Instructions for use LOPIREL
Bleeding and hematological side effects
If hematological side effects or clinical symptoms indicating a risk of bleeding occur during treatment, it is necessary to immediately conduct a blood test (aPTT, platelet count, platelet functional activity indicators) and an assessment of the functional activity of the liver.
Like other antiplatelet drugs, clopidogrel should be used with caution in patients at increased risk of bleeding associated with trauma, surgery or other pathological conditions, as well as in the case of a combination of clopidogrel with acetylsalicylic acid, NSAIDs (including COX-inhibitors). 2), heparin, or glycoprotein IIb/IIIa inhibitors. Patients should be closely monitored for signs of bleeding, including occult bleeding, especially during the first weeks of treatment and/or after invasive cardiac procedures or surgery. The combined use of clopidogrel with oral coagulants is not recommended, since this combination may increase the intensity of bleeding.
During surgical interventions, if the antiplatelet effect is undesirable, the use of clopidogrel should be discontinued 5-7 days before surgery. Patients should inform their doctor (including dentist) about the use of the drug before upcoming surgical interventions, or if the doctor prescribes a new drug for the patient.
Clopidogrel prolongs bleeding time and should therefore be used with caution in patients at risk of bleeding (especially gastrointestinal and intraocular).
Patients should be warned that stopping bleeding that occurs during the use of clopidogrel (alone or in combination with acetylsalicylic acid) requires more time, so they should inform the doctor about each case of unusual (in terms of location and/or duration) bleeding.
Due to insufficient data, clopidogrel should not be prescribed in the acute period of ischemic stroke (in the first 7 days).
Thrombotic thrombocytopenic purpura (TTP)
Very rarely, cases of TTP characterized by thrombocytopenia and microangiopathic hemolytic anemia associated with neurological disorders, renal dysfunction or hyperthermia have been reported after the use of clopidogrel, sometimes for short periods. TTP is a life-threatening condition that requires immediate intervention, including plasmapheresis.
Lactose
The drug contains lactose, so it should not be prescribed to patients with rare hereditary disorders of galactose tolerance, lapp lactase deficiency or glucose-galactose malabsorption syndrome.
Proton pump inhibitors
Clopidogrel should not be co-administered with proton pump inhibitors, for which there is evidence that they may reduce the therapeutic efficacy of clopidogrel (omeprazole/esomeprazole). If a patient needs to take proton pump inhibitors simultaneously with clopidogrel, then only those drugs of this group that have a less pronounced potential for interaction (for example, pantoprazole) should be prescribed.
Impact on the ability to drive vehicles and operate machinery
The drug does not affect or has an insignificant effect on the ability to drive vehicles and operate machinery.
Lopirel, 75 mg, film-coated tablets, 14 pcs.
Suction
After a single dose and during a course of oral administration at a dose of 75 mg/day, clopidogrel is rapidly absorbed. The average maximum plasma concentration (Cmax) of unchanged clopidogrel is about 2.2–2.5 ng/ml and is reached approximately 45 minutes after administration. According to the excretion of clopidogrel metabolites by the kidneys, its absorption is at least 50%.
Distribution
In vitro
clopidogrel and its main inactive metabolite circulating in the blood are reversibly bound to plasma proteins by 98% and 94%, respectively.
In vitro
, this bond is unsaturable over a wide range of concentrations.
Metabolism
Clopidogrel is extensively metabolized in the liver . In vitro
and
in vivo
, clopidogrel is metabolized in two ways: the first - through esterases and subsequent hydrolysis with the formation of an inactive carboxylic acid derivative (85%) from metabolites circulating in the systemic circulation, and the second way - through the cytochrome P450 system.
Initially, clopidogrel is metabolized to 2‑oxoclopidogrel, which is an intermediate metabolite. Subsequent metabolism of 2‑oxoclopidogrel leads to the formation of the active metabolite of clopidogrel, a thiol derivative of clopidogrel. In vitro,
this metabolic pathway occurs with the participation of the isoenzymes CYP3A4, CYP2C19, CYP1A2 and CYP2B6.
in vitro
studies , rapidly and irreversibly binds to platelet receptors, thereby inhibiting platelet aggregation.
With a single dose of clopidogrel in a loading dose of 300 mg, the Cmax of the active metabolite is 2 times higher than the Cmax when taking clopidogrel in a maintenance dose of 75 mg for 4 days. Cmax of the active metabolite is reached 30–60 minutes after taking clopidogrel.
Removal
Within 120 hours after human ingestion of 14C-labeled clopidogrel, approximately 50% of the radioactivity is excreted through the kidneys and approximately 46% of the radioactivity through the intestines. After a single oral dose of 75 mg, the half-life (T1/2) of clopidogrel is about 6 hours. After a single dose and repeated doses, T1/2 of the main inactive metabolite circulating in the blood is 8 hours.
Pharmacogenetics
With the help of the CYP2C19 isoenzyme, both the active metabolite and the intermediate metabolite, 2-oxoclopidogrel, are formed. Pharmacokinetics and antiplatelet effect of the active metabolite of clopidogrel, in an ex vivo
, vary depending on the genotype of the CYP2C19 isoenzyme.
The allele of the CYP2C19*1 gene corresponds to a fully functional metabolism, while the alleles of the CYP2C19*2 and CYP2C19*3 genes are non-functional. Alleles of the CYP2C19*2 and CYP2C19*3 genes are the cause of decreased metabolism in the majority of representatives of the Caucasian (85%) and Mongoloid races (99%). Other alleles associated with absent or decreased metabolism are less common and include, but are not limited to, the CYP2C19*4, *5, *6, *7, and *8 alleles. Patients who are poor metabolizers must have the two loss-of-function gene alleles listed above. Published frequencies of CYP2C19 poor metabolizer phenotypes are 2% in Caucasians, 4% in Blacks, and 14% in Chinese.
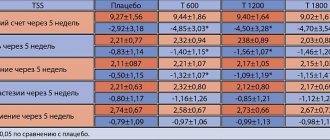
In a crossover study conducted on 40 volunteers, 10 people in each group with four subtypes of the CYP2C19 isoenzyme (ultrarapid metabolizers, extensive metabolizers, intermediate metabolizers, poor metabolizers), the pharmacokinetics and antiplatelet effect of clopidogrel at a dose of 300 mg followed by its administration were assessed. 75 mg/day and when taking clopidogrel at a dose of 600 mg followed by 150 mg/day for 5 days (reaching an equilibrium state). There were no significant differences in active metabolite exposure and mean platelet aggregation inhibition (API) (ADP-induced) values between ultrarapid, extensive, and intermediate metabolizers. In poor metabolizers, exposure to the active metabolite was reduced by 63–71% compared with extensive metabolizers. When using the 300 mg/75 mg treatment regimen in poor metabolizers, the antiplatelet effect was reduced with average IAT values of 24% (at 24 hours) and 37% (at 5 days of treatment) compared with IAT of 39% (at 24 hours). and 58% (on day 5 of treatment) in extensive metabolizers and 37% (after 24 hours) and 60% (on day 5 of treatment) in intermediate metabolizers. When poor metabolizers received the 600 mg/150 mg regimen, exposure to the active metabolite was higher than when receiving the 300 mg/75 mg regimen. In addition, the IAT was 32% (at 24 hours) and 61% (at day 5 of treatment), which was greater than that of poor metabolizers receiving the 300 mg/75 mg regimen and was similar to that in groups of patients with higher CYP2C19 intensity -metabolism, receiving a treatment regimen of 300 mg/75 mg. However, clinical outcome studies have not yet established a clopidogrel dosing regimen for patients in this group.
Consistent with the results of this study, a meta-analysis of six studies that included data from 335 volunteers treated with clopidogrel at steady state found that intermediate metabolizers reduced active metabolite exposure by 28% and poor metabolizers reduced exposure to the active metabolite by 72%. %, although IAT was reduced compared to extensive metabolizers with differences in IAT being 5.9% and 21.4%, respectively.
The effect of CYP2C19 genotype on clinical outcomes in patients treated with clopidogrel has not been assessed in prospective, randomized, controlled studies. However, few retrospective analyzes are currently available. Genotyping results are available from the following clinical studies: CURE (n=2721), CHARISMA (n=2428), CLARITY‑TIMI 28 (n=227), TRITON-TIMI 38 (n=1477) and ACTIVE-A (n=601) , as well as in several published cohort studies.
In the TRITON-TIMI 38 study and 3 cohort studies (Collet, Sibbing, Giusti), patients in the combination group who were intermediate or poor metabolizers had a higher incidence of cardiovascular events (death, myocardial infarction, and stroke) or stent thrombosis compared with those of intensive metabolizers. metabolizers.
In the CHARISMA study and one cohort study (Simon), an increase in the incidence of cardiovascular events was observed only in poor metabolizers (when compared with extensive metabolizers).
In the CURE, CLARITY, ACTIVE-A and one of the cohort studies (Trenk), there was no increase in the incidence of cardiovascular events depending on the intensity of CYP2C19 metabolism.
Clinical studies to date have not had a sufficient sample size to detect differences in clinical outcome in patients with low CYP2C19 activity.
Pharmacokinetics in special clinical situations
The pharmacokinetics of the active metabolite of clopidogrel in certain groups of patients has not been studied.
In elderly volunteers (over 75 years of age), when compared with young volunteers, there were no differences in platelet aggregation and bleeding time. No dose adjustment is required in elderly patients.
The pharmacokinetics of clopidogrel in children has not been studied.
In patients with severe kidney damage (creatinine clearance (CC) 5–15 ml/min) after repeated doses of clopidogrel at a dose of 75 mg/day, the initiation of ADP-induced platelet aggregation was lower (25%) compared with that in healthy volunteers, however the prolongation of bleeding time was similar to that in healthy volunteers receiving clopidogrel 75 mg/day. Clopidogrel was well tolerated in all patients.
In patients with severe liver damage, after daily administration of clopidogrel 75 mg/day for 10 days, the inhibition of ADP-induced platelet aggregation was similar to that in healthy volunteers. The mean bleeding time was also comparable in both groups.
The prevalence of alleles of the CYP2C9 isoenzyme genes responsible for intermediate and reduced metabolism differs among representatives of different racial groups. There is very little literature data among representatives of the Mongoloid race, which does not allow us to assess the significance of genotyping of the CYP2C19 isoenzyme for the development of ischemic complications.
Lopirel TB p/o 75 mg N 28
Description:
The tablets are pink, round, biconvex, film-coated, with an “I” engraving on one side.
1 tab.
clopidogrel hydrosulfate 97.87 mg,
corresponding clopidogrel base 75 mg
Excipients: lactose - 78.13 mg, microcrystalline cellulose - 68.75 mg, crospovidone (type A) - 13.75 mg, glyceryl dibehenate - 8.25 mg, talc - 8.25 mg, opadry II 85G34669 pink - about 8.25 mg (polyvinyl alcohol - 3.63 mg, talc - 1.65 mg, titanium dioxide (E171) - 1.63 mg, macrogol 3350 - 1.02 mg, lecithin (E322) - 0.29 mg, red iron oxide dye (E172) - 0.03 mg).
Pharmachologic effect:
Mechanism of action
Clopidogrel is a prodrug, one of whose metabolites is active and inhibits platelet aggregation. The active metabolite of clopidogrel selectively inhibits the binding of adenosine diphosphate (ADP) to the platelet P2Y12 receptor and subsequent ADP-mediated activation of the glycoprotein IIb/IIIa complex, leading to suppression of platelet aggregation. Due to irreversible binding, platelets remain immune to ADP stimulation for the remainder of their life (approximately 7-10 days), and restoration of normal platelet function occurs at a rate consistent with platelet turnover.
Platelet aggregation caused by agonists other than ADP is also inhibited by blocking enhanced platelet activation by released ADP. Because the formation of the active metabolite occurs with the help of isoenzymes of the P450 system, some of which may differ in polymorphism or may be inhibited by other drugs; not all patients have adequate inhibition of platelet aggregation.
Pharmacodynamic properties
When taking clopidogrel daily at a dose of 75 mg, from the first day of administration there is a significant suppression of ADP-induced platelet aggregation, which gradually increases over 3-7 days and then reaches a constant level (when an equilibrium state is reached). At steady state, when taking a dose of 75 mg/day, platelet aggregation is suppressed by an average of 40-60%. After discontinuation of clopidogrel, platelet aggregation and bleeding time gradually returned to baseline levels within an average of 5 days.
Clinical efficacy and safety
Clopidogrel is able to prevent the development of atherothrombosis in any localization of atherosclerotic vascular lesions, in particular in lesions of the cerebral, coronary or peripheral arteries.
The ACTIVE-A clinical trial showed that in patients with atrial fibrillation who had at least one risk factor for vascular complications but were able to take indirect anticoagulants, clopidogrel in combination with acetylsalicylic acid (compared with acetylsalicylic acid alone) reduced the combined incidence of stroke, myocardial infarction, non-CNS systemic thromboembolism, or vascular mortality, largely due to a reduction in the risk of stroke.
The effectiveness of taking clopidogrel in combination with acetylsalicylic acid was detected early and persisted for up to 5 years. The reduction in the risk of major vascular complications in the group of patients taking clopidogrel in combination with acetylsalicylic acid was mainly due to a greater reduction in the incidence of stroke. The risk of stroke of any severity was reduced when taking clopidogrel in combination with acetylsalicylic acid, and there was a trend towards a decrease in the incidence of myocardial infarction in the group treated with clopidogrel in combination with acetylsalicylic acid, but there was no difference in the incidence of non-CNS thromboembolism or vascular death. In addition, taking clopidogrel in combination with acetylsalicylic acid reduced the total number of days of hospitalization for cardiovascular reasons.
Indications:
Prevention of atherothrombotic complications
In adult patients with myocardial infarction (with a duration of several days to 35 days), ischemic stroke (with a duration of 7 days to 6 months) or with diagnosed peripheral arterial occlusive disease.
In adult patients with acute coronary syndrome:
without ST segment elevation (unstable angina or non-Q wave myocardial infarction), including patients who underwent stenting during percutaneous coronary intervention (in combination with acetylsalicylic acid);
with ST segment elevation (acute myocardial infarction) with drug treatment and the possibility of thrombolysis (in combination with acetylsalicylic acid).
Prevention of atherothrombotic and thromboembolic complications, including stroke, in atrial fibrillation (atrial fibrillation)
Patients with atrial fibrillation (atrial fibrillation) who have at least one risk factor for the development of vascular complications cannot take indirect anticoagulants and have a low risk of bleeding (in combination with acetylsalicylic acid).
Dosage regimen:
Lopirel is taken orally, regardless of meals.
Adults and elderly people with normal activity of the CYP2C19 isoenzyme
Myocardial infarction, ischemic stroke and diagnosed peripheral arterial occlusive disease
The drug is taken 75 mg 1 time/day.
Acute coronary syndrome without ST segment elevation (unstable angina, non-Q wave myocardial infarction)
Treatment with clopidogrel should be started with a single loading dose of 300 mg, then continued with a dose of 75 mg 1 time / day (in combination with acetylsalicylic acid in doses of 75-325 mg / day). Since the use of acetylsalicylic acid in higher doses is associated with an increased risk of bleeding, the recommended dose of acetylsalicylic acid for this indication should not exceed 100 mg. The optimal duration of treatment has not been formally determined.
Data from clinical studies support taking the drug for up to 12 months, with the maximum beneficial effect observed by the third month of treatment.
Acute coronary syndrome with ST segment elevation (acute myocardial infarction with ST segment elevation)
Clopidogrel should be taken once at a dose of 75 mg/day with an initial single dose of clopidogrel 300 mg in combination with acetylsalicylic acid in combination with thrombolytics or without combination with thrombolytics. In elderly patients over 75 years of age, treatment with clopidogrel should be started without taking a loading dose. Combination therapy is started as soon as possible after the onset of symptoms and continued for at least 4 weeks. The effectiveness of the combination of clopidogrel and acetylsalicylic acid in this indication for more than 4 weeks has not been studied.
Atrial fibrillation (atrial fibrillation)
Clopidogrel should be taken at a dose of 75 mg 1 time / day. In combination with clopidogrel, you should start and then continue taking acetylsalicylic acid (75-100 mg/day).
Side effect:
The safety of clopidogrel has been studied in more than 44,000 patients, incl. in more than 12,000 patients treated for a year or longer. The overall tolerability of clopidogrel was similar to that of acetylsalicylic acid, regardless of patient age, gender, and race. The following are clinically significant adverse effects observed in clinical studies: CAPRIE, CURE, CLARITY, COMMIT and ACTIVE-A. The tolerability of clopidogrel at a dose of 75 mg/day in the CAPRIE study corresponded to the tolerability of acetylsalicylic acid at a dose of 325 mg/day. Incl. Adverse reactions have been reported in spontaneous reports.
Contraindications for use:
hypersensitivity to clopidogrel or any excipient of the drug;
severe liver failure;
acute bleeding (including bleeding from a peptic ulcer or intracranial hemorrhage);
pregnancy and lactation;
children under 18 years of age (efficacy and safety of use have not been established);
rare hereditary lactose intolerance, lactase deficiency and glucose-galactose malabsorption syndrome.
Carefully:
with moderate liver failure, in which there may be a predisposition to bleeding (limited clinical experience);
for renal failure (limited clinical experience);
in case of injuries, surgical interventions (risk of increased bleeding);
for diseases in which there is a predisposition to the development of bleeding (especially gastrointestinal or intraocular);
with simultaneous administration of selective serotonin reuptake inhibitors (SSRIs);
while taking NSAIDs, incl. and selective COX-2 inhibitors;
with simultaneous administration of warfarin, heparin, glycoprotein IIb/IIIa inhibitors;
when there is a history of allergic and hematological reactions to other thienopyridines (such as ticlopidine, prasugrel) due to the possibility of cross-allergic and hematological reactions;
in patients with a genetically determined decrease in the function of the CYP2C19 isoenzyme (in patients who are weak CYP2C19 metabolizers, when clopidogrel is used in recommended doses, less of the active metabolite of clopidogrel is formed and its antiplatelet effect is less pronounced; weak metabolizers receiving clopidogrel in recommended doses in acute coronary syndrome or percutaneous coronary intervention may have a higher incidence of cardiovascular complications than patients with normal CYP2C19 function.
Use during pregnancy and breastfeeding:
As a precautionary measure, the use of Lopirel during pregnancy is contraindicated due to the lack of clinical data on its use by pregnant women, although animal studies of clopidogrel have not revealed any direct or indirect adverse effects on pregnancy, embryonic development, childbirth and postnatal development.
Breastfeeding should be discontinued when treated with Lopirel, because Studies in rats have shown that clopidogrel and/or its metabolites are excreted in breast milk. It is not known whether clopidogrel passes into human breast milk.
Use for liver dysfunction:
The drug should be used with caution in patients with moderate liver failure.
The drug is contraindicated for use in severe liver failure.
Use for renal impairment:
The drug should be used with caution in patients with moderate renal failure.
Use in children:
Contraindicated in children and adolescents under 18 years of age.
Special instructions:
Bleeding and hematological disorders
Due to the risk of bleeding and hematological undesirable effects, if clinical symptoms suspicious for bleeding appear during treatment, you should urgently do a clinical blood test, determine APTT, platelet count, indicators of platelet functional activity and conduct other necessary studies.
Clopidogrel, as well as other antiplatelet drugs, should be used with caution in patients with an increased risk of bleeding associated with trauma, surgery or other pathological conditions, as well as in patients receiving acetylsalicylic acid, other NSAIDs, incl. COX-2 inhibitors, heparin, SSRIs or glycoprotein IIb/IIIa inhibitors.
When treating with clopidogrel, especially during the first weeks of treatment and/or after invasive cardiac procedures/surgery, patients must be carefully monitored to exclude signs of bleeding, incl. hidden.
The combined use of clopidogrel with warfarin may increase the intensity of bleeding, therefore, with the exception of very rare clinical situations (such as the presence of a floating thrombus in the left ventricle, stenting in patients with atrial fibrillation), the combined use of clopidogrel and warfarin is not recommended.
If the patient is undergoing elective surgery and there is no need for an antiplatelet effect, clopidogrel should be discontinued 7 days before surgery.
Before any upcoming surgery and before starting any new drug, patients should tell their doctor (including their dentist) that they are taking clopidogrel.
Clopidogrel prolongs bleeding time, so the drug should be used with caution in patients with diseases predisposing to the development of bleeding (especially gastrointestinal and intraocular).
Patients should be warned that it may take longer to stop bleeding when taking clopidogrel (alone or in combination with acetylsalicylic acid) and that if they experience unusual bleeding (in location or duration) they should be advised talk to your doctor about this.
Thrombotic thrombocytopenic purpura
Very rarely, after the use of clopidogrel (sometimes even for a short period), cases of the development of TTP, which is characterized by thrombocytopenia and microangiopathic hemolytic anemia, accompanied by neurological disorders, renal dysfunction and fever, have been reported. TTP is a potentially life-threatening condition that requires immediate treatment, including plasmapheresis.
Acquired hemophilia
Acquired hemophilia has been reported with the use of clopidogrel. If a prolongation of the aPTT with or without the development of bleeding is confirmed, the possibility of developing acquired hemophilia should be considered. If acquired hemophilia is diagnosed, appropriate treatment should be initiated and clopidogrel should be discontinued.
Recent ischemic stroke
Taking Lopirel is not recommended for acute ischemic stroke less than 7 days old (since there is no data on its use in this condition).
In patients with recent ischemic stroke or transient ischemic attack and a high risk of recurrent atherothrombotic events, combination therapy with clopidogrel and acetylsalicylic acid has not been shown to be superior to clopidogrel monotherapy, but may increase the risk of major bleeding.
Cytochrome P450 isoenzyme CYP2C19
Pharmacogenetics: in patients with slow CYP2C19-mediated metabolism, when taking clopidogrel in recommended doses, the active metabolite of clopidogrel is formed in smaller quantities and a weaker effect on platelet aggregation is observed. Tests are available to determine the CYP2C19 genotype in patients.
Since clopidogrel is metabolized to active metabolites partly with the participation of the CYP2C19 isoenzyme, the use of drugs that inhibit the activity of this enzyme will lead to a decrease in the concentration of the active metabolite of clopidogrel. The clinical significance of this interaction is unknown.
As a precautionary measure, simultaneous use of strong and moderate inhibitors of the CYP2C19 isoenzyme is not recommended.
Cross-reactions with thienopyridines
Since hypersensitivity cross-reactions have been reported during treatment with thienopyridines, before starting treatment it is necessary to clarify the patient's history of hypersensitivity reactions to thienopyridines (clopidogrel, ticlopidine, prasugrel).
Thienopyridines may cause allergic reactions of varying severity, such as rash, angioedema or hematological cross-reactions (thrombocytopenia and neutropenia). Patients who have experienced allergic reactions and/or hematological reactions during previous treatment with one of the thienopyridines may be at increased risk of developing similar or other reactions when taking another thienopyridine. Monitoring for hypersensitivity symptoms is recommended in patients with a history of allergic reactions to thienopyridines.
Renal dysfunction
Experience with the use of clopidogrel in patients with impaired renal function is limited, so it should be used with caution in this group of patients.
Liver dysfunction
Experience in patients with moderate liver dysfunction who are at risk of developing hemorrhagic diathesis is limited. Lopirel should be used with caution in this group of patients.
Lactose content in the preparation
Lopirel should not be prescribed to patients with rare hereditary galactose intolerance, lactase deficiency and glucose-galactose malabsorption syndrome.
Impact on the ability to drive vehicles and machinery
Clopidogrel does not have a significant effect on the abilities required to drive a car or operate machinery.
Overdose:
Symptoms: an overdose of clopidogrel can lead to an increase in bleeding time with subsequent complications in the form of bleeding.
Treatment: when bleeding occurs, appropriate treatment measures are required. If rapid correction of prolonged bleeding time is necessary, platelet transfusion is recommended. No antidote for clopidogrel has been established.
Drug interactions:
Indirect anticoagulants: simultaneous use of clopidogrel and indirect anticoagulants is not recommended due to a possible increase in bleeding intensity. Although clopidogrel 75 mg/day did not affect the pharmacokinetics of S-warfarin or the INR in patients receiving long-term warfarin therapy, concomitant use of clopidogrel with warfarin increases the risk of bleeding due to an independent effect on hemostasis.
IIb/IIIa receptor blockers: the administration of IIb/IIIa receptor blockers together with clopidogrel requires caution.
Acetylsalicylic acid does not change the effect of clopidogrel, which inhibits ADP-induced platelet aggregation, but clopidogrel potentiates the effect of acetylsalicylic acid on collagen-induced platelet aggregation. However, simultaneous administration of acetylsalicylic acid with clopidogrel at a dose of 500 mg 2 times a day for 1 day did not cause a significant increase in the bleeding time caused by taking clopidogrel. There may be a pharmacodynamic interaction between clopidogrel and acetylsalicylic acid, which leads to an increased risk of bleeding. Therefore, caution should be exercised when using them simultaneously, although in clinical studies patients received combination therapy with clopidogrel and acetylsalicylic acid for up to one year.
Heparin: According to a clinical study conducted in healthy subjects, when taking clopidogrel, no change in the dose of heparin was required and its anticoagulant effect did not change. Concomitant use of heparin did not change the antiplatelet effect of clopidogrel. There may be a pharmacodynamic interaction between clopidogrel and heparin, which may increase the risk of bleeding, so the simultaneous use of these drugs requires caution.
Thrombolytics: The safety of concomitant use of clopidogrel, fibrin-specific or non-fibrin-specific thrombolytic drugs and heparin has been studied in patients with acute myocardial infarction. The incidence of clinically significant bleeding was similar to that observed in the case of combined use of thrombolytic agents and heparin with acetylsalicylic acid.
NSAIDs: In a clinical study in healthy volunteers, coadministration of clopidogrel and naproxen increased occult GI blood loss. However, due to the lack of interaction studies between clopidogrel and other NSAIDs, it is currently unknown whether there is an increased risk of gastrointestinal bleeding when clopidogrel is taken with other NSAIDs. Therefore, the prescription of NSAIDs, incl. COX-2 inhibitors should be used with caution in combination with clopidogrel.
Selective serotonin reuptake inhibitors (SSRIs): Because SSRIs affect platelet activation and increase the risk of bleeding, caution should be exercised when taking them concomitantly with clopidogrel.
Other combination therapy. Because Clopidogrel is metabolized to form an active metabolite, partly with the participation of the CYP2C19 isoenzyme; the use of drugs that inhibit this isoenzyme may lead to a decrease in the concentration of the active metabolite of clopidogrel in the blood plasma and a decrease in its clinical effectiveness. The clinical significance of this interaction is unknown. As a precaution, concomitant use of strong and moderate inhibitors of the CYP2C19 isoenzyme should be avoided.
Medicines that inhibit CYP2C19 include omeprazole and esomeprazole, fluvoxamine, fluoxetine, moclobemide, voriconazole, fluconazole, ticlopidine, ciprofloxacin, cimetidine, carbamazepine, oxcarbamazepine and chloramphenicol.
Proton pump inhibitors
When taking omeprazole at a dose of 80 mg 1 time / day together with clopidogrel or when they were taken together at an interval of less than 12 hours, the exposure to the active metabolite was reduced by 45% (loading dose) and by 40% when taking a maintenance dose. This change in values was associated with a decrease in platelet aggregation inhibition by 39% with the loading dose and by 21% with the maintenance dose. Esomeprazole is expected to have a similar interaction effect with clopidogrel. Clinical and observational studies have provided some conflicting data regarding the clinical significance of this pharmacodynamic and pharmacokinetic interaction in relation to the development of severe cardiovascular events. Due to precautionary measures, it is recommended to avoid concomitant use of omeprazole or esomeprazole with clopidogrel.
A less pronounced decrease in metabolite exposure was observed with pantoprazole or lansoprazole.
The concentration of the active metabolite was reduced by 20% when taking a loading dose and by 14% when taking a maintenance dose while taking pantoprazole 80 mg once a day. This was also accompanied by a decrease in mean platelet aggregation inhibition by 15% and 11%, respectively. These data indicate that clopidogrel can be used concomitantly with pantoprazole. There is no evidence that other drugs that reduce gastric acidity, such as histamine H2 receptor blockers (except cimetidine, which is an inhibitor of the CYP2C19 isoenzyme) or antacids, affect the antiplatelet properties of clopidogrel.
Other medicinal products: A number of clinical studies have been conducted with clopidogrel and other concomitantly prescribed drugs to examine possible pharmacodynamic and pharmacokinetic interactions. No clinically significant pharmacodynamic interactions were observed when clopidogrel was used in combination with atenolol, nifedipine, or both drugs simultaneously. In addition, the pharmacodynamic activity of clopidogrel was slightly affected by simultaneous administration of phenobarbital or estrogens.
The pharmacokinetic parameters of digoxin and theophylline did not change when they were used together with clopidogrel. Antacids did not reduce the absorption of clopidogrel.
Phenytoin and tolbutamide can be used safely concomitantly with clopidogrel (CAPRIE study), although data from studies with human liver microsomes suggest that the carboxyl metabolite of clopidogrel may inhibit the activity of cytochrome P450 isoenzyme 2C9, which may lead to increased plasma concentrations of certain drugs (phenytoin, tolbutamide and some NSAIDs), which are metabolized by the 2C9 isoenzyme of the cytochrome P450 family.
There have been no other clinical studies of the interaction of clopidogrel with drugs commonly used in patients with atherothrombotic complications. In clinical studies, no clinically significant adverse interactions were identified with ACE inhibitors, diuretics, beta-blockers, slow calcium channel blockers, lipid-lowering agents, coronary vasodilators, hypoglycemic agents (including insulin), antiepileptic drugs, hormone replacement therapy and IIb blockers /IIIa receptors.
Interaction
When combining the drug with oral anticoagulants , in particular warfarin , the likelihood and duration of bleeding may increase.
In persons with an increased risk of bleeding and taking Lopirel, it is not recommended to additionally take glycoprotein IIb/IIIa inhibitors .
It has been proven that the combination of clopidogrel and naproxen increases the risk of developing hidden gastrointestinal bleeding. However, in the case of other NSAIDs , such a pattern has not been proven. Therefore, caution should be exercised when combining these drugs.
Despite the good results of clinical studies of the interaction of the drug with heparin , caution should be exercised when taking them simultaneously.
Combining the drug with thrombolytics , since the safety of such a combination has not been clearly established.
It has been proven that daily intake of acetylsalicylic acid (up to 1000 mg per day) and clopidogrel does not affect the aggregative properties of the drug. However, the duration of co-administration of these drugs should not exceed 1 year (caution should be exercised).
The medicine can be combined with atenolol , phenobarbital , estrogens , cimetidine or nifedipine .
The drug inhibits the metabolism of drugs pharmacokinetic parameters depend on the CYP2C9 isoenzyme . In particular, the medicine may increase plasma concentrations of phenytoin and tolbutamide . You need to be careful.
It is possible to combine the drug with digoxin, theophylline, and antacids .