen and diuretics simultaneously, it is necessary to ensure that the patient has no signs of dehydration, and also monitor renal function at the beginning of simultaneous use.
With methotrexate in low doses (less than 15 mg/week):
it is possible to increase the hematological toxicity of methotrexate due to a decrease in its renal clearance during simultaneous use with NSAIDs. A blood cell count is necessary when coadministration is initiated. In the presence of even mild renal dysfunction, as well as in elderly people, careful medical supervision is necessary.
With pentoxifylline:
there may be an increased risk of bleeding. Close clinical monitoring and regular checking of bleeding time (blood clotting time) is necessary.
With zidovudine:
There is a risk of increased toxicity to red blood cells due to effects on reticulocytes, with the development of severe anemia one week after starting NSAID use. It is necessary to conduct a general blood test with counting the number of reticulocytes 1-2 weeks after starting NSAID therapy.
With oral hypoglycemic agents:
NSAIDs may enhance the hypoglycemic effect of sulfonylureas due to the displacement of sulfonylurea from sites of binding to plasma proteins.
Combinations
that
need to be taken into account
With
beta -blockers:
When used simultaneously with NSAIDs, the antihypertensive effect of beta-blockers may be reduced due to inhibition of prostaglandin synthesis.
With cyclosporine and tacrolimus:
NSAIDs may increase nephrotoxicity, which is mediated by the action of renal prostaglandins. During simultaneous use, it is necessary to monitor renal function.
With thrombolytics:
the risk of bleeding increases.
The risk of bleeding from the gastrointestinal tract increases when used simultaneously with serotonin reuptake inhibitors
(citalopram, fluoxetine, sertraline) and anticoagulants.
With probenecid:
it is possible to increase the concentration of NSAIDs in the blood plasma, which may be due to the inhibitory effect of probenecid on renal tubular secretion and/or conjugation with glucuronic acid; NSAID dose adjustment may be required.
With cardiac glycosides:
simultaneous use with NSAIDs may lead to an increase in the concentration of cardiac glycosides in the blood plasma.
With mifepristone:
Due to the theoretical risk of changes in the effectiveness of mifepristone under the influence of prostaglandin synthesis inhibitors, NSAIDs should not be used earlier than 8-12 days after discontinuation of mifepristone.
With quinolones:
Data obtained from experimental studies in animals indicate a high risk of developing seizures when NSAIDs are used concomitantly with quinolones in high doses.
If necessary, simultaneous use of the drug Dexalgin
®
25 with the above medications, you should consult your doctor.
Features of interaction
The abstract draws attention to the following nuances of joint therapy with Dexalgin:
- an increased risk of bleeding occurs when using anticoagulants, NSAIDs, Heparin, Ticlopidine, Citalopram, Fluoxetine, Sertraline;
- danger of toxic effects on the body - when treated with lithium preparations, Methotrexate, sulfonamides;
- prohibition on combination with cardiac glycosides, thrombolytics, quinolones without supervision by the attending physician;
- The development of acute renal failure can be provoked by diuretics and ACE inhibitors.
The injection solution must not be mixed in the same syringe with individual medications, the list includes: Pethidine, Hydroxyzine, Dopamine, Promethesine, Pentazocine.
DEXALGIN solution for intravenous and intramuscular administration 25 mg/ml ampoule 2 ml No. 10
Undesirable combinations: Simultaneous administration of several NSAIDs, including salicylates in high doses (more than 3 g/day) increases the risk of gastrointestinal bleeding and ulcers due to the synergistic action. When used simultaneously with oral anticoagulants, heparin in doses exceeding prophylactic doses, and ticlopidine, the risk of bleeding increases due to inhibition of platelet aggregation and damage to the gastrointestinal mucosa. NSAIDs increase the concentration of lithium in the blood plasma, up to toxic levels, and therefore this indicator must be monitored when prescribing, changing the dose and after discontinuation of NSAIDs. When used with methotrexate in high doses (15 mg/week or more), the hematological toxicity of methotrexate increases due to a decrease in its renal clearance during NSAID therapy. When used simultaneously with hydantoins and sulfonamide drugs, there is a risk of increased toxic effects of these drugs. Combinations requiring caution: If simultaneous use with diuretics, ACE inhibitors is necessary, it should be taken into account that NSAID therapy is associated with the risk of developing acute renal failure in patients with dehydration (decreased glomerular filtration due to inhibition of prostaglandin synthesis). NSAIDs may reduce the hypotensive effect of some drugs. When coadministered with diuretics, ensure that the patient's fluid balance is adequate and monitor renal function before prescribing NSAIDs. When used simultaneously with methotrexate in low doses (less than 15 mg/week), the hematological toxicity of methotrexate may increase due to a decrease in its renal clearance during NSAID therapy. Blood cell counts should be monitored weekly during the first weeks of concomitant therapy. In the presence of even mild renal dysfunction, as well as in elderly people, careful medical supervision is necessary. When used simultaneously with pentoxifylline, the risk of bleeding increases. Intensive clinical monitoring and frequent monitoring of bleeding time (blood clotting time) is necessary. When used concomitantly with zidovudine, there is a risk of increased toxicity to red blood cells due to effects on reticulocytes, with the development of severe anemia one week after administration of NSAIDs. It is necessary to control all blood cells and reticulocytes after 1-2 weeks. after starting NSAID therapy. It is possible that the hypoglycemic effect of sulfonylurea derivatives may be enhanced due to its displacement from sites of binding to plasma proteins under the influence of NSAIDs. When used simultaneously with low molecular weight heparin drugs, the risk of bleeding increases. Combinations to consider: NSAIDs may reduce the hypotensive effect of beta-blockers due to inhibition of prostaglandin synthesis. When used concomitantly with cyclosporine and tacrolimus, NSAIDs may increase nephrotoxicity, which is mediated by the action of renal prostaglandins. During combination therapy, it is necessary to monitor renal function. When prescribed simultaneously with thrombolytics, the risk of bleeding increases. When used concomitantly with probenecid, plasma concentrations of NSAIDs may increase, which may be due to inhibition of renal secretion and/or conjugation with glucuronic acid. This requires NSAID dose adjustment. NSAIDs can cause an increase in the concentration of cardiac glycosides in the blood plasma. Due to the theoretical risk of changes in the effectiveness of mifepristone under the influence of prostaglandin synthesis inhibitors, NSAIDs should not be prescribed earlier than 8-12 days after discontinuation of mifepristone. Data obtained from experimental studies in animals indicate a high risk of developing convulsions when NSAIDs are prescribed during therapy with high doses of ciprofloxacin. Pharmaceutical interactions: Dexalgin® should not be mixed in the same syringe with a solution of dopamine, promethazine, pentazocine, pethidine or hydroxyzine (a precipitate is formed). Dexalgin® can be mixed in one syringe with a solution of heparin, lidocaine, morphine and theophylline. A diluted solution of Dexalgin® for infusion should not be mixed with promethazine or pentazocine. A diluted solution of Dexalgin® for infusion is compatible with the following injection solutions: dopamine, heparin, hydroxyzine, lidocaine, morphine, pethidine and theophylline. When diluted solutions of Dexalgin® for infusion are stored in plastic containers or when using infusion systems made from ethyl vinyl acetate, cellulose propionate, low-density polyethylene or polyvinyl chloride, absorption of the active substance by the listed materials does not occur.
Analogs
If side effects or signs of intolerance to Dexalgin appear, the drug must be replaced with a suitable remedy. The list of analogues is presented:
- Depiofen, Brufen, Bofen;
- Vimovo, Brustan, Dexifen;
- Zo-tek, Ibuprex, Ibuprom;
- Ibunorm, Ibufen, Ibuprofen;
- Ibutard, Imet, Ketonal, Ivalgin;
- Irfen, Naproff, Majezik-sanovel;
- Novigan, Nurofen, Nurosan, Faspik, Promax.
The cost of the original and replacements may vary significantly.
Terms of sale and storage
Dexalgin is sold in pharmacies only with a doctor's prescription. The drug is stored in dark rooms at temperatures up to 25 degrees. The medicine is suitable:
- tablets - for 2 years, after expiration of the period they are disposed of together with household waste;
- solution in ampoules - up to 5 years; after preparation, the medicine retains its properties for no more than one day (provided the temperature is from 3 to 9 degrees and in a dark place).
Dexalgin in ampoules costs from 265 rubles, the price of tablets depends on the number of units in the package and starts from 279 rubles.
Use of the drug Dexalgin injection
Injected deeply intramuscularly, intravenously in a slow stream (duration of administration - at least 15 s) or intravenously by drip over 10-30 minutes. To prepare a solution of the drug Dexalgin Inject for intravenous infusion, use 30–100 ml of isotonic sodium chloride solution, glucose solution or Ringer's solution. The finished solution should be transparent and colorless; it must be protected from exposure to daylight. Adults The recommended dosage regimen is 50 mg of the drug every 8–12 hours. If necessary, a repeat dose can be administered at 6-hour intervals. The daily dose should not exceed 150 mg. Dexalgin Injection is intended for short-term use, and treatment should be limited to the period of acute symptoms (no more than 2 days). If possible, patients should be switched to an oral dosage form of the drug. Elderly patients Dose adjustment for this age category of patients is usually not required, however, due to the physiological age-related decline in renal function, it is recommended to prescribe the drug in lower doses in the presence of mild renal failure: the total daily dose in this case should not exceed 50 mg. Liver dysfunction: In patients with mild to moderate liver dysfunction (Child-Pugh score 5–9), the total daily dose should be reduced to 50 mg and liver function tests should be monitored frequently. Dexalgin Injection should not be prescribed to patients with severe liver dysfunction. Renal impairment For patients with mild renal impairment (creatinine clearance 50–80 ml/min), the daily dose is reduced to 50 mg. Dexalgin Injection should not be prescribed to patients with moderate or severe renal failure (creatinine clearance ≤50 ml/min). The diluted solution of the drug Dexalgin Inject is chemically stable for 24 hours, provided it is stored at a temperature of 25 ° C in a place protected from light. The solution of the drug must be used immediately after preparation. However, if it is not used immediately, medical personnel are responsible for the time and conditions of its storage until use. Typically, such a solution is stored for no more than 24 hours at a temperature of 2–8 ° C in a place protected from light, provided that the dilution was carried out under controlled and validated aseptic conditions. When storing diluted solutions of the drug Dexalgin Inject in plastic containers or when using infusion systems made of ethyl vinyl acetate, cellulose propionate, low-density polyethylene or polyvinyl chloride, absorption of the active component by these materials does not occur.