Nicergoline lyophilisate d/d/in 4 mg 5 ml No. 5 + solution
Compound
For 1 ampoule, active substance: nicergoline - 4.0 mg; excipients: tartaric acid - 1.04 mg, lactose monohydrate - 30.0 mg.
Pharmacokinetics
90% of nicergoline is metabolized in the liver to form two main metabolites: 1,6-dimethyl-8?-hydroxymethyl-10?-methoxyergoline (MMDL, a hydrolysis product) and 6-methyl-8?-hydroxymethyl-10?-methoxyergoline (MDL, product of demethylation under the action of the CYP2D6 isoenzyme). Nicergoline actively (>90%) binds to plasma proteins, and the degree of its affinity for β-acid glycoprotein is greater than for serum albumin. It has been shown that nicergoline and its metabolites can be distributed in blood cells. The pharmacokinetics of nicergoline is linear and does not change depending on the age of the patient. The ratio of the values of the area under the “first pass” curve. Studies confirm the absence of accumulation of other metabolites (including MMDL) in the blood. The secondary metabolic pathway produces 1-dimethylnicergoline via demethylation (1-DN), which is then metabolized by hydrolysis of the ester linkages to MDL. In patients with impaired renal function, there is a significant reduction in urinary MDL secretion. Bioavailability is about 60%. The half-life of the drug is about 2.5 hours. The half-life of the main metabolite (MDL) is 13-17 hours, and the second metabolite (MMDL) is from 2 to 4 hours. Nicergoline is excreted in the form of metabolites, mainly through the kidneys (approximately 80% of the total dose), and in a small amount (20%) through the intestines. In patients with severe renal failure, there is a significant decrease in the rate of excretion of metabolic products by the kidneys compared to patients with normal renal function.
Indications for use
Moderate cognitive impairment in elderly people with vascular pathology, including dementia.
Contraindications
Recent myocardial infarction, acute bleeding, severe bradycardia, impaired orthostatic regulation, hypersensitivity to nicergoline or other components of the drug, pregnancy, breastfeeding, children under 18 years of age (due to lack of data). With caution: history of hyperuricemia or padagra and/or in combination with drugs that interfere with the metabolism and excretion of uric acid. Simultaneous use with sympathomimetics (alpha and beta), moderate bradycardia.
Directions for use and doses
Intramuscular, intravenous, intra-arterial. Intramuscularly - 2-4 mg twice a day. 4 mg is dissolved in 2 or 4 ml of 0.9% sodium chloride solution. Intravenous drip - 4-8 mg in 100 ml of 0.9% sodium chloride solution. If necessary, you can repeat the administration during the day. Intra-arterial - 4 mg in 10 ml of 0.9% sodium chloride solution, administered slowly over at least 2 minutes. The dose, duration of therapy and route of administration depend on the nature and severity of the disease. In case of acute disorders and if it is impossible to take the drug orally, it is necessary to begin a course of treatment with parenteral administration of the drug, followed by a transition to taking the oral dosage form. For patients with impaired renal function (serum creatinine ≥ 2 mg/dL), the daily dose is reduced by 25-50%.
Storage conditions
In a place protected from light, at a temperature not exceeding 25 ° C. Keep out of the reach of children.
Best before date
3 years. Do not use after the expiration date stated on the packaging.
special instructions
After intravenous administration of nicergoline, patients are advised to remain in a horizontal position for 10-15 minutes after injection due to possible orthostatic hypotension. Clinical studies have shown that with single or repeated use of nicergoline, a decrease in systolic and, to a greater extent, diastolic blood pressure can be observed in patients with normal values and with high blood pressure. Nicergoline inhibits platelet aggregation and reduces blood viscosity. Therefore, more frequent monitoring of blood coagulation parameters is required in predisposed patients. Cases of fibrosis (eg, lung, heart, cardiac valves, and retroperitoneal fibrosis) have been identified due to ergot alkaloids, which have serotonin 5-HT2? receptor agonist activity. Symptoms of ergotism (including nausea, vomiting, diarrhea, abdominal pain, peripheral vasoconstriction) have been reported with the use of ergot alkaloids and their derivatives.
Description
Porous mass or powder, white or almost white, odorless.
Conditions for dispensing from pharmacies
On prescription
Dosage form
lyophilisate for the preparation of solution for injection
Use in children
Contraindicated in children under 18 years of age (due to lack of data).
Manufacturer and organization accepting consumer complaints
Company DEKO, LLC
Pharmacodynamics
Nicergoline is a synthetic derivative of ergot alkaloids, with an attached bromo-substituted nicotinic acid residue. Increases the speed of blood flow in the vessels of the upper and lower extremities, especially in case of circulatory disorders. Reduces platelet aggregation and improves hemorheological blood parameters. Nicergoline exhibits an alpha-1-adrenergic blocking effect, leading to improved blood flow. It has a direct activating effect on cerebral neurotransmitter systems: noradrenergic, dopaminergic, acetylcholinergic, which leads to optimization of cognitive processes.
Side effects
From the digestive system: dyspeptic symptoms (nausea, diarrhea), constipation, abdominal discomfort. From the central nervous system: dizziness, headache, psychomotor agitation, confusion, sleep disturbance (drowsiness or insomnia). From the cardiovascular system: decreased blood pressure, feeling of heat. Allergic reactions: itching, skin rash. Local reactions: with intravenous administration - phlebitis; with intramuscular injection - pain, burning, thickening at the injection site. Other: “flushes” of blood to the facial skin, nasal congestion, development of fibrosis, symptoms of ergotism: gastrointestinal disorders (nausea, vomiting, diarrhea, abdominal pain), vasoconstriction of peripheral vessels, coldness of the extremities, pain in the extremities, paresthesia, anxiety, fear , loss of consciousness, change in mood or behavior, development of seizures. It is possible to increase the concentration of uric acid in the blood, and this effect does not depend on the dose and duration of therapy.
Use during pregnancy and breastfeeding
Nicergoline is contraindicated during pregnancy. If it is necessary to use the drug during lactation, breastfeeding should be discontinued.
Interaction
Strengthens the effect of antihypertensive drugs. Nicergoline has an antagonistic effect on the vasoconstrictor effect of sympathomimetics through its alpha-adrenergic blocking effect. The possibility of interaction of nicergoline with drugs metabolized by the CYP2D6 isoenzyme cannot be excluded. When used simultaneously with acetylsalicylic acid, other antiplatelet agents and anticoagulants, bleeding time may increase. Caution should be exercised when used simultaneously with drugs that affect the metabolism of uric acid. Nicergoline potentiates the effect of beta-blockers on the heart.
Overdose
Symptoms: transient marked decrease in blood pressure. Treatment: place the patient in a horizontal position; in exceptional cases, with a sharp disruption of the blood supply to the brain and heart, it is recommended to administer sympathomimetics under constant monitoring of blood pressure.
Impact on the ability to drive vehicles and operate machinery
During the treatment period, you should refrain from driving vehicles and machinery, as well as from performing work that requires increased concentration and speed of psychomotor reaction (including driving a car).
Nicergoline in complex therapy of diffuse connective tissue diseases in children
Diffuse connective tissue diseases (DCT) and systemic vasculitis (SV) belong to a group of diseases characterized by systemic disorganization of connective tissue and varying degrees of damage to the microvasculature. According to a number of authors, microcirculation disorders in systemic lupus erythematosus (SLE) are caused mainly by productive vasculitis with the presence of spasm and impaired rheological properties of the blood, and in scleroderma (SD) - severe vascular sclerosis with spasm of arterioles and emptying of the vascular bed [1, 2]. Therefore, along with immunosuppressive therapy, the treatment regimen for patients usually includes drugs that improve microcirculation [3]. Anticoagulants and antiplatelet agents are included in the treatment program for lupus nephritis, SLE with manifestations of thrombotic angiopathy [4]. Additional administration of α-blockers, including nicergoline, is recommended for recurrent hemorrhagic vasculitis (HV) in children [5]. Traditionally, dipyridamole, pentoxifylline, vinca preparations, and calcium channel antagonists have been used in pediatric practice. All these drugs have varying degrees of influence on the state of the microvasculature and the aggregation properties of blood cells. However, the need to alternate drugs with different mechanisms of action, the need for a versatile effect on the state of both peripheral and organ microvasculature requires expanding the list of drugs in this group.
Nicergoline (Sermion)
is an alpha-adrenergic receptor antagonist and has a multifaceted effect in the body. Nicergoline increases the metabolic activity of the brain, manifested in improving memory and learning processes [7], and has a positive effect in various vascular pathologies of the brain due to its vasoactive and antiplatelet effects [8]. According to some authors, nicergoline has antiplatelet properties [9], which are comparable to those of pentoxifylline in in vivo and in vitro studies in patients with bronchial asthma [10]. Nicergoline is successfully used in the complex treatment of patients with hypertension [11]. It inhibits platelet activation and aggregation by epinephrine and other agents [12]. According to preliminary data, nicergoline reduces the concentration of metabolic products in skeletal muscles during hypoxia [13].
This study assessed the effectiveness of the use of nicergoline in complex therapy of children with various types of CTD and WS.
Purpose of the study
To evaluate the effectiveness and safety of using the drug nicergoline (Sermion) for the correction of dyscirculatory disorders in children suffering from CTD and WS.
Materials and methods
The study involved 35 children aged 5 to 15 years (27 girls and 8 boys). Of these, 6 patients were diagnosed with SLE, 17 with DM, 4 with dermatomyositis (DM), 4 with nonspecific aortoarteritis (NAA), and 4 with HV (Table 1).
The observation period was 12 weeks, during which the children continuously received nicergoline. In addition, 26 children took prednisolone or methylprednisolone, 8 took cytostatic drugs (methotrexate or cyclophosphamide), 15 took chloroquine, 4 took rumalone. At the beginning of the study, 28 children had previously received courses of various other drugs that affect microcirculation (nicotinamide, dipyridamole, pentoxifylline, acetylsalicylic acid), of which 12 patients did not take drugs from this group during the last two weeks.
Indications for the administration of nicergoline were signs of peripheral and/or visceral circulation disorders, Raynaud's syndrome, arterial (AH) and pulmonary (PH) hypertension, vasculitis. nicergoline was prescribed 10 mg twice a day.
To assess the effectiveness and safety of the drug, we used:
• clinical assessment (chillness of hands, feet, capillaritis, peripheral vasospasm, livedo, Raynaud's syndrome, acrosclerotic changes, trophic disorders; dynamics of blood pressure (BP), signs of pulmonary hypertension: shortness of breath, cough, physical changes in the lungs);
• laboratory and instrumental methods (detection of visceritis, coronaryitis, cerebrosculitis using ultrasound research methods, magnetic resonance imaging, echo and electrocardiography; determination of antibodies to cardiolipins, the state of the blood coagulation system according to coagulogram data, as well as general and biochemical tests of blood and urine );
• assessment of the state of microcirculation using bulbomicroscopy (BMS), rheovasography (RVG) and rheoencephalography (REG).
Research results
To determine the indications for the administration of nicergoline, all children were examined before the start of the study (Table 2). During a clinical and instrumental examination, a disorder of erythrocyte aggregation of varying degrees of severity and a slowdown in blood flow according to BMS data were revealed in 28 children, a decrease in blood supply to the vessels of the extremities according to the results of RVG - in 22 patients, various disorders of cerebral circulation according to REG data - in 20 patients (see. Table 3).
The effectiveness of the therapy was assessed after 2, 4, 8 and 12 weeks of continuous use of nicergoline. Clinical improvement in the vast majority of patients (23 patients) was observed by the end of 4 weeks of taking the drug. In another 11 children, a positive effect was achieved by the end of the 12th week. In one child with breastfeeding, nicergoline was discontinued due to dyspeptic symptoms (nausea, epigastric pain).
Manifestations of Raynaud's syndrome disappeared by the end of the 12th week in 4 patients, and in the remaining 2 they became less pronounced. In the majority of patients (18 patients), the manifestations of cutaneous vasculitis and peripheral blood supply disorders (chillness of the hands and feet, acrocyanosis, pallor and marbling of the skin) also decreased. In one patient with hypertension while taking nicergoline, blood pressure dropped to normal levels by the end of the first week; In another 2 patients, the drug allowed stabilization of blood pressure using additional low doses of enalapril (5 mg/day). In all patients with pulmonary hypertension, already at 2 weeks of taking nicergoline, there was a significant decrease in shortness of breath, cough, and the disappearance of physical changes in the lungs.
In two patients with SLE with signs of cerebrovasculitis, the use of nicergoline allowed for a more rapid regression of neurological symptoms (2 weeks) compared to patients who received only basic immunosuppressive therapy (on average 3–4 weeks).
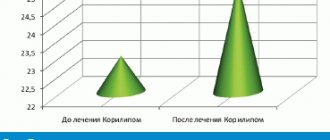
According to BMS data, in 18 children, by the end of 4 weeks of taking the drug, normalization of erythrocyte aggregation was observed (in 6 patients) or a decrease in its disturbances from grades II–III to grade I (in 12 patients). In another 9 patients, an improvement in BMS indicators was noted by the end of the observation period; in the remaining 6 patients, no significant changes were detected (Fig. 1)
After 12 weeks of taking nicergoline, an improvement in peripheral blood supply according to RVG data was noted in 17 children, and in cerebral blood supply in 18 patients.
Nicergoline was well tolerated: in only 1 patient it was discontinued due to dyspeptic disorders. Another 2 children in the first days of treatment complained of dizziness and a slight headache, which subsequently resolved on their own and did not serve as a reason to discontinue the drug. None of the patients had changes in laboratory parameters of liver and kidney function.
Thus, in the majority of patients, nicergoline had a positive effect on the rheological properties of blood and the state of microcirculation.
conclusions
Nicergoline is an effective and safe drug that has a positive effect on the microvasculature and can be recommended for use as part of complex therapy for CTD and WS in children.
Indications for the use of nicergoline in children with CTD and SV are:
• signs of damage to the peripheral microcirculatory bed (peripheral vasospasm, acrosclerotic changes, prenecrosis, trophic disorders, impaired erythrocyte aggregation according to BMS of any severity, impaired blood supply to the limb according to RVG);
• vasculitis, capillaritis;
• Raynaud's syndrome;
• antiphospholipid syndrome, hypercoagulation according to coagulogram data;
• visceral lesions of the microcirculatory bed (pneumonitis, coronaryitis, nephritis, cerebrovasculitis, etc.);
• arterial hypertension;
• pulmonary hypertension.
The list of references is on our website: www.rmj.ru
Nicergoline –
Sermion (trade name)
(Pharmacia & Upjohn)
References
1. Much E.S. Features of tissue microcirculation disorders in rheumatic main diseases // “Systemic vasculitis. Systemic lupus erythematosus.
Criteria for diagnosis and activity” (Proceedings of the symposium October 19-23, 1993), Yaroslavl, 1994; 35–6.
2. Bazhenova L.K., Tagirova R.Kh. Vascular disorders in scleroderma in children // “Modern aspects of diffuse connective tissue diseases in children” (Proceedings of the All-Union Scientific and Practical Conference, June 5-7, 1991), M., 1991; 9-10
3. Ryabova T.V. Treatment and rehabilitation of children with systemic lupus erythematosus and dermatomyositis // “Modern aspects of diffuse connective tissue diseases in children” (Proceedings of the All-Union Scientific and Practical Conference, June 5-7, 1991), M., 1991; 61–2.
4. Podchernyaeva N.S. Treatment program for clinical variants of systemic lupus erythematosus in children // - International Journal of Medical Practice, 2000; 4:11-3.
5. Lyskina G.A., Zinovyeva G.A., Kikinskaya E.G., Donov G.I. Treatment program for Henoch-Schönlein disease in children // International Journal of Medical Practice, 2000; 4:13–5.
6. Saletu V., Hochmayer I., Gronberger J., Bohmer F., Paroubek J., Wicke L., Neuhold A. Therapy of multi-infarct dementia with nicergoline: double-blind, clinical, psychometric and EEG imaging studies with 2 dosage schedules // Wien. Med. Wochenschr, 1987; 137(22):513–24.
7. Battaglia A., Broni G., Ardia A., Sacchetti G. Nicergoline in mild to moderate demencia. A multicenter, double-blind, placebo-controlled study // J. Am. Geriatr. Soc., 1989; 37 (4): 295–302.
8. Pogliani E., Recalcati P., Tantalo V., Bregnani P. Wechselwirkung zwischen Aggregationshemmem und Antikoagulantien. Eine Doppelblindstudie bei gleichzeitiger Application von Nicergolin und Acenocoumarol // Arzneimittelforschung, 1979; 29(8a): 1266–9.
9. Le-Menn R., Migne J., Prost-Dvojakovic RJ Etude ultrastructurale de l'action d'un antiaggregant sur les plaquettes sanguines. Application ala nicergoline // Therapie, 1977; 32 (2): 205–14.
10. Sidorova L.D., Domnikova N.P., Logvinenko A.S. Platelet aggregation inhibitors in the complex treatment of bronchial asthma // Klin. Medicine, 1991; 69 (11): 47–9.
11. Forette F., XVarin D., Henry JF, Hervy MP Traitment de l'hypertension arterielle du sujet age par un alpha-blocant: la nicergoline // Nouv. Presse Med., 1980; 9 (48): 3685–8.
12. Lanza F., Cazenave JP, Beretz A., Sutler-Bay A., Kretz JG, Kieny R. Potentiation by adrenaline of human platelet activation and the inhibition by the alpha-adrenergic antagonist nicergoline of platelet adhesion, secretion and aggregation / / Agents-Actions, 1986; 18 (5-6): 586–95.
13. Pastoris 0., Foppa P., Catapano M., Dossena M. Metabolite concentrations in skeletal muscle of different aged rats submitted to hypoxia and pharmacological treatment with nicergoline // Exp. Gerontol, 33(4): 303–18.
| Applications to the article |