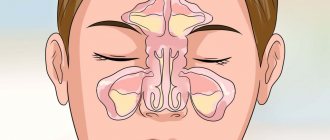
Rheumatoid arthritis
is a chronic inflammatory disease of connective tissue that most often manifests itself in the small joints of the hands and feet.
The danger of the disease lies in its systematic nature and high degree of disability. Being an autoimmune disease, rheumatoid arthritis can affect almost any joint in the body
, and also often leads to
polyarthritis
(affecting 4 or more joints). It can also manifest itself in the organs of the body - the heart, lungs, eyes, kidneys, blood vessels and others. As a result, up to 70% of patients partially or completely lose their ability to work and the ability to self-care, and in especially severe cases left without treatment, even death is possible.
Rheumatoid arthritis affects 1 to 5% of people over 45 years of age, with women getting sick on average 3-5 times more often than men due to their naturally high immunity. Therefore, it is important to be attentive to the slightest manifestations of the disease, diagnose it in time and choose good drugs for rheumatoid arthritis in accordance with the doctor’s prescriptions.
Rheumatoid arthritis is a chronic inflammatory disease of connective tissue
Development of rheumatoid arthritis
Arthritis
is a general term that refers to various types of inflammation and destructive processes occurring inside the joint. Rheumatoid arthritis belongs to the category of autoimmune diseases and involves the progression of inflammatory processes in the joint, the occurrence of which is caused by tissue damage by immune cells for various reasons, attacking the tissues of the body's own.
Inflammatory processes involve degeneration (destruction) of cartilage and further breakdown of bone tissue. Due to the fact that cartilage tissue, as a rule, is not restored, and bone tissue is deformed, during the development of rheumatoid lesions, almost irreversible consequences arise (deformation of joints, a significant decrease in mobility).
Frequent and at the same time severe pain and, as a consequence, inactivity in the absence of treatment inevitably lead to disability of patients.
Symptoms
The initial stage of the disease has virtually no obvious symptoms. Over time, slight stiffness appears in the affected joints. As a rule, it occurs in the morning, as the secretion of glucocorticoids decreases. It is difficult for the patient to move, movements are inhibited. Sometimes you need help getting up. But after 30 minutes - an hour everything returns to normal. The clinic can be rolled out over several months or even years, gradually intensifying.
Primary symptoms also include:
- periodic joint pain;
- loss of appetite;
- increased fatigue.
Second stage
characterized by rapid cell division and thickening of the synovial membrane. There is symmetrical swelling of the joints, the skin in the affected areas has an increased temperature. Sudden pain is also observed, intensifying with active movement. To complete the process, they need the same amount of rest time that was spent moving.
Third stage
― active phase of inflammation involving cartilage and bones. The affected joints begin to deform, which leads to increased pain and loss of motor function.
Rheumatoid arthritis often has concomitant joint diseases, and vague symptoms make differential diagnosis difficult. Among the most beneficial combinations are rheumatism, osteoarthritis and other systemic pathologies of connective tissue. The only specific manifestation of rheumatoid arthritis can be called nodules, so-called subcutaneous formations on the extensor surface. They can be detected by palpation.
Extra-articular manifestations of RA
Pathological processes caused by rheumatoid arthritis that occur outside the joints occur in a third of patients. These symptoms also complicate diagnosis and influence the choice of treatment tactics. Among them:
- Cutaneous vasculitis (ulcerative-necrotic, livedoangiitis, infarction of the nail bed).
- Sjogren's syndrome (damage to the salivary and lacrimal glands).
- Eye lesions (scleritis - inflammation of the deep layer of the eye, episcleritis - inflammation of the connective tissue of the eye).
- Interstitial lung disease (inflammation of the alveoli, pulmonary capillaries and other tissues).
As a result of inflammation accompanying rheumatoid arthritis, pathologies of the cardiovascular, respiratory, and nervous systems may occur. The most serious complication is AA amyloidosis, which causes kidney failure.
Separately, it is worth highlighting various associated diseases that are not directly caused, but are associated with RA. These are coronary heart disease, thromboembolism, anemia, psychoneurological disorders, among which depression deserves attention. Like any other autoimmune disease with chronic inflammation, rheumatoid arthritis affects psychological well-being. The patient is recommended to undergo psychological courses and a comprehensive, comprehensive examination.
Causes of rheumatoid arthritis
Scientists around the world are working to identify the most likely causes of rheumatoid arthritis.
Today, most experts are of the opinion that rheumatoid arthritis is a multifactorial disease, which suggests its development in the presence of a complex of diverse causes.
Possible prerequisites for the occurrence of rheumatoid arthritis may include:
- genetics, namely, a predisposition to disorders of the immune system (antigens have been identified that can lead to the transformation of humoral and cellular immunity);
- the presence in the body of infectious agents that can cause various types of immune changes (more than half of the diagnosed patients have elevated levels of antibodies to the Epstein-Barr virus).
The trigger factors that provoke the appearance of rheumatoid arthritis include:
- hypothermia;
- increased exposure to ultraviolet radiation (prolonged exposure to sunlight);
- intoxication (in particular microbial toxins);
- previous bacterial infections;
- the influence of certain medications;
- disruption of the endocrine system;
- emotional shock.
At the same time, there is an interesting fact that breastfeeding for two or more years significantly reduces the likelihood of developing the disease.
Causes of Arthritis
An unbalanced diet, disrupted sleep and wakefulness, stress and overwork not only reduce the body’s resistance to infections, but also disrupt metabolic processes, as a result of which normal nutrition of the joint is disrupted
. With general exhaustion of the body, various symptoms and types of arthritis can develop - both a sluggish chronic disease and a sharp, unexpected exacerbation. Symptoms and causes of arthritis of the joints depend on the following factors: - excessive physical activity (domestic, professional or sports); - hypothermia or severe overheating in the sun; - metabolic and autoimmune diseases (diabetes mellitus, systemic lupus, psoriasis, gout); - injuries; — uncomfortable working position or bed for sleeping; - presence of allergies; - hormonal reasons; - overweight; - unbalanced diet, poor in vitamins and minerals; — constant stress and psycho-emotional stress; — past infectious diseases (respiratory, intestinal, urogenital, including parasitic), as well as foci of chronic infection in the body (chronic tonsillitis, caries and others); - genetic predisposition (presence of arthritis in relatives); — bad habits (frequent drinking of alcohol, smoking, taking illegal substances).
Main signs and symptoms of rheumatoid arthritis
The first signs of rheumatoid arthritis are morning stiffness in joint movement, accompanied by the onset of inflammatory processes.
Initially, the small joints of the limbs are at risk of tissue resolution, which leads to the appearance of such signs of rheumatoid arthritis as the feeling of spending the night in a corset or tight gloves.
In the initial stage of the disease, the pain is of moderate intensity, but quite noticeable and sometimes comparable to toothache. It is difficult to touch the joints, any perfect movement greatly intensifies the sensation, which forces you to initially take the most comfortable positions.
The initial symptoms of rheumatoid arthritis may persist for a long period of time.
Late stages of development are accompanied by such a sign of rheumatoid arthritis as visually noticeable deformation of the joints. It is worth noting that during this period it is difficult for a person to perform simple household operations, which significantly reduces the quality of life.
In order to simplify the determination of treatment, all symptoms of rheumatoid arthritis are usually classified into two groups:
- Extra-articular manifestations – signal disturbances in the functioning of internal organs:
- decrease in muscle mass;
- thinning and dry skin;
- deformation and fragility of the nail plate;
- hemorrhages on the skin, internal bleeding;
- inflammation and enlargement of lymph nodes.
- Joint manifestations indicate the development of degenerative-dystrophic processes in the joints:
- symmetrical damage to small joints;
- visually noticeable development of the disease (swelling, stiffness, local increase in temperature);
- the appearance of boring pain.
Arthritis symptoms
Manifestations of the disease depend on its clinical form and severity of the process. The main symptoms of arthritis include local manifestations of inflammation in the joint - pain, redness and swelling of surrounding tissues, limited mobility, deformation as pathological changes progress. There is also a local increase in temperature, the affected area becomes hot when touched.
Infectious
The course of the disease depends on the type of pathogen. Often there is a sharp increase in temperature, chills, headache, and weakness. Tuberculous arthritis occurs in a chronic form, is difficult to treat and leads to severe dysfunction of the affected joint. With gonorrhea, as a rule, acute serous inflammation develops. Viral lesions go away after the infection is cured.
Gouty
Gout is a metabolic disorder that is accompanied by the deposition of uric acid salts - urates - in the joints. They penetrate the tissues, forming gouty nodes or tophas. The metatarsophalangeal joints of the thumbs are usually affected first, followed by arthritis in other areas. During an exacerbation of the disease, acute inflammation develops with tissue swelling and severe pain. After several attacks of gout, the joint becomes deformed and its function is impaired.
Rheumatoid
An autoimmune reaction develops with damage to the body’s own tissues, including joints. The causes of the disease have not been precisely established, but it is known that inflammation is triggered by infection in the body. At the onset of the disease, there is an increase in body temperature, the patient is worried about morning stiffness - a gradually passing limitation of mobility after waking up, pain and swelling at the site of inflammation. Symptoms may spontaneously disappear for several months, followed by exacerbation and progression of the disease. Damage to the hand and fingers is typical, but there are cases of atypical reactive arthritis with inflammation of the knee or shoulder joint. Gradually, without treatment, articular cartilage is destroyed, connective tissue grows, subluxations and dislocations occur, leading to disability of the patient.
Traumatic
Develops after injury to large joints - hip, knee, shoulder and others. There is pain, swelling and crunching when moving. With a closed injury and aseptic inflammation, spontaneous recovery is possible. With an open wound, the infection penetrates deep into the tissue and can cause purulent inflammation.
Psoriatic
It is characterized by damage to the terminal interphalangeal joints of the fingers and nails with simultaneous asymmetric damage to several other areas. The course of the disease occurs with relapses and remissions.
Reactive
This form is associated with a toxic-allergic reaction to an infection that develops within a week after a bacterial, viral or fungal infection. It occurs acutely, affecting 1-3 large joints. Characterized by pain at the site of inflammation, redness, swelling of surrounding tissues, and limited mobility. Other symptoms of inflammatory damage to the eye mucosa and urinary tract may also be present.
Juvenile idiopathic
Arthritis of unknown cause in children under sixteen years of age. It is believed that the basis is the genetic predisposition of the child. Prolonged exacerbations alternate with remissions and lead to early disability of the patient.
Possible complications of the disease
If you do not seek qualified help in a timely manner, as well as without treatment for rheumatoid arthritis, there is a high probability of complications, including:
- heart failure/myocardial infarction;
- renal failure;
- violation of metabolic processes;
- inflammation of the serous membranes of internal organs;
- the occurrence of bronchopleural fistulas (a direct channel between the bronchial tree and the pleural cavity).
How the disease develops
Rheumatoid arthritis is an autoimmune disease, that is, associated with a malfunction of the immune system. In arthritis, immune cells mistakenly mistake joint cells for foreign elements - viruses, bacteria - and try to destroy them. This process continues for years..
Often the disease begins with damage to the knee joint. At the beginning of the disease, the patient feels weak, unwell, loses appetite, loses weight, and the temperature can rise to 37-39 degrees. In this case, joint problems fade into the background or are completely absent. As the disease develops, more and more joints are involved in the process, and after treatment of exacerbations, the joints become less mobile and deformed.
Over time, symptoms associated with damage to internal organs and systems appear: lungs, heart, blood vessels, kidneys, eyes, salivary glands. With rheumatoid polyarthritis, dense subcutaneous nodules often form.
Classification of rheumatoid arthritis
The development of rheumatoid arthritis is classified into stages. It is important that in the early stages the disease can be quite successfully treated with medications, but in the later stages they may be ineffective. The prognosis of disability depends on the stage of the disease.
In addition to the clinical ones, there are also radiological stages of rheumatoid arthritis. Let's look at it in detail.
First stage (initial)
It proceeds quite favorably and practically does not manifest itself in any way. As a rule, there are no painful sensations, the general condition of the body is satisfactory.
It is almost impossible to identify the disease on your own.
The main symptoms of early stage rheumatoid arthritis are:
- discomfort in the joints, barely noticeable pain;
- compaction with a finger (visually noticeable thickening);
- compaction of periarticular tissues;
- stiffness of movement mainly in the morning.
X-ray manifestations:
- thinning of bone tissue;
- extremely rarely - the formation of light areas on the affected tissue.
Treatment for early-stage rheumatoid arthritis is quite simple, and the prognosis is favorable.
Second stage
It has a more pronounced clinical picture. Diagnosis of rheumatoid arthritis is carried out mainly at this stage.
Among the most pronounced symptoms of rheumatoid arthritis of the second stage are:
- damage to several groups of joints at once;
- the occurrence of quite severe pain, which weakens with active movements and stress;
- feeling of stiffness, as if “the body has gone numb”;
- visually noticeable changes (local redness of the skin).
X-ray manifestations:
- changes in bone tissue according to the type of erosion;
- cartilage deformation;
- swelling and inflammation of the joint capsule.
Treatment of stage 2 rheumatoid arthritis is predominantly medicinal. The prognosis is favorable.
Third stage
Characterized by serious changes. There are pronounced pains and limited joint mobility.
Signs of stage three rheumatoid arthritis are:
- spread of the disease to large joints of the body;
- local increase in temperature, feeling of heat;
- formation of subcutaneous nodules (mainly near the affected joints);
- noticeable deformation of cartilage tissue;
- muscle atrophy, loss of joint mobility.
X-ray manifestations:
- thinning of bone tissue, the occurrence of erosions;
- noticeable atrophy of the muscular frame;
- joint deformation;
- salt deposits, as well as calcification of joints.
Treatment of rheumatoid arthritis at this stage is carried out only in a hospital setting. The prognosis is conditionally unfavorable.
Fourth (terminal) stage
An extremely severe course of the disease, accompanied by a large number of complications.
Diagnosis of rheumatoid arthritis at this stage determines such signs as:
- severe pain that prevents rest;
- pain in the eye sockets, chest discomfort;
- partial or complete loss of sensation in the limbs;
- significant decrease in motor activity;
- spread of the inflammatory process to large muscles;
- gastrointestinal tract damage;
- the occurrence of a large number of ulcers/rashes.
X-ray manifestations:
- obviously noticeable osteoporosis;
- many erosions/cysts;
- tissue fusion;
- total deformation (not subject to restoration).
Treatment of stage four rheumatoid arthritis is only in a hospital setting. The prognosis is extremely unfavorable.
Symptoms and types of arthritis
There are several bases for classifying arthritis, which are used in making a diagnosis, clarifying the causes and symptoms of arthritis of the joints, and selecting treatment.
Due to origin
Based on their origin, arthritis is caused by:
- Infectious or parasitic infection of the body
. Reactive inflammation of the joints and periarticular tissues, as well as other symptoms of arthritis, can occur 4-6 weeks after the disease, as the body’s response to the vital activity of the pathogens themselves or a massive amount of antigens produced to combat them. Infectious arthritis also includes generalized pathologies that affect more than 3 joints and are associated with chronic infections (tuberculosis, syphilis, viral hepatitis, HIV and others). Infectious arthritis can also be triggered by the unwanted growth of microflora in the cecum in the postoperative period, as well as infection by worms or protozoa. In rare cases, inflammatory pathology occurs as a response to vaccination (usually occurs in children). With penetrating wounds and injuries, which are accompanied by ruptures of blood vessels, as well as with bites of blood-sucking insects in the periarticular area, direct infection of the joint capsule is possible. - Non-infectious reasons
. Symptoms and causes of arthritis of the joints may depend on the presence in the body of such pathologies as: - neoplasms (arthritis develops due to metastasis to articular or periarticular tissues or due to the body’s immune response to a tumor); - diseases of the blood and blood vessels (anemia, hemorrhages); - pancreatitis, pancreatic cancer (due to the influence of enzymes on the synovium of the joint); — decompression sickness due to non-compliance with safety precautions when diving; - metabolic disorders (diabetes mellitus, gout); - hormonal changes in the body (hormonal imbalances, menopause in men and women, age-related changes); - allergies to food, drugs, vaccines or chemicals, rejection of prostheses by the body; — bruises, sprains and ruptures of ligaments, muscles, tendons, fractures, as well as other injuries (including repeated microtraumas, for example, when working with vibration equipment); - wear of the joint due to instability of chondrocytes and other pathologies of cartilage tissue; - monotonous loads and the unfavorable influence of climatic and sanitary conditions in the workplace (in this case we can talk about the so-called benign arthritis, which goes away by itself when conditions change). - Unspecified reasons
. As a rule, these include secondary arthritis, which occurs against the background of autoimmune diseases (including hepatitis, rheumatoid polyarthritis, amyloidosis, systemic vasculitis, and others). Since the causes of these diseases are still not clear, the accompanying symptoms and types of arthritis also have an unspecified etiology.
According to clinical manifestations
Arthritis can affect both small and large joints, being limited to one joint or affecting several at once. Therefore, rheumatologists divide the disease into the following types:
- monoarthritis
(affects only one joint); - oligoarthritis
(observed in 2-3 joints); - polyarthritis
(occurs in 4 or more joints at the same time).
According to symptoms
According to the severity of arthritis symptoms:
- acute arthritis
(characterized by sudden onset, severe pain and rapid progression); - arthritis with a chronic course
(develops slowly, periods of remission alternate with periods of exacerbation, pain is less pronounced than with acute arthritis).
There are many symptoms of arthritis
Diagnosis of rheumatoid arthritis
You should go for a diagnosis of rheumatoid arthritis if the following symptoms occur:
- painful symmetrical swelling/edema of several joints;
- the occurrence of morning stiffness;
- presence of subcutaneous nodules;
- changes on the radiograph (detection of osteoporosis/erosions/cysts).
In order to clarify the suspected diagnosis, the following methods are used:
- MRI (magnetic resonance imaging) – makes it possible to determine the condition of the periarticular tissues;
- puncture (extracting a sample of joint (synovial) fluid) - helps determine the presence of specific cells and leukocytes.
Arthritis stages
Determining the stage of arthritis is an important diagnostic step
, which allows you to select appropriate treatment and monitor the rate of disease progression. Experts distinguish 4 stages, depending on the severity of the symptoms of arthritis, damage to cartilage and bone tissue.
1st stage of arthritis
Arthritis can begin unnoticed by the patient himself, because most symptoms of joint arthritis appear only at the 2nd stage. Particularly attentive patients note slight stiffness in the diseased joints and slight swelling, which is not helped by reducing salt in the diet. Mild pain may be felt when flexing and extending the joint, especially sharply. Patients complain of increasing fatigue and decreased stamina.
The initial stage of disease of the knee or shoulder joint is especially insidious
- in this case, the symptoms of arthritis are usually attributed to age-related changes or fatigue after a hard day.
Parents can notice grade 1 arthritis in a child by a decrease in his activity, lack of interest in games, frequent falls and awkwardness when performing physical exercises. A sick child does not like to run, avoids physical work, is capricious and whines if he is forced to exercise.
Although difficult to diagnose, stage 1 arthritis is the most treatable
. With a late onset of the disease, the prognosis is favorable: therapy may result in complete restoration of cartilage tissue.
Stage 2 arthritis
At stage 2, the pain becomes difficult to ignore. The pain syndrome intensifies in the morning and at night and can disrupt the patient’s healthy sleep. The swelling is clearly visible from the outside, but the patient himself may notice an unusual knotty or spindle-shaped shape of the fingers, thickening of the limb (associated with the accumulation of synovial fluid) in the joint and other visual signs of inflammation. At the 2nd stage of arthritis of the leg joints, gait disturbances and pain when walking are added to the symptoms.
At stage 2, irreversible changes and erosions may appear on the synovial membrane
.
Without the use of chondroprotectors - for example, Artracam sachet
- it is quite difficult to stop or slow down the process of cartilage destruction.
Stage 3 arthritis
At stage 3, visual changes and pain become significant. The joint becomes deformed, and when performing movements there is severe stiffness and pain. The simplest everyday activities cause difficulties for the patient. Even in the absence of loads, during rest, diseased joints continue to bother the patient. At this stage, most patients partially lose their ability to work - they may be assigned a disability.
Stage 4 arthritis
At the last stage of arthritis, the affected joints completely lose mobility
.
Pain torments patients continuously, creating a serious psycho-emotional burden. At this stage, only surgical treatment is indicated, since the cartilage tissue is almost completely destroyed, and the edges of the bones begin to grow together. At stage 4, the disease is irreversible
, accompanied by loss of the ability to self-care and/or independent movement, and persistent contractures.
There are 4 stages of arthritis
To make a diagnosis and exclude similar diseases, a rheumatologist performs an initial examination, palpation (palpation) of the affected joint, as well as motor tests. At the first appointment, a medical history is taken, the patient is asked about the symptoms of arthritis, after which the specialist issues a referral for tests and hardware examinations. Among them:
- general and biochemical blood test, rheumatic factor test;
- X-ray examination (in 2 standard projections);
- puncture and analysis of synovial fluid;
- arthrography (x-ray examination with preliminary administration of a contrast agent - usually performed during an inflammatory process in the shoulder or knee joint);
- arthroscopy (insertion of a sensor directly into the joint cavity through a microincision);
- Ultrasound (for large joints such as the shoulder or hip);
- serological reactions to a pathogen or antibodies to an infectious agent.
Thus, X-ray examination helps to determine the width of the joint space, osteoporosis, proliferation of osteophytes, the presence of erosions, dislocations, subluxations, and deformities. If changes are not clearly visible or bone growths interfere with their assessment, and also if there is a need to examine soft tissues, additional computed tomography (CT) or magnetic resonance imaging (MRI) may be prescribed. Ultrasound also helps to assess the extent of the disease and the changes caused by it.
Be healthy and may arthritis pass you by!
Images designed by Freepik
Treatment of rheumatoid arthritis with non-drug methods
Despite the fact that the disease cannot be completely cured, fighting it makes sense and, with the right approach, gives the best possible results.
The key objective of non-drug and drug therapy is:
- elimination of symptoms;
- achieving stable and long-term remission;
- inhibiting the activity of autoimmune reactions;
- preventing or slowing down the manifestation of complications.
Physiotherapy
Physiotherapeutic methods are aimed at accelerating tissue repair/healing, as well as supporting muscle tone and maximizing joint mobility in rheumatoid arthritis.
Physiotherapy includes:
- electrophoresis/phonophoresis (exposure to electric field/ultrasound);
- balneotherapy (mineral water baths);
- mud therapy.
It is best if the therapy is carried out in an inpatient setting.
Massage
An excellent treatment method, the use of which is necessary during the period of remission of the disease. The duration of the course and the duration of the sessions are determined by the nature of the disease.
Procedures should be performed only by a professional massage therapist, after consultation with the attending physician.
Therapeutic exercise (physical therapy)
Helps maintain mobility and also locally activates metabolic processes by improving blood circulation.
The set of exercises is selected in accordance with the current stage of the disease and taking into account the recommendations of the attending physician.
Orthopedic surgeries
Possibility of restoring the functionality and structure of joints. Today the following solutions are available:
- arthroscopy is a minimally invasive intervention (involves pinpoint punctures) performed to treat joint damage;
- endoprosthetics - replacement of components or an entire joint, providing mobility.
Pharmacotherapy of rheumatoid arthritis from the perspective of evidence-based medicine: new recommendations
R
Eumatoid arthritis (RA) is an autoimmune disease of unknown etiology, characterized by symmetrical erosive arthritis (synovitis) and a wide range of extra-articular (systemic) manifestations. RA is an extremely common disease, affecting approximately 1% of the world's population. The cardinal signs of RA include steadily progressive joint damage (chronic pain, deformation, dysfunction), leading to disability and even a decrease in the life expectancy of patients (Fig. 1).
Rice. 1. Rheumatoid arthritis: variants of the course
The development and progression of RA is determined by a complex combination of genetically determined and acquired defects (“imbalance”) of normal (immuno) regulatory mechanisms that limit the pathological activation of the immune system in response to potentially pathogenic and often physiological stimuli. This leads to a rapid transformation of the physiological (protective) acute inflammatory response into the chronic progressive inflammation that is an integral feature of RA. In RA, the Th1 type of immune response predominates, characterized by hyperproduction of “pro-inflammatory” cytokines, such as interleukin (IL)-1, tumor necrosis factor (TNF)-a (Fig. 2). It should be especially emphasized that the progression of RA is a dynamically developing process, which (both from the point of view of pathogenetic mechanisms and clinical, instrumental and laboratory manifestations) is conventionally divided into several stages:
Rice. 2. The role of cytokines in the development of rheumatoid arthritis
- early (asymptomatic) stage, characterized by vascular and cellular activation;
- advanced (rapid chronicization of inflammation) stage, manifested by impaired angiogenesis, endothelial activation, cell migration, infiltration of synovial tissue by activated CD4+ T lymphocytes, formation of rheumatoid factors and immune complexes, synthesis of “pro-inflammatory” cytokines, prostaglandins, collagenase, metalloproteinases;
- late stage, which is characterized by somatic mutation and defects in apoptosis of synovial cells.
The etiology of RA is unknown
, which makes it impossible to carry out effective etiotropic therapy.
Therefore, treatment of RA remains one of the most difficult problems of modern clinical medicine and pharmacology. However, deciphering the pathogenetic mechanisms underlying rheumatoid inflammation served as the basis for the development of the concept of “pathogenetic (basic) therapy
,” which was formed more than 10 years ago. The “basic” drugs include a large number of drugs that differ in chemical structure and pharmacological properties. They are united by the ability, to a greater or lesser extent and through various mechanisms, to suppress inflammation and/or pathological activation of the immune system. The progress made in the treatment of RA in recent years is very clearly visible when comparing the International Guidelines (American College of Rheumatology) for the pharmacotherapy of RA, published in 1996 and 2002. During this time, new “symptomatic” (COX-2 inhibitors) and basic (leflunomide, “anti-cytokines”) drugs have been developed (Fig. 3), most importantly, the concept of “early” aggressive therapy for RA has been more clearly formulated.
Rice. 3. Modern pharmacotherapy of rheumatoid arthritis
Treatment of rheumatoid arthritis
The main objectives of pharmacotherapy for RA are presented in Figure 4. In recent years, it has become especially obvious that the highest rate of increase in radiological changes in the joints is observed precisely in the early stages of RA
, which correlates with a poor prognosis. Since the use of “basic” drugs for “early” RA makes it possible to modify the course of the disease, treatment of RA (as well as many other chronic human diseases, such as diabetes mellitus, arterial hypertension, coronary artery disease, etc.) should begin as early as possible, preferably during the first 3 months after making a definite diagnosis of RA (Fig. 5). This is especially important in patients with risk factors for poor prognosis, which include high titers of rheumatoid factor, a marked increase in ESR, damage to more than 20 joints, the presence of extra-articular manifestations (rheumatoid nodules, Sjogren's syndrome, episcleritis and scleritis, interstitial lung disease, pericarditis, systemic vasculitis, Felty's syndrome). For example, in seropositive patients with polyarthritis at the onset of the disease, the likelihood of severe erosive joint damage during the first two years of the disease is extremely high (70%).
Rice. 4. Objectives of therapy for rheumatoid arthritis
Rice. 5. The importance of early aggressive treatment for rheumatoid arthritis
At the same time, attention should be paid to the difficulties of differential diagnosis of “early” RA (< 6–12 months from the onset of symptoms) from a number of other rheumatic and non-rheumatic diseases (influenza, rubella, parvovirus B19, measles, hepatitis, Lyme borreliosis, seronegative spondyloarthropathy , microcrystalline arthritis, rheumatic fever, CTD, osteoarthritis, polymyalgia rheumatica, systemic vasculitis, tumor arthritis, etc.), which can begin with “rheumatoid-like” joint damage. Below are summarized clinical and laboratory signs that allow one to suspect the onset of RA, in the presence of which the patient should be immediately referred for consultation to a rheumatologist (Fig. 6). After making a reliable diagnosis of RA (Fig. 7), all patients must undergo basic clinical (Fig. 8), laboratory and instrumental (Fig. 9) examination.
Rice. 6. Clinical signs to suspect rheumatoid arthritis
Rice. 7. Criteria for the diagnosis of rheumatoid arthritis
Rice. 8. Clinical examination of patients with rheumatoid arthritis
Rice. 9. Laboratory and instrumental examination of patients with rheumatoid arthritis
At each patient visit, the rheumatologist should assess the activity of the disease (Fig. 10). International criteria for the effectiveness of therapy and clinical remission have been developed. According to the American College of Rheumatology (ACR) criteria, evidence of treatment effectiveness may include a 20% improvement (ACR20) in swollen and painful joint scores.
, along with a 20% improvement in 3 out of 5 of the following parameters: overall assessment of the effectiveness of treatment in the opinion of the doctor and the patient, assessment of the intensity of pain in the opinion of the patient, assessment of the degree of disability and “acute-phase” indicators (Fig. 11). Assessment of radiographic progression using the Sharp method allows one to evaluate the effect of therapy on the outcome of the disease (Fig. 12).
Rice. 10. Assessment of the activity of rheumatoid arthritis
Rice. 11. Criteria for treatment effectiveness (ACR20 / ACR50 / ACR70)
Rice. 12. Modified Sharp method
Nonsteroidal anti-inflammatory drugs
The general plan for the management of RA patients is presented in Figure 13. The main method of symptomatic treatment of RA is the prescription of non-steroidal anti-inflammatory drugs
(NSAIDs)
to reduce pain and inflammation in the joints
.
Conventionally, NSAIDs are divided into short-lived (diclofenac, ketoprofen, lornoxicam (Xefocam),
etc.) (< 6 hours) and long-lived (piroxicam, naproxen, etc.) (> 6 hours). However, there is no clear relationship between the plasma half-life of NSAIDs and its clinical efficacy. “Short-living” drugs can accumulate for a long time and in high concentrations in the area of inflammation, for example, in the joint cavity. Therefore, one or two doses of “short-living” drugs are often as effective as multiple doses. When choosing an NSAID, a number of factors must be taken into account: effectiveness, tolerability, safety and cost of the drugs. In patients with risk factors for complications from the gastrointestinal tract, the drugs of choice are the so-called selective cyclooxygenase (COX)-2 inhibitors. A limitation of NSAID monotherapy is that these drugs rarely completely suppress the clinical manifestations of arthritis, do not affect the progression of joint damage, and cause side effects, especially in the elderly. Risk factors for gastrointestinal side effects include older age (over 75 years), a history of peptic ulcers, concomitant use of glucocorticosteroids, severe concomitant diseases, taking high doses of NSAIDs or simultaneous use of several drugs. For the prevention and treatment of NSAID-induced gastrointestinal lesions, H2-histamine receptor blockers (high doses only), proton pump inhibitors and misoprostol can be used. It should be emphasized: although the symptoms of dyspepsia, which very often occur while taking NSAIDs, are often relieved by low doses of H2-histamine receptor blockers, their use not only does not reduce, but may even increase the risk of severe complications from the gastrointestinal tract (perforations, perforated ulcers and gastric bleeding ). Although selective COX-2 inhibitors are significantly less likely to cause gastrointestinal damage than “standard” NSAIDs, their use may also cause undesirable effects, including symptoms of dyspepsia, delayed healing of gastric and duodenal ulcers, fluid retention, and increased blood pressure. In addition, one study showed that RA patients taking a selective COX-2 inhibitor (rofecoxib) had a higher incidence of thrombotic complications (myocardial infarction) than patients taking naproxen. However, data from other studies indicate that the use of other selective COX-2 inhibitors, meloxicam and celecoxib, does not lead to an increase in the incidence of cardiovascular thrombosis compared with patients taking “standard” NSAIDs. The use of both “standard” NSAIDs and selective COX-2 inhibitors should be carried out with extreme caution in patients with reduced intravascular volume or edema associated with congestive heart failure, nephrotic syndrome, cirrhosis and with an increase in creatinine of more than 2.5 mg%.
Rice.
13. Management of patients with rheumatoid arthritis Glucocorticoids
Treatment with low (< 10 mg/day) doses of glucocorticoids (GCS) often allows adequate control of rheumatoid inflammation
, not inferior in this regard to “basic” antirheumatic drugs with an acceptable toxicity profile, a decrease in the rate of radiological progression in patients with “early” active RA (especially when combined with methotrexate).
The administration of GCS is especially indicated in patients who do not respond to NSAIDs or have contraindications for their administration in an adequate dose. Unfortunately, in many patients, an attempt to discontinue GCS leads to an exacerbation of synovitis, even despite the use of “basic” drugs, that is, a functional glucocorticoid dependence develops. Treatment with low (<10 mg/day) doses of glucocorticoids (GCS) is often not inferior in this regard to “basic” antirheumatic drugs, has an acceptable toxicity profile, and reduces the rate of radiological progression in patients with “early” active RA (especially when combined with methotrexate) .
The administration of GCS is especially indicated in patients who do not respond to NSAIDs or have contraindications for their administration in an adequate dose. Unfortunately, in many patients, an attempt to discontinue GCS leads to an exacerbation of synovitis, even despite the use of “basic” drugs, that is, a functional glucocorticoid dependence develops. Pulse therapy GCS
(methylprednisolone, dexamethasone) allows you to achieve rapid (within 24 hours), but short-term (3-12 weeks) suppression of the activity of the inflammatory process, even in patients resistant to previous therapy. However, the effect of pulse therapy on the radiographic progression of joint damage has not been proven.
Local GCS therapy
has an auxiliary value. Its goal is to suppress active synovitis at the onset of the disease and its exacerbations in 1 or more joints, and improve joint function. However, glucocorticoids affect only the local process (and RA is a systemic disease) and cause only temporary improvement. The most effective are long-acting glucocorticoids (triamcinolone, methylprednisolone) and especially betamethasone. It should be borne in mind that not every exacerbation of monoarthritis in RA is associated with the activity of the disease itself; it may be a manifestation of infectious or microcrystalline arthritis. It is not recommended to perform repeated injections of GCS into the same joint more than once every three months. The need for more frequent injections may reflect the inadequacy of “background” therapy.
Although RA patients tend to develop osteoporosis regardless of glucocorticoid therapy, patients receiving even low doses of oral corticosteroids have an increased risk of osteoporotic fractures. This dictates the need for periodic determination of bone mineral density (BMD) using bone densitometry methods (approximately once every 12 months) and mandatory administration of calcium supplements (1500 mg) and colecalciferol (400–800 IU per day) from the moment of GCS administration. If effectiveness is insufficient, it is advisable to use other antiosteoporetic drugs, such as bisphosphonates and calcitonin.
Basic therapy
The effectiveness of “basic” drugs in the form of mono (Table 1) or combination (Table 2) therapy in controlling the symptoms of joint damage, a positive effect on radiological progression, functional status and quality of life, has been strictly proven in placebo-controlled studies. It is believed that their use can reduce the overall cost of medical care for patients, and early initiation of adequate “basic” therapy can help increase the life expectancy of RA patients. Indications for immediate (within 3 months) prescription of “basic” drugs
is definite RA, in which, despite the use of NSAIDs in adequate doses, joint pain, morning stiffness (or general malaise), active synovitis, persistent increase in ESR or CRP, and/or signs of erosive joint damage persist.
Characteristics of the “basic” drugs used for the treatment of RA are presented in Tables 3 and 4. “Basic” therapy reduces the need for NSAIDs and glucocorticoids (and therefore the likelihood of developing side effects that occur during treatment with these drugs), improves the quality of life and long-term prognosis.
The “disadvantages” of basic therapy include the need for careful monitoring of the development of side effects (Table 5–7). The choice of one or another “basic” drug depends on a number of subjective and objective factors and should be individualized whenever possible. Unfortunately, relatively few studies have been devoted to comparing the effectiveness and safety of various disease-modifying drugs and combination therapy with several disease-modifying drugs. In women of childbearing age, while taking most of the “basic” drugs, effective contraception is necessary, and in the event of pregnancy or breastfeeding, the regimen for taking the “basic” drugs must be modified. Given the high safety, many rheumatologists prefer to start “basic” therapy with hydroxychloroquine
or
sulfasalazine
, the effectiveness of which (especially in patients with “early” RA) with moderate activity has been proven in many studies. Although hydroxychloroquine monotherapy does not slow the radiographic progression of joint damage, it is generally quite effective in improving the long-term prognosis of the disease. Sulfasalazine suppresses inflammation more quickly than hydroxychloroquine within the first month of starting therapy. In addition, during treatment there is a slowdown in the radiological progression of the disease. Side effects such as nausea and abdominal pain are moderate and usually develop during the first few months of therapy. The incidence of side effects decreases with slowly increasing the dose of the drug. However, leukopenia and other more severe side effects can develop during any period of treatment, which dictates the need for periodic laboratory examination. If there is no clinical effect within 4 months, it is necessary to prescribe another “basic” drug.
In patients with “active” RA or those with risk factors for poor prognosis, the drug of choice is methotrexate
, which has the most favorable efficacy/toxicity ratio.
This allows us to consider it as the “gold standard” of pharmacotherapy for RA
when testing the effectiveness and safety of new “basic” drugs. There is evidence that more than 50% of RA patients can take methotrexate for more than 3 years, which is significantly longer than other “basic” drugs. In general, discontinuation of methotrexate treatment is more often associated with the development of side effects than with treatment failure. The incidence of many side effects (stomatitis, nausea, diarrhea, alopecia) can be reduced by prescribing folic acid, without loss of effectiveness. Relative contraindications for prescribing methotrexate are liver disease, significant renal impairment, lung disease and alcohol abuse. Although the most common side effect is increased liver enzymes, the risk of severe liver damage is low. Liver biopsy is indicated only in patients with persistent increases in liver enzyme levels after discontinuation of the drug.
Patients who are contraindicated for treatment with methotrexate, who fail to achieve sustained clinical improvement during treatment with methotrexate (up to 25 mg/week) or develop side effects, are advised to prescribe the new “basic” drug leflunomide
,
“biological” agents
, or other “basic” drugs in the form of mono- or combination therapy (Fig. 14). A decrease in RA activity and a slowdown in radiological progression during treatment with leflunomide is expressed to the same extent as with methotrexate. In addition, leflunomide can be successfully used in combination with methotrexate in patients in whom methotrexate monotherapy is insufficiently effective. However, in patients receiving combination therapy with methotrexate and leflunomide, an increase in the concentration of liver enzymes is observed significantly more often than during leflunomide monotherapy. It must be borne in mind that since the metabolism of leflunomide depends on the hepatic enteric circulation, this drug has a very long half-life and can remain in the body for more than 2 years. To eliminate it, it is recommended to use cholestyramine. Contraindications for the use of leflunomide are liver disease, immunodeficiency, and the use of rimfapicin, which causes an increase in the concentration of leflunomide.
Rice. 14. Tactics for managing patients with rheumatoid arthritis when methotrexate is ineffective
Effective drugs for the treatment of RA include gold salts. D-penicillamine and cyclosporine A are now used less frequently, primarily due to side effects. For example, against the background of D-penicillamine, the development of autoimmune syndromes (myasthenia gravis, Goodpasture syndrome, polymyositis) has been described. Long-term use of cyclosporine A is limited by the development of arterial hypertension and dose-dependent renal dysfunction, which sometimes persists after discontinuation of the drug. In addition, many drugs can cause an increase in serum levels of cyclosporine A and thus contribute to the nephrotoxicity of the latter. Therefore, cyclosoporin A is recommended to be used primarily in RA patients who are “refractory” to other “basic” drugs.
Anticytokine therapy
One of the most striking achievements in the pharmacotherapy of RA is associated with the development of a fundamentally new group of drugs, which are called “biological” agents, the mechanism of action of which is associated with the suppression of the synthesis of “pro-inflammatory” cytokines – TNF-a and IL-1, playing, as already noted, a fundamental role in the immunopathogenesis of RA. Currently, 3 groups of drugs are used in the treatment of RA, 2 of which are monoclonal antibodies (mAbs) to TNF-a - infliximab (Remicade)
and recombinant soluble TNF-a receptor coupled to the Fc fragment of IgG (Etanercept) - inhibit the synthesis and biological effects of TNF-a and recombinant soluble IL-1 antagonist (Anakinra), which suppresses the functional activity of IL-1. Data have been obtained that the use of biological inhibitors of TNF-a and IL-1 can reduce the activity of the immunopathological process and achieve a clinical effect, improve the quality of life and slow down the radiological progression of joint damage, even in patients resistant to previous therapy with standard “basic” drugs. All drugs are effective in combination with methotrexate in patients with active RA who do not respond to methotrexate monotherapy. Infliximab is approved for use in combination with methotrexate, and Etanercept and Anakinra are approved for use as monotherapy or in combination with other “background” drugs, with the exception of “biological” TNF-a inhibitors.
Extracorporeal procedures
In the complex treatment of severe RA, resistant to standard “basic” therapy, it is advisable to prescribe various extracorporeal procedures, including plasmapheresis
and
immunoadsorption using Staphylococcus protein
A.
Combination therapy
Since monotherapy with “basic” drugs in many cases does not control the progression of RA, the possibility of using combination therapy with several “basic” drugs
(Table 2). The most well-studied combinations are cyclosporine and methotrexate and “triple” therapy with methotrexate, sulfasalazine and hydroxychlorquine. It should be emphasized, however, that although the combination of cyclosporine and methotrexate is more effective than methotrexate monotherapy, with long-term use in some patients the development of arterial hypertension and an increase in creatinine levels was noted.
A more promising direction for the treatment of RA seems to be combination therapy with “basic” (methotrexate, leflunomide) and “biological” (infliximab, etc.) drugs.
Non-pharmacological treatments
To prevent the progression of joint deformation, the pattern of motor activity should be changed. For example, to prevent the development of ulnar deviation, the hand should perform radial rather than ulnar flexion: open the tap and turn the key in the lock with the left hand rather than the right one, etc. An important component of RA treatment is physical therapy
.
For mild or moderate activity, various methods of physical therapy
, especially laser irradiation of the affected joints.
Sanatorium-resort treatment is indicated only for patients with minimal RA activity or in remission. as orthopedic aids
- special devices made of thermoplastic, worn while sleeping and holding the joint in the correct position. Prosthetics of hip and knee joints and surgical treatment of deformities of the hands and feet are widely used.
Thus, over the past 5 years, significant progress has been made in the treatment of RA, significantly greater than in all previous years.
We hope that the practical use of the presented recommendations, based on international experience in the treatment of RA and “evidence medicine,” will significantly improve the prognosis of this serious disease. Literature:
1. Nasonov E.L. Anti-inflammatory therapy for rheumatic diseases. Moscow, M-CITY Publishing House, 1996, 345 pp.
2. Nasonov E.L. Non-steroidal anti-inflammatory drugs (Prospects for use in medicine) Moscow, Anko, 2000 Moscow,
3. Nasonov E.L. Nonsteroidal anti-inflammatory drugs for rheumatic diseases: standards for the treatment of breast cancer, 2001; 9, 7–8;265–270.
4. Nasonov E.L. Prospects for pharmacotherapy of inflammatory rheumatic diseases: monoclonal antibodies to tumor necrosis factor. RMJ, 2001, 9, 7–9, 280–284
5. Nasonov E.D., Skripnikova I.A., Nasonova V.A. The problem of osteoporosis in rheumatology. Moscow. "STIN", 1997; 429 pp.
6. Sigidin Ya.A., Lukina G.V. Rheumatoid arthritis. Moscow, ANKO, 2001, 328 pp.
7. Harris E,D. Jr. Rheumatoid Arthritis: pathophysiology and implications for therapy. N.Engl. J Med 1990;322:1277–1289
8. American College of Rheumatology Ad Hoc Commitee on Clinical Guidelines. Guidelines for the management of rheumatoid arthritis. Arthritis Rheum 1996;39:713–722.
9. American College of Rheumatology Ad Hoc Commitee on Clinical Guidelines. Guidelines for monitoring drug therapy in rheumatoid arthritis. Arthritis Rheum 1996;39:723–731.
10. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the Management of Rheumatoid Arthritis. 2002 Update. Arthritis Rheumatism.2002;46:328–346.
Treatment of rheumatoid arthritis with drugs
How to treat rheumatoid arthritis using medications can only be determined by the attending physician who has a complete clinical picture of the patient’s disease.
Treatment of rheumatoid arthritis with drugs is carried out under the close supervision of a specialist and is adjusted in accordance with the existing/absent progress.
Chondroprotectors
A wide group of drugs that promote the regeneration of connective tissue and improve the condition of cartilage. Available in various forms (tablets/ointments).
Frequently prescribed ones include: “Artracam”, “Mukosat”, “Chondrolone”.
Antispasmodics
Helps relieve spasms of smooth muscles surrounding inflamed joints.
The most effective are “Spazmalgon”, “Trigan”, “Maxigan”.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
They have an anti-inflammatory effect and help inhibit the activity of the enzyme that causes destructive processes. The most commonly prescribed and at the same time very effective drug is Artradol.
Biological agents
Protein-based drugs. The key purpose is to suppress inflammatory processes due to its effect on the components of the immune system.
The most effective are: “Halofuginon”, “Humira”, “Orencia”.
Treatment
Treatment of arthritis is aimed at eliminating the cause of the disease and risk factors that contribute to the development of inflammation, relieving symptoms, improving metabolism in the affected joint, and preserving its function.
This can be achieved through the use of medications, physiotherapy, physical therapy and massage. In advanced cases, with purulent processes, dislocations and subluxations, surgical intervention may be required. If the joint is completely destroyed, it can be replaced with an artificial one - endoprosthetics.
Conservative therapy, depending on the form of arthritis, includes the use of tablets, ointments and injections of various groups of drugs:
- antibiotics for bacterial infections;
- non-steroidal anti-inflammatory drugs and hormones;
- chondroprotectors – agents that improve the quality of joint tissue;
- painkillers;
- vitamins, microelements and amino acids.
Author:
Pugonina Tatyana Alekseevna, Therapist
Nutrition
Compliance with the principles of a healthy diet helps to consolidate the favorable results of successful treatment and maintain remission for as long as possible. A diet for rheumatoid arthritis and a transition predominantly to plant foods helps to significantly reduce the exacerbations that occur.
How to treat rheumatoid arthritis with diet? Experts recommend eliminating allergenic foods (for example, tomatoes and eggplants), as well as introducing more vitamins and animal proteins, which helps reduce muscle loss. Preference should be given to lean meats, as well as sea fish and baked foods.
In addition, it is recommended to give up bad habits, since any intoxication can provoke an exacerbation.