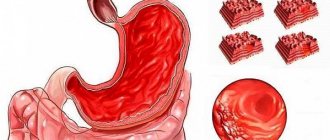
Erosive gastritis is an inflammatory disease. It affects the gastric mucosa, causing the formation of erosions of various sizes on it. These formations do not penetrate deep into the walls of the stomach and do not leave marks after healing.
It is the depth of penetration into the stomach wall that distinguishes erosive gastritis from an ulcer. The latter disease can affect not only the inner surface, but also deeper tissues and even the muscle layer.
Erosive gastritis is dangerous due to complications. Statistics show that a fifth of gastric bleeding is associated with erosions on the mucous membrane. Therefore, in modern gastroenterology, this form of the disease is increasingly referred to as “hemorrhagic gastropathy or gastritis” and “papular gastropathy.”
Erosive gastritis is a common pathology. A quarter of examinations for heartburn, abdominal pain, and nausea end with this diagnosis. The disease affects both men and women. The disease can develop at any age. True, young children are diagnosed much less often.
Studies show that in recent years, cases of diagnosing erosive gastritis have become more frequent. According to some studies, the incidence of diseases has increased tenfold. Scientists attribute this to an increase in the amount of stress, disruption of diet and quality of nutrition. This may also be due to improved diagnostic methods. When carrying out preventive examinations, the disease can be identified at the initial stage, even in the absence of complaints.
Consult a gastroenterologist
Don't delay treatment
Causes of erosive gastritis
In the vast majority of cases, the development of the disease is caused by Helicobacter pylori. However, doctors tend to believe that the mere presence of bacteria in the stomach is not enough. For the disease to appear, a combination of several factors is necessary.
The bacterium Helicobacter pylori was isolated in 1981. It is resistant to acidic conditions and is capable of secreting enzymes that weaken the protective environment of the stomach walls. By multiplying, this microorganism causes local inflammation and the formation of erosions. Helicobacter pylori is quite resistant to antibacterial drugs, which makes treatment difficult.
Research shows that more than 70% of the world's population is infected with Helicobacter pylori. At the moment, this is the most common infection. However, for various reasons, in most cases the presence of bacteria in the body does not cause the development of the disease and infection proceeds unnoticed.
In addition to the presence of pathogenic microorganisms in the stomach, the development of erosive gastritis can also be provoked by other reasons:
- severe stress
- chronic mental stress
- regular alcohol intake
- eating disorder with long periods of fasting
- eating spicy and salty foods
- smoking in the morning before breakfast
- taking certain medications
- liver and pancreas diseases
- chronic gastrointestinal diseases
- diabetes
- harmful working conditions
- reflux of the contents of the duodenum into the stomach
The combination of infection by pathogenic microorganisms with provoking factors reduces the protective function of the body. There is a release of bile, increased production of pepsin and acid. This significantly impairs the ability of the epithelium to regenerate and produce protective mucus and leads to the appearance of defects in the gastric mucosa and the formation of erosive gastritis.
Features of drug treatment
Maalox will help treat erosive gastritis.
The choice of treatment method for erosive gastritis directly depends on the causes of its occurrence. If the stomach is affected by Helicobacter pylori, treatment is carried out using antibiotics.
Most often, patients are recommended to take Amoxicillin, Tetracycline, Levofloxacin. The medications are taken over a fairly long period.
If therapy for the disease is interrupted, this will lead to re-production of pathogenic microorganisms.
During treatment of the disease, it is necessary to regulate the acidity of the stomach. At this stage of treatment, the mucous membrane is protected from the aggressive effects of gastric juice on it. In order to cure erosive antral gastritis, it is necessary to take antacids and acid blockers.
In most cases, Maalox, Almagel, Rennie, Nizatidine, etc. are taken. Each drug is characterized by its own mechanism of action. That is why, if there is a need to change the medication, it is recommended to first consult a doctor.
If the patient's condition is critical, then he needs to take liquid antacids orally. A high effect in this case is observed with Famotidine, Ranitidine, Cimetidine. If the need arises, treatment is carried out using blood replacement solutions.
Classification of forms of erosive gastritis
- Primary erosions (have no connection with previously identified pathology) and secondary (the result of progression, existing disease).
- Malignant (appears in the presence of an oncological process) and benign (can be single or multiple).
- Immature (young formations) and mature (have areas of tissue necrosis).
Based on the type and shape of formations on the mucous membrane, the following types are distinguished:
- superficial (small, flat in shape and with a distinct edge);
- full (raised above the surface of the mucosa);
- polypoid (can have a diameter of up to one and a half centimeters, do not heal for a long time and constantly worsen).
Diagnostics
Fibrogastroscopy provides the most data for correct diagnosis. During this procedure, the doctor can see the condition of the mucosal surface, examine defects - their location, quantity, area, features.
Erosion looks like small defects of different shapes and sizes. If there are less than 3 lesions, the lesions are considered single. If there are more than 3 of them, and they are localized in different parts of the organ, they are multiple.
To clarify the method of treating gastric erosion, a biopsy may be indicated - taking a small piece of the affected mucosa for microscopic examination.
Symptoms of erosive gastritis
Patients suffering from erosive gastritis can present many different complaints, both specific and nonspecific:
- nausea and rare episodes of vomiting
- decreased appetite or complete absence of it
- increased gas formation
- heartburn
- belching
- pain in the epigastrium on an empty stomach or an hour and a half after eating
- sudden weight loss
- black stool due to bleeding
- vomiting black-brown mass
Patients may also complain of increased drowsiness and fatigue, decreased tolerance to usual stress, the appearance of shortness of breath and tachycardia. Such symptoms may indicate the presence of hidden bleeding.
The pathology symptoms listed above indicate that the disease may have symptoms of gastric bleeding and the presence of mucosal defects.
Symptoms of gastric erosion
There are acute or chronic forms of the disease. Symptoms of acute gastric erosion usually affect the fundus or body of the stomach. In a chronic process, the antrum is affected (located below all other segments of the organ).
Clinical manifestations of gastric erosion are divided into the following groups.
Ulcer-like. With this clinical picture, the disease is accompanied by severe pain, which usually begins after eating, but can also occur on an empty stomach. Other symptoms are belching, vomiting, heartburn. Ulcer-like symptoms can occur in both acute and chronic gastric erosion.
Hemorrhagic. These are symptoms associated primarily with anemia and bleeding. Often there are no obvious signs of the disease. This course of gastric erosion is characteristic of the acute form of the disease.
How is erosive gastritis diagnosed?
Erosive gastritis has symptoms similar to other gastrointestinal diseases. Therefore, to clarify the diagnosis, additional examination is prescribed. Most often, doctors recommend the following laboratory and instrumental studies:
- a general blood test to determine the presence of anemia;
- determination of occult blood in feces;
- taking a section of the mucosa for cytology and histology;
- PCR for diagnosing Helicobacter pylori infection;
- fibrogastroscopy (FGDS) with a biopsy of the inflamed area;
- radiography with contrast.
Sign up for FGDS
Don't delay treatment
Treatment of erosive gastritis
For the treatment of pathology, conservative tactics are usually chosen. Surgery is very rarely required.
The basis of successful treatment is diet and regular medication. Doctors usually prescribe a set of tablets to destroy Helicobacter pylori, relieve symptoms of the disease and stimulate healing of the mucous membrane.
Since Helicobacter pylori is an antibiotic-resistant microorganism, a combination of three or four drugs is chosen to destroy it. Treatment is not easy and takes quite a long time.
If there is bleeding, in addition to taking medications, the doctor may recommend thermo- or electrocoagulation of the mucous membrane, laser exposure, staples or endoscopic stitching.
During treatment of the pathology, the patient should adhere to a fractional diet plan. There should be at least 5 small meals a day. To reduce the likelihood of mechanical damage to the mucous membrane during healing, you should eat grated food or cooked with steam. It is also necessary to avoid eating too hot or cold foods, and avoid eating salty, fried, fatty and spicy foods. Sodas, strong coffee, tea and alcoholic drinks are not allowed.
Acute erosive-ulcerative gastroduodenal lesions in patients with cardiovascular diseases
Purpose of the review: To highlight the issues of pathogenesis, diagnosis, treatment of acute erosive-ulcerative gastroduodenal lesions in patients with cardiovascular diseases, as well as their role in thanatogenesis.
Main points of the review: There is an increase in the frequency of acute erosive and ulcerative gastroduodenal lesions in patients with cardiovascular diseases and other somatic pathologies. The role of bleeding caused by them in the thanatogenesis of these diseases is underestimated. In the pathogenesis of acute erosive gastropathy in patients with cardiovascular and other somatic pathologies, many factors are summed up, primarily acute or chronic ischemia of the gastroduodenal mucosa, as well as its age-related involution, helicobacteriosis, reflux gastritis, multiple organ failure, drug damage, etc. d.
Conclusions: Despite the increase in the frequency of OEGP and the unresolved issues of their prevention, diagnosis and treatment, in recent years there has been a tendency towards a decrease in fatal gastrointestinal tract complications associated with OEGP. Antisecretory therapy, increasingly administered to patients with ischemic heart disease and CVD during the period of active influence of risk factors, reduces the likelihood of gastroduodenal bleeding in therapeutic patients by at least 50%.
Multiple hemorrhages and acute erosions of the gastric mucosa are usually combined under the term acute erosive gastropathy. This group concept cannot, however, be considered successful, since it unites a large number of nosological forms that are diverse in etiology and pathogenesis and their complications - infectious, ischemic, medicinal, oncological lesions of the stomach, requiring the use of various methods of diagnosis and treatment. In addition, a combination of erosive lesions and acute ulcers of the mucous membrane, not only of the stomach, but also of the duodenum, is often found [1 – 15].
The etiology of acute erosive and ulcerative gastroduodenal lesions (AUGD) is extremely diverse. The most important etiological factors include taking certain medications - non-steroidal anti-inflammatory drugs (NSAIDs), cytostatics, corticosteroids, etc.; alcohol intoxication; chemical and physical gastroduodenal injuries; stress, shock, disseminated intravascular coagulation syndrome of various etiologies, severe injuries, burns (Curling ulcers), frostbite; chronic atrophic gastritis, Helicobacter pylori and heilmannii infection; renal (uremic gastropathy), liver failure (hepatogenic ulcers); oncological diseases, incl. stomach tumors; blood diseases (anemia, leukemia); infectious diseases, chronic lung diseases, diseases of the neuro-endocrine system, such as neurotrauma and other lesions of the brain (especially the posterior cranial fossa), the hypothalamic-pituitary system (Cushing's ulcer); gastrin-producing tumors (Zollinger-Ellison syndrome), hyperparathyroidism, diabetes mellitus (coma, ulcerogenic effect of insulin), etc. However, in recent years, attention has been drawn to the increase in the frequency of AEHP and the resulting gastrointestinal bleeding (GIB) in patients with cardiovascular diseases, primarily coronary heart disease (CHD) and cerebrovascular diseases (CVD) [1-7 , 16 – 30].
The increase in the frequency of OEGP in patients with cardiovascular diseases and other somatic pathologies allows us to speak, in fact, about their epidemic. According to various authors, the frequency of OEGP in such patients reaches 80-90%, and the gastrointestinal tract complications caused by them – 45-55%. The wide distribution of OEGP is associated with the aging population, the influence of unfavorable ecology, exogenous (alcohol, etc.) and endogenous intoxications, iatrogenic factors (increasing the number and volume of surgical interventions, taking various medications) [2-11, 19-24, 31 ].
Thus, a comparison of the results of studies of the frequency of OEGP based on materials from 6900 autopsies of people who died from various diseases from the groups of IHD and CVD in multidisciplinary emergency hospitals with a percentage of autopsies of at least 80% in 2000-2002. (2400 autopsies) and 2003-2008. (4500 autopsies) demonstrated that over the last decade it has increased by about a third, despite the introduction into clinical practice of measures for their prevention, diagnosis and treatment [2-8, 10, 11, 20-24]. It is important to note that these studies excluded observations with diseases that could be independent causes of the development of OEGP, in addition to cardiovascular diseases: surgical pathology of the digestive organs, chronic alcohol intoxication, chronic gastritis, oncological, endocrine (except for diabetes mellitus in 2003 -2008), and infectious and allergic diseases, as well as with renal and liver failure, cachexia, with a known history of taking medications that cause OEGP. The IHD group was represented by myocardial infarction (32%), large- and small-focal cardiosclerosis (20%); CVB group - ischemic cerebral infarctions and intracerebral non-traumatic hematomas (42%), long-term consequences of cerebrovascular accidents (3%). Background diseases were arterial hypertension (71.6% for ischemic heart disease and 86.6% for CVD), type 2 diabetes mellitus (4.3 and 1.2%, respectively), or a combination of both (18.6 and 9. 6%). Combined underlying diseases were represented by a combination of diseases from the groups of IHD and CVD (21%). The ratio of men to women was 1: 1.3 for IHD, 1: 1.1 for CVD, the average age of the deceased was 67.5 ± 3.2 years [2-8, 10, 11, 20-24].
The results of the above studies showed that the frequency of OEGP was in myocardial infarction in 2000-2002. 10%, and in 2003-2008. – 18%, in chronic forms of IHD with chronic heart failure syndrome, 6 and 10%, respectively, in strokes – 8 and 14%, and in chronic forms of CVD – 4 and 9% (Fig. 1). In observations with a combination of diseases from the IHD and CVD groups, OHEP were detected much more often, in 21% of observations. Increase in the frequency of OEGP in 2003-2008. to a certain extent, can be explained by the inclusion in the analyzed group (compared to 2000-2002) of patients with diabetes mellitus, who amounted to 22.7% for coronary artery disease and 10.8% for CVD [2-8, 10, 11].
Fig. 1 Frequency (in %) of acute erosive and ulcerative gastroduodenal lesions in those who died from diseases from the ischemic heart disease and CVD groups in 2000-2002 (2400 autopsies, background disease - diabetes mellitus was excluded) and in 2003-2008. (4500 autopsies, background disease included - diabetes mellitus).
In patients with ischemic heart disease and CVD, acute erosions and ulcers were localized predominantly in the stomach (88 and 74%), in the duodenum (mainly in its bulb) - in 8 and 12% of patients, respectively, and combined damage to the stomach and duodenum was detected in 4 and 14% of observations, respectively. (Fig. 2). In the stomach, changes were more pronounced in the area of the body and lesser curvature (with ischemic heart disease - in 52±1.3%, with CVD - in 41.0±0.3%), less often - in the fundus (respectively, in 21±0. 7 and 27±0.5%) and antrum (in 27±1.5 and 25±0.2%) sections. In both IHD and CVD, superficial lesions predominated (acute erosions accounted for 47.3–87.9% of cases), rather than deep ones, such as acute ulcers [10, 11].
Fig. 2 Frequency (in%) of localization of acute erosions and ulcers in the stomach or duodenum in ischemic heart disease and CVD.
Timely diagnosis of OEGP is a problem that has not been solved to date, which is due to the peculiarities of their clinical manifestations. 30-90% of patients are characterized by an asymptomatic course, 46-58% - the absence of a typical and pronounced clinical picture, and in 25-42% of patients the symptoms of the underlying disease predominate. As a result, AEHP often goes undiagnosed until it suddenly presents with bleeding, often life-threatening. At the same time, the frequency of hemorrhagic complications of OEGP, including fatal ones, is 39-47% [3, 9, 11]. In patients with ischemic heart disease and CVD, the first manifestation of damage to the gastroduodenal mucosa is gastrointestinal tract in 25-55% of cases, and in most cases the diagnosis is first established at autopsy. It should be noted that the widespread decrease in the number of pathoanatomical autopsies, characteristic of many medical institutions, leads to an underestimation of the frequency and role of OEGP in thanatogenesis in patients with cardiovascular diseases. Most researchers agree that bleeding caused by OEGP develops much more often than is detected [2-11, 19-24].
The problem of treating gastrointestinal tract in patients with OEGP also remains unresolved. The results of conservative treatment of acute ulcers and erosions complicated by bleeding remain unsatisfactory, mortality ranges from 36.4 to 64-80% [1,3]. The outcomes of surgical treatment are also often unfavorable. Mortality after using various methods of surgical intervention is in the range of 24-44% [32-34]. Since gastrointestinal tract disorders during OEGP often occur subclinically and do not lead to significant hemodynamic disturbances, some authors believe that their clinical significance should not be exaggerated [35-37]. This opinion is opposed by data from other researchers, according to which bleeding prolongs the treatment period by an average of 4-8 days, increases the risk of repeated massive bleeding by 4 times and the risk of death by 2-4 times [2-8,36,38 ].
According to the above-mentioned pathological studies conducted in 2002-2008. in multidisciplinary emergency hospitals, gastrointestinal tract diseases of varying severity associated with OEGP developed in 67% of those who died with ischemic heart disease and 55% in CVD, but their role in thanatogenesis was different. The frequency of fatal gastrointestinal tract complications (direct causes of death) was for myocardial infarction in 2000-02. 4%, in 2003-08 – 3%, for chronic forms of IHD with chronic heart failure syndrome, 2 and 2%, respectively, for strokes – 2 and 1%, chronic forms of CVD in 2000-02. - 1%, and in 2003-08. no such deaths were identified (Fig. 3).
Fig. 3 Frequency (in%) of fatal bleeding in acute erosive-ulcerative gastroduodenal lesions in those who died from diseases from the ischemic heart disease and CVD groups in 2000-2002 (2400 autopsies, background disease - diabetes mellitus was excluded) and in 2003-2008. (4500 autopsies, background disease included - diabetes mellitus).
Thus, despite the increase in the frequency of AEGP, there is a trend towards a decrease in the fatal gastrointestinal tract complications associated with them [10,11,20,21]. It is known that antisecretory therapy, increasingly carried out in patients with coronary artery disease and CVD, increases the pH of the stomach contents to 5.0 - 7.0 units. during the period of active influence of risk factors, reduces the likelihood of gastroduodenal bleeding in therapeutic patients by at least 50% [2,3,35]. Although the share of gastrointestinal tract among the causes of death of patients with coronary artery disease and CVD did not exceed in 2000-08. 4%, the absolute number of such deaths is quite large, since nosological forms from these groups of diseases are the leading causes of death in the population. Taking into account the mortality rates for these diseases, 1 in 200 patients with myocardial infarction and 1 in 1000 with ischemic infarction or cerebral hematoma die from gastrointestinal tract. In 2009 in Moscow, among all causes of death, diseases from the IHD group amounted to 31.6, neoplasms – 19.8, and CVD – 18.3%. Among the nosological units, the leaders remain chronic forms of IHD (atherosclerotic and post-infarction cardiosclerosis - 24.1%, strokes - 6.6% and myocardial infarction - 5.5%) (Fig. 4). As a result, in Moscow, mortality from gastrointestinal tract diseases caused by OEGP is at least 1000 patients per year [10,11,20,21].
Fig.4 The most common (in %) diseases and their groups (CHD, CVD, cancer) - causes of death in Moscow in 2009.
The pathogenesis of OEGP in patients with cardiovascular diseases is not clear enough. A number of authors believe that the mechanisms of development of OEGP in patients with various somatic pathologies generally reflect the known pathogenesis of “stress” damage to the gastroduodenal mucosa, which is practically independent of the characteristics of the underlying disease. Consequently, OEGP develops as a result of peptic (acid) damage to the mucous membrane against the background of its deep ischemia with inhibition of all mechanisms of gastroprotection: secretion of bicarbonate, mucin, proliferation and regeneration of the epithelium [10,11,39-41]. It is known that with chronic circulatory failure, degenerative processes develop in many organs, including the digestive organs, especially in the gastric mucosa, which loses its resistance [15,28,29]. Other factors, such as helicobacteriosis, drugs, duodenogastric bile reflux, gastroparesis, etc., can also contribute to the development of OEGP. [1-3.37]. However, many researchers insist on the need to consider OEGP as an acute injury to the gastroduodenal mucosa associated with hyperacidity, in which the primary etiological factor is not Helicobacter pylori gastritis, as in peptic ulcers, and not long-term use of anti-inflammatory drugs, as in NSAID gastropathy, but severe somatic disease [29]. A morphological study conducted in deceased patients with ischemic heart disease and CVD, taking into account the known role of chronic atrophic gastritis and helicobacteriosis in the pathogenesis of erosive and ulcerative lesions of the stomach, did not reveal a significant difference in their frequency in two groups of observations - complicated and uncomplicated OEGP, which indicates the presence in cardiovascular diseases there are other important pathogenetic factors in the development of these complications [10,11].
Thus, the leading role in the pathogenesis of OEGP appears to be played by ischemia and microcirculatory disorders of the gastroduodenal mucosa, which cause reverse diffusion of H+, acidosis, depletion of buffer systems, death and impaired regeneration of epithelial cells [2,3,10,11, 20,21].
Morphological studies have shown that in chronic heart failure syndrome in patients with ischemic heart disease and, often, with CVD, chronic venous plethora, atrophy and sclerosis of all layers, sclerosis and hyalinosis of the walls of arterioles and small arteries develop in the gastroduodenal mucosa, cavernous structures are formed from sharply dilated veins and venules in the submucosal layer, reduction of the capillary bed, multiple superficial small foci of hemorrhage, ischemic and hemorrhagic necrosis, leading to the formation of acute erosions, more rarely, acute ulcers. An immunohistochemical study of the gastroduodenal mucosa in patients with ischemic heart disease and CVD revealed a decrease in proliferative activity and expression of growth factors and angiogenesis (TGF-β1 and VEGF), indicating inhibition of regenerative abilities and a decrease in protective functions. Such changes, typical of chronic ischemia, developed in the presence of severe stenosing atherosclerosis of the arteries of the stomach and duodenum [10,11,20,21]. In patients with coronary artery disease and acute heart failure syndrome, against the background of chronic changes in the gastroduodenal mucosa, its acute venous plethora, pronounced swelling of the submucosal and muscular layers, the appearance of extensive hemorrhages, large foci of ischemic and hemorrhagic necrosis, up to the submucosal layer, are noted. Cardiogenic shock, often against the background of chronic ischemic changes in the mucous membrane, is characterized by alternating foci of acute venous congestion and anemia, widespread thrombosis of the microvasculature, extensive multiple hemorrhages and confluent superficial foci of necrosis of the mucous membrane [10,11,20,21]. Such morphological changes in the stomach and duodenum in patients with cardiovascular diseases make it possible to substantiate the concept of ischemic disease of the stomach and duodenum, by analogy, for example, with ischemic intestinal disease. A feature of ischemic disease of the stomach and duodenum is the extremely rare development of necrosis (infarction) of the entire thickness of their walls, which is due to the extremely developed system of vascular anastomoses of these organs and multiple sources of blood supply. At the same time, the aggressive environment of the stomach, even with minor circulatory impairment and ischemia of the gastroduodenal mucosa, contributes to its damage.
The question remains open about the pathogenetic role of acute posthemorrhagic anemia in the development of exacerbations of coronary artery disease and CVD in gastrointestinal tract diseases caused by OEGP. A specially conducted retrospective analysis of medical records of inpatients and outpatients in multidisciplinary hospitals showed, even taking into account the incompleteness of information, that gastrointestinal tract complications preceded the development of myocardial infarction in 1.3%, and strokes in 0.22% of patients, which is of undoubted interest in terms of the relationship OEGP and ischemic lesions of the heart and brain [10,11,20,21].
Thus, there is an increase in the frequency of OEGP in patients with cardiovascular diseases and other somatic pathologies. The role of gastrointestinal tract diseases caused by OEGP in the thanatogenesis of these diseases is underestimated; the problems of their prevention, diagnosis and treatment remain unresolved. OEGP in patients with cardiovascular diseases is a morphological substrate of ischemic disease of the stomach and duodenum. With atherosclerosis, arterial hypertension and diabetes mellitus, the stomach and duodenum become one of the target organs, and damage to the heart and brain with ischemic heart disease and CVD aggravate the severity of pathological changes in the gastroduodenal mucosa. It should be taken into account, however, that in the pathogenesis of OEGP in patients with cardiovascular diseases and other somatic pathologies, many factors are summed up: acute or chronic ischemia of the gastroduodenal mucosa, its age-related involution and atrophy due to helicobacteriosis, reflux gastritis, drug damage, etc. .
Literature 1. Gelfand B.V., Guryanov V.A., Martynov A.N. and others. Prevention of stress-damage to the gastrointestinal tract in patients in critical conditions. Consilium Medicum 2005; 7 (6):464-71. 2. Vertkin A.L., Zairatyants O.V., Vovk E.I. Damage to the stomach and duodenum in patients with acute coronary syndrome. Attending Physician 2005; 1:66-70. 3. Vertkin A.L., Zairatyants O.V., Vovk E.I. Final diagnosis. – M.: GEOTAR-Media, 2008. 4. Kolobov S.V., Zayratiants O.V., Poputchikova E.A.. Morphological features of acute erosions and gastric ulcers in patients with myocardial infarction during treatment with the drug “Losek”. Morphological statements - 2002; 3(4):80-2. 5. Kolobov S.V., Zayratiants O.V., Khokhlova E.E., Frolova Yu.V. Acute erosive and ulcerative lesions of the stomach in emergency conditions in therapeutic patients. Abstract. report VI Congress of the Scientific Society of Gastroenterologists of Russia. – M., 2006. – P.24-25. 6. Kolobov S.V., Vertkin A.L., Zayratiants O.V., Poputchikova E.A., Mishutchenko O.P., Khokhlova E.E. Acute erosive and ulcerative lesions of the upper gastrointestinal tract in patients with myocardial infarction. Sat. proceedings of the II Congress of the Russian Society of Pathologists. – M., 2006. – T.1. — P.70-71. 7. Kolobov S.V., Zairatyants O.V., Vovk E.I., Poputchikova E.A., Mishutchenko O.P., Khokhlova E.E. Acute erosive and ulcerative lesions of the upper gastrointestinal tract. Sat. works “Current issues of morphogenesis in normal and pathological conditions.” – M.: Research Institute of Human Morphology of the Russian Academy of Medical Sciences, 2006. – P.17-18. 8. Kolobov S.V., Zairatyants O.V., Khokhlova E.E. Erosive and ulcerative lesions of the stomach and duodenum and gastrointestinal bleeding in patients with myocardial infarction. Sat. abstract report VII Moscow Assembly “Health of the Capital”. – M., 2008. – P.305-306. 9. Maev I.V. Erosive gastritis: a separate nosological form or a universal reaction of the mucous membrane to damage? Ross Journal of Gastroenterology, Hepatology, Coloproctology 2005; 15 (6):53-9. 10. Khokhlova E.E., Kolobov S.V., Zairatyants O.V., Zairatyants G.O. Acute erosive-ulcerative gastroduodenal lesions and bleeding in therapeutic and neurological patients. Sat. Proceedings of the III Congress of the Russian Society of Pathologists. – Samara: SamSMU, 2009. – P.325. 11. Yarema I.V., Kolobov S.V., Zayratiants O.V., Khokhlova E.E., Poputchikova E.A. Acute erosive-ulcerative gastroduodenal lesions in patients with coronary heart disease, cerebrovascular diseases and chronic obstructive pulmonary diseases. Surgeon 2009; 12:5-13. 14. Borchard F., Malferthemer P., von Herbay A. et al. Classification of erosions of the stomach results of a meeting of the study group of Gastroenterologic Pathology of the German Society of Pathology. Pathology - 1992; 13(5):249-51. 15. Steinberg KP Stress-related mucosal disease in the critically ill patient: risk factors and strategies to prevent stress-related bleeding in the intensive care unit. Crit Care Med 2002; 30(6): Suppl. 362-4. 16. Aruin L.I., Kapuller L.L., Isakov V.A. Morphological diagnosis of diseases of the stomach and intestines - M.: Medicine, 1998. 17. Grinevich V.B., Uspensky Yu.P., Grigoriev V.P., Kalinin A.V. Erosive changes in the gastroduodenal mucosa - a pre-ulcerative condition? Klin Med 1991; 69(11):57–9. 18. Grinevich V.B., Tkachenko E.I., Uspensky Yu.P. Classification of erosions of the mucous membrane of the stomach and duodenum. Klin Med 1996; 74(1):75–6. 19. Ivashkin V.T., Sheptulin A.A. Erosive and ulcerative lesions of the stomach and duodenum caused by non-steroidal anti-inflammatory drugs. Doctor 2001; 3:22-3. 20. Zairatyants O.V., Kolobov S.V., Khokhlova E.E., Poputchikova E.A. Acute erosive-ulcerative gastroduodenal lesions in therapeutic and neurological patients. Sat. scientific works of the conference in memory of Yu.L. Perov / Ed. Academician RAS and RAMS V.A. Tkachuk. – M.: Moscow State University Publishing House, 2009. – P.35-43. 21. Zairatyants O.V., Kolobov S.V., N.I. Polyanko, Khokhlova E.E. Acute erosive and ulcerative bleeding in therapeutic and neurological patients. Sat. abstract report VIII Moscow Assembly “Health of the Capital”. – M., 2009. – P.256-257. 22. Kolobov S.V., Zayratiants O.V., Loranskaya I.D., Simonova N.I., Poputchikova E.A. Erosive and ulcerative lesions of the upper gastrointestinal tract in patients with acute myocardial infarction. Emergency Therapy 2002; 3 (4): 63-7. 23. Kolobov S.V., Zayratiants O.V., Loranskaya I.D., Simonova N.I., Poputchikova E.A. Erosive and ulcerative lesions of the stomach and duodenum in acute myocardial infarction. Experimental and Clinical Gastroenterology 2003; 1:95-7. 24. Kolobov S.V., Vertkin A.L., Zayratiants O.V., Vovk E.I., Shamuilova M.M., Melnikova T.A., Frolova Yu.V. Treatment and prevention of gastrointestinal bleeding in patients with exacerbation of coronary artery disease. Therapist 2006; 6:15-28. 25. Bawk S. Stress ulcers — prevention of gastrointestinal bleeding in critical care units. Med J Austral - 1985; 142: (Special. Suppl):17-21. 26. Imhof M., Ohman G., Hartwig A. et al. Which peptic ulcers bleed? Results of a case-control study. DUSUK Study Group. Scand J Gastroenterol – 1997; 32 (2):131-8. 27. Jick SS The risk of gastrointestinal bleed miocardiae infarction and newly diagnosed. Pharmacotherapy – 2000; 4 (4):741-7. 28. Kantorova I., Svoboda P., Scheer P. et al. Stress ulcer prophylaxis in critically ill patients: a randomized controlled trial. Hepatogastroenterology 2004; 51(57):757-61. 29. Peterson WL The role of acid in upper gastrointestinal haemorrhage due to ulcer and stress-related mucosal damage. Aliment Pharmacol Ther 1995; 13(Suppl 1):43-6. 30. Robert G. Amer J Health-System Pharmacy 2002; 62 (10): (Suppl.2): 11-7. 31. Mikhailov A.P., Danilov A.M., Napalkov A.N., Shulgin V.L. Acute ulcers and erosions of the digestive tract: Textbook. – St. Petersburg: St. Petersburg Publishing House. Univ., 2004. 32. Stotsko Yu.M., Kurygin A.A., Musinov I.M. Vagotomy in the treatment of acute gastric ulcerations complicated by severe bleeding. Vestn hir 2001; 3:25-9. 33. Chernov V.N., Miziev I.A., Belik B.M. Prediction and prevention of acute ulcers and erosions of the stomach and duodenum in surgical patients. Vestn hir 1999; 6:12-5. 34. Sheptulin A.A. Gastropathy associated with the use of non-steroidal anti-inflammatory drugs: risk factors, treatment, prevention. Clin Perspectives in Gastroenterology and Hepatology 2001; 1:27-31. 35. Pimentel M, Roberts DE, Bernstein CN et al. Clinically significant gastrointestinal bleeding in critically ill patients in an era of prophylaxis. Am J Gastroenterol 2000; .95(10):2801-6. 36. Cook DJ, Griffith LE, Walter SD et al. The attributable mortality and length of intensive care unit stay of clinically important gastrointestinal bleeding in critically ill patients. J Crit Care 2001; 5(6):368-75. 37. Yang YX, Lewis JD Prevention and treatment of stress ulcers in critically ill patients. Semin Gastrointest Dis 2003; 14 (5):11-9. 38. Stollman N., Metz DC Pathophysiology and prophylaxis of stress ulcer in intensive care unit patients. J Crit Care 2005; 20 (1):35-45. 39. Loginov AS, Zvenigorodskaia LA, Potapova VB et al. The characteristics of peptic ulcer in subjects with concomitant ischemic heart disease. Ter Arkh 1998; 70 (3):9-13. 40. Spirt MJ Stress – related mukosal disease: risk factors and prophylactic therapy. Clin Ther 2004; 26 (6):197-213. 41. Raynard B., Nitenberg G. Is prevention of upper digestive system hemorrhage in intensive care necessary? Schweiz Med Wochenschr 1999; 129 (8): S.1605-1612.
Prevention
You can prevent the onset of the disease by observing personal hygiene measures, maintaining your diet, and giving up smoking and drinking alcoholic beverages. When working in hazardous industries, you should take precautions. When diagnosing diseases, carry out their timely treatment. You should also avoid stressful situations.
Why choose American Medical Clinic?
- Team of professionals. Candidates and doctors of medical sciences, professors and associate professors of departments of leading universities, doctors of the first and highest qualification categories work in the clinic 24 hours a day, 7 days a week. We work without holidays or weekends to ensure that you are healthy and happy.
- Regular professional development. Each doctor regularly takes advanced training courses, attends seminars, goes on internships, participates in conferences, and undergoes training abroad. This helps maintain the qualifications of doctors at the highest level. Today, the training of AMK doctors allows them to train young doctors, acting as experts at European-level seminars.
- Hi-tech. We regularly invest not only in training and professional development of personnel, but also in purchasing the most modern equipment from leading European manufacturers.
- The value of time. The American Medical Clinic has created all the conditions for a comfortable, comprehensive examination and diagnosis of a patient on the day of treatment.
- Trust from clients. Over 25 years of impeccable work, more than 500,000 patients have entrusted their health to us. More than 80% of patients recommend us to their family and friends.
- Guarantees. We are 100% responsible for the quality of the services provided, the high level of which is confirmed by many years of experience. The attention and sensitive attitude of doctors with more than ten years of experience in medical practice give a sustainable positive result.
Treatment
Along with medications for gastric erosion, diet plays an important role in successful treatment. It is recommended to avoid irritating (hot, salty, spicy, sour) foods, avoid carbonated drinks, including mineral water, and alcohol. Steamed, baked and boiled foods are shown. Fried and pickled foods are limited.
Along with the diet, food intake is also adjusted. They should be:
- fractional – 4–5 times a day;
- small in volume.
It is also recommended to take a course of psychocorrection, during which psychologists teach how to cope with stressful situations or prevent them.
Drug therapy includes the use of antibacterial drugs and gastroprotectors, which create a protective film on the surface of erosions. This protects them from the action of hydrochloric acid, pepsin, and bile acids necessary for digesting food and gives them the opportunity to heal better. If the patient is bothered by a feeling of fullness or bloating, medications to improve gastric motility are included in the treatment regimen. If there is high acidity, drugs that reduce it are also prescribed. The doctor decides how to treat gastric erosion in a particular case.
For bleeding, therapeutic treatment may be indicated. The doctor determines whether there is blood in the stomach during fibrogastroscopy or by indirect signs.