Cardosal plus film tablet 12.5mg+20mg 28 pcs
Pharmacological group:
Angiotensin II receptor antagonist.
Pharmacodynamics:
Olmesartan medoxomil - the active substance of the drug Cardosal® 20 - is a powerful specific antagonist of angnotensin II receptors (type AT1) for oral administration. Angiotensin II is the primary vasoactive hormone of the renin-angiotensin-aldosterone system and plays a significant role in the pathophysiology of arterial hypertension by acting on AT1 receptors. It is assumed that olmesartan blocks all actions of angnotensin II mediated by AT1 receptors, regardless of the source and pathway of angnotensin II synthesis. The specific antagonism of olmesartan towards angiotensin II receptors (AT1 type) leads to an increase in the activity of renin, angiotensin I and II in the blood plasma, and also helps to reduce the plasma concentration of aldosterone.
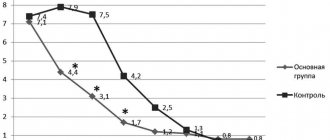
In arterial hypertension, olmesartan causes a dose-dependent, long-term decrease in blood pressure (BP). There is no evidence of the development of arterial hypotension after taking the first dose of the drug, of tachyphylaxis during long-term treatment, or of the “withdrawal” syndrome (a sharp increase in blood pressure after discontinuation of the drug).
Taking olmesartan medoxomil once a day provides an effective and mild reduction in blood pressure within 24 hours, and the effect after a single dose is similar to the effect of taking the drug twice a day at the same daily dose. The antihypertensive effect of olmesartan usually develops within 2 weeks, and the maximum effect develops approximately 8 weeks after the start of therapy.
Pharmacokinetics:
Absorption and distribution: Olmesartan medoxomil is a prodrug. It is rapidly converted to the pharmacologically active metabolite olmesartan by enzymes in the intestinal mucosa and in the portal blood during absorption from the gastrointestinal tract. Olmesartan medoxomil unchanged in blood plasma is not detected in blood plasma and/or feces. The bioavailability of olmesartan averages 25.6%.
The maximum concentration (Cmax) of olmesartan in blood plasma is achieved on average 2 hours after oral administration of olmesartan medoxomil and increases approximately linearly with increasing single dose to 80 mg.
Food intake does not have a significant effect on the bioavailability of olmesartan, therefore olmesartan medoxomil can be taken regardless of meals.
There were no clinically significant differences in the pharmacokinetic parameters of olmesartan depending on gender.
Olmesartan is bound to plasma proteins (99.7%), but the potential for a clinically significant shift in the magnitude of protein binding when olmesartan interacts with other highly binding and concomitantly used drugs is low (this is confirmed by the lack of clinically significant interaction between olmesartan and warfarin). The association of olmesartan with blood cells is insignificant. The mean volume of distribution after intravenous administration is low (16-29 L).
Metabolism and elimination: Total plasma clearance is typically 1.3 L/h (coefficient of variation 19%) and is relatively low compared to hepatic blood flow (approximately 90 L/h). Olmesartan is eliminated in two ways. After a single oral dose of 14C-labeled olmesartan medoxomil, 10-16% of the radioactive substance was excreted by the kidneys (most of it within 24 hours after taking olmesartan medoxomil), and the remaining radioactive substance was excreted through the intestines. Taking into account the systemic bioavailability of 25.6%, it can be calculated that approximately 40% of absorbed olmesartan is excreted through the kidneys, and about 60% through the hepatobiliary system. The released radioactive substance was olmesartan. No other metabolites were detected. Enterohepatic recirculation of olmesartan is minimal. Since most of olmesartan is eliminated through the liver, its use in patients with biliary obstruction is contraindicated (see section Contraindications).
The half-life of olmesartan is 10-15 hours after repeated oral administration. A steady state is achieved after taking the first few doses of the drug, and after 14 days of repeated use, no further accumulation is observed. Renal clearance is approximately 0.5-0.7 l/h and is independent of the dose of the drug.
Pharmacokinetics in patients with renal failure
In patients with renal impairment, the area under the steady-state concentration-time curve (AUC) was increased by approximately 62%, 82%, and 179% for mild, moderate, and severe impairment, respectively, compared with healthy volunteers.
Pharmacokinetics in patients with liver failure
After a single oral dose, the AUC values for olmesartan were 6% and 65% higher in patients with mild to moderate hepatic impairment, respectively, compared to healthy volunteers. The unbound fraction of olmesartan 2 hours after dosing in healthy volunteers and in patients with mild and moderate hepatic impairment was 0.26%, 0.34% and 0.41%, respectively. After repeated oral administration, the AUC for olmesartan in patients with mild to moderate hepatic impairment was 65% higher than in healthy control subjects. The mean Cmax values of olmesartan in patients with liver failure and healthy volunteers were similar. The pharmacokinetics of olmesartan medoxomil in patients with severe hepatic impairment have not been studied.
Pharmacokinetics in patients 65 years of age and older
In elderly (65-75 years) and geriatric patients (75 years and older) with arterial hypertension, the AUC of olmesartan at steady state was greater by 35% and approximately 44%, respectively, compared with younger patients, which may be partly due to associated with age-related decline in kidney function.
Side effects
- Hematopoietic reactions: thrombocytopenia.
- Reactions from nervous activity: dizziness , headache .
- Reactions from breathing: cough, rhinitis, pharyngitis, bronchitis.
- Digestive reactions: nausea, diarrhea, dyspepsia , abdominal pain, gastroenteritis , vomiting.
- Skin reactions: itching , skin rash, allergic dermatitis, Quincke's edema, urticaria.
- Reactions from the musculoskeletal system: pain in bones and joints, arthritis, back pain, cramps .
- Reactions from the genitourinary tract: genitourinary tract infections, hematuria, acute renal failure.
- Reactions from laboratory tests: increased levels of urea and creatinine in the blood, increased levels of liver enzymes.
- Circulatory reactions: tachycardia, angina , decreased blood pressure.
- Metabolic reactions: increased creatine phosphokinase levels, hyperuricemia, hypertriglyceridemia, hyperkalemia.
- General reactions: flu-like symptoms, chest pain, asthenia , peripheral edema, malaise, fatigue, drowsiness .
Instructions for use of Cardosal (Method and dosage)
Instructions for use of Cardosal prescribe taking the drug orally every day at the same time, once a day.
The recommended initial dose is 10 mg once daily. If the blood pressure reduction is not sufficient when taking 10 mg per day, it can be increased to 20 mg per day. If additional pressure reduction is required, the dosage is increased to a maximum of 40 mg per day or a diuretic (for example, hydrochlorothiazide ).
The highest daily dose is 40 mg.
Interaction
Concomitant use with potassium supplements, potassium-sparing diuretics or other drugs that can increase potassium in the blood is not recommended.
The antihypertensive effect of treatment with olmesartan is enhanced when used in combination with other antihypertensive drugs.
Nonsteroidal anti-inflammatory drugs, cyclooxygenase type 2 inhibitors, and angiotensin type 2 receptor blockers may interact synergistically to inhibit glomerular filtration. In this case, there is a possibility of acute renal failure . To avoid such phenomena, it is recommended to monitor kidney function at the beginning of therapy, as well as timely intake of a sufficient volume of fluid.
When used together with antacids , a moderate decrease in the bioavailability of olmesartan is possible.
The use of olmesartan together with lithium preparations is dangerous due to an increase in the concentration of the latter in the blood.
Overdose of the drug Cardosal plus, symptoms and treatment
There is no data on an overdose of Cardosal Plus. The most likely symptoms of an overdose of olmesartan medoxomil may be hypotension, tachycardia or bradycardia. In case of an overdose of hydrochlorothiazide, nausea, drowsiness, muscle cramps and heart rhythm disturbances are observed, especially with the combined use of cardiac glycosides or certain antiarrhythmic drugs. In case of overdose, gastric lavage is performed, activated charcoal is used, symptomatic and supportive therapy is carried out. There is no data on the effectiveness of dialysis.
Interactions of the drug Cardosal plus
Combination of olmesartan medoxomil with hydrochlorothiazide Combinations whose use is not recommended Lithium - increases its concentration in the blood serum and increases toxicity. Combinations the use of which requires caution Baclofen - may enhance the antihypertensive effect. NSAIDs, including acetylsalicylic acid - decreased antihypertensive activity; in patients with kidney pathology, renal function may deteriorate up to the development of acute renal failure. Amifostine - may enhance the antihypertensive effect. Other antihypertensive drugs - enhance the antihypertensive effect. Alcohol, barbiturates, narcotic drugs, antidepressants - the appearance or intensification of orthostatic hypotension. Olmesartan medoxomil Use with drugs that increase the level of potassium in the blood plasma (potassium-sparing diuretics, heparin, ACE inhibitors) is not recommended - hyperkalemia may develop. With the simultaneous use of non-absorbable antacids (aluminum-magnesium hydroxide), a slight decrease in the bioavailability of olmesartan medoxomil was noted. The latter does not affect the pharmacokinetics or pharmacodynamics of warfarin or the pharmacokinetics of digoxin. The combined use of olmesartan medoxomil and pravastatin in healthy probands did not affect their pharmacokinetics. In vitro, olmesartan medoxomil does not have an inhibitory effect on cytochrome P450 enzymes. Hydrochlorothiazide Combinations whose use is not recommended Concomitant use with drugs that reduce the level of potassium in the blood (other diuretics that remove potassium from the body, laxatives, corticosteroids, ACTH, amphotericin, carbenoxolone, penicillin G sodium salt, salicylates) is not recommended - hypokalemia may develop. Combinations the use of which requires caution Calcium salts - increase the level of calcium in the blood. Cholestyramine and colestipol reduce the absorption of hydrochlorothiazide. Digitalis glycosides may cause hypokalemia and hypomagnesemia with the development of arrhythmia. Drugs whose side effects are more likely to occur with hypokalemia (class Ia and III antiarrhythmic drugs, antipsychotics, e.g. thioridazine, chlorpromazine, levomepromazine, trifluoperazine, cyamemazine, sulpiride, sultopride, amisulpride, tiapride, pimozide, haloperidol, droperidol; other drugs, e.g. bepridil , cisapride, difemanil, erythromycin for intravenous administration, halofantrine, mizolastine, pentamidine, sparfloxacin, terfenadine, vincamine for intravenous administration) - the development of severe cardiac arrhythmia, up to ventricular fibrillation, is possible. Non-depolarizing muscle relaxants (tubocurarine) - enhance the effect of muscle relaxants. Anticholinergic drugs (atropine) - increase the bioavailability of thiazide diuretics. Antidiabetic drugs (insulin and oral hypoglycemic agents) - Dosage adjustments of these drugs may be necessary due to the effect of hydrochlorothiazide on glucose tolerance. Metformin is a risk of developing lactic acidosis due to possible renal failure under the influence of hydrochlorothiazide. β-adrenergic receptor blockers and diazoxide-thiazides can enhance their hyperglycemic effect. Sympathomimetics (norepinephrine) - the effect of sympathomimetics may be reduced. Drugs for the treatment of gout (probenecid, sulfinpyrazone, allopurinol) - dose adjustment of these drugs may be required due to an increase in serum uric acid levels under the influence of hydrochlorothiazide, an increase in the frequency of hypersensitivity reactions to allopurinol under the influence of hydrochlorothiazide. Amantadine increases the risk of side effects. Cytotoxic drugs (cyclophosphamide, methotrexate) - thiazides can reduce their excretion by the kidneys and thereby increase their myelosuppressive effect. Salicylates - increasing their toxic effect on the central nervous system when used in high doses. Methyldopa - possible development of hemolytic anemia. Cyclosporine increases the risk of developing hyperuricemia and gout-like complications. Tetracyclines, including doxycycline - increases the likelihood of increased urea levels in the blood.
special instructions
When using the drug in people with impaired renal function, it is recommended to regularly monitor potassium and creatinine in the blood.
It should be remembered that an excessive decrease in pressure in patients with coronary artery disease or cerebrovascular changes can cause heart attack or stroke .
When driving a vehicle during treatment with this drug, you should be careful.