Anticholinergics (anticholinergics) are medications that block different types of cholinergic receptors in organs and tissues, preventing the effects of a natural biologically active substance - the mediator acetylcholine.
Acetylcholine is a transmitter of impulses in the peripheral nervous system, regulating the functioning of many internal organs and systems (in particular, the brain, heart, bronchi, uterus, gastrointestinal tract, urinary system, etc.).
Acetylcholine realizes its effects by interacting with special structural components of cells - receptors, namely cholinergic receptors. Depending on their location and functions, adrenergic receptors are classified into M- and N-cholinergic receptors.
M-cholinergic receptors are located mainly in the brain, heart, bronchi, gastrointestinal tract, iris, and urinary tract. The effects of M-cholinergic receptor stimulation include pupil constriction, decreased intraocular pressure, increased gastric acid production, increased secretion of digestive glands, increased gastrointestinal motility and peristalsis, increased bladder tone, and decreased heart rate.
N-cholinergic receptors are localized mainly in skeletal muscles, as well as in special structures - autonomic ganglia and carotid glomeruli. When they are stimulated, muscle contraction, vasoconstriction (and, as a consequence, increased blood pressure) and stimulation of the respiratory center in the brain are observed.
There is a separate class of drugs that can stimulate cholinergic receptors (cholinomimetics, anticholinergics), and a group of drugs that can block cholinergic receptors (cholinergic blockers, anticholinergics).
Depending on the type of receptors blocked, anticholinergics are divided into M-anticholinergics, as well as N-anticholinergics (which, in turn, are divided into two separate classes: ganglion blockers and muscle relaxants). Let us consider in detail drugs that block M-cholinergic receptors.
What are M-anticholinergics?
M-anticholinergics are a group of drugs that are actively used in gastroenterology and other areas of medicine to improve the condition of patients and stop the progression of gastrointestinal diseases.
Medicines help relax the smooth muscles of the digestive tract and significantly shorten the recovery period for acute disorders. The drugs are used quite often, they are combined with other drugs to ensure maximum therapeutic effect.
Mechanism of action
M-anticholinergics (indications for use are not the only reason for prescribing medications, therefore a preliminary examination is carried out before treatment) act due to the content of components that can have a relaxing effect on the muscle fibers present in the walls of the digestive tract.
Due to this, the following is achieved:
- relaxing effect;
- suppression of the functioning of the digestive glands is observed;
- decreased production of hydrochloric acid.
Against this background, there has been a significant improvement in the condition of patients suffering from chronic severe diseases of the stomach, duodenum and intestines.
As a result of the course use of medications in combination with other drugs, there is a reduction in the recovery period and a gradual restoration of the mucous membranes of the digestive tract. Thanks to the unique protective layer that forms on the walls of organs, tissue restoration occurs.
Often with gastritis and peptic ulcers, ulcerations form on the walls of the stomach. The products help speed up their healing and prevent further tissue destruction and the development of peritonitis.
M-anticholinergics. Mechanism of action
Drugs from the group of M-anticholinergics additionally have other properties:
- They somewhat suppress the activity of the sweat glands, which reduces sweating in various disorders.
- They weaken the tonic effect of the central nervous system on internal organs.
- When taken in high doses, the heart rate increases; when taken in moderate doses, it leads to a decrease in heart rate.
- They affect the process of blood filtration in the kidneys, reducing daily diuresis.
- They suppress the patient’s activity, which is especially important during psycho-emotional arousal.
- They dilate the bronchi and help to slightly reduce the secretion of sputum, which alleviates the condition of patients with chronic diseases of the respiratory system.
- Reduce the toxic effect of certain drugs on the central nervous system.
Due to the versatility of drugs, they can be used not only in gastroenterology, but also in the treatment of pathologies of the eyes, heart, and respiratory system.
M-CHOLINOBLOCKERS (DRUGS) OF CENTRAL AND PERIPHERAL ACTION.
M-CHOLINOMIMETICS.
Localization of M-cholinergic receptors - M-cholinergic receptors are located in the postsynaptic membrane of cells of effector organs at the endings of postganglionic cholinergic (parasympathetic) fibers. In addition, they are present on neurons of the autonomic ganglia (localized outside the synapses) and in the central nervous system (in the cerebral cortex, reticular formation). There are m1-cholinergic receptors (in the autonomic ganglia and in the central nervous system), m2-cholinergic receptors (the main subtype of m-cholinergic receptors in the heart) and m3-cholinergic receptors (in smooth muscles, most exocrine glands), m4-cholinergic receptors (in the heart, the wall of the pulmonary alveoli, CNS) and m5-cholinergic receptors (in the central nervous system, in the salivary glands, iris, in mononuclear blood cells).
Drugs that excite them —
Pilocarpine hydrochloride, Aceclidine
The mechanism of action is a direct stimulating effect on m-cholinergic receptors.
Pharmacological effects:
1. Eye: contraction of the m.constrictorpupillae, constriction of the pupil (miosis), opening of the angle of the anterior chamber of the eye, improved outflow of fluid into Schlemm’s canal, contraction of the ciliary muscle and improved outflow of intraocular fluid through the trabecular meshwork, increased curvature of the lens (near focus)
2. Effect on the cardiovascular system: decrease in heart rate, decrease in atrioventricular conduction, decrease in the force of heart contractions, peripheral vasodilation (mediated through extrasynaptic M-Chr and NO release)
3. Gastrointestinal tract: increased tone and amplitude of intestinal contraction
4. Bladder: contraction of the detrusor, decrease in bladder capacity.
5. Uterus: in humans, it is not sensitive to M-agonists.
6. Respiratory system: contraction of the muscles of the bronchial tree, increased secretion of the bronchial glands
7. CNS: Parkinson-like effects.
Indications for use—
Pilocarpine is widely used in ophthalmological practice to lower intraocular pressure in glaucoma, as well as to improve eye trophism in cases of thrombosis of the central retinal vein, acute retinal artery obstruction, optic nerve atrophy, and vitreous hemorrhages.
Aceclidine is a drug that prevents and eliminates atony of the bladder, especially with an increase in the amount of urine associated with neurogenic disorders of the bladder, with atony of the muscles of the gastrointestinal tract, as well as with decreased tone and subinvolution of the uterus, to stop bleeding in the postpartum period. Aceclidine solutions are used to narrow the pupil and reduce intraocular pressure in glaucoma.
Contraindications to the use of certain drugs –
PILOCARPINE Hypersensitivity, iritis, cyclitis, iridocyclitis, keratitis, condition after ophthalmological operations and other eye diseases in which constriction of the pupil is undesirable
ACECLIDINE for bronchial asthma, severe heart disease, angina pectoris, bleeding from the gastrointestinal tract, epilepsy, hyperkinesis, during pregnancy (if the drug is not prescribed to increase the tone of the uterine muscles), as well as for inflammatory processes in the abdominal cavity before surgery.
Symptoms of muscarine poisoning are excessive salivation, profuse sweating, facial flushing, nausea, vomiting, abdominal pain, diarrhea. The pupils are constricted, vision is unclear due to a spasm of accommodation. As poisoning progresses, the following may be observed: heart rhythm disturbances, a significant decrease in blood pressure up to collapse. Due to spasm of the bronchi and increased secretion of the bronchial glands, breathing is difficult, superficial, cyanosis and convulsions are observed. Death occurs due to asphyxia.
Helpful measures - The antidote therapy is atropine sulfate, which is injected subcutaneously in the form of 1 ml of a 0.1% solution repeatedly (at 10-minute intervals), up to 3 times (if indicated). In severe cases, the drug can be administered intravenously slowly. If poison gets inside, the stomach is washed with a suspension of activated carbon, a 0.1% solution of potassium permanganate, followed by the introduction of a suspension of activated carbon and a saline laxative. A high enema is prescribed. In case of asphyxia - artificial ventilation, resuscitation measures. In case of circulatory disorders, camphor, cordiamine, caffeine-sodium benzoate are injected under the skin.
ANTICHOLINESTERASE DRUGS.
Classification of drugs by mechanism of action.
I. Reversible drugs - Physostigmine salicylate Proserin Galantamine hydrobromide
II. Irreversible drugs Armin
Pharmacological effects:
1) CNS: low doses - diffuse EEG activation, psychostimulation, high doses - generalized convulsions, coma, respiratory arrest.
2) Eye, gastrointestinal tract, MPS, breathing: effects of parasympathetic stimulation (miosis, lacrimalization, salivation, intestinal spasms, vomiting, diarrhea, frequent urination, bronchospasm, hypersecretion)
3) CVS: medium doses – moderate bradycardia and decreased cardiac output, high doses – bradycardia, decreased blood pressure
4) Skin – increased sweating
5) Skeletal muscles - fasciculation, weakness, depolarization block, paralysis.
Indications for use: myasthenic syndrome, postoperative intestinal atony, atonic constipation, disorders of bladder emptying after gynecological operations and childbirth, elimination of the effect of non-depolarizing curare-like drugs, peripheral paralysis of striated muscles, poliomyelitis, encephalitis, weakness of labor, optic nerve atrophy, for constriction of the pupil and decreased intraocular pressure in open-angle glaucoma.
Contraindications for use: mechanical obstruction of the intestines or urinary tract, bronchial asthma, hypersensitivity to anticholinesterase drugs, epilepsy, angina pectoris, atherosclerosis
Symptoms of poisoning with drugs of the FOS group
stimulation of M-cholinergic receptors (miosis, salivation, sweating, vomiting, diarrhea). The greatest threat is bronchospasm with pulmonary edema.
Help measures.
First of all, FOS should be removed from the injection sites. If it is the skin or mucous membranes, they must be thoroughly washed with a 3-5% sodium bicarbonate solution. If substances enter the digestive tract, the stomach is washed, adsorbents and laxatives are given, and high siphon enemas are prescribed. These activities are carried out repeatedly until the pronounced manifestations of intoxication disappear. If FOS enter the blood, their excretion in the urine should be accelerated (using forced diuresis). Effective methods of purifying blood from FOS are hemosorption, hemodialysis and peritoneal dialysis. An important component of the treatment of acute OP poisoning is the use of m-anticholinergics (atropine and atropine-like drugs). In addition, symptomatic therapy should be carried out. It is necessary to constantly monitor the patient's breathing. Considering that OPs cause hypersecretion of the glands, oral hygiene should be performed and secretions should be removed from the trachea and bronchi. If necessary, assisted or artificial respiration is used. In case of psychomotor agitation, chlorpromazine, diazepam, sodium hydroxybutyrate and other drugs of a depressant type are administered.
M-CHOLINOBLOCKERS (DRUGS) OF CENTRAL AND PERIPHERAL ACTION.
Mechanism of action: blockade of M-Chr. A classic example is atropine: it blocks muscarinic receptors of all types, removes the tonic effect of the central nervous system on internal organs, competitive blockade by atropine is removed by increasing the concentration of ACh or muscarinic agonists, prevents the formation of IP3 in M1- and M3-Chr or reduces the level of cAMP in M2-Chr.
Pharmacological effects of atropine:
1) Skin: blockage of sweating, dry skin, possible hyperpyrexia, hyperemia
2) Vision: cycloplegia (relaxation of the ciliary muscle), mydriasis (relaxation of the muscle that constricts the pupil), difficulty in the outflow of fluid (increased intraocular pressure), decreased lacrimalization (lacrimation)
3) Gastrointestinal tract: hyposalivation, decreased tone and motility of the gastrointestinal tract, vagal secretion of the stomach, pancreas, intestines, bile.
4) MPS: urinary retention, relaxation of the ureters.
5) Respiratory system: dilation of the bronchi, decreased secretion of the bronchial glands.
6) Cardiovascular system: bradycardia in low doses (effects on the vagal centers), tachycardia in high doses (peripheral effects), increased cardiac output
7) CNS: in therapeutic doses there is a weak stimulating effect on the central nervous system, in toxic doses - hallucinations, coma.
Other M-anticholinergics in comparison with it. If atropine has a stronger effect on the heart, bronchi, and digestive tract, then scopolamine has a stronger effect on the eyes and the secretion of a number of excretory glands. Scopolamine has a shorter duration of action than atropine.
Scopolamine differs significantly from atropine in its effect on the central nervous system. At therapeutic doses, scopolamine usually causes sedation, drowsiness, and sleep. It has a depressing effect on the extrapyramidal system and the transmission of excitation from the pyramidal tracts to motor neurons.
The synthetic drug metacin penetrates poorly through the blood-brain barrier, and therefore all its effects are mainly due to the peripheral m-anticholinergic effect. Does not affect the central nervous system. It differs from atropine in a more pronounced bronchodilator effect. The effect on the eye is much weaker than atropine.
Indications for use : peptic ulcer of the stomach and duodenum, spastic conditions of the gastrointestinal tract, biliary tract, ureters, irritable bowel syndrome, urological disorders: hyperkinesia of the bladder with cystitis, hypersalivation and increased secretion of bronchial mucus during anesthesia, reflex bradycardia and arrhythmia during anesthesia , poisoning with ACChE inhibitors, muscarine (atropine)
Contraindications for use : glaucoma, heart disease, gastrointestinal obstruction, ulcerative colitis
Symptoms of atropine poisoning: symptoms associated with the suppression of cholinergic effects and the effect of the substance on the central nervous system are observed. There is dryness of the mucous membrane of the oral cavity and nasopharynx, which is accompanied by impaired swallowing and speech. The skin becomes dry. Body temperature rises. The pupils are wide, photophobia is typical2. Characterized by motor and speech agitation, memory and orientation disorders, and hallucinations. Poisoning occurs as an acute psychosis.
Help: Treatment consists of removing unabsorbed atropine from the gastrointestinal tract (gastric lavage, tannin, activated carbon, saline laxatives), accelerating the elimination of the substance from the body (forced diuresis, hemosorption) and the use of physiological antagonists (for example, anticholinesterase drugs that penetrate well in the central nervous system). In cases of severe agitation, diazepam (Sibazon) and sometimes short-acting barbiturates are prescribed. In case of excessive tachycardia, it is advisable to use β-blockers. A decrease in body temperature is achieved by external cooling. If necessary, artificial respiration is established. Due to photophobia, it is advisable to place such patients in a darkened room.
N-CHOLINOMIMETICS.
Localization of H-cholinergic receptors: neuronal ganglia of the ANS, adrenal medulla, neurons of the central nervous system
Their stimulants: Nicotine, cytisine, anabasine hydrochloride
Mechanism of action : have a two-phase effect on n-cholinergic receptors (the excitation stage is replaced by an inhibitory effect). The first phase (excitation) is characterized by depolarization of the membranes of ganglion neurons, the second (inhibition) is due to competitive antagonism with acetylcholine.
Pharmacological effects:
1) stimulation of the autonomic ganglia (sympathetic more than parasympathetic)
2) cardiovascular system: tachycardia, peripheral and coronary vasospasm, hypertension
3) Gastrointestinal tract, urinary system: inhibition of activity
4) chemocarotid zone: stimulation of respiration
5) CNS: low doses: psychostimulation, high doses – vomiting, tremor, convulsions, coma.
Indications for use : facilitating smoking cessation, reflex cessation of breathing (during operations, injuries, etc.), shock and collaptoid states (pressor effect), respiratory and circulatory depression in patients with infectious diseases.
Contraindications for use : atherosclerosis, marked increase in blood pressure, erosive and ulcerative lesions of the gastrointestinal tract in the acute phase, bleeding from large vessels, pulmonary edema, pregnancy.
Toxicology of nicotine and tobacco smoke products.
In acute nicotine poisoning, hypersalivation, nausea, vomiting, and diarrhea are observed. Bradycardia gives way to tachycardia. Blood pressure is increased, shortness of breath turns into respiratory depression. The pupils are first constricted, then dilated. Help is mainly aimed at maintaining breathing, since death occurs from paralysis of the respiratory center. Chronic nicotine poisoning is usually associated with smoking tobacco. However, it should be borne in mind that tobacco smoke also contains other toxic substances. The symptoms of chronic poisoning are quite varied. Inflammatory processes of the mucous membranes of the respiratory tract are typical. Hypersalivation is observed. The acidity of gastric juice may decrease. Colon motility increases. Among the changes in the blood circulation, in addition to increased blood pressure and increased heart rate, there may be extrasystoles and paroxysmal tachycardia. Nicotine often contributes to the development of angina attacks and sometimes weakens vision. Serious changes are observed in higher nervous activity. Smoking tobacco causes great harm to health. It contributes to the development of coronary heart disease, lung cancer, chronic bronchitis, emphysema, etc. Premature mortality and disability of persons who abuse tobacco smoking increase.
GANGLION BLOCKERS.
Pharmacokinetics
M-anticholinergic drugs are absorbed quite well in the body of patients. Indications for their use involve the exclusion of possible contraindications that could worsen pharmacokinetic characteristics.
After oral or parenteral administration, the drugs quickly distribute through the systemic circulation. Depending on the active component in the composition, its maximum concentration in the blood is achieved after a different period of time.
Medicines from this group almost do not accumulate in the body and tissues, which is considered an advantage, since it reduces the risk of developing complications as a result of an overdose.
The active components of the products are processed mainly in the liver, after which they are excreted through the kidneys. The processing period for ingredients takes from 1 to 3 days depending on the medicine used. With liver damage, the metabolic period is slightly prolonged.
If patients suffer from kidney disease, the elimination of breakdown products of active substances in the body slows down. With prolonged use of the products, there is a slight accumulation in the tissues, which does not affect the condition.
In elderly patients, pharmacokinetic characteristics differ, which is associated with a natural slowdown of metabolism and the presence of chronic diseases of internal organs.
Why are M-anticholinergic drugs used in gastroenterology? Indications for use
Medicines from the group of M-anticholinergics are most often used to treat pathologies of the digestive system.
Main indications for prescribing medications:
- Peptic ulcer of the stomach and duodenum in acute and chronic form. The condition is often accompanied by increased production of hydrochloric acid, as well as the risk of perforation of the organ wall. The drugs help reduce this risk, which prevents the progression of the disease.
- Gastritis with severe symptoms and increased acidity of gastric juice. The drug is not used for the anacid form of inflammation of the gastric mucosa, as it can aggravate the patient's condition.
- Pathologies of the gallbladder and liver, accompanied by hepatic or biliary colic.
- Erosive lesions of the mucous membrane of the esophagus, which provoke discomfort when eating or drinking.
- Frequent heartburn as a result of reflux of stomach contents into the esophagus.
- Pancreatic tumors that provoke excessive production of substances that provoke the active formation of hydrochloric acid. As a result, its negative effect on the gastric mucosa is observed.
- Erosions and ulcers on the mucous membrane of the stomach and intestines that occur during long-term use of non-steroidal anti-inflammatory drugs.
- Exacerbation of chronic diseases of the digestive tract.
Medicines from this group can also be included in the complex treatment of pathologies of the liver, intestines, pancreas, and gall bladder. In each case, the decision to prescribe is made by the doctor based on examination data.
Indications for use
M-anticholinergic drugs are used for diseases of the gastrointestinal tract associated with spasms and excessive secretion of glands: gastric and duodenal ulcers, acute pancreatitis, cholecystitis, cholelithiasis, hepatic and intestinal colic.
M-anticholinergic drugs are also used for diseases associated with bronchospasm - bronchial asthma, chronic obstructive pulmonary disease.
M-anticholinergic agents are used to dilate the pupil and examine the fundus of the eye, as well as when selecting glasses and contact lenses to determine the refractive power of the eye lens.
M-anticholinergics are prescribed for an overactive bladder - frequent urination, urinary incontinence, and also for renal colic.
In addition, M-anticholinergic blockers are used for bradycardia, before operations to reduce the negative effects of anesthesia, as well as in case of poisoning with cholinomimetics and anticholinesterase drugs (including pesticides).
Platyphylline hydrotartrate is also used for hypertensive crisis - a sharp excessive increase in blood pressure.
Contraindications
M-anticholinergic blockers (indications for use are analyzed together with contraindications before starting therapy) are not used in case of intolerance to the components in the composition of any drug or a tendency to such manifestations.
Other contraindications for therapy include:
- Severe heart pathologies in acute and chronic form. In case of heart failure, coronary heart disease, angina pectoris, you should not use drugs from this group. During the recovery period after a myocardial infarction, medications are also not used, as there is a risk of complications and worsening symptoms.
- Acute severe liver diseases. The drugs can be used in the absence of serious disorders on the part of the organ, but if the disease progresses, it is better to abandon them.
- Ulcerative colitis in acute form. Despite the positive effects of drugs on the gastric mucosa, they can negatively affect the intestines.
- Acute obstruction of the gastrointestinal tract. In this case, the drugs can lead to serious complications.
- Severe glaucoma with severe visual disturbances.
- Gastritis with low acidity of gastric juice, which causes indigestion.
- Inflammatory pathologies of the large intestine in the acute stage.
- Severe prostatic hyperplasia, accompanied by severe disorders of the urinary system.
- The period of pregnancy and lactation, when drugs can negatively affect the condition of the mother and child.
- Acute conditions associated with gastrointestinal bleeding due to perforation of the wall of the digestive tract.
- Esophageal hernia.
The drugs are prescribed with caution to elderly patients, since they often suffer from diseases of the cardiovascular system.
pharmachologic effect
M-anticholinergics have a wide range of pharmacological effects: dilate the pupil, relax the bronchi, increase the frequency and strength of heart contractions, reduce the formation of gastric acid, inhibit the secretion of glands of the digestive tract, reduce gastrointestinal motility and peristalsis, reduce bladder tone and cause relaxation smooth muscles of the urinary tract.
Platyphylline hydrotartrate additionally dilates blood vessels and lowers blood pressure.
Side effects
M-anticholinergic blockers (indications for use do not always allow starting therapy with drugs from this group) can provoke complications if used incorrectly. Often complications are associated with intolerance to the components, which the patient did not know about before starting use. The drugs may cause dizziness, severe headache and weakness.
Often negative reactions affect the digestive tract, accompanied by nausea and vomiting. The condition is aggravated by indigestion and frequent loose stools. Sometimes complications manifest themselves in the form of persistent constipation, as well as pain in the intestinal area.
Adverse reactions affect the cardiovascular system and can reduce or increase blood pressure. When used in moderate doses, bradycardia is observed; when the dosage is exceeded, pathological tachycardia is observed.
Increased intraocular pressure is considered a common reaction with long-term use of the drugs. Even in the absence of pathologies of the visual apparatus, such complications are possible. Negative reactions can affect the urinary system, which leads to impaired urine outflow and a significant decrease in daily diuresis.
Medicines can also provoke other serious complications:
- Seizures.
- Hallucinations.
- Emotional agitation or constant drowsiness, severe weakness.
- Paralysis of the respiratory system, accompanied by suffocation and other complications associated with this disorder.
The most severe complication is coma, which develops in most cases due to drug overdose. An allergic reaction to medications manifests itself in a standard form, accompanied by a rash, irritation and severe itching.
In case of an overdose, all negative symptoms are aggravated, the condition worsens significantly, and the patient’s life is threatened. If complications occur, you should immediately stop using the medications and visit a doctor, who will normalize the condition with the help of other medications.
Precautionary measures
Drugs from the group of M-anticholinergics are not used simultaneously with some non-steroidal anti-inflammatory drugs, as well as sedatives and tranquilizers.
When using medications, the patient's condition should be monitored using special studies. The patient regularly visits the doctor, which allows him to monitor therapy and note possible deterioration that requires discontinuation of the medication.
If complications occur, treatment cannot be continued. Patients are also not allowed to independently exceed the dosage or prolong the therapeutic course.
When using drugs in combination with some antihistamines, the antacid effect may be enhanced, which is worth considering. Often, M-anticholinergic drugs are prescribed in combination with anti-inflammatory medications, which enhance their effectiveness.
Do not prescribe drugs simultaneously with other antacids based on similar components, which can lead to complications.
Classification of M-anticholinergic drugs
Drugs of the M-anticholinergic group are classified into:
- systemic drugs: atropine sulfate, butylscopolamine (scopolamine butylbromide), hyoscine, platiphylline hydrotartrate;
- selective M1-anticholinergic blockers that affect the formation of hydrochloric acid in the stomach: pirenzepine, telenzepine;
- drugs affecting bronchial tone: ipratropium bromide, tiotropium bromide, umeclidinium bromide, aclidinium bromide, glycopyrronium bromide;
- drugs that affect bladder tone: tolterodine, oxybutynin, solifenacin, darifenacin, trospium chloride;
- drugs that affect pupil size: atropine sulfate, tropicamide, cyclopentolate.
List of drugs, dosage regimen
M-anticholinergic drugs (indications for use should be studied by patients in advance) are represented by a fairly large group of medications. There are many drugs in this group used for various disorders.
But some of them are used most often:
- Becarbon – a product based on belladonna extract and sodium bicarbonate, which is available in tablet form and has a pronounced antacid, antispasmodic effect on the patient’s digestive tract. Additionally, the medication reduces the secretion of the digestive glands, which has a positive effect on the condition of patients. The remedy is prescribed for indigestion, gastritis and some other diseases. The dosage regimen involves taking 1 tablet 3 times a day 30 minutes before meals. Treatment lasts up to 3 weeks depending on the severity of the symptoms.
- Besalol also contains belladonna extract, but is additionally enriched with the component salol or phenyl salicylate, which enhances its effectiveness. The tablets have pronounced antispasmodic and antiseptic properties and are prescribed for various pathologies of the digestive tract. Take 1 tablet orally 3 times a day. Treatment usually does not last longer than 3 weeks.
- Bellalgin is considered a more effective remedy, since it contains not only a plant extract, but also metamizole, benzocaine and sodium bicarbonate. The medicine helps eliminate spasms and pain in the digestive organs. Used in short courses to improve the condition and stop the progression of the disease. The daily dosage of the medication for patients is 3-6 tablets, which should be divided into 3 doses during the day. The duration of therapy is usually 5-7 days.
- Gastrocepin is a medicine based on pirenzepine as the main active ingredient. It is actively used in gastroenterology, as it has pronounced antacid properties, which reduces the acidity of gastric juice and reduces its negative impact on the walls of the organ. The drug can be taken orally, 2 tablets per day, it is also administered intramuscularly, 2 ml intramuscularly. Treatment can last 2-3 weeks.
- Buscopan always used in combination with other agents to achieve an antispasmodic effect. The drug helps to relax the smooth muscles of the digestive tract, which significantly alleviates the condition and helps cope with severe disorders. Tablets are taken orally, 2 pieces per day for 5-10 days.
- Atropine is considered the most important and potent representative of the group of M-anticholinergic drugs. It has pronounced properties and is used for pathologies of the stomach, gall bladder and some other diseases. The drug in the form of a solution is administered intravenously, subcutaneously or intramuscularly. They are prescribed in short courses of 7-10 days with daily administration of 1 ml of medication. The dosage and duration of use may vary depending on the individual patient.
- Metacin is more effective than some other drugs, as it has pronounced antispasmodic properties and reduces the activity of the digestive glands. Take 2-3 tablets per day before meals. Treatment lasts up to 14 days. Often the use is combined with the use of other medications that enhance the effect and shorten the course of therapy.
Such products are used most often, as they have pronounced properties. Other medications are not prescribed in most cases.
M-anticholinergics
- Mechanism of action
- Pharmacokinetics
- Dosage regimen
- Side effects
Anticholinergics are drugs that prevent the development of the effects of acetylcholine in the autonomic ganglia, in skeletal muscles and in organs receiving parasympathetic innervation. M-anticholinergic agents are distinguished by strength and duration of action: short (diagnostic) - Tropicamide (Midriacyl) and long (therapeutic) action - atropine, cyclopentolate (Cyclomed), scopolamine, homatropine methyl bromide.
This group of drugs also includes the combination drug Midrimax.
Depending on the organs and tissues in which m-cholinergic receptors are located, they can be of three types:
- m1 – receptors are located in nerve cells (brain, peripheral nerve plexuses),
- m2 - receptors - in the heart,
- m3 - receptors - in the smooth muscles of the eye, bronchi, bile and urinary tract, intestines, as well as gland cells: sweat, salivary, bronchial, gastric.
The presence of several modifications of m-cholinergic receptors allows you to selectively influence one of them and avoid the development of unnecessary effects. For example, reduce smooth muscle tone without changing the activity of the heart, or dilate the pupils to examine the fundus without causing relaxation of the intestines.
Indications for use
- Spasms of accommodation of a semi-persistent and persistent nature in children with refractive errors.
- Complex therapy of inflammatory diseases of the anterior part of the eye to prevent the development of posterior synechiae.
For diagnostic purposes, M-anticholinergics are used for:
- pupil dilation during ophthalmoscopy
- achieving cycloplegia for the purpose of studying refraction in children
- preoperative preparation of patients for vitreoretinal surgery and cataract surgery.
Mechanism of action
| Pharmacodynamics of cycloplegic mydriatics | ||||
| A drug | Midriaz | Cycloplegia | ||
| t until the max effect develops, min | duration, days | t until the max effect develops, min | duration, days | |
| Atropine | 30-40 | 7-10 | 60-180 | 6-12 |
| Homatropine methyl bromide | 40-60 | 1-3 | 30-60 | 1-3 |
| Scopolamine | 20-30 | 3-7 | 30-60 | 3-7 |
| Cyclopentolate | 30-60 | 1 | 25-75 | 0,25-1 |
| Tropicamide | 20-40 | 0,25 | 20-35 | 0,01 |
As a result of blockade of M-cholinergic receptors located in the sphincter of the pupil and the ciliary muscle, passive dilation of the pupil occurs due to an increase in the tone of the muscle that dilates the pupil and relaxation of the muscle that constricts it. At the same time, due to relaxation of the ciliary muscle, accommodation paresis occurs.
An intensely pigmented iris is more resistant to dilatation; to achieve a sufficient mydriatic effect, it may be necessary to increase the concentration of the drug or the frequency of administration. As a result of increasing the dose of the drug, systemic side effects and symptoms of overdose may develop in this group of patients.
Pupil dilation can trigger an acute attack of glaucoma in patients with angle-closure and mixed glaucoma, people over 60 years of age, and people with hyperopia who are predisposed to angle-closure glaucoma due to the fact that they have a shallow anterior chamber.
By blocking M-cholinergic receptors in other organs and tissues, drugs of this group reduce the secretion of the lacrimal, salivary, bronchial, sweat and gastric glands. Anticholinergic drugs reduce the tone of smooth muscles of internal organs (bronchi, urethra, bladder and gastrointestinal tract). They have a moderate stimulating effect on the central nervous system (excitement, hallucinations, etc.) and a delayed long-term sedative effect. By lowering the tone of the vagus nerve, they lead to an increase in heart rate (HR) and an increase in conduction along the Hiss bundle. In high doses they cause vasodilation.
Pharmacokinetics
Ocular pharmacokinetic data are available only for atropine. When applied topically (drip or subconjunctival), atropine accumulates in almost all tissues of the eye, where it is partially hydrolyzed under the influence of the enzyme atropine esterase. When applied topically, it is well adsorbed into the systemic circulation. T1/2 is 2 hours. About 40% is metabolized in the liver. The unchanged drug and its metabolites are excreted in the urine.
Dosage regimen
For therapeutic purposes, use 3-4 times a day. To achieve cycloplegia, 3-4 repeated instillations are required with an interval of 10-15 minutes 1 hour before the test.
Side effects
| Clinically significant interactions of M-anticholinergic drugs | |
| Medicines | Result of interaction |
| Nitrates | Increased risk of increased IOP |
| Procaine (Novocaine) | Enhanced anticholinergic effect |
| Monoamine oxidase inhibitors | Cardiac arrhythmias may occur (especially when used with atropine) |
| Lily of the valley preparations | When taken orally with atropine, a mutual weakening of the effects is observed. |
- From the cardiovascular system - tachycardia.
- From the side of the central nervous system—hallucinations, agitation; in large doses, small children and the elderly may experience respiratory paralysis, mental and motor restlessness, dizziness, convulsions, and hallucinations.
- On the part of the organ of vision - subcapsular cataract, exophthalmos, glaucoma, increased IOP.
- From the gastrointestinal tract - dry mouth, constipation.
- From the urinary system - difficulty urinating.
- On the part of the organ of vision - transient decrease in vision, photophobia, swelling and hyperemia of the skin of the eyelids and conjunctiva
To reduce systemic side effects, it is necessary to clamp the tear ducts at the inner corner of the eye for several minutes after instillation.
Contraindications
- Hypersensitivity.
- PAOG or anatomically narrow angle of the anterior chamber of the eye.
Features of the use of M-anticholinergic drugs for various pathologies
Depending on the specific disease, a specialist can prescribe drugs from the group of M-anticholinergic blockers to patients according to different schemes. He can also combine several drugs from this group to achieve a pronounced result. The drugs can also be used not only for pathologies of the digestive system.
| Diseases | Use of medications |
| Hepatic and biliary colic | For such pathologies, the patient may be prescribed Gastrocepin at a dosage of 2 ml per day. The drug is administered intramuscularly. Additionally, the doctor usually uses Bellargin and prescribes 2 tablets to the patient 2 times a day for 5 days. Usually this is enough to eliminate symptoms and alleviate the condition. |
| Threat of premature birth | For such disorders, the patient takes Metacin 1 tablet 2-3 times a day, depending on the severity of the condition. Additionally, she may be prescribed medications from other groups. |
| Dyspeptic disorders of various origins | For such disorders, Gastrocepin is prescribed in tablet form in courses of 10 days. It helps to significantly improve the condition. The patient takes 1 tablet 3 times a day before meals. |
| Peptic ulcer, gastritis with increased acidity of gastric juice | For such disorders, Becarbon is combined with the use of Metacin. The first one is taken 2 tablets 2 times a day, the second drug is taken 1 tablet 3 times a day. Treatment lasts from 2 to 3 weeks. |
| Kidney pathologies accompanied by the formation of stones or sand | To provide an antispasmodic effect to facilitate the removal of stones and sand, Besalol is prescribed. The daily dosage is 6 tablets, which should be divided into 3 times during the day at equal intervals. Therapy is continued for 7-14 days. |
| Heartburn | For heartburn, Gastrocepin or Becarbon is prescribed, 2-3 tablets per day before meals. Therapy is usually symptomatic, but it is often combined with other drugs to increase effectiveness. Therapy can last from 1 to 3 weeks, depending on the advanced state of the condition and the presence of concomitant complications from other organs. |
for different conditions, the dosage and regimen of medication may differ, which depends on the individual characteristics of each patient, but it is important to use the drugs as directed and strictly follow the recommendations. This will significantly reduce the risk of complications.
M-anticholinergics are a broad group of medications with pronounced therapeutic properties. Indications for their use involve prescribing them to improve the condition of patients with gastritis, peptic ulcers and certain pathologies of the liver and gallbladder.
Many drugs can provoke serious complications, so you should not use them yourself without prior examination.
M-anticholinergics in the treatment of overactive bladder
Overactive bladder (OAB) is a severe urinary disorder that affects at least 17% of the population over 40 years of age, of whom 56% are women and 44% are men (16). At the same time, there are differences due to gender, age, and ethnicity.
Figure 1. Prevalence of OAB in different age groups (Milsom I., Abrams P., Cardozo L. et al., 2001)
Figure 2. Prevalence of OAB symptoms (SIFO Group Survey)
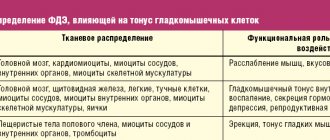
Table 1. Topical characteristics of M-cholinergic receptors in the human body (BJU may 2000; Vol. 85, Supp. 3: 35)
Table 2. Comparison of the affinities for M-cholinergic receptors (in vitro) of tolterodine and oxybutynin
Table 3. Comparative characteristics of the selectivity of various M-anticholinergic drugs (Vesicare SmPC, Astellas, 2005)
Table 4. Changes in core symptoms of detrusor overactivity based on 12-week studies of fesoterodine (Pfizer labs., 2008)
Typically, the prevalence of OAB is underestimated because the vast majority of studies include patients with only one of the symptoms of urge incontinence (14, 16). With age, the number of patients with various disorders of the lower urinary tract function increases significantly, especially with OAB (Figure 1) (8, 20).
Some current evidence suggests that the role of M2 receptors may be more pronounced with age. It is believed that these receptors may play an important role in the age-dependent increase in the α1-adrenergic receptor response in bladder tissue, and facilitation of the contractile response associated with α1A-adrenergic receptors may be the cause of bladder overactivity in older people.
The clinical manifestation of detrusor overactivity is characterized by urgency, pollakiuria, nocturia, and urge incontinence (or urge urinary incontinence) (Figure 2). Occurring at any time and often in an inconvenient place, these symptoms bring significant anxiety to patients.
Urinary incontinence, or even urinary incontinence, may also be a consequence of urethral instability caused by fluctuations in maximum urethral pressure of more than 15 cmH2O. Art. Urinary incontinence is not a prerequisite for a diagnosis of OAB, since half of the patients have only sensory symptoms: frequent daytime and nighttime urination, urgency. This variant of the symptom complex is called dry OAB.
It should be borne in mind that the presence of detrusor overactivity detected during urodynamic study does not mean that the patient should suffer from urinary incontinence. For example, asymptomatic detrusor overactivity is reported in 42% of healthy women over 65 years of age (20). In the case of urge urinary incontinence, it is customary to talk about wet, or wet, OAB (14, 20, 22).
With age, researchers note a significant increase in the proportion of wet OAB. Between the ages of 65 and 74 years, up to 20% of women experience urge urinary incontinence. According to a Swedish study, in older people 75 years of age and older, 42% of women and 35% of men suffer from urge urinary incontinence (Stenzelius K., Mattiasson A., Hallberg IR, Westergren A., 2004).
With age, the frequency of symptoms increases to 30% in people over 65 years of age and to 40% after 70 years of age. In European countries, almost 22 million people suffer from this serious disease, but only 27% of them receive treatment, indicating a lack of recognition of the problem by both patients and health care providers (20).
The prevalence of urinary frequency and urgency is similar among men and women, and urge incontinence is more common in women in older age groups. The etiology and pathogenesis of imperative urinary disorders caused by bladder overactivity are still unclear. There are several theories about the development of this disease. Nerve degeneration is a common sign of developing an unstable bladder. It is possible that detrusor overactivity is caused by age-related changes not only in the urinary tract, but also in the central nervous system (CNS). It is obvious that various changes in both the peripheral nervous system and the central nervous system can be the cause of detrusor overactivity.
There is an opinion that the etiology of OAB is associated with qualitative changes in the smooth muscles themselves. Normally, smooth muscle cells in the bladder are in a state of spontaneous activity. During filling, however, their activity is not synchronized because each of the cells is connected to only a few of its neighbors, and there is no particular interconnection between individual bundles. The synchronous activation observed during micturition is not possible without dense dense innervation, and large numbers of smooth muscle cells must be activated by nerve impulses.
Elbadawi A. et al. (1997) used electron microscopy to examine biopsy tissue samples from elderly patients with urodynamically documented voiding dysfunction. The researchers described a so-called circuit breaker pattern, or disconnected pattern, found in patients with OAB. The peculiarity of this model was the moderate expansion of intercellular spaces, the presence of rare intermediate connections between cells, but was distinguished by the excessive content of special characteristic protruding joints and the close fit of cell supports. It has been suggested that protruding junctions and cellular support borders mediate direct communication between individual smooth muscle cells and that they are involved in the generation of muscle contraction in patients with OAB. Five patients initially in this study with detrusor stability developed a detrusor overactive state over time. Ultrastructural studies of new biopsy materials showed the presence of a so-called disconnection pattern, in contrast to previous biopsies performed on the same patients (Elbadawi A., Hailemariam S., Yalla SV, Resnick NM, 1997).
In older men, the development of OAB symptoms is often accompanied by bladder outlet obstruction (IVO) as a result of prostate disease. About 60% of men with BOO report symptoms of OAB. There is no precise explanation for the relationship between bladder outlet obstruction and OAB. According to Wein AJ (2003), OAB occurs in 52-80% of men with BOO due to prostatic hyperplasia, and in 38% of men it continues to occur after surgical removal of obstruction.
Existing studies indicate a number of neurological changes (Steers WD, De Groat WC, 1988, Sibley GN, 1987) and an increase in α-adrenergic activity as a result of detrusor ischemia (Perlberg S., Caine M., 1982) due to its hypertrophy against the background of IVO. With detrusor hypertrophy resulting from obstruction, metabolic demands increase coupled with decreased blood flow, leading to anoxia and neuronal death (Levin RH et al., 1999). Moreover, there is evidence that the density of cholinergic nerve fibers in the detrusor is 60% less in the group of patients with BPH and BOO compared to a group of patients of the same age and without BOO. The authors believe that a significant decrease in nerve fiber density in response to BOO due to BPH may lead to impaired neuromuscular control of the bladder.
A large role in the development of imperative urination disorders in menopausal women is given to estrogen deficiency and associated atrophic changes in the urothelium and dystrophic changes in the bladder muscle (2-4). This may be the cause of the sensory symptoms that accompany dry OAB (pollakiuria, nocturia, urinary urgency). 70% of women associate their appearance with the onset of menopause (16), which is considered one of the main risk factors for the development of OAB in women. According to Versi E. et al. (1995), the frequency of stress urinary incontinence in women decreases with increasing duration of postmenopause, and simultaneously with increasing age, the frequency of detrusor overactivity increases. Some studies have shown that individual neurons in the spinal cord contain estrogen receptors and are targets for estrogen. The presence of estrogen receptors in neurons of central brain regions raises the possibility that endocrine age-related changes may act through supraspinal voiding control.
The development of detrusor hypoxia and, as a consequence, metabolic disorders in its structure impairs its contractility. This suggests that ischemia and hypoxia may underlie intramural neuronal damage and lead to changes in bladder smooth muscle function in patients with detrusor overactivity. Ischemia leads to apoptosis of smooth muscle cells, in addition to disruption of nerve conduction. Nerve tissue is more sensitive to ischemia than smooth muscle, and some of this damage is almost irreversible. Nerve degeneration is a common sign of developing an unstable bladder. With detrusor hypertrophy resulting from obstruction, metabolic demands increase coupled with decreased blood flow, leading to anoxia and neuronal death (Levin RH, 1999).
Abrams P. (1985) believes that detrusor overactivity in patients with BPH is not the result of BOO, but a consequence of age-related changes in the bladder wall. Despite the conflicting data, it should be recognized that both age and BOO can lead to postsynaptic denervation of the bladder. This circumstance once again emphasizes the important role of the nervous system in controlling the storage function of the bladder.
The role of hereditary factors is being studied, and a number of modern studies indicate the possibility of genetic changes in the presence of OAB.
According to the classical physiological concept, bladder function is ensured by the antagonistic interaction of the sympathetic and parasympathetic parts of the nervous system (14). The sympathetic department is responsible for relaxing the detrusor and contracting the urethral sphincter, the parasympathetic department is responsible for contracting the detrusor and relaxing the sphincter. Activation of one or another system determines the condition of the lower urinary tract. Receptors in the area of the endings of the sympathetic nerves of the bladder and urethra, depending on the physiological effects that occur when they are stimulated, are divided into a- and b-adrenergic receptors.
Stimulation of a-adrenergic receptors leads to a contraction of smooth muscle fibers of these parts of the urinary tract and an increase in urethral resistance. Stimulation of b-adrenergic receptors causes inhibition of detrusor activity and its physiological adaptation to the incoming volume of urine. Adrenergic inhibitory neurons mainly arise from n .
hypogastricus
, while the excitatory nerves are believed to arise from the pelvic nerve and are of the cholinergic type. The receptors of the parasympathetic (cholinergic) nerve system are evenly distributed in the muscular wall of the bladder and are almost never found in the area of its base and urethra. Stimulation of these receptors causes detrusor contraction.
There are currently five known molecular subtypes of muscarinic M-cholinergic receptors, and tissues can contain varying numbers of different subtypes (Table 1).
For example, human bladder smooth muscle contains mixed populations of M2 and M3 subtypes. Particularly noteworthy are the M3 receptors, through which the impulse to contract the detrusor is transmitted, and the M2 receptors, the effect on which prevents the relaxation of its smooth muscles. The main number of muscarinic receptors in the bladder falls on the M2 subtype (80%). It is known that M2 receptors make up 4/5 of all muscarinic receptors in the bladder.
Stimulation of M3 receptors by acetylcholine leads to phosphoinositol hydrolysis and ultimately to the accumulation of intracellular calcium and smooth muscle contraction. Activation of M2 receptors leads to inhibition of adenylate cyclase and restores sympathetic-associated relaxation of bladder smooth muscle. The end result is the most efficient and complete emptying of the bladder.
Some current evidence suggests that the role of M2 muscarinic receptors may be more pronounced with age. The predominance of activity of cholinergic receptors of the parasympathetic part of the autonomic nervous system is characterized by a decrease in the physiological capacity of the bladder during the filling phase, a rapid increase in detrusor pressure, as well as an increase in intravesical and detrusor pressure during the emptying phase with an increase in the maximum volumetric flow rate of urine and a reduction in urination time.
The prevalence of activity of b-adrenergic elements of the sympathetic link is determined by an increase in the physiological capacity of the bladder and a decrease in the maximum values of intravesical and detrusor pressure. The presence of uncoordinated contractions of the detrusor is regarded as evidence of increased activity of muscarinic-sensitive cholinergic neurostructures, evenly distributed throughout the detrusor body. It is known that the function of the lower urinary tract is carried out due to the close antagonistic interaction of adrenergic and cholinergic receptors of the sympathetic and parasympathetic parts of the autonomic nervous system. Therefore, it is clear that if at least one type of receptor is damaged or functionally insufficient, this entire system of harmonious balance is certainly disrupted due to the predominance of the action of the opposite group of receptors (11).
According to modern understanding, many receptors for various transmitters have been found in the lower urinary tract, including such as nitric oxide and substance P. Various co-transmitters and neuromodulators have a stimulating effect on bladder smooth muscle, such as ATP, substance P, GABA, NPY and various others. The possible presence of various neurotransmitters and modulators in the lower urinary tract has been much debated over the past twenty years.
The connection between detrusor hyperactivity and increased activity of the parasympathetic division of the autonomic nervous system has been proven and explains the therapeutic effect of the use of blockers of peripheral muscarinic-sensitive cholinergic receptors. Against their background, the influence of the parasympathetic link weakens, and the sympathetic one increases, thereby reducing intravesical pressure, uncoordinated contractions of the detrusor are reduced or suppressed, the effective capacity of the bladder increases and the adaptive function of the detrusor improves (5, 6).
Pharmacotherapy is one of the most common methods of treating OAB. According to the recommendations, this is the method of choice. This is followed by behavioral therapy, physical therapy and other treatments. The drug method is of interest primarily due to its availability, the possibility of long-term use and individual selection of the dose and treatment regimen. Pathogenetic pharmacotherapy should be focused on the possible mechanisms of development of OAB - myogenic and neurogenic. Pharmacological treatment of overactive bladder is a complex problem. Both domestic and foreign scientists have dealt with the issue of symptomatic treatment of this condition.
For the treatment of OAB, anticholinergic drugs are most often used, first proposed by Langworthy O. (1936), which disrupt the conduction of impulses in the parasympathetic ganglia or prevent the interaction of the parasympathetic transmitter acetylcholine with M-cholinergic receptors (Diokno A. Lapides J., 1972). Most of these drugs cause inevitable side effects, which makes it necessary for the doctor to maintain a balance between the advantages and disadvantages of the drugs. Antimuscarinic action usually causes dry mouth, constipation, difficulty in accommodation, and drowsiness. The drugs should not be prescribed to patients with impaired urine flow from the bladder (obstructive uropathy), bowel obstruction, ulcerative colitis, glaucoma, or myasthenia gravis. In a normal bladder, cohesion between muscle fiber bundles ensures that the occurrence of diffuse activity does not lead to an increase in bladder pressure. In an unstable (overactive) bladder, these connections are strengthened, which leads to a wave of diffuse excitation, urgency and uncontrolled detrusor contractions. This hypothesis explains the effectiveness of antimuscarinic drugs in urge urinary incontinence. If some of the ganglia are excited directly by sensory nerves, then suppression of this effect should lead to the elimination of both urgency and unstable contractions.
One of the most well-known anticholinergic drugs is atropine, which has a pronounced systemic effect. And although some pilot studies have shown significant effectiveness and safety of its intravesical use for hyperreflexia, the most common method of administration at present is electrophoresis. The lack of selectivity of the drug's action, without a doubt, becomes a negative factor, since it determines the low effectiveness of its therapeutic doses against the symptoms of hyperactivity. The drug is currently of more historical interest, and is practically not used in the treatment of detrusor overactivity.
Fowler S. (1996) proposed an anticholinergic drug - oxybutynin. Previously, oxybutynin, which has antimuscarinic, antispasmodic and local anesthetic effects, was called the “gold standard” in the treatment of OAB, although not all of the above properties are observed when using therapeutic doses. Individual dosage adjustment is necessary, and patients are warned that this will take a certain period of time, during which it is necessary to visit a doctor. The optimal dose is considered to be the one that gives the desired effect with minimal side effects. Doses for oral administration range from 2.5 mg once to 5 mg 4 times a day. The standard starting dose for adults is 5 mg 2-3 times a day. In the elderly, a rational starting dose is 2.5 mg 2-3 times a day. The dose must be maintained for 7 days before adjustment (either decreasing or increasing, depending on the severity of the clinical effect). In order to reduce the severity of side effects, the dose of oxybutynin is reduced. Malone-Lee J. et al. (1992) suggested reducing the dose to 5 mg per day, Moore K. et al. (1990) – up to 3 mg, and Bemelmans BLH et al. (2002) – up to 2.5 mg 3 times a day.
If oral administration of oxybutynin is not possible, Brendler C. et al. (1989), Maderbacher H., Jilg G. et al. (1985), Weese D. et al. (1993) proposed a method of administering 5 mg of oxybutynin directly into the bladder, dissolved in 30 ml of sterile water, 2-3 times a day. Enzelsberger et al. (1995) proposed 20 mg of oxybutynin dissolved in 40 ml of water to be administered into the bladder for 10 days. In a double-blind, randomized study, no adverse reactions were noted, and the use of intravesical oxybutynin was recommended in case of severe side effects with oral administration.
An alternative method of using oxybutynin in rectal suppositories was proposed by Wiskind AK et al. (1994). A good therapeutic effect was noted, but side effects such as dry mouth and inhibition of peristalsis persisted.
Tolterodine is the first drug specifically developed for the treatment of patients with bladder overactivity, manifested by frequent urinary urgency and urge urinary incontinence. This drug is developed using an integrated approach to achieve bladder selectivity. Tolterodine is a competitive antagonist of M-cholinergic receptors, which is a mixed antagonist of M2 and M3 cholinergic receptors localized in the bladder and salivary glands, blocks calcium channels and, thus, has a dual effect on the bladder. The drug is selective for the bladder. The safety, efficacy and tolerability of tolterodine were assessed in four randomized, double-blind, parallel, multicenter, 12-week studies in patients with overactive bladder (Appell RA, et al., 2001, Drutz H., Appell RA, 1997, Nilvebrant L. et al., 1997). Studies have shown good tolerability of the drug, high efficiency and pronounced selectivity for cholinergic muscarinic receptors of the bladder compared to receptors of the salivary glands, in contrast to oxybutynin (Table 2).
The selectivity of tolterodine allows for long-term use of the drug. Moreover, according to research results, the frequency of side effects with long-term (up to 2 years) use of tolterodine does not increase, but rather decreases. Thus, the incidence of dry mouth after a year of using the drug is 36%, and by the second year of taking the drug it decreases to 19% (16). The frequency of urination after 12 months of use decreased by 22% and the frequency of episodes of urge incontinence by 58%.
In foreign literature there is data on the use of tolterodine in children 1 mg 2 times a day, which led to a decrease in the frequency of urination, a decrease in episodes of urinary incontinence, and there were no serious side effects. A study by M. Munding and H. Wessells (2001) found that tolterodine reduces the number of episodes of urge incontinence. Improvement or cure was observed in 73% of children taking the drug. According to P. Abrams et al. (2001), tolterodine does not significantly reduce peak urinary flow rate, does not reduce detrusor pressure at peak urinary flow rate, and does not cause a clinically significant increase in residual urine in men with OAB and BOO due to BPH. This effect of tolterodine is undoubtedly very important in such a large category of urological patients.
Another form of tolterodine is extended-release capsules of 4 mg, used once a day (except for patients with severe impairment of liver and kidney function, in which case capsules of 2 mg per day are used).
Another M-anticholinergic drug that is used to treat OAB is trospium chloride. It is a parasympatholytic with peripheral, atropine-like effects, as well as ganglionic myotropic effects similar to papaverine. Trospium chloride is a competitive antagonist of acetylcholine at postsynaptic membrane receptors, blocks the muscarinic action of acetylcholine and inhibits the response caused by postganglionic parasympathetic activation of the vagus nerve. It has a high affinity for M1 and M3 cholinergic receptors. Trospium chloride reduces the tone of the smooth muscles of the bladder, has a relaxing effect on the smooth muscles of the detrusor bladder, both due to the anticholinergic effect and due to the direct myotropic antispastic effect.
Trospium chloride is a quaternary ammonium compound with an antimuscarinic type of action. Although the bioavailability of trospium chloride is inferior to that of tertiary amines, this does not affect its effectiveness, but only determines the need for its use in higher doses. The dose of the drug is selected individually from 30 to 90 mg per day, depending on the clinical picture and severity of the disease. The concentration of trospium chloride after a single dose ranges from 20 to 60 mg, proportional to the dose taken. Trospium chloride is more hydrophilic relative to the tertiary compounds oxybutynin and tolterodine, penetrates the blood-brain barrier less well and is less likely to cause side effects from the central nervous system.
A study of 75 women with OAB incontinence (Fuertes et al., 2000) demonstrated not only an effective effect of trospium chloride (daily dose 40 mg, treatment duration 8 weeks) on the clinical manifestations of detrusor overactivity and urodynamic parameters, but also an improvement in quality indicators patients' lives by 35%. When comparing the effectiveness of trospium chloride and tolterodine in a double placebo-controlled study in patients with urinary urgency disorders, both drugs showed a decrease in urinary frequency - by 23% and 28% for tolterodine and trospium chloride, respectively, and an increase in urinary volume - by 39% and 33% respectively. The number of episodes of urinary incontinence was reduced by 67% and 73% for tolterodine and trospium chloride, respectively. The severity of side effects was similar in both subgroups (12). According to D.Yu. Pushkarya et al. (2004), while taking trospium chloride for 12 weeks, there was a decrease in the number of urinations per day by 20%, a decrease in the average number of episodes of urinary incontinence by up to 40%, and an increase in the volume of urination by 18.8%.
A new drug successfully used to treat OAB is the M-anticholinergic blocker solifenacin (Vesicare). Solifenacin, the active substance of Vesicare, is a specific competitive inhibitor of muscarinic receptors (M-cholinergic receptors), predominantly of the M3 subtype. However, solifenacin has low or no affinity for other receptors and ion channels. The maximum effect after taking Vesicare in doses of 5 or 10 mg can be detected after 4 weeks, which was shown in double-blind randomized clinical trials in men and women with OAB syndrome. The clinical effect of taking Vesicare is observed within the first week of treatment, and effectiveness remains for at least 12 months. There is no need to adjust the dose of Vesicare depending on the patient's age. The area under the concentration/time curve (AUC) is similar in elderly (65-80 years) and healthy young adults (<55 years). The time to reach maximum concentration is slightly lower, and the half-life is increased by 20% in elderly patients. These differences are not clinically significant.
The initial dose of Vesicare is 5 mg 1 time per day; if necessary, the dose can be increased to 10 mg 1 time per day. The most common side effect of Vesicare is dry mouth (occurring in 11% of patients receiving a daily dose of 5 mg and 4% receiving placebo). Solifenacin is characterized by a low incidence of side effects typical of antimuscarinics (for example, dry mouth), which is due to the higher selectivity of the drug to bladder tissue. Vesicare is more bladder selective than tolterodine and oxybutynin (Table 3).
The effectiveness of the drug in doses of 5 mg 10 mg has been studied and proven in many clinical studies in patients with OAB syndrome: a statistically significant decrease in the number of urinations (including at night), episodes of urgency, and an increase in the average volume of urination was noted. The effect appeared already during the 1st week of treatment, reaching its maximum value after 4 weeks. The effectiveness of the drug is maintained over long-term use (at least 12 months).
According to studies, with the use of solifenacin at a dose of 5 mg and 10 mg per day, the number of episodes of urgency is reduced by 49% and 55%, respectively, the number of episodes of urgent urinary incontinence - by 58% and 62%, respectively, the frequency of urination (by 5 mg per day) – by 19%, and the volume of urine excreted increases by 21% (VesicareÒ SmPC, Astellas, 2005).
Taking into account the high selectivity and good tolerability of the drug, its high effectiveness is noted with long-term (up to 60 weeks) use. According to the results of a study conducted by Haab F. et al. (2005), after 60 weeks of use of solifenacin at a dosage of 5 mg per day, 62.7% of patients began to retain urine, 43.1% decreased episodes of urgency, 41.8% decreased urinary frequency, 23.1% of patients got rid of nocturia. 81% of patients participating in the study completed the study, and only 4.8% dropped out due to adverse events.
Of the M-anticholinergic blockers that are not yet registered in Russia, darifenacin and fesoterodine should be noted. Darifenacin is an M3 receptor antagonist, but is characterized by a more selective effect compared to other anticholinergic drugs. So far it is known that at a dose of 2.5 mg it does not affect the salivary glands. With darifenacin treatment, urodynamic parameters improve only at a dose of 10 mg per day (24).
Fesoterodine is a new muscarinic receptor antagonist also used as a drug to treat OAB syndrome. The effectiveness of fesoterodine was shown in blinded randomized controlled trials in comparison with placebo and with tolterodine. The European Medicines Agency approved the use of fesoterodine in clinical practice in April 2007. The recommended starting dose of fesoterodine is 4 mg per day once (the dose can be increased to 8 mg once). The bioaccumulation of the active metabolite of fesoterodine is 52%. After a single or multiple oral
dose of fesoterodine from 4 mg to 28 mg, plasma concentrations of the active metabolite are proportional to the dose taken . After approximately 5 hours, maximum plasma levels of the drug are reached. Accumulation of the drug in the blood does not occur even with multiple doses of fesoterodine. The results of clinical 12-week studies of fesoterodine in relation to the main symptoms of OAB are presented in Table 4.
In addition to the above-mentioned selectivity for the bladder, an important property of Vesicare and other selective M-anticholinergics is the convenience of administration - once a day, which, along with high safety, significantly increases adherence to treatment on the part of patients. The emergence of such modern drugs gives hope for more effective, safe and convenient treatment of patients with OAB in the future. The results of the studies demonstrate more significant indicators of the effectiveness of M-anticholinergic blockers in combination with a-blockers in various groups of patients, as well as drugs for hormone replacement therapy in menopausal women.
It is likely that in the future it is necessary to move away from the principles of monotherapy for symptoms of a complex of imperative urination disorders, since we see a real way to increase the effectiveness of treatment of this complex disease in complex therapy, including not only various types of pharmacotherapy, but also physical, psychological and other methods of treatment.