Norepinephrinum
General recommendations
Only administered intravenously!
The individual dose of the drug is set by the doctor depending on the clinical condition of the patient.
Norepinephrine should be administered through central venous access devices to reduce the risk of extravasation and subsequent tissue necrosis (see section "Special Instructions").
Before starting or during therapy, correction of hypovolemia, hypoxia, acidosis, and hypercapnia is necessary.
Administration of the drug
The recommended initial dose and rate of administration of the drug is from 0.1 to 0.3 mcg/kg/min. The infusion rate is progressively increased by titration in steps of 0.05-0.1 mcg/kg/min according to the observed pressor effect until the desired normotension is achieved.
There are individual differences in the dose required to achieve and maintain normotension. The goal is to achieve the lower limit of normal systolic pressure (100-120 mm Hg) or achieve a sufficient level of the average value (above 65-80 mm Hg, depending on the patient’s condition). The individual dose, due to the high variability of the clinical response when administering the drug, is set depending on the patient's condition.
Norepinephrine should be used simultaneously with adequate replenishment of circulating blood volume.
It is necessary to be careful about injecting the drug solution under the skin and into muscles due to the risk of developing necrosis.
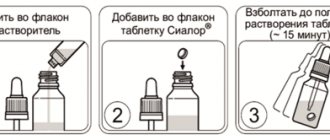
Concentrate dilution
Before use, the concentrate should be diluted in a 5% dextrose solution.
Do not administer undiluted! Do not mix with other drugs!
For administration using a syringe infusion pump, add 48 ml of a 5% dextrose solution to 2 ml of concentrate for preparing a solution for intravenous administration of the drug Norepinephrine, 2 mg/ml.
For administration via a dropper, add 480 ml of a 5% dextrose solution to 20 ml of concentrate for preparing a solution for intravenous administration of the drug Norepinephrine, 2 mg/ml.
With both dilution options, the final concentration of the resulting solution for intravenous administration is 80 μg/ml norepinephrine hydrogen tartrate, which corresponds to 40 μg/ml norepinephrine base.
After diluting the concentrate, the resulting solution must be used within the next 12 hours.
Volume of fluid administered: the dilution level depends on the patient's condition. If the administration of a large volume of liquid is required, the drug should be diluted with a large amount of dextrose and, thus, a drug with a lower concentration should be used for administration. If it is undesirable to introduce a larger volume of liquid, the concentrate is diluted with a smaller volume of glucose dextrose, obtaining a more concentrated solution.
To determine the infusion rate of a drug solution with a concentration of 80 mcg/ml and the corresponding amount of norepinephrine hydrotartrate, you can use the data from the table:
Table. Calculation of the infusion rate (ml/h) of a solution of the drug Norepinephrine with a concentration of 80 mcg/ml*
| Patient's body weight (kg) | Norepinephrine hydrotartrate dose (mcg/kg/min) | Amount of norepinephrine hydrogen tartrate (mg/h) | Infusion rate (ml/h) |
| 50 | 0,05 | 0,15 | 1,875 |
| 0,1 | 0,3 | 3,75 | |
| 0,2 | 0,6 | 7,5 | |
| 0,3 | 0,9 | 11,25 | |
| 0,5 | 1,5 | 18,75 | |
| 1 | 3 | 37,5 | |
| 2 | 6 | 75 | |
| 60 | 0,05 | 0,18 | 2,25 |
| 0,1 | 0,36 | 4,5 | |
| 0,2 | 0,72 | 9 | |
| 0,3 | 1,08 | 13,5 | |
| 0,5 | 1,8 | 22,5 | |
| 1 | 3,6 | 45 | |
| 2 | 7,2 | 90 | |
| 70 | 0,05 | 0,21 | 2,625 |
| 0,1 | 0,42 | 5,25 | |
| 0,2 | 0,84 | 10,5 | |
| 0,3 | 1,26 | 15,75 | |
| 0,5 | 2,1 | 26,25 | |
| 1 | 4,2 | 52,5 | |
| 2 | 8,4 | 105 | |
| 80 | 0,05 | 0,24 | 3 |
| 0,1 | 0,48 | 6 | |
| 0,2 | 0,96 | 12 | |
| 0,3 | 1,44 | 18 | |
| 0,5 | 2,4 | 30 | |
| 1 | 4,8 | 60 | |
| 2 | 9,6 | 120 |
| *When using a different dilution of the concentrate, you should replace the value of the solution concentration in the formula used: | |
| Infusion rate (ml/h) = _ | dosage (mcg/kg/min) x patient weight (kg) x 60 (min) ________________________________________________ 80 µg/ml |
Arterial pressure
The duration, rate of administration and dosage of the norepinephrine solution are determined by cardiac monitoring data with mandatory medical monitoring of blood pressure (every 2 minutes until normotension is achieved, then every 5 minutes throughout the infusion) to avoid the occurrence of arterial hypertension.
Discontinuation of therapy
Drug therapy should be reduced gradually, since abrupt withdrawal can lead to acute arterial hypotension.
The duration of treatment can last from several hours to 6 days.
Features of the drug's effect upon first use or upon withdrawal
At the beginning of the infusion, it is necessary to titrate the dose of the drug until the target blood pressure is achieved. With long-term use, a decrease in plasma volume is possible (correction is necessary to avoid recurrent hypotension when the drug is discontinued).
Description of the drug EGILOK
Registration number: _______________
Trade name: Egilok®
International nonproprietary name: metoprolol
Dosage form: tablets
Composition : each tablet contains 25 mg, 50 mg or 100 mg of the active ingredient metoprolol tartrate. Excipients: microcrystalline cellulose 41.5/83/166 mg, sodium carboxymethyl starch (type A) 7.5/15/30 mg, colloidal anhydrous silicon dioxide 2/4/8 mg, povidone (K-90) 2/4/ 8 mg, magnesium stearate 2/4/8 mg.
Description : Tablets 25 mg: White or almost white, round, biconvex tablets with a cross-shaped dividing line and a double bevel (double snap shape) on one side and engraved E 435 on the other side, odorless.
Tablets 50 mg: White or almost white, round, biconvex tablets, scored on one side and engraved E 434 on the other side, odorless.
Tablets 100 mg: White or almost white, round, biconvex tablets, bevelled, scored on one side and engraved E 432 on the other side, odorless.
Pharmacotherapeutic group : selective beta1-blocker
ATX code: C07AB02
PHARMACOLOGICAL PROPERTIES
Pharmacodynamics:
Mechanism of action:
Metoprolol suppresses the effects of increased sympathetic system activity on the heart and also causes a rapid decrease in heart rate, contractility, cardiac output and blood pressure.
For arterial hypertension, metoprolol reduces blood pressure in patients in the standing and lying position. The long-term antihypertensive effect of the drug is associated with a gradual decrease in total peripheral vascular resistance.
In arterial hypertension, long-term use of the drug leads to a statistically significant decrease in the mass of the left ventricle and an improvement in its diastolic function.
In men with mild or moderate hypertension, metoprolol reduces mortality from cardiovascular causes (primarily sudden death, fatal and non-fatal heart attack and stroke).
Like other beta-blockers, metoprolol reduces myocardial oxygen demand by reducing systemic blood pressure, heart rate and myocardial contractility. A decrease in heart rate and a corresponding prolongation of diastole when taking metoprolol ensures improved blood supply and oxygen uptake by the myocardium with impaired blood flow. Therefore, for angina pectoris, the drug reduces the number, duration and severity of attacks, as well as asymptomatic manifestations of ischemia, and improves the patient’s physical performance.
In myocardial infarction, metoprolol reduces the mortality rate by reducing the risk of sudden death. This effect is primarily associated with the prevention of episodes of ventricular fibrillation. A reduction in mortality can also be observed with the use of metoprolol in both the early and late phases of myocardial infarction, as well as in high-risk patients and patients with diabetes mellitus. Use of the drug after myocardial infarction reduces the likelihood of non-fatal recurrent infarction.
In chronic heart failure against the background of idiopathic hypertrophic obstructive cardiomyopathy, metoprolol tartrate, taken starting from low doses (2-5 mg/day) with a gradual increase in dose, significantly improves heart function, quality of life and physical endurance of the patient.
In case of supraventricular tachycardia, atrial fibrillation and ventricular extrasystoles, metoprolol reduces the frequency of ventricular contractions and the number of ventricular extrasystoles.
At therapeutic doses, the peripheral vasoconstrictor and bronchoconstrictor effects of metoprolol are less pronounced than the same effects of non-selective beta-blockers.
Compared with non-selective beta-blockers, metoprolol has less effect on insulin production and carbohydrate metabolism. It does not increase the duration of hypoglycemic attacks.
Metoprolol causes a slight increase in triglyceride concentrations and a slight decrease in serum free fatty acid concentrations. There is a significant decrease in total serum cholesterol concentrations after several years of taking metoprolol.
Pharmacokinetics:
Metoprolol is quickly and completely absorbed from the gastrointestinal tract. The drug is characterized by linear pharmacokinetics in the therapeutic dose range.
The maximum concentration in blood plasma is achieved 1.5-2 hours after oral administration.
After absorption, metoprolol undergoes significant first-pass metabolism through the liver. The bioavailability of metoprolol is approximately 50% with a single dose and approximately 70% with regular use.
Taking with food can increase the bioavailability of metoprolol by 30-40%.
Metoprolol is slightly (~ 5-10%) bound to plasma proteins.
The volume of distribution is 5.6 l/kg.
Metoprolol is metabolized in the liver by cytochrome P-450 isoenzymes. Metabolites do not have pharmacological activity.
The half-life (t1/2) averages 3.5 hours (from 1 to 9 hours). The total clearance is approximately 1 l/min.
Approximately 95% of the administered dose is excreted by the kidneys, 5% as unchanged metoprolol. In some cases this value can reach 30%.
There were no significant changes in the pharmacokinetics of metoprolol in elderly patients.
Impaired renal function does not affect the systemic bioavailability or excretion of metoprolol. However, in these cases there is a decrease in the excretion of metabolites. In severe renal failure (glomerular filtration rate less than 5 ml/min), a significant accumulation of metabolites is observed. However, this accumulation of metabolites does not increase the degree of beta-adrenergic blockade.
Impaired liver function has little effect on the pharmacokinetics of metoprolol. However, in severe liver cirrhosis and after a portacaval shunt, bioavailability may increase and overall body clearance may decrease. After portacaval shunt, the total clearance of the drug from the body is approximately 0.3 L/min, and the area under the concentration-time curve increases approximately 6 times compared with that in healthy volunteers.
INDICATIONS FOR USE
Arterial hypertension (in monotherapy or (if necessary) in combination with other antihypertensive drugs); functional disorders of cardiac activity, accompanied by tachycardia.
Coronary heart disease: myocardial infarction (secondary prevention - complex therapy), prevention of angina attacks.
Heart rhythm disturbances (supraventricular tachycardia, ventricular extrasystole).
Hyperthyroidism (complex therapy).
Prevention of migraine attacks.
CONTRAINDICATIONS
Hypersensitivity to metoprolol or any other component of the drug, as well as other beta-blockers; atrioventricular block (AV) II or III degree; sinoatrial block; sinus bradycardia (heart rate less than 50/min), sick sinus syndrome; cardiogenic shock; severe peripheral circulatory disorders; heart failure in the stage of decompensation, age under 18 years (due to the lack of sufficient clinical data), simultaneous intravenous administration of verapamil, severe bronchial asthma and pheochromocytoma without simultaneous use of alpha-blockers.
Due to insufficient clinical data, Egiolok® is contraindicated in acute myocardial infarction, accompanied by a heart rate below 45 beats/min, with a PQ interval of more than 240 ms, and systolic blood pressure below 100 mm Hg.
CAREFULLY
Diabetes mellitus, metabolic acidosis, bronchial asthma, chronic obstructive pulmonary disease (COPD), renal/liver failure, myasthenia gravis, pheochromocytoma (with simultaneous use with alpha-blockers), thyrotoxicosis, AV block of the first degree, depression (including history), psoriasis, obliterating diseases of peripheral vessels (“intermittent” claudication, Raynaud’s syndrome), pregnancy, lactation, old age, in patients with a burdened allergic history (a decrease in response is possible when using adrenaline).
USE IN PREGNANCY AND LACTATION
The use of the drug is not recommended during pregnancy. The use of the drug is possible only when the benefit to the mother outweighs the potential risk to the fetus. If taking the drug is necessary, you should carefully monitor the fetus and then the newborn for several days (48 - 72 hours) after birth, as bradycardia, respiratory depression, decreased blood pressure and hypoglycemia may develop.
Although only small amounts of the drug are excreted into breast milk when taking therapeutic doses of metoprolol, the newborn should be kept under observation (bradycardia is possible). The use of the drug during lactation is not recommended. If it is necessary to use the drug during lactation, it is recommended to stop breastfeeding.
METHOD OF APPLICATION AND DOSES
Egilok® tablets are taken orally. The tablets can be taken with food or without regard to meals. If necessary, the tablet can be broken in half.
The dose should be adjusted gradually and individually to avoid excessive bradycardia. The maximum daily dose is 200 mg.
Recommended doses:
Arterial hypertension
For mild or moderate arterial hypertension, the initial dose is 25-50 mg twice a day (morning and evening). If necessary, the daily dose can be gradually increased to 100-200 mg/day or another antihypertensive agent can be added.
Angina pectoris
The initial dose is 25-50 mg two to three times a day. Depending on the effect, this dose can be gradually increased to 200 mg per day or another antianginal drug can be added.
Maintenance therapy after myocardial infarction
The usual daily dose is 100 - 200 mg/day, divided into two doses (morning and evening).
Heart rhythm disturbances
Initial dose is 25 to 50 mg two or three times daily. If necessary, the daily dose can be gradually increased to 200 mg/day or another antiarrhythmic agent can be added.
Hyperthyroidism
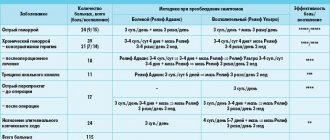
The usual daily dose is 150-200 mg per day in 3 to 4 doses.
Functional heart disorders accompanied by palpitations
The usual daily dose is 50 mg 2 times a day (morning and evening); if necessary, it can be increased to 200 mg in two doses.
Preventing migraine attacks
The usual daily dose is 100 mg/day in two divided doses (morning and evening); if necessary, it can be increased to 200 mg/day in 2 divided doses.
Special patient groups
If renal function is impaired, no change in dosage regimen is required.
In liver cirrhosis, a dose change is usually not required due to the low binding of metoprolol to plasma proteins (5-10%). In case of severe liver failure (for example, after portacaval shunt surgery), it may be necessary to reduce the dose of Egilok®.
In elderly patients, no dose adjustment is required.
SIDE EFFECTS
Egilok® is usually well tolerated by patients. Side effects are usually mild and reversible. The following side effects have been reported in clinical trials and during therapeutic use of metoprolol. In some cases, the connection between an adverse event and the use of the drug has not been reliably established. The frequency parameters of side effects listed below are defined as follows: very often: 10%, often: 1-9.9%, infrequently: 0.1-0.9%, rarely: 0.01-0.09%, very rarely ( including individual messages): 0.01%.
From the nervous system: very often - increased fatigue; often - dizziness, headache; rarely - increased excitability, anxiety, impotence/sexual dysfunction; uncommon - paresthesia, convulsions, depression, decreased concentration, drowsiness, insomnia, nightmares; very rarely - amnesia/memory impairment, depression, hallucinations.
From the cardiovascular system: often - bradycardia, orthostatic hypotension (in some cases, syncope is possible), coldness of the lower extremities, palpitations; uncommon - temporary increase in symptoms of heart failure, cardiogenic shock in patients with myocardial infarction, first degree atrioventricular block; rarely - conduction disturbances, arrhythmia; very rarely - gangrene (in patients with peripheral circulatory disorders).
From the digestive system: often - nausea, abdominal pain, constipation or diarrhea; infrequently - vomiting; rarely - dryness of the oral mucosa, impaired liver function.
From the skin: infrequently - urticaria, increased sweating; rarely - alopecia; very rarely - photosensitivity, exacerbation of psoriasis.
From the respiratory system: often - shortness of breath with physical effort; uncommon - bronchospasm in patients with bronchial asthma; rarely - rhinitis.
From the senses: rarely - blurred vision, dryness and/or irritation of the eyes, conjunctivitis; very rarely - ringing in the ears, disturbance of taste.
Other: infrequently - weight gain; very rarely - arthralgia, thrombocytopenia.
Taking Egilok® should be discontinued if any of the above effects reaches a clinically significant intensity, and its cause cannot be reliably determined.
OVERDOSE
Symptoms: marked decrease in blood pressure, sinus bradycardia, atrioventricular block, heart failure, cardiogenic shock, asystole, nausea, vomiting, bronchospasm, cyanosis, hypoglycemia, loss of consciousness, coma.
The symptoms listed above may increase with the simultaneous use of ethanol, antihypertensive drugs, quinidine and barbiturates.
The first symptoms of overdose appear 20 minutes - 2 hours after taking the drug.
Treatment: careful monitoring of the patient is necessary (monitoring blood pressure, heart rate, respiratory rate, renal function, blood glucose concentration, serum electrolytes) in the intensive care unit.
If the drug has been taken recently, gastric lavage with activated charcoal may reduce further absorption of the drug (if lavage is not possible, vomiting can be induced if the patient is conscious).
In case of excessive decrease in blood pressure, bradycardia and threat of heart failure - intravenously, at intervals of 2-5 minutes, beta-adrenergic agonists - until the desired effect is achieved, or 0.5-2 mg of atropine intravenously. If there is no positive effect, dopamine, dobutamine or norepinephrine (norepinephrine). For hypoglycemia - administration of 1-10 mg of glucagon, installation of a temporary pacemaker. For bronchospasm, beta2-agonists should be administered. For convulsions - slow intravenous administration of diazepam. Hemodialysis is ineffective.
INTERACTIONS WITH OTHER MEDICINES
The antihypertensive effects of Egilok® and other antihypertensive drugs are usually enhanced. To avoid hypotension, careful monitoring of patients receiving combinations of these drugs is necessary. However, the summation of the effects of antihypertensive drugs can be used, if necessary, to achieve effective blood pressure control.
The simultaneous use of metoprolol and blockers of “slow” calcium channels such as diltiazem and verapamil can lead to increased negative inotropic and chronotropic effects. Intravenous administration of calcium channel blockers such as verapamil should be avoided in patients receiving beta-blockers.
Caution should be exercised when taken concomitantly with the following drugs:
Oral antiarrhythmic drugs (such as quinidine and amiodarone) - risk of bradycardia, atrioventricular block.
Cardiac glycosides (risk of bradycardia, conduction disorders; metoprolol does not affect the positive inotropic effect of cardiac glycosides).
Other antihypertensive drugs (especially the guanethidine, reserpine, alpha-methyldopa, clonidine and guanfacine groups) due to the risk of hypotension and/or bradycardia.
Stopping the simultaneous use of metoprolol and clonidine should definitely begin by stopping metoprolol, and then (after a few days) clonidine; If clonidine is first discontinued, a hypertensive crisis may develop.
Some drugs acting on the central nervous system, such as hypnotics, tranquilizers, tri- and tetracyclic antidepressants, antipsychotics and ethanol, increase the risk of arterial hypotension.
Anesthesia (risk of cardiac depression).
Alpha and beta sympathomimetics (risk of arterial hypertension, significant bradycardia; possibility of cardiac arrest).
Ergotamine (increased vasoconstrictor effect).
Beta2-sympathomimetics (functional antagonism).
Nonsteroidal anti-inflammatory drugs (for example, indomethacin) may weaken the antihypertensive effect.
Estrogens (possibly reducing the antihypertensive effect of metoprolol).
Oral hypoglycemic agents and insulin (metoprolol may enhance their hypoglycemic effects and mask the symptoms of hypoglycemia).
Curare-like muscle relaxants (increased neuromuscular blockade).
Enzyme inhibitors (for example, cimetidine, ethanol, hydralazine; selective serotonin reuptake inhibitors, for example, paroxetine, fluoxetine and sertraline) - increased effects of metoprolol due to an increase in its concentration in the blood plasma.
Enzyme inducers (rifampicin and barbiturates): the effects of metoprolol may be reduced due to increased hepatic metabolism.
Concomitant use of sympathetic ganglion blockers or other beta blockers (eg eye drops) or monoamine oxidase inhibitors requires careful medical monitoring.
SPECIAL INSTRUCTIONS
Monitoring of patients taking beta-blockers includes regular measurement of heart rate (HR) and blood pressure, blood glucose concentration in patients with diabetes mellitus. If necessary, for patients with diabetes mellitus, the dose of insulin or hypoglycemic agents for oral administration should be selected individually. The patient should be taught how to calculate heart rate and instructed about the need for medical consultation if the heart rate is less than 50 beats/min. When taking a dose above 200 mg per day, cardioselectivity decreases.
In case of heart failure, treatment with Egilok® begins only after reaching the stage of compensation of cardiac function.
There may be an increase in the severity of hypersensitivity reactions and a lack of effect from the administration of usual doses of epinephrine (adrenaline) in patients with a burdened allergic history.
Anaphylactic shock may be more severe in patients taking Egilok®.
May increase symptoms of peripheral arterial circulation disorders.
Abrupt discontinuation of Egilok® should be avoided. The drug should be discontinued gradually by reducing doses over approximately 14 days. Abrupt withdrawal may worsen angina symptoms and increase the risk of coronary events. When discontinuing the drug, special attention should be paid to patients with coronary artery disease.
For exertional angina, the selected dose of Egilok® should ensure the heart rate at rest is within 55-60 beats/min, and during exercise - no more than 110 beats/min.
Patients who use contact lenses should take into account that during treatment with beta-blockers, there may be a decrease in the production of tear fluid.
Egilok® may mask some clinical manifestations of hyperthyroidism (for example, tachycardia). Abrupt withdrawal in patients with thyrotoxicosis is contraindicated as it can increase symptoms.
In diabetes mellitus, it can mask tachycardia caused by hypoglycemia. Unlike non-selective beta-blockers, it practically does not enhance insulin-induced hypoglycemia and does not delay the restoration of blood glucose concentrations to normal levels. If Egilok® is prescribed to patients with diabetes mellitus, the blood glucose concentration should be monitored and, if necessary, the dose of insulin or oral hypoglycemic agents should be adjusted (see section “Interaction with other drugs”).
If necessary, beta2-adrenergic stimulants are prescribed to patients with bronchial asthma; for pheochromocytoma - alpha-blockers.
If surgical intervention is necessary, it is necessary to warn the surgeon/anesthesiologist about the therapy being performed (choosing a general anesthesia agent with minimal negative inotropic effect); discontinuation of the drug is not recommended.
Drugs that reduce catecholamine levels (for example, reserpine) may enhance the effect of beta-blockers, so patients taking such combinations of drugs should be under constant medical supervision to detect an excessive decrease in blood pressure or bradycardia.
In elderly patients, regular monitoring of liver function is recommended. Correction of the dosage regimen is required only if an elderly patient develops increasing bradycardia (less than 50 beats/min), a pronounced decrease in blood pressure (systolic blood pressure below 100 mm Hg), atrioventricular block, bronchospasm, ventricular arrhythmias, severe liver dysfunction , sometimes it is necessary to stop treatment. In patients with severe renal failure, monitoring of renal function is recommended.
Special monitoring should be carried out for the condition of patients with depressive disorders taking metoprolol; in case of development of depression caused by taking beta-blockers, it is recommended to discontinue therapy.
If progressive bradycardia occurs, the dose should be reduced or the drug discontinued.
Due to the lack of sufficient clinical data, the drug is not recommended for use in children.
Impact on the ability to drive vehicles and complex equipment. Caution must be exercised when driving vehicles and when engaging in potentially hazardous activities that require increased concentration (risk of dizziness and fatigue).
RELEASE FORM
Tablets 25 mg: 60 tablets in a brown glass bottle with a PE cap with an accordion shock absorber, with first opening control. 1 bottle along with instructions for use is packed in a cardboard box. Or 20 tablets in a blister made of PVC/PVDC//al. foil. 3 blisters along with instructions for use are packed in a cardboard box.
Tablets 50 mg: 60 tablets in a brown glass bottle with a PE cap with an accordion shock absorber, with first opening control. 1 bottle along with instructions for use is packed in a cardboard box. Or 15 tablets in a blister made of PVC/PVDC//al. foil. 4 blisters along with instructions for use are packed in a cardboard box.
Tablets 100 mg: 30 or 60 tablets in a brown glass bottle with a PE cap with an accordion shock absorber, with first opening control. 1 bottle along with instructions for use is packed in a cardboard box.
BEST BEFORE DATE
5 years. Do not use after the expiration date indicated on the package
STORAGE CONDITIONS
Store at a temperature of 15 to 25 °C, out of the reach of children.
VACATION CONDITIONS
On prescription
MANUFACTURER
CJSC "EGIS Pharmaceutical Plant"
1106 Budapest, st. Keresturi 30-38, HUNGARY,
phone: (36-1)803-5555, fax: (36-1)803-5529
Representative office of CJSC "EGIS Pharmaceutical Plant" (Hungary), Moscow
121108, Moscow, st. Ivana Franko, 8, phone: (495) 363-39-66
* In the case of packaging and packaging of the drug in Russia, the following is additionally indicated:
Prepackaged, packaged:
SERDIX LLC
Russia, 142150 Moscow region, Podolsky district, Sofiino village, building 1/1