Sedatives are medications that reduce increased irritability, conflict, nervous tension, and have a slight calming effect by reducing the excitability of the nervous system.
Despite the wide selection of drugs with a pronounced sedative effect (tranquilizers), sedatives are used very actively, especially in cases of high nervous excitability, irritability, sleep disturbances, especially associated with negative emotions, and neurosis-like conditions that are accompanied by heart pain.
Unlike tranquilizers, sedatives, especially herbal ones, do not have such a pronounced calming effect. At the same time, sedatives are well tolerated by patients, they do not have serious negative effects - they do not cause muscle relaxation, gait disturbances, a feeling of lethargy, or a decrease in the speed of mental reactions.
To sedatives, addiction does not develop (decrease in effect with long-term use) and drug dependence (an irresistible need to use the drug again and again).
Due to these advantages, sedatives are very widely used throughout the world.
The best sedatives for the nervous system.
October 8, 2022
65535
4.9
9
Content
- How to choose a sedative
- Top 10 safe sedatives
- Dormiplant
- Magnesium-Diasporal
- Persen
- Avexima Dobrokam
- Novo-Passit
- Positive
- Stressovitis
- Tenoten
- Afobazole
- Motherwort Forte Evalar
Today's rhythm of life is a constant cycle of events, a “race”, during which each of us strives to complete a lot of tasks. Hence the eternal stress. And if we add here financial instability, problems in the family or at work... Often the nervous system simply cannot cope, which is fraught with neuroses and depression.
If you feel that you can’t cope on your own, and your nervous system is becoming more and more unstable every day, be sure to consult a doctor (neurologist, psychiatrist or psychologist) - he will select a sedative that will eliminate the problem and prevent negative consequences from developing.
How to choose a sedative
Our list of nerve pills are over-the-counter medications that are prescribed for minor stress, have a gentle effect on the nervous system and mostly contain natural ingredients. Typically, such medications are used for mild insomnia, when a person is nervous before an important event, for problems at work, in his personal life - in general, with increased emotional stress. But if, during treatment with sedatives, anxiety does not go away after a week or two, you need to consult a doctor again - he will prescribe stronger drugs.
Plant-based sedatives (such as Persen, Novo-Passit) are indicated for patients with temporary anxiety. If a person is under stress for a long time and feels negative symptoms, but there is no reason for this, it is necessary to check the thyroid gland, donate blood for anemia, vitamin D, and undergo tests for anxiety disorders and depression. In parallel with taking sedatives, it is important to learn relaxation techniques and talk to a psychologist to work through your anxious thoughts. Read also: Top 5 drugs for insomnia that are sold without a prescription The best over-the-counter drugs for the treatment of insomnia
Dormiplant
A sedative made in Germany, which contains valerian and lemon balm. Dormiplant helps well with increased nervous excitability and problems falling asleep. Contraindications include intolerance to the components of the drug, as well as liver failure. Dormiplant tablets are easy to swallow because they are not very large, round, with beveled edges. You need to take sedative tablets twice a day (morning and evening), 2 pieces, regardless of meals. Those who have taken this remedy write that Dormiplant is an excellent help for sleep problems. And if a person gets full rest at night, then during the day he is less irritable and is in a good mood. Dormiplant is often prescribed by neurologists for severe stress. Sometimes patients have adverse reactions - nausea and abdominal pain.
Dormiplant
Dr. Willmar Schwabe, Germany
increased nervous excitability;
insomnia (difficulty falling asleep). from 408
826
- Like
- Write a review
Dosage and duration of therapy
These factors are determined by a medical professional on an individual basis. If we consider the new generation of anxiolytics, they function softer and more gentle than other drugs. The first signs of improvement may be noticeable after a few days, but to overcome stressful situations you need to continue treatment for up to several weeks. The dosage differs significantly for each individual drug, so you need to pay due attention to the recommendations and instructions.
what are sedatives
Magnesium-Diasporal
This is a mineral complex to strengthen the nervous system and heart health. The drug contains 300 mg of magnesium, which completely covers the daily requirement of this mineral in the body. “Magnesium-Diasporal” is presented in the form of a powder, which must be dissolved in water, juice, tea, or simply poured into the mouth and washed down. Take this sedative once a day, regardless of food. The complex helps well with increased anxiety, problems falling asleep, aggression, increased fatigue, muscle cramps and cardioneurosis. Contraindications include age under 12 years, renal failure, breastfeeding (Magnesium-Diasporal is often prescribed to pregnant women to reduce the tone of the uterus and relieve irritability). It is a safe sedative, but its effect is temporary and it is expensive.
Magnesium-Diasporal
Protina Pharmazeutische GmbH, Germany
Indications for the drug Magnesium-Diasporal 300 are magnesium deficiency, accompanied by symptoms such as minor sleep disturbances, increased irritability, mild anxiety, increased fatigue, spasms of the calf muscles.
from 199
5.0 8 reviews
2517
- Like
- Write a review
Persen
A sedative that has long been prescribed by doctors and has proven itself to be excellent. Persen contains three active ingredients: mint, valerian and lemon balm. They soothe and relieve spasms. Persen is prescribed for insomnia, increased nervous agitation, irritability, and sleep problems. It should be borne in mind that these nerve pills are not suitable for people with low blood pressure and those who have problems with the biliary tract. The tablets are easy to swallow and can be taken with or without food. Dosage – 2-3 pieces per day. For insomnia, you need to take Persen an hour before bedtime, 2-3 tablets. The drug has a cumulative effect, it is safe, and has no withdrawal effect. A sedative helps eliminate the “nervous lump” in the throat. Rare side effects include allergic manifestations, constipation and bronchospasm.
Persen
Lek d.d., Slovenia
A sedative of plant origin, which is used for: increased nervous excitability;
- insomnia; - irritability; - depressive states; - panic disorders. from 190
5.0 1 review
1752
- Like
- Write a review
Classification of sedatives
Based on their origin, sedatives that are widely used in clinical practice are grouped into the following classes:
- herbal preparations: valerian extract, motherwort tincture, peony tincture, hawthorn tincture, passionflower extract, mint herb, lemon balm herb and combinations thereof;
- synthetic drugs: sodium bromide, potassium bromide, magnesium lactate, magnesium sulfate, phenobarbital.
In addition, many psychoactive substances can have a sedative effect and reduce the level of irritability. These drugs include anxiolytics (tranquilizers), antidepressants, some antipsychotics, as well as antiarrhythmic and antihypertensive drugs (for example, the β-blocker propranolol) and antihistamines and antiallergic drugs (for example, diphenhydramine).
Avexima Dobrokam
An excellent safe psycholeptic prescribed for sleep problems. "Avexima Dobrocam" contains 250 mg of bromcamphor and is prescribed for increased nervousness, tachycardia, pressure surges, insomnia and cardialgia. You can buy Avexima Dobrocam without a prescription; in small doses it is indicated even for children over 7 years old and pregnant women. Typically, the course of treatment with this sedative lasts two weeks (1-2 tablets three times a day). You cannot exceed the dosage on your own, because your body temperature may increase, convulsions and breathing problems are possible. While taking Avexima Dobrocam, the speed of reactions decreases, so it is better to avoid driving a car.
Dobrokam
Irbitsky Chemical Plant, Russia
- increased excitability;
- asthenia; - cardialgia; - tachycardia; - lability of blood pressure. from 146
618
- Like
- Write a review
Indications for use
Sedatives are used to treat neurasthenia - conditions that are accompanied by increased irritability, absent-mindedness, conflict, and nervous tension.
In addition, sedatives are used in the complex treatment of diseases that are easily aggravated by stress - angina pectoris (oxygen starvation of the heart), hypertension (persistently high blood pressure), gastric and duodenal ulcers, pruritic neurodermatoses (skin diseases that are accompanied by itching). ), migraine.
In addition, sedatives are used for hysteria, menopausal syndrome, and vegetative-vascular dystonia.
Novo-Passit
Another well-known plant-based sedative, which contains 7 medicinal plants: hops, St. John's wort, lemon balm, elderberry, valerian, hawthorn, passionflower, and guaifenesin (a substance that reduces anxiety). Novo-Passit has a complex effect: it suppresses anxiety and calms. The drug is prescribed for increased mental fatigue, sleep problems, nervous overexcitation, and mental stress. You need to take Novo-Passit three times a day, 1 tablet (usually before meals). If apathy and fatigue are felt while taking a sedative, the morning and daily dose can be halved. The interval between taking tablets should be at least 4-6 hours. In reviews, many people write that Novo-Passit begins to act almost immediately after the start of treatment. An important plus is the absence of drowsiness, lethargy and apathy, as well as the withdrawal effect. There are practically no side effects with Novo-Passit, rarely problems with digestion.
Novo-Passit
IVEX Pharmaceuticals, Czech Republic; Teva Pharmaceutical Industries, Germany
Novo-passit is a combination drug, the pharmacological activity of which is due to its constituent components of an extract based on medicinal plant raw materials with a predominantly sedative (calming) effect and guaifenesin, which has an anxiolytic (anti-anxiety) effect.
from 174
5.0 1 review
2561
- Like
- Write a review
Symptoms of stress
Photos from open sources
Positive
A herbal multi-component sedative to improve the functioning of the nervous system under increased psycho-emotional stress. The drug “Positive” is prescribed for causeless anxiety, prolonged stress, to improve mood during the day and for insomnia at night. The Positive capsules contain eleutherococcus, ginseng, and ginkgo biloba. All these natural ingredients have a gentle effect on the nervous system. The drug should be taken in the morning with food, the course of treatment is two weeks (can be repeated after 1-2 months). Contraindications include serious heart problems, hypertension, and pregnancy.
Positive
V-MIN+, LLC, Russia
As a food supplement - a source of tryptophan, eleutherosides, panaxosides, flavonoids, an additional source of selenium, vitamins (B6, B12, folic acid), containing 5-hydroxytryptophan.
from 214
197
- Like
- Write a review
Stressovitis
Natural sedative based on motherwort, linden, hops, vitamin B6 and magnesium. An excellent drug for those who are in a stressful situation, regularly experience nervous overload, feel irritability, unreasonable anxiety, and restlessness. You need to take only one Stressovit capsule per day with food. The course of treatment is 2-3 weeks. After a month you can repeat the course. Judging by the reviews of those who took Stressovit, the drug has a cumulative effect, it is well tolerated and has no side effects.
Stressovitis
Unifarm, USA
Stressovit is a complex biologically active remedy for reducing psycho-emotional stress, restoring the nervous system, relieving stress and increasing performance.
from 350
5.0 2 reviews
1802
- Like
- Write a review
Features of the treatment of neurasthenia
Tinctures and alcohol extracts contain ethanol, which causes the main side effects - general weakness, fatigue, indifference to the environment, weakened memory, drowsiness.
In addition, alcohol-containing sedatives reduce physical and mental abilities, so they are not recommended for use by patients whose work requires quick mental, behavioral and emotional reactions - drivers, dispatchers, operators, etc., as well as people with alcohol addiction. Such patients need to choose drugs without alcohol, for example, dry plant extracts or combinations thereof.
All sedatives enhance the effect of other drugs that depress the central nervous system - antipsychotics, tranquilizers, anticonvulsants.
Most sedatives cause a decrease in libido and potency.
Tenoten
Tenoten is a safe over-the-counter anxiolytic and nootropic based on antibodies to a brain-specific protein. The drug calms well, relieves anxiety, but does not inhibit or cause drowsiness. Tenoten is often prescribed for stress and the initial stages of depression. Calming lozenges are taken twice a day, 1-2 pieces. The course of treatment with Tenoten is 1-3 months. The positive effect of the medicine occurs within a couple of days after the start of treatment. "Tenoten" helps to establish normal sleep, ensures a good mood and relieves nervous tension. An important plus is the prolonged action of Tenoten: after the end of treatment, the sedative effect lasts for a long time.
Tenoten
Materia Medica Holding, Russia
TENOTEN is a calming drug with a stress-protective effect, indicated for all people with symptoms of anxiety: patients with anxiety disorders and healthy people in stressful situations.
The drug calms, relieves anxiety, irritability, nervousness, and evens out mood. Unlike other sedatives, it does not have unwanted side effects and does not have a sedative or muscle relaxant effect. In the treatment of somatic and neurological diseases, Tenoten has a vegetative-stabilizing and nootropic effect. from 152
1286
- Like
- Write a review
Read also Drugs to improve memory: neurologists recommend Drugs to improve blood circulation in the brain and memory.
Addictions caused by sleeping pills
Dependent sleeping pills consist of two groups - barbituric acid derivatives and non-barbituric substances. Abuse of sleeping pills listed as drugs is considered drug addiction, and abuse of other sleeping pills is considered substance abuse.
From the group of barbituric acid derivatives, drugs include sodium etaminal (Nembutal) and sodium amytal (Barbamyl). Of the non-barbiturate hypnotics classified as narcotics, Noxiron should be mentioned first.
The mechanism of their action and the nature of the dependence are similar. According to the terminology adopted by the WHO commission of drug experts, this type of addiction
is called
barbituric.
According to the life period (half-life) in the body and, accordingly, the duration of action, barbiturates are divided into 3 groups: a) short-lived (half-life 3-8 hours) - thiopental (pentothal), hexobarbital (hexonal); b) intermediate - amobarbital sodium (amytal sodium, barbamyl) - half-life 8-42 hours, pentobarbital sodium (ethaminal sodium, nembutal) - half-life 14-48 hours; c) long-lived (half-life 24-140 hours) - phenobarbital (luminal), veronal. The subject of abuse is most often drugs of the second group, less often - the first. Hypnotics are used both orally and intravenously.
Derivatives of barbituric acid were first used as hypnotics and sedatives in 1903 (Veronal). Then their range and scope of use began to rapidly expand, and drugs for intravenous use were created. Since the 1940s, barbiturates have been widely used to treat mental patients, in particular to treat depression. Some descriptions of disorders due to barbiturate use appeared already in the 30s and 40s. Already in the first edition of the textbook on psychiatry by V.A. Gilyarovsky (1931) one can find a mention of the possibility of addiction to barbiturates. In the 50s, in some foreign countries (USA, Norway), publications appeared that pointed out the dangers of barbiturate abuse and the possibility of developing addiction. In 1956, barbiturates were brought under international control, but despite this, the abuse of them and other sleeping pills continued to increase. This is primarily due to the fact that these drugs are very widely used in general medical practice.
Barbiturate dependence has many common features with alcohol abuse. They are determined by the fact that both alcohol and barbiturates, having some stimulating properties, have a more pronounced sedative effect.
Mechanism of action.
Barbiturates taken orally are absorbed in the small intestine. When released into the bloodstream, they bind to proteins and are metabolized in the liver. Approximately 25% of barbiturates are excreted unchanged in the urine, which is essential for diagnosing barbiturate intoxication.
The main mechanism of action of barbiturates is due to the fact that they penetrate the internal lipid layers and liquefy the membranes of nerve cells, disrupting their function and neurotransmission. Barbiturates block the excitatory neurotransmitter acetylcholine, while stimulating the synthesis and increasing the inhibitory effects of GABA. As addiction develops, cholinergic function increases while GABA synthesis and binding decreases. Both pharmacodynamic and metabolic components play a role in barbiturate tolerance. The metabolic component involves inducing liver enzymes. Tissues become less sensitive to barbiturates. Barbiturates can cause an increase in the stability of nerve cell membranes over time. In general, barbiturates have an inhibitory effect on the central nervous system, which is clinically manifested by hypnotic, euphoric, as well as sedative, anxiolytic and anticonvulsant effects. They potentiate the effect of analgesics; in toxic doses, they inhibit external respiration and the activity of the cardiovascular system (due to inhibition of the corresponding center in the medulla oblongata). With an overdose of barbiturates, previously intact individuals consistently develop disturbances of consciousness: stupor, stupor and coma. Severe poisoning is accompanied by a decrease in cardiovascular activity and hyporeflexia. Causes of death: respiratory failure, acute liver failure, shock reaction with cardiac arrest.
Clinical manifestations.
Among those who abuse sleeping pills, two groups of patients are distinguished [Kotlova L.M., 1973; Pyatnitskaya I.N., 1994; Smulevich A.B., 1983; Babayan E.A., 1988; Kaplan HL, Sadock BJ, 1988]. Patients of the first group begin to take sleeping pills in therapeutic doses as prescribed by a doctor or independently for various diseases. Persons belonging to the second group immediately begin to take sleeping pills in order to induce euphoria.
The first group includes primarily persons with neurotic mood disorders, social adaptation disorders, and alcoholism. Sleeping pills initially improve their subjective state - they relieve insomnia, smooth out affective disorders, and make the experiences associated with insufficient adaptation to the environment less relevant. But with constant long-term use of even therapeutic doses, mental dependence occurs. At the first stage, it is insignificant and taking the drugs can be stopped without significant discomfort. However, with long-term regular use of sleeping pills, the previous therapeutic dose gradually ceases to have the desired effect, and there is a need to increase the dose, i.e. tolerance arises. Mental dependence is also increasing. The patient believes that normal sleep is impossible without sleeping pills. Gradually, the doses of the drug begin to exceed therapeutic doses, which leads to the formation of physical dependence.
The timing of the formation of dependence is determined by the dose, frequency of taking the drug and method of administration. According to I.N. Pyatnitskaya (1994), the minimum daily dose of barbiturates, which can cause physical dependence within 3 months of daily use, is 0.5 g of sodium amytal; daily intake of 0.8 g of barbiturate can initially cause an increase in tolerance, the formation of mental, and then after 1-1.5 months of physical dependence.
Many patients with all kinds of agrypnic neurotic disorders can take double therapeutic doses of sleeping pills for a long time (years), they experience a very slow increase in tolerance, although mental dependence on the drugs is formed and mild organic personality changes appear (lack of concentration, memory impairment, slowness, mood disorders ).
The transition from abuse to addiction usually occurs unnoticed by the addict himself. The symptoms of the disease develop in a very short time. One of the important signs of a developed addiction is taking sleeping pills during the daytime. Although patients are often not aware of this and believe that taking sleeping pills during the day only “calms them down,” this can serve as an important differential diagnostic sign of an emerging disease.
Patients belonging to the second group immediately begin to take sleeping pills in search of euphoria, using double and triple therapeutic doses for this. In these cases, the goal of obtaining euphoria is especially important. The onset of the disease in this group of patients occurs quickly, especially with intravenous administration of the drug.
The euphoric effect of barbiturates in the two groups mentioned is different. In the first group of patients who took therapeutic doses for a long time, and then began to increase them, euphoria is more smoothed out, occurs when taking doses of 0.4-0.5 g, manifests itself in an improvement in the emotional state, an uplift in mood, as well as in activation, tide strength, energy, desire to move, speak, increased appetite. This state lasts up to 4 hours and turns into sleep with light and pleasant dreams. Patients wake up with a feeling of vigor, relaxation and good mood. They usually do not regard this condition as intoxication and claim that they take increased doses of barbiturates in order to improve performance. Patients of the second group, having a focus not on falling asleep, but on a euphoric effect, take the drugs from the very beginning in an environment that prevents falling asleep. Moreover, they use intravenous administration, in which an initial dose of 0.3 g can immediately induce euphoria that lasts 6 hours and progresses to sleep. Upon awakening, amnesia of intoxication is almost always noted.
Gradually, during the process of anesthesia, the initial euphoric effect begins to decrease and tolerance develops. In the first group of patients, the need for increasing doses arises after a longer period - after 6-12 months, reaching a level of 0.6-2 g. In the second group, tolerance during intravenous administration develops very quickly - within several days of continuous use of the drug in doses, exceeding therapeutic levels, and when taken orally - after 1 - 1.5 months. There is cross-tolerance between barbiturates and alcohol.
Subsequently, the formation of drug addiction occurs in both groups according to the same patterns.
After 2-3 years of regular use of barbiturates, the need for further increases in doses decreases, and tolerance reaches a certain limit. The duration of dose stabilization period in the first group is several years, in the second group it is 4-6 months. Then there is a tendency to reduce doses. During this period, patients suffering from barbituromania often experience overdoses.
As is known, the physiological effect of sleeping pills consists of two phases: in the first, short phase, a stimulating effect is manifested, in the second, longer phase, a sedative effect. Tolerance develops primarily to the sedative effect.
In contrast to opium addiction, with barbituromania the upper limit of the dose that the patient can tolerate does not differ so sharply from the initial dose that can cause euphoria, i.e. The range between narcotic and lethal doses is small. In this case, when taking a constant dose, the stimulating effect may become predominant, forcing the patient to increase the dose to obtain the desired sedative effect, sometimes to life-threatening levels. This leads to overdose.
After stopping taking barbiturates, tolerance drops very quickly: 2-3 weeks after stopping taking the maximum tolerated dose returns to the original level. Hence the frequency of overdoses and deaths after patients are discharged from the hospital. According to some authors [Pyatnitskaya I.N., 1994; Kaplan HL et al., 1988], overdoses in barbituromania are almost inevitable at a certain stage.
An overdose of barbiturates is accompanied by dizziness, nausea, and vomiting. L.M. Kotlova (1972) describes in overdoses the presence of profuse sweat, hiccups, a feeling of lightheadedness, pain in the eyes, and drooling. After vomiting, relief may occur. During the process of anesthesia, 4-6 months after the first overdose, taking large doses is no longer accompanied by the listed phenomena, and without any warning signs, loss of consciousness occurs, followed by amnesia.
When dependent on barbiturates, when not taking them, a state of dissatisfaction and weakness develops, accompanied by “dark thoughts,” anxious concerns, fears, and irritability, which intensify in the evening. Insomnia is also common. Taking barbiturates in these cases becomes a source of calm and satisfaction.
With intravenous administration, as well as with opiate addiction, barbiturate drug addicts highlight the first phase of the action of sleeping pills - the “arrival”. It occurs immediately and, according to the descriptions of patients, lasts several seconds. Patients say that their “consciousness has blacked out,” “their head has gone spinning,” “it’s dark in the eyes,” and the surroundings are not perceived. After a few seconds, the second phase of the action of the sleeping pill begins, reminiscent of alcohol intoxication. It is characterized by motor activity, causeless fun, a desire to move and at the same time disordered movements, distractibility of attention, a reduced level of judgment, and irritability. Cheerfulness sometimes immediately turns into anger. Patients are either disinhibited or drowsy. There is a progressive deterioration in motor coordination, euphoria or depression. Paradoxical motor agitation, bradycardia, and slurred speech are possible.
In a somatic state, attention is drawn to a decrease in urination, a decrease in blood pressure and body temperature, hypersalivation, hyperemia of the sclera and skin, increased sweating; skin with a characteristic greasy tint; the tongue is coated with a dirty gray coating. A neurological examination reveals lateral nystagmus, diplopia, dysarthria, dysmetria, impaired coordination of movements, instability when walking and standing, decreased tendon and abdominal reflexes, dilated pupils, and sluggish reaction to light. This state lasts 2-3 hours. Gradually, mental and motor activity decreases, and the patient falls asleep. The sleep is heavy, deep, and it is difficult to wake up a drugged person. Muscle hypotonia is pronounced. If sleep occurs during the day, it is short. It may be difficult to fall asleep the next night. Upon awakening, lethargy, weakness, weakness, and inability to concentrate are noted. Sometimes there is muscle weakness, tremors, and often headache. Nausea and vomiting are possible. There is no appetite, and there is often thirst. In some cases, a glass of hot water renews the feeling of intoxication: dizziness, increased mood, increased activity.
Diagnosis of barbiturate intoxication.
Rough neurological symptoms distinguish this intoxication from alcoholic intoxication. Therefore, the doctor’s attention should be drawn to dysarthria, ataxia, lack of coordination of movements, large lateral nystagmus, sharp dilation of the pupils with a sluggish reaction to light, hypersalivation, hyperhidrosis, a tendency to anger and aggression.
Intoxication with sleeping pills differs from opiate anesthesia by impaired consciousness, the above-mentioned neurological symptoms, pupil size, skin color, hypersalivation, hyperhidrosis, inability to dissimulate, and lack of ease of emotions.
In contrast to hashish intoxication, in these cases there are pronounced neurological symptoms and more severe affective reactions with anger and aggressiveness.
After about 6 months, with regular use of barbiturates, physical dependence is formed, characterized by the occurrence of withdrawal syndrome. By this time, tolerance has already been established at the same level - 1 g, sometimes 1.5-2 g. The nature of intoxication changes. During intoxication, mobility is maintained, but the movements are quite coordinated. Retardation and gross awkwardness of movements disappear. Intoxication, unless there is an overdose, is not accompanied by impaired consciousness. There is no disinhibition and talkativeness that is observed in the initial period. Affects become stuck, and attacks of anger and aggression are possible. During the period of intoxication, speech is monotonous and monotonous, oligophasic, with perseverations. The affect is angry, stagnant, reminiscent of the affect of a patient with epilepsy. Sleep is further disrupted. The patient can fall asleep only when taking an increased dose of sleeping pills. In case of overdose, there is no vomiting, no sleep occurs, and coma immediately develops without the sleep stage. Very characteristic is the loss of quantitative control during intoxication and, as a consequence of intoxication, a deep disorder of consciousness with subsequent amnesia. Overdoses are more common, often fatal. Compulsive craving for drugs is expressed.
Withdrawal syndrome
with abuse of sleeping pills, severe. It occurs within the first 24 hours after withdrawal of the drug, reaches its peak severity on the 3-4th day and is slowly reduced.
By the end of the first day after drug withdrawal, the mood of patients becomes anxious and melancholy, with anxiety being in the foreground. Irritability, touchiness, short temper, tearfulness are expressed, sleep is upset. For the first 1-2 nights, patients sleep, although little (no more than 5-6 hours), with nightmares and severe sweating. On the 2-3rd day, sleep disturbances reach a maximum, up to complete insomnia. During the same period, affective disorders, dysphoria, and agitation also reach their maximum. Suicidal tendencies and demonstrative self-cutting are common. Subsequently, progressive weakness, dizziness, and distortion of visual perception are observed. Blood pressure is unstable, and a sharp drop may occur, leading to collapse and death. Such cardiovascular disorders are especially typical for barbituromaniacs who use high doses of drugs. On the 3-4th day, unpleasant sensations arise in different parts of the body, pain in large joints (knees, shoulders, elbows), aching pain in the pit of the stomach, nausea, vomiting, weight loss. All patients have tremor of the eyelids, fingers of outstretched arms, and tongue. Involuntary muscle twitching, mainly in the calf muscles, is very characteristic.
Withdrawal syndrome from abuse of sleeping pills is dangerous due to the occurrence of convulsive seizures and psychoses. They are observed when taking large doses of drugs and can replace each other. Thus, a patient may have 1 or 2 convulsive seizures during the first day after discontinuation of the drug, and psychosis develops on the 2-3rd day (usually at night).
Convulsive phenomena occur more often on the 3-5th day of deprivation or a significant reduction in doses of sleeping pills. They are characterized by full-blown convulsive seizures, indistinguishable from seizures in genetic epilepsy. According to JHJaffe (1989), 75% of patients using at least 0.8 g of fast-acting barbiturates per day experience seizures, and those using higher doses experience grand mal seizures.
Psychosis occurs on the 3-8th day of deprivation or a sharp reduction in large daily doses of sleeping pills. Psychoses are usually represented by delirium, less often - verbal hallucinosis. Delirium caused by deprivation of sleeping pills is similar in clinical manifestations to alcohol delirium. It is distinguished by the greater severity of anxiety, tension, and anger of patients, the rarity of tactile hallucinations, the greater proportion of auditory hallucinations, and the presence of muscle twitching. Rarely occurring hallucinatory delusional psychoses resemble schizophrenic psychoses. Their structure includes hallucinations and delusions; patients may be in a substupor or, on the contrary, exhibit panic reactions.
Withdrawal syndrome from abuse of sleeping pills lasts an average of 3 weeks, sometimes up to 4-5 weeks. Mood disorders, periodic craving for drugs, poor sleep, dysphoric reactions, and decreased appetite can last the longest. A turning point during abstinence is noted with the appearance of appetite - on the 10th-14th day. Considering the possibility of developing epileptic seizures and psychoses, suicidal tendencies, as well as severe somatic consequences, withdrawal syndrome from the abuse of sleeping pills is life-threatening for patients.
In advanced cases, withdrawal syndrome can transform. It becomes protracted (up to 2 months or more), although its symptoms seem to lose their severity. The pain syndrome is less pronounced, the intensity of pain decreases, dysphoria is replaced by sluggish subdepression. Sometimes persistent depression with suicidal tendencies comes to the fore. The somatic status is dominated by functional disorders of the cardiovascular system: collapse, signs of myocardial dystrophy on the ECG. Convulsive seizures often become serial (5-10 seizures per day) and are not controlled by anticonvulsants. This corresponds to epileptiform changes on the EEG. Severe delirious states are also observed.
Consequences of long-term drug addiction.
With prolonged abuse of sleeping pills, a peculiar defect is formed very quickly, reminiscent of a psychopathic-like organic one. Fatigue, exhaustion of attention, insufficient ability to concentrate, and the impossibility of intense mental activity appear. Working capacity gradually decreases: patients work only for short periods, provided they take a sufficient dose and achieve a state of mental and physical comfort during the period of intoxication. The circle of interests is narrowing. Patients become irritable, dysphoric, and angry.
The appearance of patients is characteristic: they are pale, pasty, their complexion has a dirty earthy tint, their tongue is coated. Trophic disorders are noted: wounds do not heal for a long time, they fester; many skin pustular rashes; eyes lose their shine; hair becomes brittle.
Gradually, patients develop a state of toxic encephalopathy, manifested in slowness of thought processes and speech, and a pronounced intellectual-mnestic decline. Characteristic barbituric dementia
with decreased intelligence, difficulty with the slightest mental effort, slowness of thinking, slow speech, limited vocabulary, severe memory impairment. Patients are not critical of their condition and the disease in general. They do not have any moral and ethical standards of behavior. They are dirty and sloppy. The state of lethargy and apathy is often replaced by severe dysphoric reactions with anger, sometimes aggressiveness. The face is amicable, mask-like. Personality changes are pronounced. Patients are selfish and deceitful. Moral degradation exceeds that of all other forms of drug addiction. All this together creates the characteristic appearance of patients who abuse sleeping pills for a long time. A.B. Smulevich (1983) compares the initial state of barbituromania with a pseudoparalytic one.
Afobazole
The active ingredient of Afobazole is fabomotizole (tranquilizer). This sedative is prescribed for autonomic disorders, anxiety, depression, and cognitive disorders. Afobazole is usually well tolerated, although it can sometimes cause headaches. Take the drug three times a day, 1 tablet after meals. The course of treatment with Afobazol is 2-4 weeks. The positive effect of the sedative occurs on the 5-7th day of treatment and persists after discontinuation of the drug for another 7-14 days. Patients write that Afobazole is well tolerated, does not cause drowsiness or decreased concentration, and does not cause muscle weakness, dependence, or withdrawal symptoms.
Afobazole
OJSC Pharmstandard-Leksredstva, Russia
Afobazole is used in adults for anxiety conditions: generalized anxiety disorders, neurasthenia, adaptation disorders.
The drug is also prescribed for somatic diseases: bronchial asthma, irritable bowel syndrome, systemic lupus erythematosus, hypertension, coronary heart disease, arrhythmias. from 204
2240
- Like
- Write a review
Sedatives and hypnotics
Sedatives (from the Latin Sedatio - calm) have a regulatory effect on the processes of inhibition and excitation in the central nervous system, facilitate the onset of sleep, enhance the effect of hypnotics, analgesics and other neurotropic substances. They are usually well tolerated, do not cause serious side effects, addiction or dependence, and do not have extensive contraindications for use. This group of drugs includes preparations of valerian and other plants, bromides.
| | Attention! Do not start pharmacological treatment without consulting a psychiatrist |
1. Rhizomes with roots of valerian (Rhizomatа cum radicibus Valerianae). They prepare tinctures, infusions, valerian extracts, sedative mixtures, and make camphor-valerian drops. Valerian preparations contain essential oil, the main part of which is the ester of borneol and isovaleric acid, free valeric acid and borneol, organic acids, including valeric acid (C-15 H-12 0–2), which has an antispasmodic effect, tannins, alkaloids, sugars and other substances.
2. Valocormidum . Ingredients: velerian tincture (10 ml), lily of the valley tincture (10 ml), belladonna tincture (5 ml), sodium bromide (4 g), menthol (0.25 g), distilled water (up to 30 ml). Soothing and antispasmodic. Used to treat cardiovascular neuroses accompanied by bradycardia. Prescribe 10–20 drops 2–3 times a day before meals. Available in 30 ml bottles.
3. Valosedan . Ingredients: valerian extract (0.3 g), hop tincture (0.15 g), hawthorn tincture (0.133 g), rhubarb tincture (0.83 g), sodium barbital (0.2 g), ethyl alcohol (20 ml ), distilled water (up to 100 ml). Used to treat neuroses and neurosis-like conditions, 1 teaspoon 2-3 times a day.
4. Corvalolum. Composition: ethyl ester of a-bromoisovaleric acid (about 2%), phenobarbital (1.82%), sodium hydroxide (to convert phenobarbital into soluble phenobarbital sodium - about 3%), peppermint oil (0.14%), mixture ethyl alcohol 96% and distilled water up to 100%. Similar to foreign Valocordin (milocordin). Has a sedative, mild hypnotic, antispasmodic effect. Used to treat neurasthenia with irritable weakness, mild coronary spasms, tachycardia, sleep disorders, intestinal spasms, early stages of hypertension. Prescribed orally before meals, 15–30 drops 2–3 times a day. The dose can be increased to 40–50 drops (for tachycardia and vascular spasms). Available in 15 ml bottles.
5. Motherwort herb (Herba Leonuri). Contains essential oil, saponins, tannins, alkaloids. In terms of action and indications for use, it is close to valerian. Motherwort tincture (Tinktura Leonuri) is taken 30–50 drops 3–4 times a day before meals. Liquid motherwort extract is taken 20 drops 3 times a day.
6. Passionflower herb (Herba Passiflorae). Passionflower tincture and extract have a calming and anticonvulsant effect. Passionflower extract is taken 20–40 drops 2–3 per day for 20–30 days.
7. Sodium bromide (Natrii bromidum). Used as a sedative and anticonvulsant. It is prescribed orally before meals in tablets and mixtures, as well as intravenously. When taken orally, the dose for adults is from 0.1 to 1 g 3-4 times a day. For children under 1 year - 0.05-0.1 g, up to 2 years - 0.15 g, 3-4 years - 0.2 g, 5-6 years - 0.25 g, 7-9 years — 0.3 g, 10–14 years — 0.4–0.5 g. Available in powders and tablets of 0.5 g; 3% solution in 100 ml bottles.
8. Potassium bromide (Kalii bromidum). Prescribed orally 0.5 g 2-3 times a day. In pediatric practice, a solution of potassium bromide (1%, 2% and 3%) is used.
9. Bromcamphora. Prescribed orally after meals in powders, tablets for adults - 0.15-0.5 g 2-3 times a day, children under 2 years old - 0.05 g, 3-6 years old - 0.1 g, 7-9 years old - 0.15 g, 10-14 years - 0.15-0.25 g 2-3 times a day.
10. Sympathil. Sedative, calming combined remedy (includes in one tablet dry esolate extract 20 mg, hawthorn flower extract 75 mg, magnesium oxide 124.35 mg, microcrystalline cellulose, salt carboxymethyl starch (type A), stearic acid, azorubine (E 122). Eliminates anxiety , increased emotionality, reduces the excitability of the central nervous system and cardiovascular system, normalizes sleep.
Prescribed orally before meals, 2 tablets per day (morning and evening).
Side effects: gastralgia, diarrhea. Contraindications for use: severe renal failure, hypersensitivity, pregnancy, breastfeeding. It is not recommended to combine with medications containing quinidine (renal excretion of quinidine is reduced due to alkalinization of urine and its overdose is possible). In case of an overdose of Sympathil, there may be a delay in urination.
Release form: tablets.
Sleeping pills, or hypnotics, are no longer the same as they were used relatively recently. Barbiturates have practically gone out of use; their place has been taken by tranquilizers with a hypnotic effect, antidepressants, and some neuroleptics. However, the new drugs are far from ideal sleeping pills. The following sleeping pills are mainly used.
1–3. Nitrazepam, flunitrozepam, triazolam - see “Tranquilizers”.
4. Bromizovalum. N-(a-bromoisovalerianyl)-urea. Synonyms: Bromural, Bromodorm, Sedural, Somnurol, etc. Has a calming and moderate hypnotic effect. Well tolerated. As a sedative, adults are prescribed 0.3-0.6 g 1-2 times a day, and as a sleeping pill - 0.6-0.75 g half an hour before bedtime. For children, bromizal is prescribed for insomnia, chorea, whooping cough, 0.03–0.1–0.25 g per dose. Available in tablets of 0.3 g in a package of 10 pieces. It is included in the anticonvulsant drugs gluferal, pagluferal, and in the Sereysky mixture.
5. Methaqualone . Synonyms: Dormogen, Dormotil, Motolon, Bendor, Holodorm, Mekvalon, Revonal, Somnidon, Tofinal, etc. A sedative, hypnotic with anticonvulsant and antitussive effects. Enhances the effect of barbiturates, analgesics, and neuroleptics. Mainly used in the treatment of insomnia. Prescribe 0.2 g orally half an hour before bedtime. When waking up early, take another 0.1 g. It is usually well tolerated. Available in tablets of 0.2 g in a package of 10 pieces.
6. Zopiclone - see "Tranquilizers".
7. Hemineurin. Synonyms: Geminevrin, Chlomethiazole, Somnevrin, etc. It is a derivative of chlormethiazole. It has a sedative, hypnotic and anticonvulsant effect. Indicated for the treatment of sleep disorders, status epilepticus, delirium, eclampsia and pre-eclamptic conditions, alcohol withdrawal, for the relief of mania, acute psychomotor agitation and pain relief during labor.
Prescribed orally and intravenously. As a sleeping pill, 2-4 capsules are prescribed (in capsules the drug is absorbed faster and acts more actively than in tablets) or tablets before bedtime, as a sedative - 1-2 capsules (tablets) 1-2 times a day before meals. For status epilepticus and delirium, the drug is administered intravenously in a stream of 40–100 ml of a 0.8% solution for 3–5 minutes or intravenously in a drip of 60–150 drops per minute until sleep; then the infusion is slowed down, maintaining shallow sleep (a total of up to 500–1000 ml is administered). Acute withdrawal syndrome is stopped by prescribing 2–4 capsules orally on the first day (after half an hour you can add 2 more capsules), on the 2nd and 3rd days - 3 capsules, on the 4th–6th day - 2 capsules and subsequent 4 days - 1 capsule. Mania is relieved by intravenous infusion of 40–80 ml of a 0.8% solution of the drug; for eclampsia, 30–50 ml of solution is administered dropwise (60 drops per minute), and upon the onset of drowsiness, the dose is reduced to 15–10 drops per minute. For labor pain relief, 2-3 capsules are prescribed, adding 2-3 capsules every 3 hours if necessary (no more than 7 capsules in total).
Side effects: local phlebitis, respiratory depression, hypotension and collapse, dyspepsia, allergic reactions. Patients with alcoholism may become dependent on the drug, so it should not be prescribed for more than 7 days in a row.
Release forms: capsules and tablets of 500 mg of gemineurin; 0.8% solution in bottles of 100 and 500 ml.
8. Ivadal. Synonym: Zolpidem, Ivadal. Selectively excites the omega 1 receptor subtype of the GABA-A receptor complex, promotes the opening of chloride channels, and potentiates inhibition processes in the central nervous system. Strengthens (mutually) the effect of sedatives, is incompatible with alcohol. In therapeutic doses, it shortens the period of falling asleep, reduces the number of night awakenings, lengthens the duration of the 2nd–4th phases of slow-wave sleep, and improves its quality. Indicated for the treatment of sleep disorders.
It is prescribed orally just before bedtime, once. The dose is individual. Adult patients are usually given 10 mg, persons over 65 years of age - 5 mg (if necessary - no more than 10 mg). For situational sleep disturbances, the drug is taken for 2–7 days, for chronic insomnia - up to a month, no more.
Side effects: drowsiness, headache, dizziness, gait disturbance, agitation (at night or upon cessation of treatment), anterograde amnesia, confusion, visual disturbances, nightmares, abdominal pain, dyspepsia, skin rash, itching; with long-term therapy - addiction, dependence.
Contraindications for use: sleep apnea, severe myasthenia gravis, severe respiratory or liver failure, breastfeeding, pregnancy, breastfeeding, hypersensitivity. In case of overdose - stunning consciousness up to coma (gastric lavage, intake of activated charcoal, symptomatic therapy are necessary). Use with caution in case of respiratory and liver failure; combination with benzodiazepines is undesirable.
Release form: tablets of 10 mg in packages of 7 and 10 pieces.
For other drugs with sedative and hypnotic effects, see the headings “Neuroleptics”, “Antidepressants”, “Tranquilizers” and “Nootropics”.
Back to contents
Motherwort Forte Evalar
A sedative tonic drug with a mild effect, which can be bought without a prescription. “Motherwort Forte Evalar” has been used for a long time, so it is time-tested. This natural remedy contains motherwort extract, magnesium carbonate and vitamin B6. The medicine reduces nervous tension, relieves irritability and unjustified anxiety. Motherwort Forte smoothly lowers blood pressure, works as a mild muscle relaxant, and strengthens the heart muscle. Even with prolonged use, this sedative is not addictive. Usually Motherwort Forte is taken 1-2 tablets per day with meals. Contraindications include peptic ulcer, pregnancy, gastritis during an exacerbation.
Motherwort Forte Evalar
Evalar, Russia
Motherwort Forte Evalar helps to quickly relieve nervous tension and irritability, and improve emotional well-being.
Its unique composition contains exactly that variety of motherwort, which grows in Altai and has one of the highest rates of sedation. In addition, only in Motherwort Forte Evalar the high daily dosage of motherwort (100 mg) is enhanced with the “elements of calm” magnesium and vitamin B6. from 9
4.5 2 reviews
619
- Like
- Write a review
Psychiatry Psychiatry and psychopharmacotherapy named after. P.B. Gannushkina No. 06 2022
The article discusses the state of affairs with anxiolytics, hypnotics and sedatives in the clinical practice of a psychiatrist in Russia at the present time. Topical issues of the applied use of drugs, their features, and prescription tactics are covered.
Keywords:
anxiolytics, hypnotics and sedatives, benzodiazepine tranquilizers, tranquilizers in Russia, anxiolytics in Russia.
For citation:
Maslov K.A. Anxiolytics, hypnotics and sedatives in Russia in modern clinical practice of a psychiatrist. Issues of applied practical application. Psychiatry and psychopharmacotherapy. 2019; 21 (6): 4–10.
Anxiolytics, hypnotic drugs and sedatives in Russia, in modern clinical practice of the psychiatrist. Questions of applied practical application
K.A. Maslov
Evgrafov Regional Mental Hospital, Penza, Russia
Abstract
In the article there is a speech about a situation with anxiolytics, hypnotic drugs and sedatives in clinical practice of psychiatry in Russia now. Relevant issues of applied use of these drugs, their features, appointment tactics.
Key words:
anxiolytics, hypnotic drugs and sedatives, benzodiazepine tranquilizers, tranquilizers in Russia, anxiolytics in Russia.
For citation:
Maslov KA Anxiolytics, hypnotic drugs and sedatives in Russia, in modern clinical practice of the psychiatrist. Questions of applied practical application. Psychiatry and Psychopharmacotherapy. 2019; 21 (6): 4–10.
Introduction
Anxiolytics - drugs that reduce anxiety and restlessness, according to the international (recommended by the World Health Organization - WHO) anatomical-therapeutic-chemical classification belong to group "N" (drugs for the treatment of diseases of the nervous system), namely N5 (psycholeptics), subgroup - N05B (anxiolytics) [1]. The group of psycholeptics also includes subgroups N05A (antipsychotic drugs) and N05C (hypnotics and sedatives). A somewhat outdated name for anxiolytic drugs is tranquilizers, and an even more outdated one is the so-called “minor tranquilizers” (“major tranquilizers” were previously called antipsychotic drugs) [2–5]. Currently, the overwhelming number of anxiolytics are representatives of the group of benzodiazepines, the mechanism of action of which is based on the effect on a certain area (site) of one of the types of receptors for gamma-aminobutyric acid (GABA), namely the GABAA receptor. As a result, the affinity of the GABA inhibitory transmitter of the central nervous system (CNS) to these receptors increases and its effect increases (increasing the inhibitory postsynaptic potential), the excitability of neurons in the CNS, as well as in the periphery (in spinal cord cells and peripheral tissues), decreases. These receptors are sometimes called benzodiazepine receptors [6]. Nowadays, the most common and prescribed group of anxiolytics in Russia and in the world are benzodiazepine derivatives (the so-called benzodiazepine tranquilizers, or benzodiazepines) [7–9], so further we will mainly talk about them.
A Brief History of Anxiolytics, Hypnotics and Sedatives
The first fairly powerful representatives of the group (except for bromine and valerian preparations) were derivatives of barbituric acid (the so-called barbiturates), namely barbital, which has been used in clinical practice since 1903 [10], with a mechanism of action somewhat similar to benzodiazepines ( including modulating the GABAA receptor). Then, from the 2nd half of the 1950s, benzodiazepines appeared (one of the first, chlordiazepoxide, synthesized in 1955, entered clinical practice in 1960) [11]. Subsequently, a large number of benzodiazepines appeared, the most successful of which, and subsequently the “gold standard,” was diazepam, which entered clinical practice in 1963 [12]. In the 1950s, the problem of barbiturate addiction was recognized worldwide [13]. The advent of benzodiazepines by the 1970s significantly reduced the distribution and prescription of barbiturates, almost completely replacing them with benzodiazepine tranquilizers in the treatment of anxiety and sleep disorders, shifting barbiturates to the niche they occupy to this day (mainly as drugs for anesthesia and for the treatment of epilepsy) [11]. In the 1980s, benzodiazepines suffered the same fate as barbiturates, and the problem of dependence on them was recognized [14]. Since the 1980s, the so-called “Z-drugs” (non-benzodiazepine benzodiazepine receptor agonists) entered clinical practice: zopiclone - since 1986, zolpidem - since 1992, zaleplon - since 1999, which partially replaced benzodiazepines from therapy sleep disorders and have firmly occupied the niche of selective sleeping pills [15]. Currently, there are drugs with a mechanism of action not related to the effect on benzodiazepine receptors, such as hydroxyzine (used in clinical practice since 1956) [16, 17], etifoxine (since the 1960s) [18], buspirone ( since 1986) [19–21]. It is also necessary to note the presence on the Russian market of such popular non-benzodiazepine drugs as tetramethyltetraazabicyclooctanedione (in clinical practice in Russia since 1978) [29], preparations of valerian rhizomes and fabomotizol (in clinical practice in Russia since 2005) [30].
Treatment and side effects
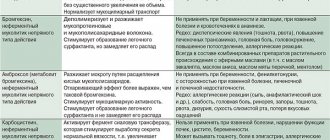
Anxiolytics, hypnotics and sedatives (mainly the benzodiazepine group) have four main therapeutic effects [22, 23]: • hypnotic; • anxiolytic; • anticonvulsant; • muscle relaxant; • sedative1; • vegetative stabilizing1. The downside of the therapeutic effects are side effects and complications, the most common are excessive sedation and drowsiness, the risk of falls, memory and concentration problems, withdrawal symptoms and the risk of addiction, disruption of sleep architecture, dizziness, paradoxical effects in the form of reactions of intoxication and arousal. and aggression [22]. The degree of severity and the relationship between therapeutic and side effects determines the range of clinical use of the drug. The main clinically significant problems with the use of benzodiazepine tranquilizers and tactics for their prevention and correction are presented in Table. 1.
Currently in Russia (according to some estimates) [7–9], the most popular anxiolytics in clinical practice are (in descending order) tofisopam, tetramethyltetraazabicyclooctanedione, bromodihydrochlorophenylbenzodiazepine, diazepam, fabomotizol. Of the hypnotics and sedatives, the most popular in clinical practice in Russia [7–9] are (in descending order) melatonin and zopiclone. For comparison, currently in the USA (according to some estimates) [26], the most popular among the group of anxiolytics in clinical practice are (in descending order) alprazolam, clonazepam (according to the anatomical-therapeutic-chemical classification, it is assigned to group N03 - antiepileptic drugs, although in fact is a benzodiazepine tranquilizer and has a powerful anti-anxiety effect), lorazepam, buspirone, hydroxyzine, diazepam. Of the hypnotics and sedatives, the most popular in clinical practice in the United States [26] is zolpidem.
Classifications
There are several classifications of anxiolytics, hypnotics and sedatives. Some experts in the field of psychiatry propose a classification of drugs (in particular antipsychotics) based on their receptor mechanism of action [31]. This approach is logical and consistent, and also perfectly complements clinical classifications. Obviously, a similar approach would be relevant for the classification of drugs from the group of anxiolytics, hypnotics and sedatives (we can distinguish, for example, benzodiazepine receptor agonists and a group of drugs with non-benzodiazepine receptor action). Perhaps in the future, researchers will attempt a similar classification of these drugs. Based on the duration of action (half-life - T1/2), anxiolytics, hypnotics and sedatives are divided into several groups. There are several approaches to classification by duration of action. Domestic researchers identify drugs with short (up to 5 hours), medium (5–24 hours) and long-acting (more than 24 hours) effects [24]. American and European researchers distinguish [32, 33] drugs with short (up to 6 hours), medium (6–24 hours) and long (more than 24 hours) action. Australian researchers identify drugs with ultrashort (up to 6 hours), short (6–12 hours), medium (12–24 hours) and long (more than 24 hours) action [25]. It should be noted that these classifications overlap in many ways. Taking into account the average WHO recommended sleep duration [34] and the average daylight hours in the Northern Hemisphere in the European part of Russia, the classification of researchers from Australia seems to be the most suitable for clinical practice [25]. The classification of anxiolytics, hypnotics and sedatives by duration of action (T1/2 of the drug and T1/2 of its active metabolites in ascending order) is presented in Table. 2. The advantages, disadvantages and optimal tactics for using anxiolytics, hypnotics and sedatives are presented in table. 3.
In addition to classification by duration of action, the strength of the drug is of important clinical importance, and therefore the concept of the so-called diazepam equivalent [39] (similar to “chlorpromazine equivalent”) has been introduced into clinical practice since 1985 [37, 38]. Diazepam equivalent is a dose of the drug equivalent to 10 mg of diazepam in terms of therapeutic effect [37]. The classification of anxiolytics, hypnotics and sedatives by strength (in descending order) is presented in Table. 4 [37, 38].
Non-benzodiazepine tranquilizers
Currently in Russia, in psychiatric clinical practice, there are three main non-benzodiazepine tranquilizers - hydroxyzine, etifoxine, buspirone, sometimes tofisopam is also conditionally included in this group, although it is a benzodiazepine derivative, but according to its stated properties it is classified as a so-called atypical benzodiazepine. The advantages of these drugs are that they are devoid of the main side effects of benzodiazepine tranquilizers, such as daytime sleepiness (with the exception of hydroxyzine), risks of addiction and withdrawal syndrome, cognitive toxicity, but at the same time they also have a much weaker anxiolytic effect, due to with which they are often used when withdrawing benzodiazepine tranquilizers, if it is impossible to use benzodiazepines (in case of individual intolerance, risks of developing dependence syndrome or withdrawal syndrome), if it is necessary to drive a vehicle while taking therapy (with the exception of hydroxyzine), in elderly patients (since they do not suppress cognitive processes, memory and attention, do not cause an increase in tolerance, withdrawal syndrome, dependence syndrome, do not have a sedative and relaxing effect, suppress fear and anxiety). I would like to note that in addition to the above medications, non-benzodiazepine drugs also include tetramethyltetraazabicyclooctanedione, melatonin, fabomotizol, and valerian rhizome preparations. However, in scientific studies for the indications stated by the manufacturers in the instructions, the effectiveness of these drugs has not been confirmed (either there are low-quality studies on their effectiveness, or there is reliable data on ineffectiveness) [40–45], and given that the last two drugs are widely sold in pharmacy chains Russia and are over-the-counter, they can be conditionally classified as drugs of the so-called “preclinical” stage (most often, patients take them independently before seeking medical help, i.e., use them for self-medication). Drugs such as bromizal, bromides and others are not discussed in the article, since they have very limited use in Russia, and there are no high-quality studies confirming their clinical effectiveness.
Application tactics
Taking into account the officially registered instructions for the use of drugs, there are currently several main established tactics for the use of anxiolytics, hypnotics and sedatives in the clinical practice of psychiatry in Russia.
1. Outpatient tactics: a) treatment of anxiety as part of complex therapy - an anxiolytic is prescribed in short courses (usually up to 2 weeks, maximum 3 weeks, with a break between courses of at least 1 month) in small or medium doses in combination with treatment of concomitant psychiatric or somatic pathologies; b) covering the antidepressant (the so-called “benzodiazepine bridge tactics”) - an anxiolytic is prescribed in a short course (usually up to 2 weeks, maximum 3 weeks, in small or medium doses) for the period of development of the action of the antidepressant in order to quickly relieve anxiety, as well as relieve possible undesirable effects phenomena of the initial stage of antidepressant therapy; c) treatment of sleep disorders - an anxiolytic or hypnotic and sedative drug is prescribed in a short course (usually a maximum of 2 weeks) in small or medium dosages once before bedtime, followed by transition to episodic use against the background of complex therapy of sleep disorders (drug and psychotherapeutic treatment of comorbid psychiatric pathology , drug treatment of somatic pathology); d) treatment of panic attacks (an anxiolytic is prescribed for occasional use in small or medium doses to relieve panic attacks in addition to the main therapy); e) correction of anxiety, sleep disorders, neuroleptic complications, to improve compliance (adherence to therapy) in patients receiving antipsychotic therapy - an anxiolytic is prescribed in small or medium doses, in short courses of up to 1 month, followed by withdrawal during periods of selection of antipsychotic therapy and during periods exacerbations with increasing dosages of antipsychotic drugs. 2. Stationary tactics. Rapid relief of psychomotor agitation, agitation, severe anxiety (an anxiolytic is prescribed more often in injection form in medium or above average doses in a short course of up to 1 week, maximum 2 weeks, in addition to the main therapy, usually antipsychotics or antidepressants until their main effect develops and for its potentiation); mainly used are 2 drugs available for parenteral administration - bromodihydrochlorophenylbenzodiazepine and diazepam. Of all existing anxiolytics, hypnotics and sedatives in Russia (according to the State Register of Medicines) [7], at least 13 names of anxiolytics and at least 10 names of hypnotics and sedatives are registered, not counting drugs that are classified as drugs from other groups (for example, clonazepam). Anxiolytic, hypnotic and sedatives currently registered in Russia, taking into account trade names, are presented in Table. 5 (with the exception of trade names of the form “international nonproprietary name” - INN or “INN-manufacturer”) [7]. In addition to classification by duration (T1/2) of action and strength (diazepam equivalent), important parameters for clinical practice are the price and availability of the drug (legislative regulation of drug prescribing, pharmacy chain policies), but they are largely subject to change (price changes, legislative practice national health care system), the final decision on prescribing a particular drug is made by the attending physician, taking into account the indications, contraindications, clinical profile of the drug, its pharmacodynamics, pharmacokinetics, individual characteristics of the patient and the above parameters. Important aspects of the use of anxiolytics, sedatives and hypnotics are the age at which they are approved for use, the effect on driving and activities requiring increased concentration, as well as use during pregnancy and lactation (according to official instructions for drugs)2 [7 ]. Most of these drugs currently used in Russia (namely: diazepam, chlordiazepoxide, hydrazinocarbonylmethylbromophenyldihydrobenzdiazepine, etifoxine, bromodihydrochlorophenylbenzodiazepine, diazepam + cyclobarbital, nitrazepam, zopiclone, zaleplon, melatonin), are approved for use from 18 years of age, are not recommended for use during driving vehicles and is contraindicated during pregnancy (especially in the first trimester) and lactation. However, for other drugs of these groups, these aspects (according to the instructions for use) [7] are somewhat different; they are presented in table. 6 2.
Conclusion
Despite its “venerable” age (more than half a century from the discovery of the first representatives of the group of benzodiazepine tranquilizers) and the large number of modern antidepressants and other psychotropic drugs that affect anxiety and have an anxiolytic effect that have appeared in clinical practice (including in Russia) in recent decades , benzodiazepine receptor agonists (mostly benzodiazepine tranquilizers), as typical representatives of anxiolytics, hypnotics and sedatives, firmly occupy their niche in psychiatric practice, which can be briefly described as “short-term complex treatment of anxiety and sleep disorders.” Their therapeutic effect, side effects and associated problems of use and ways to overcome them have been well studied in numerous scientific studies, many of them are included in the WHO Model List of Essential Medicines [46] and currently remain widely used drugs in modern psychiatric practice in Russia , and all over the world.
1. Additionally highlighted by researchers in Russia [23, 24]. 2. The data may differ significantly (depending on the manufacturer - trade name of the drug, release form, dosage, according to the instructions for the drug officially registered in Russia at the time of writing), it is necessary to clarify the information in each specific case according to the instructions.
About the author
Maslov Konstantin Andreevich – psychiatrist, State Budgetary Healthcare Institution “OPB named after. K.R. Evgrafova. Email