A combined antimicrobial and anti-inflammatory drug for external use is one of the most effective for clearing acne from the skin. In just a few applications, Zinerit dries and eliminates painful rashes, allowing you to avoid subsequent troubles with scars and uneven complexion.
Composition of Zenerite
Zinerit contains two bottles with a complex of drugs and a solvent, intended for further mixing.
The first bottle of the drug complex includes 1200 mg of erythromycin and 360 mg of micronized zinc acetate dihydrate
– active ingredients.
The second bottle of solvent includes 8.36 ml of diisopropyl sebacate and 21.6 ml of ethanol - additional components.
1 milliliter of prepared lotion consists of 40 mg of erythromycin and 12 mg of micronized zinc acetate dihydrate
, as well as 250 mg of diisopropyl sebacate and 550 mg of ethanol.
Pharmacodynamics and pharmacokinetics
Zenerite is an erythromycin-zinc
a complex preparation characterized by
anti-acne effectiveness, which is manifested due to the combined effect of its active ingredients.
Effects of the antibiotic erythromycin
are aimed at suppressing the replication
of microorganisms (bacteriostatic effect) that cause acne
(
acne
):
epidermal streptococcus
(Streptococcus epidermidis) and
propionibacterium acne (Propionibacterium acne).
Zinc activity
lies in its
astringent
effect and reducing
the secretion of the sebaceous glands
(sebum).
The complex combination of all the ingredients of the drug creates good conditions for their penetration into the skin. The bulk of zinc binds to follicular epithelial cells
and does not penetrate into the systemic circulation.
A small fraction of erythromycin undergoes systemic absorption and is subsequently excreted from the human body.
Acne (acne vulgaris, acne) is one of the most common skin diseases, affecting up to 85% of people aged 12 to 24 years. In the age groups 25–34 and 35–44 years, the incidence of acne is 8 and 3%, respectively. The incidence of severe forms, according to various authors, is 5–14% of the total incidence of acne.
Acne as a skin lesion in adolescence has been known since ancient times. Until the 17th century Three terms have been used to characterize these lesions. Ionthos is a Greek word meaning “bearded” and describes the rash that appears along with the growth of a beard. The Latin word varus means “papular eruptions on the face.” The term “acne” appears to be due to a scribal error that transformed the Greek word akme (top) or achne (foam) into acne. The term “acne” was first used in literature in 542 BC. e. Aethius is the personal physician of Emperor Justinian. The Viennese physician Herba (1816–1877) associated acne with damage to the sebaceous gland (SG) in the pilosebaceous follicle (SVF) and gave a description of the process close to modern ones.
Pathogenesis of acne
Most SGs are structurally associated with hair follicles of long, bristly or vellus hair. Depending on the type of hair and the size of the SF flowing into its follicle, it is customary to distinguish three types of SVF. The first is represented by terminal hair and large SGs (involved in the pathological process in hidradenitis). SVF of the second type - vellus hair - has tiny hair, a large excretory opening and disproportionately large SGs. The third type of SVF, which is involved in the pathological process in acne to the greatest extent, consists of rudimentary hair, which practically does not come to the surface of the skin, and large multi-lobed SGs.
SF flow into the follicular canal at a certain level, due to which the SVF duct is usually divided into two parts - acro- and infrainfundibulum. The epithelium of the upper part, like the epidermis, is keratinized, and the longer lower part of the duct (4/5 of the length), like the SG ducts, is lined with multilayered squamous non-keratinizing epithelium. Normally, the cohesion of cells in it is low, and they are quickly washed away by sebum onto the surface of the epidermis.
In the pathogenesis of acne, leading importance is given to four factors (see figure). The initial link is hereditarily caused hyperandrogenism (HA), which can manifest itself in the form of an absolute increase in the amount of hormones (absolute GA) or increased sensitivity of receptors to a normal or reduced amount of androgens in the body (relative GA).
The onset of functioning in puberty of the hypothalamus–pituitary–gonadal system is characterized by a sharp increase in the synthesis of testosterone, the main steroid of the testes. The formation of estrogens (mainly estradiol) begins in the ovaries, the immediate precursor of which is androstenedione, the main androgen of the ovaries.
A certain contribution to the synthesis of androgens in the body (especially in women) is made by the adrenal cortex. Its zona reticularis produces the main androgen precursor, dehydroepiandrosterone, which, after isomerization to androstenedione, is reduced to testosterone. The production of androgens in the adrenal glands increases markedly if the biosynthesis of glucocorticoids is disrupted due to a deficiency of one of the hydroxylases (adrenogenital syndrome).
Hyperandrogenism of gonadal origin is possible with excessive stimulation of the gonads by luteinizing hormone of the pituitary gland, with tumor degeneration of androgen-producing cells (Leydig in the testes and theca cells in the ovaries) or with a deficiency of enzymes that catalyze the transition of testosterone to estradiol. The main part of testosterone (97–99%) circulating in the blood is in a bound state (with sex hormone binding globulin - SHBG).
Conditions of relative GA are more common with normal or reduced levels of androgens in the body. In SG cells - sebocytes - testosterone under the action of the enzyme 5α-reductase type 1 is converted into a more active metabolite - dihydrotestosterone, which is a direct stimulator of the growth and maturation of sebocytes, the formation of sebum. The main causes of relative GA are increased activity of 5α-reductase type 1, increased density of nuclear receptors for dehydrotestosterone, or an increase in the free fraction of testosterone in the blood as a result of decreased synthesis of SHBG in the liver. Thus, the changes in hormonal levels noted above lead to an increase in the size of the SG and their increased functioning.
The key element in the pathogenesis of acne is follicular hyperkeratosis. In the increased volume of sebum, the concentration of essential α-linolenic (cis-9,12,15-octadecatrienoic) acid (LA) decreases. Its deficiency may be due to both a deficiency in food and a deficiency of enzymatic systems that ensure the entry of LA into the body and distribution in it. By suppressing the expression of the transglutaminase enzyme, LA is the main regulator of keratinocyte differentiation. Transglutaminase is involved in the synthesis of keratin 1 and 10 fractions, proteins involucrin, loricrin and fillagrin - the main components of the cementing intercellular substance of corneocytes. Increased transglutaminase activity causes retention hyperkeratosis in the infrainfundibulum of the SVF. The predominance of the processes of proliferation and dyskeratosis over desquamation of the epithelium ultimately leads to the closure of the SVF duct. If obstruction predominates in the acroinfundibulum, an open comedon is formed, the black color of which is due to the oxidation products of sebum lipids, mainly squalene, and not melanin, as previously thought. Obturation in the infrainfundibulum area of the SVF leads to the formation of a closed comedon. Obstruction of the SVF duct by comedones creates favorable anaerobic conditions for the proliferation of facultative anaerobes Propionibacterium acnes and Propionibacterium granulosum.
The SVF duct is inhabited by aerobic staphylococcus and micrococci, facultative anaerobes P. acnes and P. granulosum. Anaerobic conditions in the infrainfundibulum of the SVF are unacceptable for aerobic bacteria, therefore staphylococcus and micrococci are localized in the acroinfundibulum and do not play a significant role in the pathogenesis of acne, unlike P. acnes [4].
The density of skin colonization with P. acnes changes with age, reaching a maximum during puberty. The highest density of P. acnes is observed in seborrheic areas, since sebum is a breeding ground for these microorganisms.
It has been established that P. acnes has a direct and indirect effect on the occurrence of both non-inflammatory (open and closed comedones) and inflammatory acne (papules, pustules, nodules). Extracellular lipase of microorganisms hydrolyzes sebum triglycerides to glycerol, which is a nutrient substrate for microorganisms, and free fatty acids, which have comedogenic properties.
Pro-inflammatory factors, such as interleukins (IL) 1a, 1b and 8, tumor necrosis factor a, acting on the SVF wall, activate keratinization processes, making a significant contribution to the implementation of the second factor in the pathogenesis of acne - follicular hyperkeratosis. The concentration of IL-1a in the area of open comedones is 1000 times higher than that in areas of healthy skin [4, 5].
IL-1a activates hyperkeratotic processes by directly stimulating receptors on keratinocytes and increasing the release of other bioactive molecules, such as vascular endothelial growth factor and retinoic acid binding protein. In addition, P. acnes has been shown to produce vasoactive amines similar to histamine, which increase inflammation.
Pro-inflammatory cytokines activate the enzyme cyclooxygenase, as a result of which the main inflammatory mediator, leukotriene B4, is formed from arachidonic acid, which stimulates Langerhans cells, neutrophils, T-lymphocytes, monocytes and eosinophils with their subsequent release of hydrolytic enzymes and nitric oxide. Destruction of the SG wall with the release of its contents into the dermis causes a picture of inflammation, which manifests itself in the form of papules, pustules, nodules and cysts.
Clinical picture of acne
Acne rashes are represented by a pseudopolymorphic rash, which is characterized by a clear stage in the evolution of elements. Initial skin changes in acne are represented by open or closed (according to the level of obstruction of the SVF duct) comedones. A comedon is a “cast” of the SVF duct, consisting of rejected corneocytes and microorganisms glued together with sebum. Open comedones, unlike closed comedones, resolve spontaneously and without a trace in approximately 80% of cases. The addition of an inflammatory reaction around the comedone leads to its destruction and the subsequent formation of papules and then pustules. The development of an inflammatory reaction in the dermis leads to the formation of nodes, and when they suppurate, cysts. The resolution of comedones, papules and pustules occurs without a trace. Nodules and cysts leave behind foci of dyspigmentation and, depending on the fibroplastic response of the skin, hypotrophic (ice-pick), hypertrophic or keloid scars. True acne must be differentiated from acne-like rashes based on the signs presented in table. 1.
To assess the severity of acne in practical conditions, the most convenient classification is proposed by the American Academy of Dermatology (in our modification):
- I degree is characterized by the presence of comedones (open and closed) and up to 10 papules;
- II degree – comedones, papules, up to 5 pustules;
- III degree – comedones, papulopustular rash, up to 5 nodes;
- IV degree is characterized by a pronounced inflammatory reaction in the deep layers of the dermis with the formation of multiple painful nodes and cysts; the severity of skin lesions was within grades II and III.
Acne treatment
To cope with grade I acne and prevent further transformation of comedones into inflammatory elements, it is often sufficient to prescribe medicinal cosmetics that provide both regression of acne elements and skin care. For more severe forms of acne, a properly selected range of medicinal cosmetics used during drug therapy, as well as after its completion, can reduce the treatment time and achieve consolidation of the results of anti-acne treatment.
Anti-acne agents used today include both systemic and local drugs. The choice of treatment method should be determined by the severity and distribution of the rash (face, torso).
A fairly large group of products is represented by retinoids for local and systemic use. Retinoids are any agents capable of inducing specific biological responses by binding and activating retinoic acid receptors. Based on their chemical structure, all retinoids are divided into four groups, or generations. In the treatment of acne, first-generation retinoids are used - derivatives of retinoic acid (retinol, tretinoin, isotretinoin) and retinoid-like compounds (fourth generation retinoids) for local therapy - adapalene, a derivative of naphthoic acid. The therapeutic effectiveness of retinoids is associated with the activation of retinoid-sensitive receptors of type g, localized in the SVF duct, which leads to a decrease in the cohesion of keratinocytes and accelerates their desquamation, i.e., an anti-comedogenic effect is realized.
Benzoyl peroxide (BP) preparations have antimicrobial, anti-inflammatory and comedolytic activity. Being a powerful oxidizing agent, BP, in contact with the cell membrane of bacteria, has a bactericidal effect. Benzoic acid formed during the destruction of BP acts bacteriostatically. Benzoic acid does not accumulate in tissues, does not have a systemic effect and is quickly excreted unchanged in the urine. The anti-inflammatory effect of BP consists of the inactivation of free radical oxygen species at the site of inflammation and the destruction of free fatty acids (a 50% reduction in the amount within 15 days). The comedolytic effect is explained by the fact that BP, by its chemical structure, is a peroxide (i.e., a strong oxidizing agent), which destroys the structures of the comedones. Preparations based on BP effectively act on P. acnes and other microorganisms without the development of microbial resistance, which allows them to be used for a long time.
Based on the etiopathogenesis of acne, for the treatment of this disease in women, substances that have a suppressive effect on the GA state, i.e., antiandrogens, seem to be adequate and pathogenetically substantiated means.
Among the drugs that affect the severity of androgenization, combined oral contraceptives (COCs) are the most widely used. Taking into account the anti-acne effect in dermatological practice, preference among COCs is given to monophasic low-dose drugs that include a gestogen with antiandrogenic activity. COCs containing 0.035 mg ethinyl estradiol and 2 mg cyproterone acetate or 0.03 mg ethinyl estradiol and 3 mg drospirenone meet these requirements.
The anti-acne effect of COCs is complex. Firstly, exogenously administered ethinyl estradiol and gestogen through a negative feedback mechanism, suppressing the production of follicle-stimulating and luteinizing hormones by the pituitary gland, reduce the synthesis in the ovaries of both estrogens and progesterone, and their precursors - androgens. Secondly, ethinyl estradiol increases the production of SHBG in the liver, with which it binds (i.e. is in an inactive state) up to 99% of androgens.
Exacerbation of acne in the second half of the menstrual cycle is caused, on the one hand, by increased stimulation of the androgen receptors of the SVF by progesterone and androgens, and on the other hand, by perifollicular edema, which aggravates the obstruction of the SVF duct. A significant increase in the amount of estrogen in the second phase of the cycle stimulates the synthesis of angiotensinogen (the precursor of angiotensin II) in the liver, which in turn induces the production of aldosterone by the adrenal glands.
Azelaic acid (15% gel, 20% cream) has a comedolytic, antibacterial and anti-inflammatory effect, which is applied to a previously cleansed face with acne severity I–II twice a day for at least six months.
Antibiotics have pronounced antimicrobial and anti-inflammatory effects in acne. As monotherapy and in combination with other anti-acne drugs, systemic antibiotics for grades II–IV of the process (especially when the rash is localized other than the face on the torso) are used for three to six months. The most common among them are: doxycycline (100 mg 2 times a day), tetracycline (500 mg 2 times a day), clindamycin (150–300 mg 3 times a day) and erythromycin (500 mg 2 times a day) [2, 7, 9]. In Europe, minocycline (100 mg/day) is widely used, which is one of the most effective antibiotics for acne, associated with a minimal risk of developing resistance to it and the development of adverse reactions (disorders from the gastrointestinal tract, vaginal candidiasis, etc.). Less commonly, sulfonamides are used as antimicrobial agents (co-trimoxazole - 480 mg 2 times a day) [1, 5, 6].
Among local antibacterial agents, erythromycin (Zinerit) and clindamycin (Dalacin-T) preparations deserve attention. Local antibacterial drugs are used for acne of II–III severity, both as monotherapy and in combination with topical retinoids for at least 3 months.
The main adverse reaction during long-term antibiotic therapy for acne is gram-negative folliculitis (GNF). Type 1 GNF is characterized by a rash grouped in the perioral and perinasal areas (but other localization is also possible) in the form of pustules with whitish contents, surrounded by a narrow rim of hyperemia; type 2 GNF is characterized by a papular-nodular rash, from which microorganisms of the genus Proteus are inoculated. Etiopathogenetically, the basis of GNF is a violation of the bacterial biocenosis in the SVF. Long-term use of antibiotics suppresses the vital activity of the gram-positive saprophytic flora of the skin, which inhibits the growth of gram-negative microorganisms [3, 8].
Slower healing of inflammatory acne is due to the presence of inflammatory mediators synthesized by P. acnes, the expressed resistance of P. acnes to destruction by neutrophils and monocytes, and the persistence of P. acnes (phagocytosed bacteria remain viable for a long time, despite the antimicrobial effect). In addition, hypersecretion of sebum does not allow creating the necessary concentration of the antibiotic in the ducts of the gastrointestinal tract. Therefore, to reduce the mass of P. acnes in spill elements by 10% of their initial amount, at least a three-week treatment period is required.
Among the antibiotics recommended for the treatment of acne presented on the domestic pharmaceutical market, we focused on a drug for external use - Zenerit lotion (Astellas Pharma, the Netherlands), which is a combination of erythromycin (4%) and zinc acetate (1.2%).
Zinerit lotion is available without a prescription. Using an applicator, it is applied in a thin layer to the acne-affected area of the skin. To do this, tilt the bottle down with light pressure. The application speed can be adjusted by the pressure applied by the applicator. An approximate single dose is 0.5 ml, in a bottle – 30 ml. After drying, the solution becomes transparent and leaves no marks on the skin or clothing. Zinerit must be used 2 times a day, the average duration of treatment is 10–12 weeks. Zinerit can be combined with other local and systemic anti-acne drugs.
The pronounced anti-acne effect of Zinerit lotion is explained by its reaction to all parts of the pathogenesis of acne. Erythromycin binds to the 50S ribosomal subunit, which is found only in bacteria, which leads to disruption of protein synthesis and stops the growth of microorganisms. An important effect of erythromycin on acne is its effect on P. acnes. The concentration of erythromycin (4%) promotes optimal penetration of the drug into the skin. By reducing microbial contamination, erythromycin eliminates or sharply weakens both follicular hyperkeratosis and the inflammatory response.
Zinc, which is part of Zinerit, inhibits 5α-reductase type 1, thereby preventing the transformation of testosterone into DTS and, as a result, weakens the initial factor in the pathogenesis of acne - androgen-induced hypersecretion of sebum. In addition, zinc has an anti-inflammatory and antiseptic effect and promotes epithelization.
The purpose of our work was to evaluate the anti-acne effectiveness and tolerability of Zinerit lotion, used as monotherapy in men and women with acne of II and III severity, as well as in combination with COCs in women with acne of III severity.
5 men and 9 women with acne of II severity and 12 men and 10 women with acne of III severity received monotherapy with Zenerit lotion for 3 months. During the first three months of treatment, 27 women with grade III acne who were prescribed systemic anti-acne therapy in the form of COCs (0.035 mg ethinyl estradiol and 2 mg cyproterone acetate) for a period of 6 months were also prescribed local anti-acne therapy with Zinerit lotion.
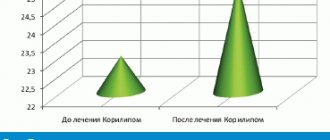
The dynamics of the number of open and closed comedones, papules and pustules was assessed before the start of treatment, after 1, 2 and 3 months of therapy. Before the start of treatment and after 3 months, along with counting acne elements, the level of sebum secretion (USS) was determined using the Sebumeter SM 810 device (Courage + Khazaka electronic GmbH, Germany), the operating principle of which is based on the quantitative determination of sebum by photometry. The normal level of USCS is 60–90 and 10-6 g/cm2.
After three months of treatment, a more pronounced anti-acne effect was observed in patients receiving COCs in combination with Zinerit lotion. By the end of the course of monotherapy with Zinerit lotion, a state of clinical cure was recorded in 28.6 and 31.8% of patients with acne of II and III severity, respectively. In patients with grade III acne who received COCs in combination with Zinerit lotion, clinical cure was observed in 48.2% of cases (Table 2).
During the first half of the course of treatment, in the first two groups of patients receiving monotherapy with Zinerit lotion, there was a more pronounced regression of pustules (by 81.6%) and open comedones (by 64.5%) than during the second half of the course. During the second half of the course of therapy (compared to the first), more pronounced dynamics were noted in the regression of closed comedones (by 75.3%) and papules (by 74.2%). During the first half of the course of therapy, the degree of regression of these elements was 50.3 and 46.5%, respectively.
In patients of the third group who received COCs in combination with Zinerit lotion, during the first and second half of the treatment period there was a more pronounced regression of inflammatory elements (by 62.8 and 64.2%) compared to non-inflammatory elements (by 48.6 and 56. 6%). The dynamics of regression of open comedones, papules and nodes was approximately the same during the first and second half of the treatment period. During the second half of the course of therapy, the dynamics of regression of pustules was ahead of that during the first half of the course (86.0 compared to 76.7%).
SVR (10-6 g/cm2) before treatment and after 3 months of therapy was respectively: 212 ± 25 and 163 ± 12.3 – in patients of the first group, 226 ± 28.3 and 142 ± 18.1 – in patients of the second group and 241 ± 35 and 108 ± 12.8 – in women of the third group.
Treatment with Zinerit lotion was well tolerated in all patients. Four patients from the third group during the first week from the start of treatment noted slight dry skin after applying the drug. Additionally, they were recommended moisturizing medicinal cosmetics, which allowed them to eliminate the phenomenon of dryness within three to five days.
Thus, taking into account the effect of Zinerit lotion on all parts of the pathogenesis of acne, as well as the results of our own observations on the effectiveness of therapy with this drug, Zinerit lotion can be recommended as a first-line treatment for up to three months for patients with acne of degrees II and III with pronounced inflammatory changes . Women with acne of III severity when the process is localized on the face and torso should be prescribed combination therapy with Zinerit lotion and COC containing 0.035 mg of ethinyl estradiol and 2 mg of cyproterone acetate.
Zinerit, instructions for use
To use Zinerit correctly, you should mix the complex preparation
and
solvent
, which are in different bottles to extend the shelf life of the drug. Before mixing both components of the future lotion, you need to make sure that the shelf life of the drug and the integrity of both bottles correspond. Below are recommendations on how to make a Zenerit solution for acne at home, suitable for further direct use.
Preparation of lotion:
· first of all, you need to unscrew the caps (lids) from both bottles and at the same time keep the cap from the bottle with the complex of drugs;
· pour out the solvent
into a bottle of
powder
and screw the lid tightly on;
· immediately and thoroughly shake the mixture (for 60 seconds);
· remove the cap;
· remove the applicator
;
· insert applicator
into the neck of the lotion bottle and screw on the cap.
The solution prepared in this way is ready for use and can be stored at a temperature of 15-20°C for 5 weeks. To control the expiration date, you can write the date of manufacture on the lotion bottle.
Further instructions for the use of Zinerit involve its external application only. After unscrewing the cap from the bottle with the prepared lotion, you need to attach the applicator
to the affected areas of the skin and apply the drug in a thin layer, lightly pressing on the base of the inclined bottle.
Applications
made to previously cleaned areas of the skin with a frequency of 2 times every 24 hours (morning and evening).
The speed of application
depends on the force of pressure on the base of the bottle. The average single dose is 0.5 ml. The duration of the full treatment course can reach 10-12 weeks.
Photos before and after using Zenerit for 10 weeks:
The data on whether Zinerit helps against acne in a shorter period of use is purely individual. In some cases, an improvement in the condition of the patient's skin was observed after only 14 days of using the drug.
Note!
The description of the drug Zinerit on this page is a simplified author’s version of the apteka911 website, created on the basis of the instructions for use.
Before purchasing or using the drug, you should consult your doctor and read the manufacturer's original instructions (attached to each package of the drug). Information about the drug is provided for informational purposes only and should not be used as a guide to self-medication. Only a doctor can decide to prescribe the drug, as well as determine the dose and methods of its use.
special instructions
After applying the drug to the skin and completely drying, the lotion becomes invisible.
With long-term use of Zenerit, it is theoretically possible to develop cross-resistance
in relation to other
macrolides
,
Clindamycin
and
Lincomycin
.
When carrying out applications
precautions should be taken to prevent application of the drug to
the mucous membranes of the eyes
,
nose and mouth
, in order to avoid
irritation
and/or
burns
.