Pheochromocytoma originates from the cells of the central part of the adrenal gland. It can occur at any age, including in children, but more often it is detected at the age of 20-50.
The adrenal glands produce a number of biologically active substances that are vital for the body. For example, they synthesize the hormones adrenaline and norepinephrine; They are also called catecholamines or “fight or flight” hormones. The fact is that during various stressful situations, these substances are released into the blood, regulating heart rate, metabolism and blood pressure and forcing the body to act when danger arises. Most pheochromocytomas are diagnosed in the central (brain) part of one or both adrenal glands.
Causes of pheochromocytoma
It is still unknown what causes the development of the disease. It was found that the tumor begins its development from chromaffin cells of the adrenal medulla. It is these cells that produce epinephrine (adrenaline) and norepinephrine (norepinephrine).
The risk of getting sick increases if the patient already has:
- multiple endocrine neoplasia type II or MEN II. Men suffer from this rare hereditary disease; tumors develop in the thyroid and parathyroid glands, on the lips, in the tongue, and in the gastrointestinal tract.
- Hippel-Landau disease, when multiple tumors occur in the nervous and endocrine systems, pancreas and kidneys.
- neurofibromatosis type 1: multiple tumors appear in the skin - neurofibromas, pigmented spots appear on the skin, and a tumor of the optic nerve also occurs.
- hereditary paraganglioma/pheochromocytoma syndrome, which occurs due to mutations in genes.
- Carney's triad: paragangliomas, pulmonary chondroma, gastric stromal tumor.
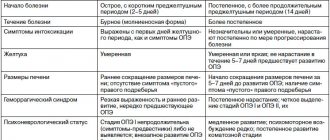
Clinical picture
The main symptom is arterial hypertension (constant, paroxysmal or mixed form). A characteristic feature of the hemodynamic (hypertensive) crisis in pheochromocytoma is its short duration and so-called self-limitation.
Additional symptoms include:
- orthostatic hypotension;
- sweating;
- constant headaches;
- feeling of inner trembling, anxiety;
- general weakness, decreased ability to work.
The classic course of pheochromocytoma is indicated when patients have hypertensive crises with a sudden increase, primarily in systolic blood pressure, which can reach 300 mm Hg. Crises can be provoked by slight physical activity, palpation of the abdomen, sometimes by taking β-blockers, and when pheochromocytoma is localized in the wall of the bladder, by urination; are accompanied by rapid heart rate (up to 180/min), arrhythmias and/or changes in the electrocardiogram (ECG) like acute coronary ischemia (usually not associated with coronary circulation disorders, but due to the direct toxic effect of catecholamines).
Also during an attack, tremors, tinnitus, anxiety or fear, dilated pupils, sweating, chest or abdominal pain, nausea or vomiting are often noted. Vasoconstriction of the extremities under the influence of catecholamines can cause pain and paresthesia, intermittent claudication, Raynaud's syndrome, ischemia, and trophic ulcers. Hyperglycemia and glycosuria, leukocytosis may be detected. The duration of an attack can be from several minutes (usually) to several hours (much less often). The attack usually ends suddenly. With pheochromocytoma, decompensation of previously undetected diabetes mellitus or impaired glucose tolerance is possible. When examining the fundus, spastic angiopathy is revealed. In pheochromocytoma, the severity of changes in the fundus does not correspond to the malignancy of the course of hypertension.
In approximately 10% of cases, pheochromocytoma is a familial disease and is inherited in an autosomal dominant manner. Pheochromocytomas and accompanying tumors of the thyroid gland and nervous tissue are of neuroectodermal origin, as evidenced by the presence of neuron-specific enolase in all these tumors. Apparently, the occurrence of such tumors is due to disturbances in the proliferation and differentiation of neural crest cells.
MEN type IIa. This hereditary syndrome is caused by a defect in one of the loci of chromosome 10. Components of the syndrome: medullary thyroid cancer, hyperplasia or adenoma of the parathyroid glands (clinically manifested as hyperparathyroidism), pheochromocytoma and (less commonly) bilateral adrenal hyperplasia.
MEN type IIb. EC components of the syndrome: pheochromocytoma, medullary thyroid cancer, mucosal neuromas, thickening of the corneal nerves, gastrointestinal ganglioneuromas; often Marfan-like appearance.
Other associated syndromes. 5% of patients with pheochromocytoma have neurofibromatosis (Recklinghausen's disease). A combination of pheochromocytoma, neurofibromatosis and somatostatin-containing carcinoid tumor of the duodenum has been described. A combination of pheochromocytoma with Hippel-Lindau disease (retinocerebellar hemangioblastomatosis) and acromegaly was observed.
Classification
The formation of the adrenal glands is distinguished, i.e. pheochromocytoma itself. In addition to the adrenal glands, a small number of chromaffin cells in the form of small clusters can be found in the heart, head, neck, bladder, and along the spine. Tumors in these cells are called paragangliomas. They have a similar effect on the body as pheochromocytomas, as the same hormones are released.
Classification of pheochromocytoma according to ICD-10
The disease is placed in section D35.0 - “Benign neoplasm of other and unspecified endocrine glands.”
Pathogenesis
The clinical symptoms of pheochromocytoma are associated with the effect on the body of catecholamines excessively produced by the tumor. In addition to catecholamines (norepinephrine, adrenaline, dopamine), pheochromocytoma can secrete ACTH, calcitonin, serotonin, somatostatin, vasoactive intestinal polypeptide, the strongest vasoconstrictor - neuropeptide Y and other active substances that cause diverse effects.
Pheochromocytoma is an encapsulated tumor with good vascularization, about 5 cm in size and an average weight of up to 70 g. Pheochromocytomas are found in both large and smaller sizes; Moreover, the degree of hormonal activity does not depend on the size of the tumor.
Symptoms and signs of adrenal pheochromocytoma
The main signs that will help suspect the disease are:
- elevated blood pressure levels
- increased, rapid, or irregular heartbeat
- excessive sweating for no reason
- severe headache
- pale face
- shortness of breath.
More rare symptoms may include:
- anxiety, depressing expectation of trouble
- abdominal pain, constipation
- weight loss
Catecholamine crises
The disease is characterized by the sudden onset of symptoms. These manifestations are called catecholamine crises. Their duration ranges from 15 to 20 minutes. The attack can occur several times a day or less often; in severe cases, there can be up to 25 crises per day. The attack usually ends as suddenly as it begins. During the period between crises, blood pressure may drop to normal or remain high.
Possible triggering factors for crises:
- physical exercise
- stress, nervous tension
- change in body position
- intestinal peristalsis
- contractions or childbirth.
Eating foods rich in tyramine can also trigger a crisis. This biogenic amine is abundant in fermented foods, for example:
- in mature cheeses
- in dried and smoked meat
- in avocados, bananas, beans
- in marinated fish
- in sauerkraut
- in some beers.
The release of hormones can be triggered by drugs (amphetamine, cocaine) and some medications:
- vasoconstrictors (decongestants)
- monoamine oxidase inhibitors
- dopamine receptor blockers
- serotonin reuptake inhibitors
- muscle relaxants
- glucocorticosteroids.
Diagnosis of pheochromocytoma
The endocrinologist begins the diagnosis with questioning, finding out hereditary predisposition, and studying the history of the disease. Then he measures blood pressure and calculates heart rate.
Analyzes
Next, laboratory tests are usually prescribed to study the levels of adrenaline, norepinephrine and their metabolites:
- determination of metanephrine and normetanephrine in urine collected per day
- determination of the level of free metanephrine in blood plasma.
Measuring urinary catecholamine levels and vanillylmandelic acid levels is not currently used because false-positive results are common.
At elevated levels of biologically active substances, tests use imaging methods that will help identify the tumor:
- computed tomography (CT) of the abdominal organs and adrenal glands. The method allows you to detect formations larger than 5 mm.
- scintigraphy, which is used if there is a suspicion of a tumor outside the adrenal glands. When conducting research, it is necessary to take into account the possibility of asymmetric accumulation of the isotope in normal adrenal glands.
- positron emission tomography (PET). This method is more sensitive than scintigraphy in detecting metastatic lesions.
If several family members have the disease or developed before the age of 40, genetic testing is performed. For patients over 50 years of age, genetic testing is rarely prescribed.
WHO (2004) defines pheochromocytoma as a tumor of chromaffin cells of the adrenal medulla that produces catecholamines - adrenal paraganglioma. Extra-adrenal paraganglial tumors are classified as extra-adrenal paragangliomas. Cells of the diffuse sympathetic nervous system, sympathetic paravertebral ganglia and adrenal medulla have a single origin from neuroectodermal cells, thus pheochromocytoma is neuroendocrine in nature.
Epidemiology
According to the results of interclinical autopsy data, per 100 thousand studies, pheochromocytoma is detected in 20-150 cases (on average 50) [1, 2]. According to summary literature data, in 30-70% of cases the diagnosis of pheochromocytoma is established posthumously [3]. The population incidence of the disease was considered low for a long time; data was reported on one observation per 200 thousand population [4], the incidence was one observation per 2 million people per year [5]. It is believed that in 1% of cases among patients with arterial hypertension (AH) aged 30 to 50 years, the cause of high blood pressure (BP) is a tumor of chromaffin tissue (AH is detected in 25% of the population).
Small groups of chromaffin cells can be located in almost any area of the body, head and neck. In 90% of cases, pheochromocytomas arise in the adrenal medulla, in 8% - in the para-aortic lumbar paraganglia. Much less often, tumors are localized outside the adrenal glands: in less than 2% of cases - in the abdominal and chest cavity and in less than 0.1% of cases - in the neck. One of the most common extra-adrenal localizations of chromaffin (50-80%) is a Zuckerkandl tumor, arising from the para-aortic sympathetic ganglion located in the area where the inferior mesenteric artery originates from the aorta. Extra-adrenal chromaffin tumors can also be detected at the base of the brain, in the chest (including the heart and pericardium), in the scrotum, and chromaffins of the inner ear have been described [6].
In adult patients, in approximately 80% of cases there is a unilateral solitary tumor, in 10% there is a bilateral process. In children, bilateral tumors account for 25% of cases and another 25% for extra-adrenal tumors. Multiple tumors (both adrenal and extra-adrenal) are found more often in children than in adults (in 35 and 8% of cases, respectively). In hereditary forms, more than 70% of patients have bilateral tumors [7].
Pheochromocytoma can occur at any age, but most often occurs between 20 and 40 years. The incidence of pheochromocytomas in adult men and women is the same, while among sick children, 60% are boys [1].
Less than 10% of pheochromocytomas are malignant. As a rule, they are localized outside the adrenal glands.
Although pheochromocytomas can reach large sizes (over 3 kg), most have a mass of less than 100 g and a diameter of less than 10 cm. These tumors are highly vascularized and receive blood from any of the three arteries supplying the adrenal gland [7].
Genetically determined pheochromocytomas
According to prospective and retrospective genetic studies performed on large samples of patients with chromaffin tumors, almost 30% of patients have genetic defects that are transmitted in an autosomal dominant manner. It is these mutations that are responsible for the phenotypic implementation of pheochromocytomas [8, 9].
In 32-38% of cases, there is a mutation in the genes responsible for the synthesis of succinate dehydrogenase, D- or B-subunit (SDHD or SDHB). The disease is manifested by the appearance of functioning paragangliomas, usually multiple, with a high malignant potential. The phenotypic penetrance of pheochromocytoma in such patients is 15-40%. Bilateral damage to the adrenal glands is observed in 40% of cases, extra-adrenal damage - in 70%. With this genetic defect, paragangliomas are characterized predominantly by a norepinephrine type of secretion [10].
In 30-35% of patients with familial forms of the disease, pheochromocytoma is detected as part of von Hippel-Lindau disease - a mutation occurs in the VHL gene of the 3rd chromosome. Possible phenotypic manifestations: retinal hemangiomatosis, hemangio- and neuroblastomas of the central nervous system, cysts (polycystic disease) or kidney cancer, small cystic transformation and pancreatic cancer.
Extra-adrenal lesions occur in 30% of cases. The frequency of bilateral lesions reaches 80%. Multicentric lesions in at least one adrenal gland are observed in almost 90% of cases. Pheochromocytomas manifest in the first or second decade of life. With a mutation in the VHL gene, the predominant type of tumor secretion is norepinephrine. In the case of functioning paraganglioma syndrome and von Hippel-Lindau disease, genetic diagnosis is extremely important, since the phenotypic penetrance of pheochromocytoma in these diseases is low and family history may not be traced [11-13].
In 20-25% of patients with hereditary lesions, a combination of pheochromocytoma with medullary thyroid cancer (MTC) is detected as part of the MEN type 2 syndromes. In this disease, a mutation occurs in the RET oncogene of chromosome 10 (exons 10-16), which is responsible for the synthesis of tyrosine kinase. The disease manifests itself in the second or third decade of life. There is a high frequency of bilateral lesions - up to 80%. There are no extra-adrenal lesions. A multicentric benign lesion of the adrenal gland is noted. In MEN syndrome, the predominant type of tumor secretion is adrenaline. Other clinical manifestations of the syndromes are possible: hyperparathyroidism, ganglioneuromatosis of the mucous membranes of the gastrointestinal tract, Marfan-like appearance. In MEN type 2 syndrome, the phenotypic penetrance of pheochromocytoma is high (80%), so a family history of the disease is easily traced. Laboratory genetic diagnosis is of greater importance in determining tactics for medullary cancer in this form of the disease [6].
In 8-14% of cases of genetically determined pheochromocytomas, Recklinghausen's disease (neurofibromatosis type I) is detected. The NF1 gene mutation occurs in the 17q-11 region. Neurofibromatosis type I syndrome is diagnosed by typical skin manifestations that have high (100%) phenotypic penetrance; There is no need to verify the genetic diagnosis in the presence of pheochromocytoma in such patients. The phenotypic penetrance of pheochromocytoma in such patients reaches 20-35%, the frequency of extra-adrenal lesions is up to 50%.
Pathogenesis and pathophysiology
Hemodynamic fluctuations in pheochromocytoma are not always a direct consequence of increased production of catecholamines directly by the tumor. One of the factors influencing blood pressure fluctuations in pheochromocytoma is the presence of a significant catecholamine depot in the endings of the sympathetic nerves. Norepinephrine released by these endings acts on the receptors of efferent cells at the synapse. Any stimulation of the sympathetic system may stimulate a crisis caused by the neurogenic effects of norepinephrine released from the synaptic stores rather than their chromaffin tumor. In this case, a significant increase in catecholamine levels is not observed.
With increased secretion of catecholamines, a positive chronotropic effect is observed due to the effect on β1 receptors of the heart. These receptors are sensitive to norepinephrine; adrenaline has virtually no effect on them. The chronotropic effect may be influenced by a reflex slowing of the rhythm as a response to the higher amplitude of the increase in blood pressure when exposed to norepinephrine.
The effect of adrenaline is directed primarily at α1-receptors of blood vessels in the skin, mucous membranes, and internal organs. With the secretion of norepinephrine, its pronounced vasoconstrictor effect on the α1 receptors of the vessels of the striated muscles is observed to a greater extent. In terms of quantity, they have a greater share in the formation of peripheral vascular resistance compared to the receptors of the vessels of the skin, mucous membranes and internal organs.
An important pathogenetic link that explains the less pronounced vasoconstrictor reaction in response to the effects of adrenaline is the stimulation by adrenaline of β2-adrenergic receptors, which give a vasodilating effect.
In the kidneys, when exposed to β-receptors of the juxtaglomerular apparatus, renin is released, and, as a consequence, the renin-angiotensin-aldosterone system is activated. This mechanism causes increased manifestations of arterial hypertension and partially explains the persistent form of increased blood pressure in patients with pheochromocytomas. Sometimes the cause of diagnostic errors in small pheochromocytomas is an increase in aldosterone levels. When β2 receptors are stimulated, bronchi dilatation is also observed; this effect is of less clinical significance. A manifestation of the β2-receptor effect is also relaxation of the uterine muscles.
In the intestine, there is a certain synergism of the effects of catecholamines on α- and β-adrenergic receptors. Stimulation of receptors of all types causes suppression of motor function and increases the tone of the sphincters of the gastrointestinal tract. These effects lead to chronic constipation in patients with pheochromocytoma, which causes intoxication and aggravates hypovolemic manifestations. In combination with hypokalemia, which increases paresis of the intestinal muscles, constipation is a serious clinical problem.
Unlike the intestinal adrenergic receptors, the pancreatic receptor apparatus responds with a multidirectional effect on catecholamine stimulation. Stimulation of β-adrenergic receptors in the pancreas increases the release of insulin and glucagon, and increases glycogenolysis in the liver. At the same time, stimulation of α-adrenergic receptors in the pancreas neutralizes the effect of stimulation of β-receptors.
Increased sweating, especially pronounced during an attack, is associated with stimulation of α-receptors of the sweat glands of the skin. Stimulation of β3 receptors of lipocytes promotes lipolysis, which leads to a decrease in the subcutaneous fat layer.
Repeated attempts to create models of the clinical course of pheochromocytoma, depending on the predominant type of hormonal secretion, have not had significant success. This is due to the following reasons:
— variability in the development of the receptor apparatus for catecholamines in different organs;
— excessive deposition of norepinephrine due to the mechanism of reverse neuronal uptake in the presynaptic endings of the sympathetic nervous system;
- a disorder of receptor sensitivity against the background of long-standing hypercatecholaminemia.
— violation of the general systemic control of hemodynamics in conditions of relative hypovolemia occurring in patients with pheochromocytoma.
Hypovolemia in pheochromocytoma is one of the leading syndromes that determine the severity of the patient's condition. Having a “masking” effect on the results of measuring peripheral blood pressure, this often leads to diagnostic errors and incorrect decisions regarding the treatment of the patient. Hypovolemia syndrome is largely responsible for microcirculation disorders in vital organs.
Among the reasons influencing the decrease in the volume of circulating fluid in patients with pheochromocytomas, centralization of blood circulation is noted. This occurs due to increased peripheral vascular resistance and a shunting effect. A significant component in the formation of hypovolemia is the release of fluid from the vascular bed into the “third space” as a result of changes in the permeability of the vascular wall due to persistent vasoconstriction and the formation of fibromuscular dysplasia during prolonged vascular spasm. Important factors influencing the occurrence of hypovolemia are increased sweating and chronic constipation.
In the pathogenesis of changes in the cardiovascular system, the occurrence of morphological changes in the myocardium against the background of hypercatecholaminemia plays an important role. One of the most common misconceptions that leads to late detection of pheochromocytoma is overdiagnosis of myocardial ischemia. It should be noted that both electrocardiographic and laboratory signs of cardiomyocyte destruction are not specific.
Unfortunately, in some patients it is impossible to distinguish changes resulting from the direct effect of catecholamines on the myocardium from “coronary problems” that preceded the disease. However, the occurrence of arrhythmias, myocardial necrosis, laboratory cytolytic syndrome and electro- and echocardiographic changes in most cases are not associated with changes in coronary circulation.
The main cause of cardiotoxic changes in hypercatecholaminemia is intracellular disruption of the action of enzymes responsible for the phosphorylation process. This leads to changes in intercellular and intracellular ion exchange and the oxidative intracellular cycle (the so-called toxic catecholamine myocardial dystrophy). High afterload against the background of non-coronary myocardial dystrophy or myocardial necrosis can lead to acute left ventricular failure (cardiac asthma, pulmonary edema). With a long history of pheochromocytoma and progressive cardiosclerosis against the background of myocardial hypertrophy, concentric and then dilated cardiomyopathy occurs, inevitably leading to chronic heart failure. Paroxysms of cardiac arrhythmias are a high risk factor for sudden death in these patients.
Against the background of increased episodes of catecholamine release into the bloodstream and an increase in the intensity of secretion, a state of “uncontrolled hemodynamics” may arise - frequent and chaotic alternation of episodes of high and low blood pressure, which is practically not corrected with medication or gives a paradoxical response to the administration of drugs. The main sign of the state of “uncontrolled hemodynamics” is a tendency to progressive hypotension. The main threat in the state of “uncontrolled hemodynamics” is the development of catecholamine shock.
Catecholamine shock is fundamentally different from the state of “uncontrolled hemodynamics” in that during its development, persistent uncontrollable hypotension is noted against the background of cardiac arrhythmias, which lead to ineffective cardiac output. This phenomenon is associated, on the one hand, with a change in the sensitivity of adrenergic receptors against the background of constant intense stimulation, depletion of cells of the cardiac conduction system, and on the other, with a change in the mechanisms of inactivation of catecholamines.
In the state of “uncontrolled hemodynamics” and catecholamine shock, as an extreme manifestation of this condition, a paradoxical situation arises in which the central vessels sharply narrow (systolic blood pressure in the aorta is 300 mm Hg and above), and vascular hypotension occurs in the periphery. Treatment measures carried out under these conditions do not contribute either to the improvement of the patient’s condition or to the correct diagnosis.
Of the clinically significant pathophysiological effects in pheochromocytoma, it is necessary to pay attention to the occurrence of “secondary” diabetes mellitus or impaired glucose tolerance, which is due to the acceleration of glycogenolysis in the liver, a decrease in insulin production due to stimulation of α-adrenergic receptors of the pancreas. Some authors believe that with pheochromocytoma, decompensation of the clinical manifestations of previously undiagnosed diabetes mellitus or impaired glucose tolerance occurs.
Clinical picture
The most common and main clinical manifestation of pheochromocytoma is a hemodynamic crisis, which is characterized by a sudden increase in systolic blood pressure to 200-250 and even 300 mm Hg. and more, is accompanied by the appearance of unaccountable fear, a feeling of internal trembling. There is pallor of the skin, or, on the contrary, redness of the face. A characteristic symptom of peripheral microcirculation disorders during an attack is the appearance of a “marble” skin pattern, which is more pronounced during frequent crises. A paroxysm of increased blood pressure was almost always accompanied by profuse sweating. Unlike other conditions accompanied by sweating, with pheochromocytoma, patients do not characterize sweating during a crisis as “cold” or “sticky” sweat. A common symptom during an attack is decreased visual acuity and double vision. A hemodynamic crisis may be accompanied by nausea, vomiting, and severe abdominal pain. During an attack, dilated pupils, headaches, pain in the lower back and epigastric region are noted with varying frequency.
In some patients, the main symptom of a crisis increase in blood pressure is pain in the heart (compressive pain behind the sternum, possibly radiating to the shoulder, arm, between the shoulder blades). One of the most constant manifestations is a heartbeat of up to 140-180 beats/min, much less often - normosystole or bradycardia. In some patients, an increase in blood pressure is accompanied by rhythm disturbances (the occurrence of frequent atrial and/or ventricular extrasystole, paroxysm of sinus tachycardia, paroxysm of atrial fibrillation). A terrible symptom of pheochromocytoma is shortness of breath during a crisis. This may indicate both excitation of the respiratory center during hypercatecholaminemia and the development of acute left ventricular failure, which manifests itself to varying degrees, from cardiac asthma to pulmonary edema.
A characteristic manifestation of a hypertensive crisis in pheochromocytoma is its short duration and so-called self-limitation. A single attack of increased blood pressure usually lasts from 5 to 15-20 minutes. Often, medical services at the prehospital stage, due to objective reasons, do not even have time to register the true degree of increase in blood pressure. During a series of attacks, patients note that fluctuations in blood pressure do not depend on the drugs administered. In the post-attack period, most patients experience normalization of skin color, disappearance or reduction of sweating, pain, feelings of internal trembling, and fear. Some patients experience an imperative urge to urinate and excessive urination (urine is usually light-colored).
Much less common than other symptoms in pheochromocytoma is the provocation of an attack by any factor: physical activity, palpation of the tumor, change of posture, heavy food, prolonged fasting, anesthesia, emotional trauma, taking β-blockers, defecation, and in rare cases (when the tumor is localized in the urinary tract). bladder) by urination. The frequency of development of the symptom ranges from 5 to 15%, but in other forms of arterial hypertension this symptom practically does not occur.
A permanent form of increased blood pressure occurs with pheochromocytoma in 10-50% of cases, paroxysmal - in 42-87%, a mixed variant of the clinical course - in 1/3.
One of the most persistent symptoms in the interictal period is dizziness, which increases with orthostasis (almost 65%). Postural hypotension is a nonspecific symptom, which is more pronounced the higher the blood pressure amplitude. This sign is extremely important for assessing the severity of the patient’s condition, as it indicates hypovolemia. An orthostatic test can identify hypovolemic disorders with greater accuracy than the patient’s active complaints of dizziness during orthostasis.
Diabetes mellitus with pheochromocytoma, as a rule, does not have a clinically persistent course.
When examining the fundus, spastic angiopathy is revealed. In pheochromocytoma, the severity of changes in the fundus does not correspond to the malignancy of the course of hypertension. Observations of decreased vision up to its complete loss are described. It should be noted that these observations are described mainly in children and are more often observed in acute cerebrovascular accidents.
The variety of symptoms in pheochromocytoma indicates dysfunction of most organs and systems. However, a component of hyperfunction of the sympathetic-adrenal system is an integral part of such common diseases as essential hypertension and neurocirculatory dystonia. Therefore, the characteristic symptoms of pheochromocytoma - high blood pressure levels, tachycardia, sweating, weakness, headache, internal trembling, etc., detected either individually or in combination, are not specific. In this regard, their use for the primary diagnosis of pheochromocytoma seems doubtful. However, as with any other serious disease, timely diagnosis largely determines the prognosis and quality of life after surgery for patients in this category.
Methylated catecholamine derivatives
An increased level of methylated catecholamine derivatives (MCDs) in biological media has a pathogenetic connection with chromaffin tumor [14, 15]. Under physiological conditions (in the absence of pheochromocytoma), MPCs are formed as a result of inactivation (methylation) of norepinephrine in the synaptic space by the enzyme catecholamine-O-methyltransferase. This enzyme is detected in high concentrations in any chromaffin tumor. Methylation of catecholamines, without affecting the synthesis of adrenaline and norepinephrine, changes the nature of tumor excretion in favor of inactive meta- and normetanephrine. This process is an adaptive mechanism of intratumoral inactivation of adrenaline and norepinephrine. It is MPC that serves as the pathophysiological basis for the lack of clinical activity of pheochromocytomas [16].
The MIC level is an integrative indicator of tumor activity over 24 hours. The method for determining free MIC in plasma has high sensitivity and specificity, reaching 95-100%. The study of urine MIC is practically not inferior to the sensitivity (93%) and specificity (75%) of determining the level of free plasma MIC [17].
The method allows you to obtain additional information useful for the clinician, since MPC excretion reflects the predominant type of catecholamine secretion by the tumor. Thus, if the synthesis of adrenaline predominates in the tumor, then there is an increase in the daily excretion of metanephrine; if tumor synthesis of norepinephrine predominates, then the excretion of normetanephrine increases; with a mixed type of tumor production, an increase in both BMD indicators is possible. In most observations, for the intraoperative management of patients, information about the predominant type of secretion is important and influences anesthetic tactics. Thus, the norepinephrine type of secretion is characterized by a more pronounced effect on blood pressure, tachycardia amplitude, and arrhythmogenicity; the predominance of adrenaline production is more dangerous from the point of view of bradycardia, while the vasopressor effect is less aggressive [18].
The use of this method allows us to solve an even more pressing problem from an epidemiological point of view. A normal level of MIC in biological fluids makes it possible with a high degree of probability to deny the symptomatic genesis of arterial hypertension associated with overproduction of catecholamines by a chromaffin tumor. The method for determining BMD can be used once in patients with arterial hypertension to exclude pheochromocytoma.
In the context of the possibility of determining the level of MPC in plasma and urine, a review of the diagnostic capabilities of determining adrenaline, norepinephrine and vanillylmandelic acid in daily urine and pharmacological tests has more historical than clinical value [6, 11].
Topical diagnostics
Topical diagnosis of pheochromocytoma or paraganglioma can be started only if clinically necessary and there is reasonable suspicion of a chromaffin tumor. If such assumptions are based on identifying an increased level of BMD, then the results should significantly exceed normal values. In patients with a hereditary predisposition or a history of pheochromocytoma, even questionable results of hormonal studies are an indication for topical diagnosis.
Computed tomography (CT) and magnetic resonance imaging (MRI) are equal methods of primary diagnosis in all patients, except children, pregnant women and people with allergies to contrast agents. The primary stage of topical diagnosis includes CT or MRI of the abdominal cavity and retroperitoneal space. If a tumor is not found, then examination of the pelvis, chest and neck is necessary. It should be remembered that with this tactic, metastatic lesions of long bones may be missed.
Despite the high sensitivity of CT and MRI, the anatomical approach to topical diagnosis is nonspecific. In some observations, identification of the chromaffin nature of the tumor is extremely important. Currently, the greatest specificity of functional topical diagnostics is achieved by using scintigraphy with metaiodobenzylguanidine labeled with the 123I isotope (MYBG-123I).
You can refrain from performing scintigraphy with MYBG-123I in cases of identified adrenal tumors with a diameter of less than 5 cm, in which there is a significant increase in the level of metanephrine in plasma or urine. This is explained by the fact that small tumors rarely metastasize, and tumors with predominant secretion of adrenaline are in most cases located in the adrenal gland.
Despite the advantages of scintigraphy with MYBG-123I, its sensitivity leaves much to be desired, especially in the diagnosis of metastatic lesions. In this regard, other functional mapping methods are used. Positron emission tomography (PET) scans use the promising new specific radionuclides 6-18F-fluorodopamine, 18F-dihydroxyphenylalanine (DOPA), 11C-hydroxyephedrine, or 11C-epinephrine to diagnose pheochromocytoma. Recent studies have demonstrated the superiority of these methods compared to scintigraphy with MYBG-123I and MYBG-131I. Cumulative diagnostic methods such as octreoscan and PET with 18F-fluorodeoxyglucose are not recommended as the first stage of topical diagnosis. These examination options can be used in patients with a negative result of scintigraphy with MYBG-123I, with rapidly growing tumors with high metabolic activity or with somatostatin receptors [19, 20].
The algorithm for examining patients with pheochromocytoma is presented in the figure.
Figure 1. Algorithm for examining patients with pheochromocytoma.
Issues of preoperative preparation of patients
To carry out stabilizing therapy in patients with pheochromocytoma, it is necessary first of all to assess the severity of the patient’s condition and determine priorities and criteria for the adequacy of the upcoming treatment. It should be noted that indicators such as tumor size, duration of arterial hypertension, amplitude and frequency of blood pressure increases cannot be a reliable criterion for assessing the severity of a patient’s condition with pheochromocytoma. In the foreground is the problem of the functional state of target organs suffering from catecholamine intoxication, such as the heart, kidneys, and brain, because these factors have a greater influence on the intra- and postoperative prognosis. The main goal of preoperative preparation is to increase the functional reserves of target organs in anticipation of the upcoming operation and inevitable hemodynamic crises.
Both α- and β-adrenergic blockers are used to treat patients with pheochromocytoma, and the duration and selectivity of action of the drugs are in the widest range.
At the present stage, doxazosin, a selective long-acting α1-adrenergic blocker for oral use that affects the entire spectrum of α1-adrenergic receptors of resistive vessels, can be recommended as the most effective drug for preoperative adrenergic blockade. The half-life of the drug is less than 22 hours. The effective dose is achieved after 2-3 hours. It is prescribed in a dose of 1 to 16 mg/day for 1-2 doses from an initial dose of 1-2 mg/day. In the absence of hypovolemia, the drug does not cause hypotension in the interictal period. Additional advantages of the drug are its positive effect on blood lipid composition (doxazosin reduces the concentration of low-density lipoproteins), a decrease in platelet aggregation ability, and a decrease in the size of the prostate gland during benign hyperplasia.
Unlike drugs from the group of α-adrenergic blockers with a symptomatic mechanism of action, the use of α-methylparatyrosine (metyrosine, demser) is based on the pathogenetic aspects of pheochromocytoma. The drug blocks tyrosine kinase, which regulates the synthesis of catecholamines. It is prescribed at an initial dose of 250 mg 4 times a day, followed by a possible dose increase to 4 g/day. The dose is adjusted according to the hypotensive effect. It is necessary to use the drug for at least a week before surgery. Among the side effects, it should be noted the possibility of prolonged intra- and postoperative hypotension, as well as a different range of psychosthenic manifestations, and therefore the use of the drug as the main means of preoperative preparation is limited. α-Methylparatyrosine is considered the drug of choice for the treatment of metastatic pheochromocytoma. Unfortunately, the drug is not registered in Russia.
In combination with the use of antihypertensive drugs, one of the main stages of preoperative preparation is to achieve a β-blocking effect in the presence of tachycardia or cardiac arrhythmias. With the existing abundance of drugs in this group, preference is given to cardioselective drugs due to the undesirable effects of blocking β2-adrenergic receptors - hypokalemia and paradoxical arterial hypertension. Prescription of β-blockers is possible after achieving an α-blocking effect. If this condition is not met, a paradoxical worsening of the course of arterial hypertension cannot be ruled out, which is associated with the leveling of the β2-dilating effect of adrenaline.
During planned surgery, long-acting α-blockers and drugs that affect the synthesis of catecholamines should be discontinued the day before.
In connection with the development of endoscopic surgery in leading specialized clinics, endoscopic adrenalectomy has become the method of choice in the treatment of pheochromocytomas [21].
Malignant pheochromocytomas
To ensure optimal information content, the conclusion of a morphological study must contain standard elements. According to WHO criteria (2004), the malignant structure of a tumor from chromaffin tissue is determined by the presence of metastases, and not by local invasion. Even extensive invasion is a vague indicator of possible metastasis, while encapsulated tumors do not exclude the appearance of distant metastases. Thus, reports on the morphological types of pheochromocytomas and paragangliomas distinguish two types of aggressive behavior of tumors, which are caused by different biological characteristics and necessitate different treatment approaches. The first type is characterized by the detection of metastases, the familial form of the disease, detection of the primary tumor at the age of younger than 30 years, multicentric or bilateral lesions. The second type includes the detection of nuclear and cellular polymorphism, atypia, the presence of vascular invasion, and invasion into the tumor capsule [22].
Currently, there is no consensus on a formal grading scale for malignancy, however, there are accepted criteria for malignancy in individual pathology associations. Typically, the scale includes basic and additional criteria. The high malignant potential of pheochromocytoma may include the presence of metastases, extra-adrenal lesions, detection of the tumor at the age of under 15 years, belonging to such familial syndromes as paraganglioma syndrome, von Hippel-Lindau disease, neurofibromatosis-1. The low malignant potential of pheochromocytoma includes single tumors of the adrenal glands, belonging to the MEN type 2 syndrome, and late manifestation of the tumor [21].
The frequency of detection of metastatic lesions in pheochromocytoma (depending on the genetic defect and tumor location) ranges from 3 to 36%. The patient's life expectancy depends on the location of the metastatic process. A trend towards short-term life expectancy (less than 5 years) is observed in patients with metastases in the liver and lungs, long-term is more often observed with metastatic bone lesions; 5-year survival rate is 34-60%. An unfavorable prognosis determines the need to identify a group of patients with existing or probable metastases. Currently, when a primary tumor is identified, there is no reliable marker of malignancy other than the SDHB mutation.
There are several options for managing patients with metastatic pheochromocytoma, but none of the methods leads to complete cure. Reducing tumor size alleviates clinical manifestations, but its effect on survival has not been proven. Surgical debulking may facilitate subsequent radiotherapy and/or chemotherapy. External beam radiation therapy and radiofrequency ablation are alternative treatments for bone metastases. Chemotherapy with a combination of cyclophosphamide + incristin + dacarbazine can give tumor regression and clinical improvement in 50% of patients, but the treatment result, unfortunately, is short-term. The only effective method that serves as an addition to the surgical treatment of malignant pheochromocytomas is therapy with MYBG-131I [21, 23].
Treatment of pheochromocytoma
In rare cases, taking medications can help control blood pressure. The main method of treatment is removal of the tumor.
Surgical treatment of pheochromocytoma
Adrenalectomy surgery is performed either laparoscopically, with the insertion of miniature surgical instruments through small incisions in the abdomen, or through open access to the tumor, when an incision is made in the skin of the abdomen. If the tumor is large (more than 8 cm), the open method is preferable, since during removal it is important not to damage the tumor capsule. Both types of operations are performed under general anesthesia.
If malignancy of pheochromocytoma is detected, the treatment options are as follows:
- surgical removal of the tumor
- radiation therapy
- chemotherapy
- tumor ablation using radio wave method or cryotherapy
- embolization therapy by blocking the artery supplying the tumor
- targeted therapy by blocking specific enzymes, proteins or molecules that affect tumor growth.
Medicines prescribed before surgery
To prepare for surgery, 7-14 days before the operation, the following is prescribed:
- alpha-blockers. These drugs reduce the effect of excess norepinephrine on the body and stabilize blood pressure by relaxing the vascular muscles. Doxazosin, prazosin, and phenoxybenzamine are usually used.
- beta blockers, which also lower blood pressure and heart rate by blocking the action of adrenaline. For example, atenolol, metoprolol and propranolol are used.
- calcium channel blockers, for example, diltiazem, amlodipine, nifidepine. Since diltiazem gently lowers blood pressure and has a relatively short duration of action, it is used for minor increases in blood pressure.
Often calcium channel blockers are added to alpha and beta blockers.
Emergency care for a sharp increase in blood pressure
If a patient with pheochromocytoma has a sharp increase in blood pressure, then an urgent need to call a doctor and, under his supervision, reduce the pressure. The following are used as emergency medications:
- phentolamine 5 to 20 mg intravenously
- tropafen 1%, 1-2 ml intravenously, very slowly
- sodium nitroprusside starting at 0.25 mcg per kilogram of body weight per minute IV.
- labetalol 100 mg orally. It is possible to administer intravenously at a dose of 20 mg, i.e. A 1% solution is administered in an amount of 2 ml.
The use of methyldopa, minoxidil, pentamine, and benzohexonium is undesirable.
Complications of pheochromocytoma
Constant production of hormones increases blood pressure and can damage the heart, kidneys, and brain. Life-threatening conditions may occur, such as:
- arrhythmia
- myocardial infarction
- stroke
- renal failure
- acute respiratory distress syndrome.
Catecholamine shock
This complication is due to the fact that catecholamines are not inactivated and continue to act on the blood vessels. In this case, the change in pressure becomes unpredictable, episodes of increased pressure are chaotically replaced by hypotension. Alpha-blockers are used for treatment; in severe cases, hospitalization in the intensive care unit is necessary.
Malignant pheochromocytoma
Rarely, malignancy may occur, i.e. malignancy of education. This condition is called malignant pheochromocytoma. The diagnosis is confirmed by a biopsy, detection of metastases in the bones or other organs.