Anatomy of the larynx
In an adult, the larynx is located at the level of the IV-VI cervical vertebrae along the midline of the neck. At the top it comes into contact with the hyoid bone, at the bottom it passes into the trachea, at the back it is covered with fiber and communicates with the pharynx. The anterior surface of the larynx is covered with muscles, fascia and skin.
The organ has a complex anatomical structure - it contains cartilage, ligaments, many muscles and joints. The large thyroid cartilage, also called the Adam's apple, is palpated on the neck and protrudes significantly forward in men.
Functions of the larynx:
- respiratory – regulation of external respiration, its depth and rhythm;
- insulating (protective) - protection of the respiratory tract from food entering during swallowing, harmful impurities from the air (for this, a spasm of the larynx occurs), evacuation of foreign particles trapped in the respiratory tract by coughing;
- vocal (phonatory) - the formation of vowels and parts of consonant sounds when air passes through the glottis.
Laryngeal cancer is a malignant neoplasm, most often developing from squamous epithelium. Localized in all parts of the organ.
The first is the voice, the second is the melody
A person’s ability to produce sounds of different strength, pitch and timbre is associated with the movement of the vocal cords under the influence of a stream of exhaled air. The strength of the sound produced depends on the width of the glottis: the wider it is, the louder the sound. The width of the glottis is regulated by at least five muscles of the larynx. Of course, the force of exhalation itself, caused by the work of the corresponding muscles of the chest and abdomen, also plays a role. The pitch of the sound is determined by the number of vibrations of the vocal cords in 1 second. The more frequent the vibrations, the higher the sound, and vice versa. As you know, tightly stretched ligaments vibrate more often (remember a guitar string). The muscles of the larynx, in particular the vocal muscle, provide the necessary tension to the vocal cords. Its fibers are woven into the vocal cord along its entire length and can contract either as a whole or in separate parts. Contraction of the vocal muscles causes the vocal cords to relax, causing the pitch of the sound they produce to decrease.
Having the ability to vibrate not only as a whole, but also in individual parts, the vocal cords produce additional sounds to the main tone, the so-called overtones. It is the combination of overtones that characterizes the timbre of the human voice, the individual characteristics of which also depend on the condition of the pharynx, oral cavity and nose, movements of the lips, tongue, and lower jaw. The airways located above the glottis act as resonators. Therefore, when their condition changes (for example, when the mucous membrane of the nasal cavity and paranasal sinuses swells during a runny nose), the timbre of the voice also changes.
Despite the similarities in the structure of the larynx of humans and apes, the latter are not able to speak. Only gibbons are capable of producing sounds that are vaguely reminiscent of musical sounds. Only a person can consciously regulate the force of exhaled air, the width of the glottis and the tension of the vocal cords, which is necessary for singing and speech. The medical science that studies the voice is called phoniatry.
Even in the time of Hippocrates, it was known that the human voice is produced by the larynx, but only 20 centuries later Vesalius (16th century) expressed the opinion that sound is produced by the vocal cords. Even now, there are various theories of voice formation, based on individual aspects of the regulation of vocal cord vibrations. Two theories can be cited as extreme forms.
According to the first (aerodynamic) theory, voice formation is the result of vibrational movements of the vocal folds in the vertical direction under the influence of an air stream during exhalation. The decisive role here belongs to the muscles involved in the exhalation phase and the muscles of the larynx, which bring the vocal cords together and resist the pressure of the air stream. Adjustment of muscle function occurs reflexively when the mucous membrane of the larynx is irritated by air.
According to another theory, the movements of the vocal folds do not occur passively under the influence of an air stream, but are active movements of the vocal muscles, carried out by command from the brain, which is transmitted along the corresponding nerves. The pitch of the sound, associated with the frequency of vibration of the vocal cords, thus depends on the ability of the nerves to conduct motor impulses.
Some theories cannot fully explain such a complex process as voice formation. In a person who has speech, the function of voice formation is associated with the activity of the cerebral cortex, as well as lower levels of regulation, and is a very complex, consciously coordinated motor act.
Morbidity statistics
Laryngeal cancer accounts for 2.6% of all cancers. It is in first place in terms of incidence among head and neck tumors. In 95% of cases, malignant lesions of the larynx are squamous cell carcinoma, 2% each are glandular cancer and basal cell carcinoma, and 1% are rare types of cancer.
Men are more susceptible to the disease - they are diagnosed 9-10 times more often than women. 80-95% of patients are men from 40 to 60 years old. Most of them are heavy smokers.
The survival prognosis directly depends on the stage at which the cancer is detected and its location. If the tumor is detected at stage I, the five-year survival rate is 85%, at stage II – 70%, at stage III – 60%, at stage IV it decreases to 20%.
When chemoradiotherapy is started in the early stages, stable remission is achieved in 85-95% of cases, in late stages - in 30-40%.
Neoplasms of the upper part of the larynx give metastases to regional lymph nodes in 35-45% of cases, of the lower part - in 15-20%. In the area of the vocal cords, the lymphatic network is less developed, so the tumor in this area metastasizes rarely and late.
Anatomy of cartilage
When studying the structure of the larynx, special attention should be paid to the cartilage present.
They are presented as:
- Cricoid cartilage. This is a wide plate in the form of a ring, covering the back, front and sides. On the sides and edges, the cartilage has articular areas for connection with the thyroid and arytenoid cartilages.
- Thyroid cartilage, consisting of 2 plates that fuse in front at an angle. When studying the structure of a child’s larynx, these plates can be seen to converge in a rounded manner. This happens in women too, but in men it usually develops an angular protrusion.
- Arytenoid cartilages. They have the shape of pyramids, at the base of which there are 2 processes. The first, the anterior one, is the place for fastening the vocal cord, and the second, the lateral cartilage, is where the muscles are attached.
- Horn-shaped cartilages, which are located on the tops of the arytenoids.
- Epiglottic cartilage. It has a leaf-shaped form. The convex - concave surface is lined with mucous membrane, and it faces the larynx. The lower part of the cartilage extends into the laryngeal cavity. The front side faces the tongue.
Causes and risk factors
Laryngeal cancer, like other cancers, develops from mutated cells of normal tissues or benign tumors. Cell malignancy, or malignancy, occurs under the influence of external factors; there are also diseases that have a high risk of degeneration.
External factors that provoke the occurrence of laryngeal cancer:
- smoking and chewing tobacco;
- drinking alcohol;
- occupational hazards - dust, high and low temperatures, benzene vapors, petroleum products, phenol resins.
Diseases prone to malignancy:
- long-standing papillomatosis;
- fibroma with a wide base;
- leukoplakia;
- pachydermia;
- dyskeratosis;
- ventricular cysts;
- chronic inflammatory processes.
Symptoms of laryngeal cancer
The first signs of a tumor are nonspecific, they are similar to the symptoms of many inflammatory diseases, and it is difficult to suspect an oncological process from them and, even more so, to determine its location.
Early symptoms:
- low-grade fever;
- weakness, fatigue, general malaise;
- drowsiness.
Late signs vary depending on where the neoplasm develops.
Supraglottic cancer is characterized by:
- dryness and sore throat;
- discomfort and pain when swallowing, radiating to the ear on the side of the tumor, choking;
- sensation of a foreign body in the larynx;
- dull voice.
Symptoms of a neoplasm on the vocal cords:
- change in voice, loss of sonority and melody;
- hoarseness and hoarseness.
- When a tumor develops in the subglottic region, patients complain of:
- paroxysmal dry cough;
- voice disorders.
In the late period, when cancer of any localization grows into the lumen of the larynx, difficulty breathing, attacks of suffocation, putrid breath, and cough with blood clots appear. Due to discomfort when swallowing, the patient limits food intake, and exhaustion develops.
The sooner a person seeks help, the more effective the treatment will be. Even early signs (weakness, fatigue) should be a reason to visit a doctor. In this case, it is possible to diagnose the tumor at an early stage. If you experience coughing or difficulty swallowing, you should consult a doctor immediately.
Human larynx: its structure and functions
The human larynx is a flexible, finely structured organ of the respiratory system that connects the pharynx to the trachea. It is extremely important for the breathing and digestion process, as it pushes out harmful elements trying to enter the respiratory tract. Sounds are also produced in the larynx; with the help of the vocal folds, the timbre, tone and volume of a person’s speech are regulated.
The device of the larynx
The larynx consists of dense tissue and is a short tube of nine cartilages, covered with epithelium characteristic only of the throat. The cartilages are connected to each other by special ligaments.
The human larynx is located in the area of the sixth and fourth vertebrae, behind the skin on the front side of the neck. The top of the organ approaches the nasal part of the pharynx, coming into contact with the bone located under the tongue.
The structural features of the larynx completely depend on the functions assigned to this organ. Externally, the tube of the laryngeal system schematically resembles two connected triangles touching at the vertices. The tube tapers towards the center but widens at both edges. The middle of the laryngeal system is the glottis - the uppermost fold of the vestibule of the vocal cords. The areas above and below the glottis are called supraglottic and subglottic, respectively.
On the sides of the organ between the vocal fold and the vestibule of the larynx there are deep pockets - the so-called Morganian ventricles of the larynx. These components of the larynx go up and forward to the arytenoid folds. When infected, they are the first to lose their original shape, which indicates the development of the disease. The vestibular parts of the larynx, which, if the functioning of the vocal cords is disrupted, can perform their function, sometimes become the center of inflammatory processes and swelling.
The pharynx is located at the back of the larynx; large blood vessels and nerve endings run along the sides. The pulsation of the carotid arteries can be easily felt on the neck on both sides of the throat.
The vocal cords are formed by a pair of yellowish-white parallel folds connected by muscles and stretched in the cavity of the larynx. One side of the vocal cords is attached to the angle of the thyroid cartilage, the other - to the arytenoid cartilage. Slightly above the sound gap is the vestibule of the larynx - the upper part of the cavity of this organ. It is surrounded by the edges of the plates of the thyroid cartilage, closed from below with folds, in front above the vestibule there is a corner of the thyroid cartilage (the commissure is the area of the vocal cords where the thyroid plates form an angle) and the epiglottis. Between the lateral sides of the vestibule of the larynx there are slit-like ventricles, stretching to the arytenopharyngeal folds.
The lower part of the larynx, located under the glottis and externally resembling a cone, is connected to the trachea. In a child at an early age, the elastic cone of the larynx consists of plastic connective tissue. This place is prone to increased swelling and the development of inflammatory processes.
Laryngeal cartilages
The anatomy of the larynx is quite complex. This organ is a framework of six forms of cartilage. Three paired and three unpaired cartilages support the overall structure. Let's look at each cartilage separately.
Paired cartilages:
- Horn-shaped - elastic formations shaped like a cone. This type of cartilage is found on the top of the two arytenoid elements.
- The arytenoids are areas of connective tissue that visually resemble triangles located on the plates of the cricoid cartilage. Consist of hyaline cartilage.
- Cuneiform - like horn-shaped, are elastic cartilages located near the top of the arytenoid plates.
Unpaired cartilages:
- Cricoid - consists of two parts of different shapes. The first part is a lamellar structure, the second part is formed from hyaline cartilage that forms the laryngeal border of the lower part, shaped like a thin arch.
- The epiglottis is an elastic tissue that creates groove-shaped cartilage. Its task is to raise the pharynx during food intake, or more precisely, directly at the moment of swallowing it. As it descends, the epiglottic cartilage completely covers the glottis.
- The thyroid is a cartilage formed by two plates located at an angle. This cartilage is called the Adam's apple. When the plates are connected at an angle of 90 degrees - typical for men - it protrudes noticeably on the surface of the neck. In women, the cartilages that make up the Adam's apple converge at an angle of more than 90 degrees, which makes it invisible under the skin. A special membrane connects this cartilage to the hyoid bone.
Muscles of the larynx
The structure of the human larynx involves the presence of various muscles. These muscles are divided into two types - external and internal muscles of the larynx. Internal muscles are responsible for changes in the length of the vocal cords, the degree of their tension and location in the throat. During their transformation, the sound produced is regulated. The extrinsic muscles act as a unit to perform the movements of the pharynx during eating, breathing, and voice production. The following types of muscles of the laryngeal cavity are distinguished:
- adductors (constrictors) - three types of muscles, two paired and one unpaired, compressing the glottis;
- Abductors (dilitors) are fragile muscle structures, problems with which can lead to paralysis of the laryngeal ligaments. The main task of this type of muscle is to expand and open the glottis - a function opposite to the purpose of the laryngeal adductors;
- cricothyroid muscle - when it contracts, the thyroid cartilage moves upward or forward, thereby regulating the tension of the vocal cords and maintaining their tone.
Functions
The anatomy and physiology of the larynx are entirely dependent on the functions of the larynx. Human life activity is directly related to its three main tasks - respiratory, protective and voice-forming. Let's look at each of them in more detail.
- Respiratory function: Without air, the human body cannot exist. The larynx, being part of the respiratory system, regulates the flow of oxygen into the throat. This activity is carried out due to the expansion and contraction of the glottis. Also, in the throat, too cold air warms up to pass into the lungs in this form.
- Protective function: carried out due to the work of many glands located on the epithelial layer. One of the ways of protection is the presence of so-called cilia - nerve endings. If pieces of food accidentally enter the respiratory system rather than the esophagus, the cilia immediately react and coughing attacks occur, allowing the foreign object to be pushed out. The epithelium directs any harmful element back into the external environment. When a foreign object hits the glottis, it completely closes access to the inside of the larynx and pushes it out using reflex actions (clearing the throat). The tonsils are located in the larynx - part of the immune system that fights elements of the pathogenic environment and does not allow them to enter the body. Porous tonsils trap germs and viruses with the help of special depressions - lacunae.
- Voice-forming function of the larynx (phonatory): the sound produced by a person is regulated here. The timbre of the voice depends on the structure of the human larynx and its individual characteristics. The length of the vocal cords determines the tone of the voice—the shorter the vocal cords, the higher the pitch. Therefore, high voices are typical for women and children with short vocal chords. In boys, by a certain age, a metamorphosis of the laryngeal structure occurs, and the voice begins to break. The phonatory function of the larynx is the most musical: the vocal cords allow us to sing and speak beautifully, subject to professional voice control. Interestingly, only a couple of octaves may be enough for singing, but up to seven octaves are usually involved in speech production.
The respiratory function is directly related to the protective function, since muscles and cartilage control the force and volume of inhalation and warm the air before it enters the lungs.
Let us focus on the voice-forming function of the larynx as the main one.
Voice-forming function
The structure of the throat and larynx may change depending on age. Babies have a short larynx, located three vertebrae higher than that of adults. The entrance to the larynx in children is much wider; they do not yet have corniculate cartilages and sublingual joints, which appear only at the age of seven.
In boys and girls under ten years of age, the structure of the larynx is practically the same. Next, age-related characteristics of the larynx are formed - in adolescence (after twelve years), the voice of boys begins to break. This occurs due to the increased production of male sex hormones and the development of the gonads, which leads to an increase in the length of the vocal cords. Transformation of the larynx is also typical for girls, but the change in the voice in women appears slowly and imperceptibly, and in men the voice can be significantly modified within one year.
The male larynx is about a third larger than the female, and the vocal cords are thicker and longer, so the stronger sex usually has a rougher and lower voice. The volume of speech depends on the width of the glottis, which is regulated by five muscles - the larger the gap, the louder the sound. When you exhale air, the vocal cords begin to move, this affects the change in the strength of the voice, its timbre, and pitch. In addition to the larynx, the lungs and chest muscles are involved in the process of speech formation - the sonority of the voice also depends on their strength.
The phonatory function of the larynx is a consequence of the coordinated work of the entire human body. The larynx is involved in the formation of sound; the oral cavity, lips and tongue transform it into speech. Many organs are connected to the larynx, and human health depends on their general condition.
This suggests that human speech - the timbre and tone of the voice - are a reflection not only of the structural features of the larynx, the mood of the individual, and an indicator of the activity of other body systems. A change in a person’s voice can indicate his physical condition or the presence of health problems. The timbre of the voice changes when a person has a cold, sore throat, or suffers from other throat diseases. Even taking hormones can lead to a temporary change in voice.
The vocal muscle provides the necessary tension on the vocal cords. It can be reduced either completely or partially. When the ligaments relax, speech becomes lower.
Due to the fact that the muscle creates local tension in the vocal cords, it becomes possible to reproduce additional sounds - overtones. It is their combination that determines the timbre of human speech.
Innervation and blood circulation
The blood supply to the larynx and thyroid glands is carried out using the carotid and subclavian arteries. The posterior laryngeal and thyroid arteries are also adjacent to the larynx.
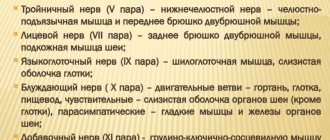
Innervation of the larynx is the presence of nerve endings in the anatomy of the throat. Excitation and transmission of nerve impulses occurs thanks to the vagus nerve, consisting of parasympathetic, sensory motor fibers. The vagus nerve ensures the reflex function of the organ - the transfer of neurons to the cortical speech and sound centers. The nerve fibers form a pair of large nerve ganglia.
The first node consists of two types of fibers: external - innervates the lower muscle, responsible for contractions of the throat and cricothyroid cartilage, and internal - penetrates the mucous membrane of the larynx, located above the sound lumen, the mucous membrane of the epiglottis and the beginning of the tongue.
The recurrent nerve contains the same types of fibers; the right recurrent laryngeal nerve separates from the vagus nerve where it intersects the subclavian artery. On the left, the recurrent nerve splits off from the vagus at the height of the arched aorta. Two nerves surround the vessels and rise up on opposite sides of the larynx, cross under the thyroid gland and adjoin the subglottic cavity of the larynx.
The nervous system occupies an important place in the anatomy of the larynx; its damage can lead to serious consequences. When one side of the larynx is affected, only one side of the vocal cords and laryngeal cavity is affected. Damage to both sides leads to problems with the functioning of the respiratory system.
The structure of the larynx is extremely interesting and is determined by its functions. Studying the anatomy of this organ is necessary not only to broaden your horizons, but also to conduct self-examination in case of urgent need. With the appropriate knowledge, you will be able to take adequate measures for diseases of the larynx and do not miss the moment to consult a doctor to choose proven methods of prevention or begin effective treatment.
Classification
Classification of laryngeal cancer is carried out according to different criteria.
Localization of education
There are three anatomical sections of the organ:
- supraglottic (vestibular);
- middle (vocal cords);
- subglottic
Cancer of the supraglottic region develops most often - from 65% to 70% of all laryngeal tumors. It appears on one side and quickly spreads to the other. Neoplasms in this area are characterized by aggressive growth and rapid appearance of metastases.
A tumor of the middle section is diagnosed in 25-30% of cases. Usually develops on one vocal cord. Less aggressive than in the supraglottic. Voice disorders force patients to see a doctor quickly, which is why ligament tumors are often detected in the early stages. Localization of the formation facilitates surgical access to it.
Neoplasms of the subglottic region are the rarest - approximately 2% of cases. At the same time, they are characterized by fairly rapid infiltrative growth, and their location complicates surgical access and increases the risk of injury to the vocal cords during surgery.
Stages of laryngeal cancer, Russian classification
According to the prevalence of the process, malignant lesions of the larynx are divided into four stages - I, II, III and IV, stage III has substages a, b, IV - a, b, c, d.
| Stage | Characteristic |
| I | The formation is limited in size and does not extend beyond the mucous membrane of one anatomical part of the larynx. |
| II | The process completely covers one anatomical part of the larynx (all layers can be involved), does not spread beyond its limits, and does not metastasize. |
| III | a – the tumor extends beyond one anatomical part of the larynx, spreads to adjacent tissues, and causes immobility of half of the larynx. b – in addition to the spread of cancer to neighboring anatomical areas, regional lymph nodes are affected: one fixed or several mobile enlarged nodes are detected. |
| IV | a – spread of the tumor to neighboring organs. b – the formation occupies a significant part of the larynx and penetrates into the underlying tissue. c – fixed metastases are detected in the lymph nodes of the neck. d – tumor of any size, metastasizes to regional lymph nodes and distant organs. |
Growth pattern
Exophytic cancer - grows into the lumen of the organ or outward. The formation usually occurs on the wall of the larynx and grows outward, blocking the lumen of the upper respiratory tract. It has no clear boundaries, the surface of the tumor is lumpy, with papillary growths.
Endophytic (infiltrative) cancer - grows inward, into the tissue of the organ. It looks like an infiltrate with ulcerations, without clear contours. Penetrates into the thickness of adjacent tissues.
Mixed - combines the features of exo- and endophytic growth.
Histological structure
Most often, laryngeal cancer arises from squamous epithelial cells. Glandular cancer, basal cell carcinoma and other rare types of tumor are diagnosed much less frequently. Some types are further subdivided:
- Squamous cell carcinoma : non-keratinizing – arises from non-keratinizing epithelium, grows quickly, has a high risk of metastases;
- keratinizing – develops slowly, metastases appear after a long period of time.
- poorly differentiated - it is difficult to determine the type of cells and tissues that make up the neoplasm, the tumor is characterized by a high degree of malignancy, grows quickly and metastasizes;
Anatomical structure
To understand the functions of the larynx, it is necessary to clearly understand its anatomical structure.
Cartilage
The components of the organ in question are paired cartilages:
- thyroid,
- ring,
- epiglottis.
Among the unpaired cartilages the following stand out:
- arytenoid,
- cricoid.
The cartilages presented above are interconnected by ligaments and joints, due to which they can move, facilitated by the muscles of the larynx.
The cricoid cartilage looks like a ring, its ring looks forward, the “stone” looks back. Next, the thyroid and arytenoids are attached. The largest is the thyroid. It forms walls. Their parts are plates that stand at an obtuse angle in women, and at an acute angle in men (due to which the “Adam’s apple” protrudes).
The arytenoid cartilages are a pyramid, the base of which is attached to the cricoid cartilage. Two types of processes extend from the arytenoids:
- muscular,
- voice.
The muscular process controls the arytenoid cartilage, causing the vocal process to change position and influence the attached vocal cord.
- What is the human pharynx and oropharynx: structure, functions
All of the listed cartilages are hyaline, that is, they have the following characteristics:
- density,
- glassiness,
- elasticity.
They show a tendency to ossify. Ossification can occur as an age-related change, which affects the timbre of the voice.
Epiglottis
This part is a kind of “lifting shield” above the entrance of the laryngeal opening. From below, the epiglottis adjoins the thyroid cartilage. The main function representing the operation of this part of the system under consideration is to protect the respiratory entrance from foreign particles entering the lungs by closing its entrance.
Vocal cords
The ligaments are the primary mechanics that produce sound, traveling from the vocal processes to the thyroid cartilage. Between their pair there is a gap that allows a stream of air to pass through when a person breathes.
Laryngeal muscles
The muscles of this system are divided into large groups:
- internal, whose role is to guide the vocal cords,
- external, controlling the movements of the pharynx.
Intrinsic muscles exhibit a special distribution pattern:
- sound laryngeal, that is, the main adductors, there are only three of them,
- abductor - one muscle,
- cricothyroid muscle, which controls the tension of the ligaments.
Each type of muscle listed above performs a number of functions:
- the abductor expands the glottis, if it is damaged, this threatens the loss of speech abilities,
- adductors are responsible for narrowing the glottis, paired and unpaired types of muscles work simultaneously,
- The cricothyroid muscle controls the thyroid cartilage upward and forward, exerting proper tension on the ligaments.
The extrinsic muscles of the larynx are classified as:
- sternothyroid,
- thyrohyoid,
- thyroid.
The coordinated work of these muscles makes it possible to carry out movements of the pharynx during swallowing, breathing, and speech production.
- Cricoid unpaired cartilage of the larynx: its structure and functions
The main function of muscles is to change the position of the cartilage of the organ. The muscles of the larynx, according to the nature of their action on the glottis, are divided as follows:
- expanding,
- narrowing,
- changing the tension of the ligaments.
Thanks to the work of the muscles, the entire work of the system in question is carried out. Without them, breathing, respiratory protection, and speech production are impossible.
Laryngeal cavity
The cavity has an hourglass shape. The middle part, which is greatly narrowed, contains folds of the vestibule, or the so-called false vocal folds. The vocal cords are located below. On the sides are the ventricles, which are atavistic in nature. In some animals, such bags are very developed and serve as resonators.
The entire cavity, except for the ligaments, is lined with a mucous membrane consisting of ciliated epithelium, which reacts to the slightest touch thanks to a huge number of glands that cause a cough reflex when the mucosa is irritated by any foreign object. The mucous membrane covers the fibro-elastic membrane.
Diagnosis of laryngeal cancer
During the initial visit, the doctor collects an anamnesis of the patient’s life and illness, asks him about the presence of provoking factors, conducts a visual examination, palpation of the neck, indirect laryngoscopy - examination of the larynx with a mirror on a long curved handle.
If there is still suspicion of a tumor formation, the patient is prescribed direct laryngoscopy . This is an invasive diagnostic procedure during which the larynx, trachea, and bronchi are examined using a laryngoscope (rigid method) or a flexible fiberscope. As a rule, during direct laryngoscopy, a biopsy of the neoplasm is performed - biomaterial is taken for cytological and histological analysis.
of tumor markers SCC and CYFRA 21-1 is considered an effective diagnostic method . To analyze tumor markers, venous blood is taken from the patient.
To assess the degree of tumor invasion, damage to the lymph nodes, and the presence of metastases in distant organs and tissues, additional procedures are used: CT or MRI , PET scan , biopsy of sentinel lymph nodes , scintigraphy , radiography .
Treatment methods
For laryngeal cancer , radiation chemotherapy (rarely), targeted therapy , and surgery . A single method or an integrated approach can be used, depending on the stage of the tumor, its location, degree of aggressiveness, growth pattern, and extent of the process.
Conservative therapy
Almost always, the first stage of treatment is radiation therapy . It is used to treat cancer of the middle section of the larynx, which is highly radiosensitive, as well as for tumors of the upper and lower regions of the larynx of stages I-II. Radiation is sometimes combined with hyperbaric oxygenation - saturating the blood with oxygen in a special chamber. This procedure enhances the effect of rays on degenerated cells and reduces damage to healthy tissue.
Treatment of stage III-IV laryngeal cancer, localized in the upper region of the organ, begins with chemotherapy . Chemotherapy is ineffective for the lower and middle parts of the larynx.
Radiation and chemotherapy can be used in combination.
Targeted therapy is the directed effect of a drug on the epidermal growth factor receptor. In laryngeal cancer, a large amount of the EGFR receptor protein is often found on the surface of tumor cells, which stimulates cell division. The drug Cetuximab, used for targeted therapy of the disease, suppresses the activity of this receptor. The drug is administered intravenously, usually used in combination with radiation, and in later stages - together with chemotherapy.
Surgical treatment
Sometimes, for stages I-II of laryngeal cancer, conservative therapy is sufficient. If it turns out to be ineffective, as well as for tumors detected at stages III-IV, surgical intervention is recommended. Before surgery, radiation therapy is always indicated to reduce the size of the tumor.
For stage I-II tumors, doctors try to perform organ-preserving resection: hemilaryngectomy - removal of one vocal cord, supraglottic laryngectomy - removal of part of the larynx above the ligamentous apparatus.
In the early stages, laser removal of the tumor using an endoscope can be used. The advantage of this method is that it is less traumatic; the disadvantage is that it is not possible to take a tissue sample for histological examination.
In later stages of the disease, it is necessary to resort to radical operations: chordectomy - complete removal of the vocal cords, total laryngectomy. In this case, the patient completely loses his voice.
Auxiliary Operations
In addition to direct removal of the malignant tumor, other surgical operations are performed. When laryngeal cancer metastasizes to regional lymph nodes or there is a high risk of metastases, these nodes are excised along with the surrounding tissue. The operation is called a cervical dissection .
When the larynx is completely removed, the patient needs a tracheostomy , a surgically created hole in the trachea. When creating a tracheostomy, the upper end of the trachea is sutured to the skin of the neck.
If laryngeal cancer makes it difficult to eat, the patient will have gastrostomy tube placed directly into the stomach.
If necessary, after extensive surgery, reconstructive plastic - operations that allow at least partially restoring the functions of the removed organs.
Pain in the larynx
General information
The larynx is the upper part of the respiratory tract and also the organ of voice production. It is located at the level of the III-VI cervical vertebrae (slightly higher in children), opens from above into the pharynx, and below passes into the trachea. The skeleton of the larynx is formed by cartilages:
unpaired (cricoid, thyroid, epiglottis);
paired (arytenoid, corniculate, wedge-shaped)
They are connected to each other by joints and ligaments. The hypoglossoid membrane connects the larynx to the hyoid bone. Between the thyroid and cricoid cartilages is the cricothyroid ligament. It is sometimes resorted to dissection in case of acute laryngostenosis.
On the inner surface of the larynx there are vocal folds, the basis of which are paired vocal cords and vocal muscles. Above them are the vestibular folds, their basis is made up of the ligaments of the vestibule. Between the vestibular and vocal folds on each side are the ventricles of the larynx .
The space between the vocal folds is called the glottis. There are three sections in the laryngeal cavity: the upper, or vestibule (above the vestibular folds), the lower (under the vocal folds) and the middle, narrowest, located between the vestibular and vocal folds. The mucous membrane of the larynx is covered with columnar ciliated epithelium. On the vocal folds and upper parts of the epiglottis, the epithelium is multilayered squamous. The submucosal layer of the lower part of the larynx is loose, prone to swelling, especially in childhood. The larynx performs a respiratory, protective (spasm of the larynx and cough when a foreign body enters it or the presence of harmful impurities in the air) and voice-forming functions.
Pain in the larynx due to illness
With bruises, compression, cartilage fractures , or separation of the larynx from the trachea, shock may occur. Other signs of damage are expressed by the following characteristic symptoms:
- hemoptysis;
- pain in the larynx when swallowing and coughing;
- labored breathing.
On palpation , crepitus of the subcutaneous tissue (subcutaneous emphysema) and crunching of broken cartilages are noted. The victim may be at risk of suffocation caused by displacement, laryngeal edema and mediastinal emphysema. Poisoning with acids and caustic alkalis (acetic essence, soldering liquid, bath washing liquid, carbolic, oxalic acid, caustic soda, ammonia). Signs of poisoning are burns of the lips, oral mucosa, as well as:
- pain in the larynx;
- copious amounts of saliva;
- bloody vomiting.
The most common inflammatory diseases of the larynx are acute and chronic laryngitis. Less commonly, abscess, phlegmon, chondroperichondritis, diphtheria, tuberculosis and syphilis of the larynx develop. An abscess occurs as a result of the introduction of infectious agents during injury to the mucous membrane of the larynx. The disease initially occurs as a common sore throat, followed by hoarseness and difficulty breathing. Phlegmon of the larynx occurs with the following symptoms:
- high body temperature;
- chills;
- difficulty breathing;
- sharp pain in the larynx when swallowing,
Against this background, and also as a complication of influenza , chondroperichondritis of the larynx can occur, in which the inflammatory process spreads to the hyaline cartilages of the larynx, causing them to suppurate and melt with the formation of fistulas and sequestration. Diphtheria of the larynx (diphtheria croup) occurs more often in children. Due to the formation of fibrinous exudate in the area of the vocal cords and under them, increasing stridor, laryngostenosis develop, and pain in the larynx . Severe intoxication is noted. Laryngeal tuberculosis is often a complication of pulmonary tuberculosis. Patients' complaints of a sore throat, pain in the larynx, and hoarseness depend on the stage, location, extent and form of the process. When diagnosing, one should take into account the medical history, complaints, general condition of the patient, laboratory data (detection of Mycobacterium tuberculosis in sputum, results of tuberculin tests). A patient with suspected laryngeal tuberculosis should be referred to a phthisiatrician or otolaryngologist. Of the benign tumors, the most common are fibromas and papillomas . Angiomas and lymphangiomas are rarely observed. The main symptom of benign tumors of the larynx is hoarseness and pain in the larynx. To establish a diagnosis in all cases, a histological examination of the material obtained from a tumor biopsy is necessary.
Laryngeal cancer
Laryngeal cancer occurs predominantly in men, usually over the age of 40. Precancerous diseases of the larynx can be:
- leukoplakia;
- papillomas;
- keloid scars.
With cancer of the upper part (vestibule) of the larynx, there is soreness, a sensation of a foreign body, and pain in the larynx when swallowing, often radiating to the ear. With cancer of the true vocal cords, the most characteristic initial symptom is hoarseness .
With cancer of the lower larynx, slowly increasing difficulty breathing and hoarseness are more typical. As the tumor spreads to surrounding tissues and organs, these symptoms intensify, laryngostenosis gradually develops, metastases appear in the lymph nodes and nodes of the neck, and the general condition of the patients worsens.
When localized on the true vocal cords, voice formation is disrupted very early: first, the timbre of the voice changes, it becomes rough, and then hoarseness . Hoarseness most often forces the patient to see a doctor.
Later, as the tumor grows, the hoarseness intensifies, and the patient can only speak in a whisper. Along with this, another symptom develops, shortness of breath. In advanced stages, pain appears when swallowing.
With cancer of the epiglottis and arytenoid cartilages, the feeling of pain is preceded by a feeling of awkwardness or something foreign. In case of tumor disintegration and secondary perichondritis, pain in the larynx increases significantly. After some more time, hemoptysis, choking, and difficulty in passing food through the esophagus appear.
The decaying tumor emits a stench. Patients lose weight, become weaker, and cachexia increases. Clinical manifestations of laryngeal cancer are quite varied and depend primarily on the location and extent of the tumor lesion . Symptoms of cancer of the supraglottic region are scanty; at first, mainly unpleasant sensations or slight pain in the larynx are noted.
When the vocal folds are affected, the early and main symptom is gradually increasing hoarseness . Only cancer of the subglottic region occurs latently for a long time, difficulty breathing increases gradually and hoarseness increases slowly.
Other reasons
Foreign bodies enter the larynx mainly from the oral cavity. More often observed in children who have the habit of holding small objects in their mouths. A dangerous condition associated with small objects entering the respiratory tract: fish bones, needles, beads, coins. If the foreign body cannot be coughed out, it slips down into the trachea (all the way to the bronchi).
Larger objects can cause complete blockage of the lumen of the larynx - suffocation develops. With small foreign bodies, a convulsive cough, pain in the larynx, the face and lips turn blue, and hoarseness are observed. When completely blocked, suffocation occurs and death occurs. The main symptoms of gastroesophageal reflux disease are:
- heartburn;
- acute pain in the larynx;
- air burps;
- burning and feeling of pressure.
Zhennia occurs in the epigastric region 15-40 minutes after eating and is provoked by foods that stimulate the synthesis of acid and bile: fried, spicy food, sour juices, alcohol, especially dry red wine, carbonated drinks, consumption of soft-boiled eggs, radishes, radishes, large amounts of vegetable fat If you have pain in the larynx, seek help from an otolaryngologist, oncologist, or infectious disease specialist.
Forecast
The prognosis of the disease depends on how early the tumor is detected. Unfortunately, laryngeal tumors are often diagnosed late due to the nonspecificity of early symptoms.
Newly diagnosed stage III laryngeal cancer is 46.8%, stage IV – 17.0%. The mortality rate in the first year from the moment of diagnosis for lesions of the larynx is 24.2%.
A large number of patients develop resistance to radiation and chemotherapy. When conservative therapy is used, recurrent tumors occur in 20-40% of cases, the treatment of which is only possible through surgery.
Without treatment, laryngeal cancer lasts from one to three years. The prognosis of 85-90% of cases of complete recovery is given only if the tumor is detected early, treatment is started in a timely manner and completely completed.
Prevention of laryngeal cancer
Quitting smoking cigarettes, pipes, hookahs, and chewing tobacco is the basis for preventing the disease. Eliminating alcoholic beverages or reducing their consumption will help prevent not only laryngeal cancer, but also other pathologies.
There is an opinion that red meat and smoked meats increase the risk of cancer. You should reduce their number in the menu, eat fresh vegetables and fruits more often.
It is important to undergo medical examinations on time - medical examinations, medical examinations at enterprises. If you suspect a disease of the larynx, even if general symptoms appear, you should consult a doctor.
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.