Definition
Erosive gastritis is one of the types of inflammatory process of the gastric mucosa, in which superficial erosions are formed on it, which is accompanied by a violation of the secretory, endocrine, motor and evacuation functions of the organ. A gastroenterologist treats acute and chronic pathologies of the gastrointestinal tract. The Department of Gastroenterology at the Elena Malysheva Clinic in Izhevsk specializes in providing consultative, diagnostic and therapeutic care to patients with diseases of the digestive system, including erosive gastritis.
Additional methods and means of treating gastritis
When treating gastritis, it often becomes necessary to involve specialists from other fields of medicine. This is due to the fact that diseases of the gastrointestinal tract rarely go away without leaving a trace for the body as a whole, which requires treatment of complications. In addition, the disease can be triggered by factors unrelated to the gastrointestinal tract. Thus, erosive gastritis in the acute stage is often accompanied by gastric bleeding, leading to anemia, which makes it necessary to involve a hematologist in the treatment. And the cause of damage to the gastric mucosa can be allergic reactions or endocrine disorders - the area of influence of an immunologist-allergist and endocrinologist.
Symptoms of erosive gastritis
Pathological processes in the stomach, depending on the depth of damage, duration of existence, and prevalence, determine the development of various clinical manifestations. The main symptoms of gastric damage with erosive gastritis are a feeling of discomfort in the left hypochondrium, and then the occurrence of pain of varying intensity associated with eating.
Symptoms that appear in patients as the disease progresses:
- pain in the epigastric region - in the upper abdomen under the xiphoid process;
- heaviness in the stomach;
- heartburn, belching sour, rotten;
- bad breath;
- nausea, vomiting with blood;
- unstable stool: alternating diarrhea and constipation;
- change in color of stool – black feces;
- flatulence;
- dry pale skin;
- dull, brittle hair;
- dizziness;
- weight loss.
Erosion of the stomach and duodenum
Classification:
- Erosion as a manifestation of a malignant or systemic process in the gastric mucosa (cancer, lymphoma, Crohn's disease, etc.).
- Benign erosions: acute erosions (hemorrhagic);
- “chronic” erosion (erosion completa); erosions can be single or multiple;
- chronic erosive (lymphocytic) gastritis;
- erosive-hemorrhagic gastritis and duodenitis.
In addition, it is advisable to distinguish primary erosions and so-called secondary erosions that accompany the underlying disease.
Classification issues remain relevant to this day.
At the World Congress of Gastrointestinal Endoscopy, a Round Table meeting was devoted to terminology and semantics in endoscopy, in particular, it was discussed what terminology and classification of erosions to use when interpreting endoscopic examinations and when there is erosion as a complication or as a disease.
Attempts to classify erosive processes have been made by other authors. The definition of chronic erosions seems especially difficult.
In the medical literature, along with the term “chronic erosion,” the term “complete” erosion (erosion complete) is widely used, and with the development of numerous chronic erosions, the term “smallpox” (varioloform) gastritis, chronic erosive (verrucous) gastritis is used. In our opinion, the most The term “chronic erosion” seems acceptable, indicating the phase of the process (exacerbation or remission).
It is much more difficult to classify duodenal erosions. It is proposed to distinguish between acute and chronic erosions of the duodenum, but the authors admit that it is much more difficult to differentiate erosions of the duodenum than the stomach.
As a result of studies, it was established that the concentration of serum gastrin in patients with gastric erosions corresponds to normal values; in patients with erosive duodenitis and duodenal ulcer in the phase of incomplete scarring, the concentration of gastrin is almost the same. A slight difference was noted in the content of pituitary hormones (GH, TSH), progesterone and estradiol in patients with erosive duodenitis and with incomplete scarring of the duodenal ulcer.
Gastroduodenal erosions occur in various conditions of the acid secretion function of the stomach; There is no clear relationship between the tendency of erosion to heal and the level of gastric acid secretion.
An important practical issue is the question of the characteristics of the course of erosive damage (the duration of their existence, the tendency to relapse).
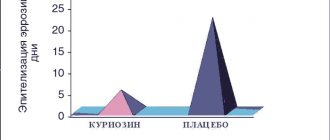
Studying the evolution of erosions and acute ulcers and determining the duration of their existence is a difficult task, largely dependent on the timing and thoroughness of endoscopic examination of the stomach. Dynamic endoscopic observation of patients with gastroduodenal erosions (endoscopy was carried out at various intervals from 2 to 7 times) showed that flat (acute) erosions last on average 7-10 days, but sometimes up to 2-8 weeks (depending on the prevalence and severity of the process ). Acute erosions almost always affect the proximal parts of the stomach (subcardial section, body of the stomach). Chronic erosions can be detected in the stomach for a long time (up to 6 years or more). Erosion of this type is localized, as a rule, in the antrum of the stomach. Duodenal erosions exist for a long time, for many weeks and months.
The question of the tendency of erosions to relapse is important. We concluded that only a portion of the erosive lesions recur. In these cases, chronic erosions occur in the antrum of the stomach, and flat defects of the mucous membrane are more often observed in the duodenal bulb. In most cases, there was no tendency for the reappearance of erosions of the stomach and duodenum.
Various clinical syndromes have been identified in patients with gastroduodenal erosions. Hemorrhagic syndrome is observed in approximately 20% of patients with erosive lesions of the stomach and duodenum, often in the form of repeated bleeding. Sometimes this syndrome is manifested by black stools (melena), less often by vomiting mixed with blood or “coffee grounds” vomiting, a collapsed state, and a decrease in hemoglobin. But, as a rule, the bleeding is hidden, so-called occult, in nature. Patients gradually develop chronic posthemorrhagic anemia. Signs of occult bleeding - general weakness, slowly progressing anemia, the presence of occult blood in the stool - are a direct indication for a thorough examination of the upper gastrointestinal tract. Of course, it is necessary to exclude damage to the colon and rectum during a comprehensive diagnosis. An ulcer-like syndrome is most often observed in patients with gastroduodenal erosions. Patients complain of periodic pain in the epigastric region associated with food intake, heartburn, belching, and nausea.
In patients with erosions and ulcers of the stomach and duodenum, symptoms of chronic diffuse liver diseases, lesions of the biliary tract and pancreas, diseases of the esophagus, tumors of the gastrointestinal tract, diseases of the cardiovascular system,
Dynamic endoscopic observation of patients with gastroduodenal erosions makes it possible to speak in favor of the hypothesis that acute and chronic erosions are stages of the same process. Chronic erosions can exist for many months and even years. They usually disappear, but sometimes transform into polyp-like folds or changes in the mucous membrane such as focal hyperplasia (“warty gastritis”).
One of the most difficult problems is the relationship between erosions and chronic ulcers. The hypothesis about the continuous development of the process from ecchymosis through hemorrhagic erosion to ulcer did not meet with unanimous support. Some scientists argue that erosions and ulcers are different lesions that do not transform into one another. There is doubt that erosion is a prestage of an ulcer. Others do not completely deny the possibility of acute erosions turning into chronic ulcers. T. loshida during dynamic endoscopic examination observed the transition of acute erosions into acute multiple gastric ulcers.
We observed that erosive gastritis and duodenitis often precede the development of duodenal ulcers. It is also possible to develop erosions at the site of a duodenal ulcer during its healing. As you know, Japanese researchers consider this outcome to be one of the options for healing duodenal ulcers. A unique variant of peptic ulcer disease can also be considered simultaneous or staged recurrent damage by erosions of the terminal part of the esophagus, the outlet part of the stomach and duodenum, which was observed in several patients in the autumn and spring periods over a number of years.
Thus, there is an undoubted relationship between gastroduodenal erosions and peptic ulcer disease. This is evidenced, firstly, by relapses of the ulcerative process, starting with erosive lesions of the stomach, the debut and healing of duodenal ulcers in the form of erosions of the bulb, as well as the very frequent combination of erosive gastritis and duodenitis with duodenal ulcer (in 37 and 44% of cases, respectively ).
Undoubtedly, the question of the possibility of transforming erosive lesions into polyps and (or) stomach cancer is always very important.
The hypothesis of Japanese researchers about the transition of erosions through the stage of verrucous changes into polyps and cancer has been studied in different countries. L. It is possible to transform chronic erosions into polypoid formations, the morphological study of which reveals moderate changes in the gastric glands and cystically dilated ducts, but at the same time does not reveal typical signs of an adenomatous polyp. A group of researchers did not observe the development of polyps in patients with chronic erosions for 4 years.
Sometimes erosions develop at the apex of polyps; in this case, it is difficult to resolve the issue of the primacy of erosive damage. Long-term dynamic observation of 90 patients with chronic erosions revealed their disappearance, or the appearance in their place of focal hyperplasia (what endoscopists usually call “warty”, or verrucous, gastritis of the stomach). Nevertheless, the presence of focal hyperplasia at the site of chronic erosions, the peculiarities of the histogenesis of the epithelium in their area, and the identification of chronic erosions at the apex of polyps do not exclude the possibility of the evolution of chronic erosions with focal foveolar hyperplasia into hyperplasiogenic polyps. In any case, in our opinion, there is a possibility of such a transition.
The hypothesis about the natural evolution of chronic erosions into a cancer process is supported by few authors studying this issue. The research results do not confirm the hypothesis about the transition of erosions into a cancerous process.
Studies of the severity of dysplasia found in various lesions of the stomach (polyps, ulcers, erosions, chronic gastritis) indicate that with gastric erosions, mostly mild or moderate dysplasia is detected.
In our opinion, these data serve as indirect evidence of the thesis about the insignificant probability of malignancy in chronic erosions, but, of course, it is difficult to completely exclude such a possibility in a particular case. Therefore, the doctor must carefully examine the patient using gastrobiopsy and morphological study of drugs over time.
Summarizing the results of observations and literature data, we can assume that it is not yet possible to confidently support the hypothesis about the natural evolution of chronic erosions into a cancer process. We should first of all exclude the possibility of the existence of an early form of cancer (type II c) or ulceration that arose against the background of an infiltrative process in stomach (cancer, lymphomatosis). We cannot exclude the possibility of the simultaneous existence of a cancer process and chronic erosions in the stomach.
It is necessary to remember the existence of an early cancer process in the form of erosive and ulcerative lesions, which has been proven by the work of Japanese doctors (type II c). Secondly, we should talk about gastric erosions that accompany the development of a cancerous process in the stomach or tumors of the colon and rectum.
Diagnosis
The success of treatment depends on a correct diagnosis. At the Ardenium clinic, each patient is diagnosed individually and is prescribed only the necessary research methods that can identify the characteristic signs of the disease in order to make an accurate diagnosis. Exist:
- Physical research methods: inspection, palpation, percussion;
- Fibrogastroduodenoscopy – visual examination of the mucous membrane of the stomach and the initial part of the duodenum using fiber-optic technology;
- Ultrasound of the abdominal organs involved in the digestion process: liver, pancreas;
- Biopsy is a histological examination of biological samples taken from the walls of the stomach;
- Clinical and biochemical blood tests;
- Determination of pH of gastric juice;
- Fecal occult blood test.
Results of an application to the First Family Clinic of St. Petersburg
The priority task of our clinic’s specialists is not only to cure erosive gastritis, but also to eliminate the causes of this disease and any identified complications. This allows you to regain excellent health and quality of life that was disrupted by the disease. Using the latest advances in the field of gastroenterology allows us to guarantee the highest possible treatment results and return you to health.
“The First Family Clinic in St. Petersburg provides effective and comfortable treatment for erosive gastritis in our multidisciplinary centers. Our specialists are waiting for you in the Petrogradsky district at 16 Kamennoostrovsky Ave. (Petrogradskaya, Chkalovskaya, Gorkovskaya metro stations) and in the Primorsky district (at 36/2 Kolomyazhsky Ave. (Pionerskaya metro station) and "Specific").
To make an appointment, as well as to receive detailed information regarding the services of our clinic, call +7 (812) 300-5-300, order a call back or use the online appointment form with a doctor.
Treatment of erosive gastritis of the stomach
Treatment of erosive gastritis is multifaceted and is aimed at eliminating the causes that were the provoking factor in the development of the disease. It includes medications and diet therapy. Individually for each patient, taking into account the examination results, clinical picture, background diseases, the doctor draws up a treatment regimen and selects medications.
Goals of therapy:
- relief of the patient's condition;
- rapid restoration of the integrity of the gastric mucosa;v
- normalization of the functional activity of the organ;
- prevention of complications;
- correction of extragastric disorders (anemia, intestinal disorders).
- Symptoms of erosive gastritis determine both treatment and further prognosis of the disease.
Advantages of treatment at the Ardenium clinic
The Ardenium Medical Center is equipped with high-quality equipment, the examination of which provides reliable diagnostics. At the clinic, appointments are carried out by experienced specialists with the first and highest qualification categories, which confirms their high professionalism.
Doctors improve their knowledge through advanced training courses and take an active part in scientific and practical conferences and seminars. In complex cases, patients are advised by doctors with scientific degrees of candidates and doctors of science. The Ardenium Medical Center successfully uses both classical, well-proven diagnostic and treatment methods, as well as modern innovative technologies.
When the first signs of trouble in the stomach appear (a feeling of heaviness after eating, belching), you should not delay a visit to the doctor. Contacting a specialist will help you identify the causes of the pathology in a timely manner, properly treat and prevent complications, and in the chronic course of the disease, increase the period of remission.
An appointment with a gastroenterologist at the Ardenium Clinic can be made either by telephone or by filling out a special online form.
Acute erosive gastritis in the acute stage: treatment
To identify the causes of complaints with which the patient consulted a doctor, we use a wide range of diagnostic methods and tools.
For this purpose, expert-class medical equipment is used (digital ultrasound machine, Japanese-made fibrogastroendoscope, etc.) and laboratory tests of blood, urine, and feces. This provides the doctor with the most detailed picture of the disease and allows one to exclude other pathologies that have similar clinical manifestations.
Drug treatment of erosive gastritis is prescribed taking into account the results of the examination, and is an individual program developed for each patient separately.
Etiological factors
The disease develops acutely and is characterized by damage to the gastric epithelium in response to the influence of aggressive factors. The main causes of this type of gastritis are:
- long-term use of NSAIDs;
- alcohol abuse;
- mental stress, neuroses;
- radiation exposure;
- mucosal ischemia;
- iatrogenic damage to the organ when inserting a nasogastric tube;
- eating too spicy or hot food.
With erosive gastritis, acidity increases, which contributes to the progression of the disease. Point erosions that occur in the first day after the initial exposure can transform into extensive foci of epithelial damage. Most often, the process develops in the mucous membrane of the stomach.
Clinicians also highlight the acute stress-induced inflammation seen in intensive care unit patients. Pathogenesis is associated with decreased blood flow in the vessels of the abdominal cavity and lack of enteral nutrition.
Treatment approaches
Drug treatment includes long-term use of antisecretory drugs that provide a persistent increase in acidity in the stomach, which is necessary for rapid healing of erosions. For emergency treatment of bleeding, methods of surgical hemostasis (vessel clipping or electrocoagulation) are used.
Correction of water and electrolyte balance is carried out using infusion of crystalline and colloidal solutions.
Adequate treatment of the disease is impossible without prescribing a diet. The menu for erosive gastritis should consist of lean meats and fish, boiled or baked, cereals, stewed vegetables, and soups. Patients are advised to limit the consumption of fresh fruits and vegetables, meat broths, and yeast dough products as much as possible.
The prognosis is relatively favorable; with timely initiation of therapy, recovery occurs in most patients.