Obstructive bronchitis is an inflammation of the bronchi, which is accompanied by a narrowing of their lumen due to swelling or spasm, as well as the accumulation of thick mucus, which leads to impaired ventilation. The disease manifests itself as a wet cough, shortness of breath, and wheezing. Unlike other forms of bronchitis, the treatment regimen in this case is broader: antispasmodic therapy, hormonal drugs and more are often included.
Acute obstructive bronchitis often develops in young children, while adults are more susceptible to chronic disease. In the second case, concomitant disorders are often observed, that is, we are talking about chronic obstructive pulmonary disease.
How is acute obstructive bronchitis diagnosed?
- To diagnose acute obstructive bronchitis, the pulmanologist carries out a full examination: will study the patient’s complaints, perform an examination, auscultation, and measure the level of oxygen in the blood;
- Using spirometry, he will be able to make a decision: to prescribe inhalers with a drug that dilates the bronchi, or the patient can do without them;
- A blood test is required to identify markers indicating the onset of inflammation. In addition, all possible pathogens of acute bronchitis will be identified;
- Radiography turns out to be useless in order to make an accurate diagnosis of “acute bronchitis”; it will not help determine diseases such as lung cancer, pulmonary embolism and all types of bronchiectasis. But with its help, the doctor can rule out pneumonia. It is for this reason that CT examination of the lungs is increasingly being prescribed.
For more accurate treatment, it is very important to make a correct diagnosis. It will be necessary to exclude such possible diseases as:
- pneumonia;
- postnasal drip;
- whooping cough;
- acute heart failure;
- thromboembolism in the pulmonary artery;
- lungs' cancer.
Excluding these and many other diseases of the respiratory system will allow you to begin effective treatment.
Diagnostics
The beginning of diagnosis consists of a thorough collection of complaints and medical history. An informative method is to listen to breathing in the lungs using a phonendoscope. Obstruction is characterized by the presence of scattered dry or moist rales. In addition to the examination, if necessary, the doctor may prescribe additional tests:
- X-ray of the OGK;
- Spirometry;
- General blood analysis;
- Blood biochemistry (to determine markers of inflammation);
- Bacteriological examination of sputum and culture for sensitivity to antibiotics;
- CT or MRI of the lungs to assess the presence and nature of changes in them3.
After making a diagnosis, the doctor should talk about the prevention of exacerbations of obstructive bronchitis and prescribe a course of treatment.
How is obstructive bronchitis treated?
Doctors warn that you should not trust the advice of “professional” doctors who conduct their consultations via the Internet. Moreover, you should not take antibiotics while self-medicating. Only after examination and tests will the doctor be able to tell what exactly you are sick with.
You should seek medical help immediately if:
- high fever lasts more than 4 days, accompanied by severe chills;
- if you have a cough with green or yellow sputum, especially if there are traces of blood in it;
- wheezing and whistling in the chest are observed;
- with difficulty breathing and suffocation.
Most often, bronchitis is treated in a hospital setting. In this case, not only antibiotics are used, but also other drugs that are prescribed only after a complete examination.
Course of the disease and symptoms
Adults during the period of remission of the disease do not stop coughing. The cough is characterized as dry; a little mucous sputum may be released. Shortness of breath is constant or intermittent. During an exacerbation, the nature of the sputum is different. It becomes completely purulent or either mucopurulent. In severe cases, streaks or even blood clots are found in the sputum, which is called hemoptysis. The cough is severe, constant, and there is wheezing.
Another symptom of obstructive bronchitis in adults, as already noted, is shortness of breath. It can be present from the first day of the disease, but in some cases it appears later. This symptom is recorded in 100% of cases of the disease in question. Shortness of breath can vary in severity and intensity, which depends on the severity of obstructive bronchitis, the absence or presence of concomitant complications and other chronic diseases that can worsen during the same period.
In patients, the inhalation period is increased. Not only the respiratory muscles take part in the expansion of the chest, but also an additional group of muscles of the back and shoulder-scapular region. Oxygen deficiency in the body causes cyanosis (blue discoloration) of certain areas, mainly the nail plates and lips on the face. The patient generally feels unwell (malaise), sweating is increased, and it is even more pronounced with coughing and increased shortness of breath.
Other common symptoms:
- muscle pain
- joint pain
- body aches
- increase in body temperature
- increased blood pressure (BP)
- feeling of fear and anxiety due to the occurrence and intensification of shortness of breath
- decreased productivity in severe cases
How to identify chronic bronchitis
Determining the extent of the disease, as well as making an accurate diagnosis, completely depends on the indicators obtained during diagnosis. However, you can determine the form yourself if you pay attention to the following symptoms:
- Cough if it continues for 3 months and does not stop for 2 years. Particular attention should be paid to a wet and deep cough, when sputum of various colors is coughed up. The appearance of sputum indicates an inflammatory process in the bronchi, accompanied by thick secretion of the mucous membrane. It is worth saying that chronic bronchitis is accompanied by a violation of the ability to remove phlegm from the lungs. As a result, damage and even death of the ciliated epithelium occurs, which lines the tubes of both bronchi. The separation of sputum stops, as a result it will be viscous and stringy;
- The temperature begins to rise when the body turns on its protective function in response to the penetration of microbes. The person experiences chills. This produces green mucus, often accompanied by an unpleasant odor. Such a symptom may occur in pneumonia or obstructive chronic bronchitis;
- Fatigue increases. A severe, lingering cough leads to the body becoming exhausted both physically and mentally;
- Severe wheezing and whistling are heard in the chest, which is the main symptom of exacerbation of chronic obstructive bronchitis. Moreover, these sounds will be audible both to the person himself and to those around him;
- Shortness of breath appears, meaning that the body does not have enough oxygen;
- Chest pain intensifies as a result of severe coughing and general fatigue of the body.
Prevention
To prevent exacerbations of chronic bronchitis, a person must first give up smoking and work in conditions of increased air pollution. An adequate response of local immunity to viruses and bacteria is also very important. If there is no such response, activation of local immunity is required, since the body’s protective factors can eliminate most of the pathogens that lead to bronchitis.
IRS®19 is a drug with an immunomodulatory local effect, which includes a mixture of 18 bacterial lysates. It comes in the form of a nasal spray and acts directly on the nasal mucosa, which is considered the entry point for viruses and bacteria into the respiratory tract4.
IRS®19 activates immune cells of the nasal mucosa and begins to act immediately upon contact with the mucous membrane5. When added to standard symptomatic therapy, IRS®19 reduces the duration of symptoms by 2 times5. The drug is used for the treatment and prevention of respiratory diseases in children and adults from three months.
Basic means of diagnosing obstructive bronchitis
To obtain the most accurate diagnosis, it is very important to conduct high-quality diagnostics.
- Computed tomography allows you to immediately exclude diseases that have similar symptoms, such as lung cancer, pneumonia or bronchiectasis;
- Spirometry or FVD is a breathing test that makes it possible to exclude bronchial asthma from a possible list of diseases. With its help, COPD is detected;
- Thanks to blood tests, doctors can detect the presence of an inflammatory process occurring in the body. The degree of activity of microorganisms and viruses that cause inflammation will be determined immediately;
- Using sputum cultures, it is possible to identify bacteria that provoke inflammatory processes in the bronchi.
Causes and pathogens
Frequent bronchopulmonary diseases are more common in children than in adults, since adults have stronger immunity and adhere to preventive measures. But in practice, it turns out that obstructive bronchitis in adults is quite common. Among the causes that do not depend on humans are viruses and bacteria. Obstructive bronchitis can occur against the background of any viral infection. The most common pathogens:
- influenza viruses
- parainfluenza viruses
- rhinoviruses
- adenoviruses
- combination of bacteria and viruses
Factors predisposing to obstructive bronchitis in adults are the presence of foci of chronic infection in the nasopharynx and frequent colds. Any infection, including the disease in question, can spread either downward or upward. Doctors advise: when you get a cold, you need to stay in bed. Because any cold can “sink” into the lungs. This means that obstructive bronchitis in some cases is a complication of influenza or acute respiratory infections.
Smoking is also a cause or contributing factor. Smokers can no longer be scared of lung cancer, because often such cases remain for adherents of the bad habit only a scary story that does not occur in practice. But bronchitis is noted in almost all “experienced” smokers.
The concept of “smoker's chronic bronchitis” has long been used by doctors. This condition is characterized by shortness of breath, specific breathing, and a strong hacking cough, which appears especially often in the morning. After smoking, the coughing attack is less, and then it increases again. Therefore, by smoking another cigarette, a person alleviates his condition. But in this process the bronchi are damaged even more.
Obstructive bronchitis in adults also occurs among passive smokers. If a person is predisposed to colds, has a weakened immune system, and someone in his constant environment smokes, in such a person a bronchopulmonary inflammatory process begins in some cases.
Another factor predisposing to illness is involvement in hazardous work. Obstructive bronchitis in adults is found among those who work:
- at metallurgical enterprises
- in the mines
- agriculture
- construction
- railway services
- printing houses
Employees of enterprises with increased occupational health risks belong to the risk group for bronchopulmonary pathologies. Not so long ago, the disease in question was considered more masculine. But statistics in recent years have shown that among patients there is an equal number of people of both sexes. And the reason for this is partly the consequences of emancipation: women began to smoke, drink more alcohol and work more in hazardous industries. The reason lies in the gradually deteriorating environmental situation.
Basic ways to avoid bronchitis or quickly recover from illness
If you want to prevent the occurrence or development of bronchitis, you should be careful about your health. For example, smokers are advised to quit or reduce the number of cigarettes they smoke. This will reduce the rate of development of COPD and reduce the severity of cough. Playing sports or traveling, especially walking or cycling, will not interfere.
It is recommended to undergo annual vaccination to protect against influenza, as well as pneumonia, which is done once every five years.
Obstructive bronchitis - treatment in adults and children
Treatment of acute and chronic obstructive bronchitis in children and adults includes:
- peace;
- air humidification in the apartment;
- plenty of warm drinks;
- medicinal/alkaline inhalations.
The patient is prescribed antiviral drugs - Ribavirin, Interferon, etc. If the obstruction is severe, the following are used:
- mucolytic agents (Lazolvan, Acetylcysteine);
- expectorants (ACC, Ambroxol);
- antispasmodics (No-shpa, Papaverine);
- bronchodilator inhalers (Berodual, Salbutamol, Astmopent).
Help improve sputum discharge:
- Percussion chest massage. The skin is rubbed, paying maximum attention to the muscles of the chest and intercostal space. Afterwards, the patient lies on his stomach and lowers his head down. The doctor taps the chest from the back.
- Back muscle massage.
- Vibration chest massage. The vibration effect on tissue, provided with the help of special vibration massagers, reduces the inflammatory process.
- Breathing exercises.
Antibiotics for the treatment of obstructive bronchitis in children and adults are prescribed:
- in case of secondary microbial infection;
- if the disease is caused by bacteria;
- in the absence of positive dynamics from the treatment methods used.
Antibacterial drugs can achieve the best effect for obstruction:
- from the group of macrolides, for example, Azithromycin, Erythromycin;
- from the group of protected penicillins - Amoxicillin + Clavulanic acid.
Bronchodilator medications that improve the quality of life of patients and normalize breathing include:
- xanthines (Theophylline);
- b2-agonists (Berotec);
- anticholinergics (Atrovent).
When there is an increased level of carbon dioxide in the blood and tissues (hypercopnia), oxygen therapy is used. Treatment with an air environment allows you to increase oxygen pressure, due to which detoxification, oxidative and regenerative processes are activated, the heartbeat and breathing rate are normalized, and performance increases.
Treatment of obstructive bronchitis with folk remedies
Treatment of obstructive bronchitis in children and adults at home can be carried out using the following recipes.
- Compress with honey and butter. You need to mix the components in equal proportions. Apply the mixture to the chest area and back. Cover the top with cellophane film and a towel. Keep it on all night. Repeat every day until recovery.
- Elecampane decoction. Pour one spoon of herb into a liter of boiling water. Infuse, strain. Drink 3 times a day.
- Black radish with honey. It is necessary to make a hole in the radish, put 1 tbsp there. natural honey. Leave for 1 day. Take the resulting liquid 1 tsp. 3-4 times a day after meals.
- Onions with honey (expectorant). You need to cook two peeled onions in an enamel bowl for 2 hours. Then grind them in a blender. Add 4 tbsp to the onion pulp. honey, 4 tbsp. sugar, 2 tbsp. vinegar. Mix. Take the mixture 1 tsp. every hour for one week.
- Viburnum with honey (for barking cough). To prepare the medicine, put 200 g of viburnum and 200 g of honey in an enamel bowl. Pour in 100 g of water. Cook until boiling over low heat. When it boils, reduce the heat and wait until all the water has boiled away. Transfer the hot paste into a glass jar. Every hour eat 1 tbsp. medications.
- Buckwheat infusion. Place 40 g of buckwheat flowers in a thermos. Pour in 1 liter of boiling water. Leave for 1 hour. Strain. Drink the resulting volume throughout the day.
- Freshly squeezed carrot juice. Prepare carrot juice, mix it in equal proportions with natural honey. Take a spoonful every hour on the first day of treatment and every 2 hours on the second and third days.
- Sage decoction. 3 tbsp. put the collection in an enamel pan. Pour in a liter of milk and bring to a boil. After boiling, cook over low heat for 15 minutes. Remove from heat, cover with a lid. Leave for one hour. Strain. Add 3 tbsp to the broth. honey Drink 1/2 glass 5 times a day.
The most effective methods of treating chronic obstructive bronchitis
For treatment, first of all, contact a pulmonologist who will prescribe examination and treatment. At the Integramed respiratory medicine clinic, appointments are conducted by pulmonologists with 20 years of experience. Applicable:
- Therapy carried out with specially developed drugs. First of all, these will be medications that make it possible to dilate the bronchi - bronchodilators. They are used as inhalations. As a result of the effect of the medicine, the bronchi expand, which improves breathing and mucus removal;
- Antibiotics are used that successfully destroy bacteria and viruses that provoke inflammatory processes. Their dosage is prescribed only by a pulmonologist or therapist;
- It is possible to prescribe an oxygen inhalation procedure;
- A vibration massage of the chest will also not be amiss, as it allows for a better effect on the lungs and speeds up the removal of phlegm.
- In some cases, folk remedies can also help. But only in consultation with your doctor and in the indicated doses.
Treatment
Therapy for obstructive bronchitis should be comprehensive. To reduce obstruction syndrome, bronchodilators are used - drugs that relieve spasm and expand the lumen of the bronchi. This makes breathing easier and eliminates shortness of breath. Medicines that thin mucus and relieve cough are also prescribed. If a bacterial cause of bronchitis is confirmed, a course of antibiotics is necessary to prevent the infection from developing into pneumonia. Antihistamines (antiallergic) drugs are used if the obstruction is caused by an allergic component.
Modern therapy of chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD) is a disease characterized by progressive, partially reversible bronchial obstruction, which is associated with inflammation of the airways that occurs under the influence of unfavorable environmental factors (smoking, occupational hazards, pollutants, etc.). It has been established that morphological changes in COPD are observed in the central and peripheral bronchi, pulmonary parenchyma and vessels [8, 9]. This explains the use of the term “chronic obstructive pulmonary disease” instead of the usual “chronic obstructive bronchitis,” which implies a predominant lesion of the bronchi in the patient.
The recently published recommendations of leading experts from the American and European Thoracic Societies emphasize that the development of COPD in patients can be prevented, and with its treatment it is quite possible to achieve success [7].
The morbidity and mortality of patients from COPD continues to increase worldwide, primarily due to the high prevalence of smoking. It has been shown that this disease affects 4–6% of men and 1–3% of women over 40 years of age [8, 10]. In European countries, it causes the death of 200–300 thousand people annually [10]. The high medical and social significance of COPD was the reason for the publication, at the initiative of the WHO, of an international consensus document devoted to its diagnosis, treatment, prevention and based on the principles of evidence-based medicine [8]. Similar recommendations have been issued by the American and European Respiratory Societies [7]. In our country, the 2nd edition of the Federal Program on COPD was recently published [1].
The goals of COPD therapy are to prevent disease progression, reduce the severity of clinical symptoms, achieve better exercise tolerance and improve the quality of life of patients, prevent complications and exacerbations, and reduce mortality [8, 9].
The main directions of treatment for COPD are reducing the impact of adverse environmental factors (including smoking cessation), patient education, the use of medications and non-drug therapy (oxygen therapy, rehabilitation, etc.). Various combinations of these methods are used in patients with COPD in remission and exacerbation.
Reducing the impact of risk factors on patients is an integral part of the treatment of COPD, which helps prevent the development and progression of this disease. It has been established that quitting smoking can slow down the increase in bronchial obstruction. Therefore, treatment of tobacco addiction is important for all patients suffering from COPD. The most effective in this case are conversations with medical personnel (individual and group) and pharmacotherapy. There are three tobacco dependence treatment programs: short (1–3 months), long-term (6–12 months) and a program to reduce smoking intensity [2].
It is recommended to prescribe medications for patients with whom the doctor’s conversations were not sufficiently effective. A careful approach should be taken to their use in people who smoke less than 10 cigarettes per day, adolescents and pregnant women. Contraindications to nicotine replacement therapy are unstable angina, untreated peptic ulcer of the duodenum, recent acute myocardial infarction and cerebrovascular accident.
Increasing patients' awareness allows them to increase their performance, improve their health, develop the ability to cope with the disease, and increase the effectiveness of treatment of exacerbations [8]. Forms of patient education vary from distributing printed materials to holding seminars and conferences. The most effective is interactive training, which is carried out in a small seminar.
The principles of treatment of stable COPD [6, 8] are as follows.
- The volume of treatment increases as the severity of the disease increases. Its reduction in COPD, unlike bronchial asthma, is usually impossible.
- Drug therapy is used to prevent complications and reduce the severity of symptoms, the frequency and severity of exacerbations, increase exercise tolerance and the quality of life of patients.
- It should be borne in mind that none of the available drugs affects the rate of decrease in bronchial obstruction, which is the hallmark of COPD.
- Bronchodilators are central to the treatment of COPD. They reduce the severity of the reversible component of bronchial obstruction. These funds are used on an on-demand or regular basis.
- Inhaled glucocorticoids are indicated for severe and extremely severe COPD (with forced expiratory volume in 1 s (FEV1) less than 50% of predicted and frequent exacerbations, usually more than three in the last three years or one or two in one year, for the treatment of which Oral steroids and antibiotics are used.
- Combination therapy with inhaled glucocorticoids and long-acting β2-agonists has a significant additional effect on pulmonary function and clinical symptoms of COPD compared with monotherapy with either drug. The greatest impact on the frequency of exacerbations and quality of life is observed in patients with COPD with FEV1<50% of predicted. These drugs are preferably prescribed in inhalation form containing their fixed combinations (salmeterol/fluticasone propionate, formoterol/budesonide).
- Long-term use of tableted glucocorticoids is not recommended due to the risk of systemic side effects.
- At all stages of COPD, physical training programs are highly effective, increasing exercise tolerance and reducing the severity of shortness of breath and fatigue.
- Long-term administration of oxygen (more than 15 hours per day) to patients with respiratory failure increases their survival.
Drug treatment of stable COPD
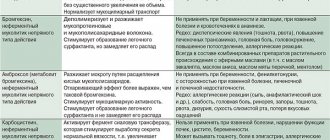
Bronchodilators. These include β2-adrenergic agonists, anticholinergics, and theophylline. The forms of release of these drugs and their effect on the course of COPD are given in tables 1 and .
The principles of bronchodilator therapy for COPD [6–8] are as follows.
- The preferred route of administration of bronchodilators is inhalation.
- Changes in pulmonary function after short-term administration of bronchodilators are not an indicator of their long-term effectiveness. A relatively small increase in FEV1 can be combined with significant changes in lung volumes, including a decrease in residual lung volume, which helps reduce the severity of shortness of breath in patients.
- The choice between β2-adrenergic agonists, anticholinergics, and theophylline depends on their availability, the individual sensitivity of patients to their action and the absence of side effects. In elderly patients with concomitant diseases of the cardiovascular system (coronary artery disease, heart rhythm disturbances, arterial hypertension, etc.), anticholinergics are preferred as first-line drugs.
- Xanthines are effective for COPD, but due to the possibility of developing side effects, they are classified as “second-line” drugs. When prescribing them, it is recommended to measure the concentration of theophylline in the blood. It should be emphasized that only long-acting theophyllines (but not aminophylline and theophedrine!) have a positive effect on the course of COPD.
- Long-acting inhaled bronchodilators are more convenient, but also more expensive than short-acting ones.
- Regular treatment with long-acting bronchodilators (tiotropium bromide, salmeterol and formoterol) is indicated for moderate, severe and extremely severe COPD.
- The combination of several bronchodilators (for example, anticholinergics and β2-agonists, anticholinergics and theophyllines, β2-agonists and theophyllines) may increase effectiveness and reduce the likelihood of side effects compared with monotherapy with a single drug.
Metered aerosols, powder inhalers and nebulizers are used to deliver β2-agonists and anticholinergics. The latter are recommended in the treatment of exacerbations of COPD, as well as in patients with severe disease who have difficulty using other delivery systems. For stable COPD, metered dose and powder inhalers are preferred.
Glucocorticoids. These drugs have pronounced anti-inflammatory activity, although in patients with COPD it is significantly less pronounced than in patients with asthma. Short (10–14 days) courses of systemic steroids are used to treat exacerbations of COPD. Long-term use of these drugs is not recommended due to the risk of side effects (myopathy, osteoporosis, etc.).
Data on the effect of inhaled glucocorticoids on the course of COPD are summarized in Table 2. It is shown that they have no effect on the progressive decrease in bronchial obstruction in patients with COPD. Their high doses (for example, fluticasone propionate 1000 mcg/day) can improve the quality of life of patients and reduce the frequency of exacerbations of severe and extremely severe COPD.
The reasons for the relative steroid resistance of airway inflammation in COPD are the subject of intense research. This may be due to the fact that corticosteroids increase the lifespan of neutrophils by inhibiting their apoptosis. The molecular mechanisms underlying resistance to glucocorticoids are not well understood. There have been reports of a decrease in the activity of histone deacetylase, which is a target for the action of steroids, under the influence of smoking and free radicals, which may reduce the inhibitory effect of glucocorticoids on the transcription of “inflammatory” genes and weaken their anti-inflammatory effect.
Recently, new data have been obtained on the effectiveness of combination drugs (fluticasone propionate/salmeterol 500/50 mcg, 1 inhalation 2 times a day and budesonide/formoterol 160/4.5 mcg, 2 inhalations 2 times a day, budesonide/salbutamol 100/200 mgk 2 inhalations 2 times a day) in patients with severe and extremely severe COPD. It has been shown that their long-term (12 months) administration improves bronchial patency, reduces the severity of symptoms, the need for bronchodilators, the frequency of moderate and severe exacerbations, and also improves the quality of life of patients compared to monotherapy with inhaled glucocorticoids, long-acting β2-adrenergic agonists and placebo [ 5, 14].
Vaccines . Influenza vaccination reduces the severity of exacerbations and mortality in patients with COPD by approximately 50%. Vaccines containing killed or inactivated live influenza viruses are usually administered once in October - the first half of November.
There is insufficient data on the effectiveness of the pneumococcal vaccine, containing 23 virulent serotypes of this microorganism, in patients with COPD [8, 9]. However, some experts recommend its use in this disease to prevent pneumonia [6].
Antibiotics. Currently, there is no convincing data on the effectiveness of antibacterial agents to reduce the frequency and severity of non-infectious exacerbations of COPD.
Antibiotics are indicated for the treatment of infectious exacerbations of the disease, directly affect the duration of elimination of COPD symptoms, and some help lengthen the interval between relapses.
Mucolytics (mucokinetics, mucoregulators). Mucolytics (ambroxol, carbocysteine, iodine preparations, etc.) can be used in a small proportion of patients with viscous sputum. Widespread use of these agents in patients with COPD is not recommended.
Antioxidants. N-acetylcysteine, which has antioxidant and mucolytic activity, can reduce the duration and frequency of exacerbations of COPD. This drug can be used in patients for a long time (3–6 months) at a dose of 600 mg/day.
Immunoregulators (immunostimulants, immunomodulators). Regular use of these drugs is not recommended due to the lack of convincing evidence of effectiveness.
Patients with genetically determined α1-antitrypsin deficiency who develop COPD at a young age (before 40 years) are possible candidates for replacement therapy. However, the cost of such treatment is very high, and it is not available in all countries.
Non-drug treatment of stable COPD
Oxygen therapy
It is known that respiratory failure is the main cause of death in patients with COPD. Correction of hypoxemia using oxygen supply is a pathogenetically based treatment method. There are short-term and long-term oxygen therapy [4, 15]. The first is used for exacerbations of COPD. The second is used for extremely severe COPD (with FEV1<30% of predicted) constantly or situationally (during physical activity and during sleep). The goal of oxygen therapy is to increase the partial tension of oxygen (PaO2) in arterial blood to at least 60 mmHg. Art. or saturation (SaO2) to at least 90% at rest, during physical activity and during sleep.
In stable COPD, continuous long-term oxygen therapy is preferable [9]. It has been proven that it increases the survival of patients with COPD, reduces the severity of shortness of breath, the progression of pulmonary hypertension, reduces secondary erythrocytosis, the frequency of episodes of hypoxemia during sleep, increases exercise tolerance, quality of life and neuropsychic status of patients [3, 4].
Indications for long-term oxygen therapy in patients with extremely severe COPD (with FEV1 < 30% of predicted or less than 1.5 l):
- PaO2 is less than 55% of the expected value, SaO2 is below 88% with or without hypercapnia;
- PaO2 - 55–60% of the expected value, SaO2 - 89% in the presence of pulmonary hypertension, peripheral edema associated with decompensation of the pulmonary heart or polycythemia (hematocrit more than 55%).
Gas exchange parameters should be assessed only against the background of a stable course of COPD and no earlier than 3–4 weeks after an exacerbation with optimally selected therapy. The decision to prescribe oxygen therapy should be based on measurements obtained at rest and during exercise (eg, a 6-minute walk). Re-evaluation of arterial blood gases should be performed 30–90 days after the start of oxygen therapy.
Long-term oxygen treatment should be carried out for at least 15 hours a day. The gas flow rate is usually 1–2 l/min; if necessary, it can be increased to 4 l/min. Oxygen therapy should never be prescribed to patients who continue to smoke or suffer from alcoholism.
Compressed gas cylinders, oxygen concentrators and liquid oxygen cylinders are used as oxygen sources. Oxygen concentrators are the most economical and convenient for home use.
Oxygen is delivered to the patient using masks, nasal cannulas, and transtracheal catheters. The most convenient and widely used are nasal cannulas, which allow the patient to receive an oxygen-air mixture with 30–40% O2. Oxygen is delivered to the alveoli only in the early phase of inspiration (the first 0.5 s). The gas arriving later is used only to fill the dead space and does not participate in gas exchange. To increase delivery efficiency, there are several types of oxygen-saving devices (reservoir cannulas, devices that supply gas only during inspiration, transtracheal catheters, etc.). In patients with extremely severe COPD who have daytime hypercapnia, the combined use of long-term oxygen therapy and non-invasive ventilation with positive inspiratory pressure is possible [9]. It should be noted that oxygen therapy is one of the most expensive methods of treating patients with COPD. Its introduction into everyday clinical practice is one of the most pressing medical and social tasks in Russia.
Rehabilitation
Rehabilitation is a multidisciplinary program of individualized care for patients with COPD, designed to improve their physical, social adaptation and autonomy. Its components are physical training, patient education, psychotherapy and rational nutrition [7].
In our country, this traditionally includes sanatorium-resort treatment. Pulmonary rehabilitation should be prescribed for moderate, severe and extremely severe COPD. It has been shown to improve performance, quality of life and survival of patients, reduce shortness of breath, the frequency and duration of hospitalizations, and suppress anxiety and depression. The effect of rehabilitation remains after its completion. It is optimal to work with patients in small (6–8 people) groups with the participation of specialists in various fields for 6–8 weeks.
In recent years, much attention has been paid to rational nutrition, since weight loss (> 10% within 6 months or > 5% within the last month) and especially loss of muscle mass in patients with COPD is associated with high mortality. Such patients should be recommended a high-calorie diet with a high protein content and dosed physical activity that has an anabolic effect.
Surgery
The role of surgical treatment in patients with COPD is currently the subject of research. The possibilities of using bullectomy, lung volume reduction surgery, and lung transplantation are currently being discussed.
The indication for bullectomy in COPD is the presence in patients of bullous pulmonary emphysema with large bullae causing the development of shortness of breath, hemoptysis, pulmonary infections and chest pain. This surgery results in decreased shortness of breath and improved lung function.
The value of surgery to reduce lung volume in the treatment of COPD has not yet been sufficiently studied. The results of a recently completed study (National Emphysema Therapy Trial) indicate a positive effect of this surgical intervention compared with drug therapy on the ability to perform physical activity, quality of life and mortality in patients with COPD who have predominantly severe upper lobe emphysema and an initially low level of performance [12]. However, this operation remains an experimental palliative procedure that is not recommended for widespread use [9].
Lung transplantation improves the quality of life, pulmonary function and physical performance of patients. Indications for its implementation are FEV1 е25% of the expected, PaCO2>55 mm Hg. Art. and progressive pulmonary hypertension. Factors limiting the performance of this operation include the problem of selecting a donor lung, postoperative complications and high cost (110–200 thousand US dollars). Operative mortality in foreign clinics is 10–15%, 1–3-year survival rate, respectively, 70–75 and 60%.
Stepwise therapy for stable COPD is shown in the figure.
Treatment of cor pulmonale
Pulmonary hypertension and chronic cor pulmonale are complications of severe and extremely severe COPD. Their treatment involves optimal therapy for COPD, long-term (>15 hours) oxygen therapy, the use of diuretics (in the presence of edema), digoxin (only with atrial fibrillation and concomitant left ventricular heart failure, since cardiac glycosides do not affect contractility and ejection fraction of the right ventricle) . The use of vasodilators (nitrates, calcium antagonists and angiotensin-converting enzyme inhibitors) is controversial. Their use in some cases leads to deterioration of blood oxygenation and arterial hypotension. However, calcium antagonists (nifedipine SR 30–240 mg/day and diltiazem SR 120–720 mg/day) can probably be used in patients with severe pulmonary hypertension when bronchodilators and oxygen therapy are insufficiently effective [16].
Treatment of exacerbations of COPD
Exacerbation of COPD is characterized by an increase in the patient's shortness of breath, cough, change in the volume and nature of sputum and requires changes in treatment tactics. [7]. There are mild, moderate and severe exacerbations of the disease (see Table 3).
Treatment of exacerbations involves the use of medications (bronchodilators, systemic glucocorticoids, and antibiotics if indicated), oxygen therapy, and respiratory support.
The use of bronchodilators involves increasing their doses and frequency of administration. The dosage regimens for these drugs are given in tables 4 and . Administration of $beta;2-adrenergic agonists and short-acting anticholinergics is carried out using compressor nebulizers and metered dose inhalers with a large-volume spacer. Some studies have shown equivalent effectiveness of these delivery systems. However, for moderate and severe exacerbations of COPD, especially in elderly patients, preference should probably be given to nebulizer therapy.
Due to the difficulty of dosing and the large number of potential side effects, the use of short-acting theophyllines in the treatment of exacerbations of COPD is the subject of debate. Some authors admit the possibility of their use as “second-line” drugs if inhaled bronchodilators are insufficiently effective [6, 9], others do not share this point of view [7]. It is likely that the prescription of drugs in this group is possible if the rules of administration are observed and the concentration of theophylline in the blood serum is determined. The most famous of them is the drug aminophylline, which is theophylline (80%) dissolved in ethylenediamine (20%). Its dosage schedule is given in Table 5. It should be emphasized that the drug should be administered only intravenously. This reduces the likelihood of developing side effects. It cannot be administered intramuscularly or by inhalation. The administration of aminophylline is contraindicated in patients receiving long-acting theophyllines due to the risk of overdose.
Systemic glucocorticoids are effective in treating exacerbations of COPD. They shorten recovery time and ensure faster recovery of lung function. They are prescribed simultaneously with bronchodilators when FEV1 <50% of the normal level. Typically, 30–40 mg of prednisolone per os or an equivalent dose intravenously is recommended for 10–14 days. Longer use does not lead to increased effectiveness, but increases the risk of side effects. In recent years, data have emerged on the possibility of using inhaled glucocorticoids (budesonide), administered via nebulizer, in the treatment of exacerbations of COPD as an alternative to systemic steroids [11].
Antibacterial therapy is indicated for patients who have signs of an infectious process (increased amount of sputum, change in the nature of sputum, elevated body temperature, etc.). Its options for various clinical situations are given in Table 6.
The advantages of antibacterial therapy [13] are as follows.
- Reducing the duration of exacerbations of the disease.
- Preventing the need for hospitalization of patients.
- Reducing the period of temporary disability.
- Prevention of pneumonia.
- Prevention of progression of airway damage.
- Increased duration of remission.
In most cases, antibiotics are prescribed by mouth, usually for 7–14 days (with the exception of azithromycin).
Oxygen therapy is usually prescribed for moderate and severe exacerbations of COPD (with PaO2 <55 mm Hg, SaO2 <88%). In these cases, nasal catheters or a Venturi mask are used. To assess the adequacy of oxygenation and PaCO2 levels, blood gas composition should be monitored every 1–2 hours [7]. If the patient's acidosis or hypercapnia persists, artificial ventilation is indicated. The duration of oxygen therapy after stopping an exacerbation in the presence of hypoxemia usually ranges from 1 to 3 months.
If the patient's condition is severe, non-invasive or invasive artificial pulmonary ventilation (ALV) should be performed. They differ in the way the patient and the respirator communicate.
Non-invasive ventilation consists of providing the patient with ventilation support without tracheal intubation. It involves the delivery of oxygen-enriched gas from a respirator through a special mask (nasal or oral-nasal) or mouthpiece. This method of treatment differs from invasive mechanical ventilation in that it reduces the likelihood of mechanical damage to the oral cavity and respiratory tract (bleeding, strictures, etc.), the risk of developing infectious complications (sinusitis, hospital-acquired pneumonia, sepsis), and does not require the administration of sedatives, muscle relaxants and analgesics, which may have an adverse effect on the course of an exacerbation.
The most commonly used non-invasive ventilation mode is positive pressure respiratory support.
It has been established that non-invasive mechanical ventilation reduces mortality, reduces the time of patient stay in hospital and the cost of treatment. It improves pulmonary gas exchange, reduces the severity of shortness of breath and tachycardia.
Indications for non-invasive artificial ventilation [8, 9]:
- severe shortness of breath with the participation of accessory muscles and paradoxical movements of the anterior abdominal wall;
- respiratory rate > 25 per minute;
- acidosis (pH 7.3–7.35) and hypercapnia (PaCO2 - 45–60 mm Hg).
Invasive mechanical ventilation involves intubation of the airway or tracheostomy. Accordingly, the connection between the patient and the respirator is carried out through endotracheal or tracheostomy tubes. This creates a risk of developing mechanical damage and infectious complications. Therefore, invasive mechanical ventilation should be used in severe condition of the patient and only when other treatment methods are ineffective.
Indications for invasive mechanical ventilation [8, 9]:
- severe shortness of breath with the participation of accessory muscles and paradoxical movements of the anterior abdominal wall;
- respiratory rate > 35 per minute;
- severe hypoxemia (pO2< <40 mmHg);
- severe acidosis (pH <7.25) and hypercapnia (PaCO2> 60 mm Hg);
- respiratory arrest, impaired consciousness;
- hypotension, heart rhythm disturbances;
- the presence of complications (pneumonia, pneumothorax, pulmonary embolism, etc.).
Patients with mild exacerbations can be treated on an outpatient basis.
Outpatient treatment of mild exacerbations of COPD [7–9] includes the following steps.
- Assessment of the level of patient education. Checking inhalation technique.
- Prescription of bronchodilators: short-acting β2-adrenergic agonist and/or ipratropium bromide through a metered dose inhaler with a large-volume spacer or through a nebulizer in an on-demand mode. If ineffective, intravenous administration of aminophylline is possible. Discuss the possibility of prescribing long-acting bronchodilators if the patient has not received these drugs previously.
- Prescription of glucocorticoids (doses may vary). Prednisolone 30–40 mg per os for 10–14 days. Discussion of the possibility of prescribing inhaled glucocorticoids (after completion of treatment with systemic steroids).
- Prescribing antibiotics (according to indications).
Patients with moderate exacerbations usually need to be hospitalized. Their treatment is carried out according to the following scheme [7–9].
- Bronchodilators: short-acting β2-agonist and/or ipratropium bromide via a metered-dose inhaler with a large-volume spacer or an on-demand nebulizer. If ineffective, intravenous administration of aminophylline is possible.
- Oxygen therapy (with Sa<<90%).
- Glucocorticoids. Prednisolone 30–40 mg per os for 10–14 days. If oral administration is not possible, an equivalent dose is administered intravenously (up to 14 days). Discuss the possibility of prescribing inhaled glucocorticoids via a metered dose inhaler or nebulizer (after completion of treatment with systemic steroids).
- Antibiotics (according to indications).
Indications for referring patients to specialized departments are [7–9]:
- a significant increase in the severity of symptoms (for example, the occurrence of shortness of breath at rest);
- lack of effect from the treatment;
- the appearance of new symptoms (eg, cyanosis, peripheral edema);
- severe concomitant diseases (pneumonia, heart rhythm disturbances, congestive heart failure, diabetes mellitus, renal and liver failure);
- new occurrence of heart rhythm disturbances;
- elderly and senile age;
- impossibility of providing qualified medical care on an outpatient basis;
- diagnostic difficulties.
The risk of death in a hospital is higher when patients develop respiratory acidosis, have severe concomitant diseases and require ventilation support [9].
With severe exacerbations of COPD, patients are often hospitalized in the intensive care unit; indications for this are:
- severe shortness of breath that cannot be controlled by bronchodilators;
- disturbance of consciousness, coma;
- progressive hypoxemia (PaO2<50 mmHg), hypercapnia (PaCO2>60 mmHg) and/or respiratory acidosis (pH<7.25), despite the use of oxygen therapy and non-invasive ventilation.
Treatment of severe exacerbations of COPD in the emergency department [7–9] involves the following steps.
- Oxygen therapy.
- Ventilation support (non-invasive, less often invasive).
- Bronchodilators. A short-acting β2-agonist and/or ipratropium bromide via a metered-dose inhaler with a large-volume spacer, two puffs every 2–4 hours, or via a nebulizer. If ineffective, intravenous administration of aminophylline is possible.
- Glucocorticoids. Prednisolone 30–40 mg per os for 10–14 days. If oral administration is not possible, use an equivalent dose intravenously (up to 14 days). Discuss the possibility of prescribing inhaled glucocorticoids via a metered dose inhaler or nebulizer (after completion of treatment with systemic steroids).
- Antibiotics (according to indications).
In the next 4-6 weeks, the patient should be re-examined by a doctor, and his adaptation to everyday life, FEV1, correct inhalation technique, understanding of the need for further treatment are assessed, blood gases or oxygen saturation are measured to study the need for long-term oxygen therapy. If it was prescribed only during an exacerbation during hospital treatment, then, as a rule, it should be continued for 1–3 months after discharge.
To prevent exacerbations of COPD, it is necessary to: reduce exposure to risk factors; optimal bronchodilator therapy; inhaled glucocorticoids in combination with long-acting β2-adrenergic agonists (for severe and extremely severe COPD); annual flu vaccination. n
Literature
- Chronic obstructive pulmonary disease. Federal program / Ed. acad. RAMS, Professor A.G. Chuchalin. — 2nd ed., revised. and additional - M., 2004. - 61 p.
- Chuchalin A.G., Sakharova G.M., Novikov Yu.K. Practical guide to the treatment of tobacco addiction. - M., 2001. - 14 p.
- Barnes P. Chronic obstructive pulmonary disease//New Engl J Med. - 2000 - Vol. 343. - N 4. - P. 269–280.
- Barnes P. Management of chronic obstructive pulmonary disease. - Science Press Ltd, 1999. - 80 p.
- Calverley P., Pauwels R., Vestbo J. et al. Combined salmeterol and fluticason in the treatment of chronic obstructive pulmonary disease: a randomized controlled trial // Lancet. - 2003. - Vol 361. -N 9356. - P. 449–456.
- Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care // Thorax. - 2004. - Vol. 59, suppl 1. - P. 1–232.
- Celli BR MacNee W and committee members. Standards for diagnosis and treatment of patients with COPD: a summary of ATS/ERS position paper // Eur Respir J. - 2004. - Vol. 23. - N 6. - P. 932–946.
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. NHLBI/WHO workshop report. — National Heart, Lung, and Blood Institute. Publication number 2701, 2001. - 100 p.
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. NHLBI/WHO workshop report. — National Heart, Lung, and Blood Institute, update 2004 // www.goldcopd.com.
- Loddenkemper R., Gibson G. J., Sibille et al. European Lung White Book. The first comprehensive survey on respiratory health in Europe, 2003. - P. 34–43.
- Maltais F., Ostineli J., Bourbeau J. et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary diseases: a randomized controlled trial // Am J Respir Crit Care Med. - 2002. - Vol. 165. - P. 698–703.
- National Emphysema Treatment Trial Research Group. A randomized trial comparing lung volume reduction surgery with medical therapy for severe emphysema // N Engl J Med. - 2003. - Vol. 348. - N 21. - P. 2059–2073.
- Niederman MS Antibiotic therapy of exacerbation of chronic bronchitis // Seminars Respir Infections. - 2000. - Vol. 15. - N 1. - P. 59–70.
- Szafranski W., Cukier A., Ramiez A. et al. Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease // Eur Respir J. - 2003. - Vol 21. - N 1. - P. 74–81.
- Tierp B., Carter R. Long term oxygen therapy//UpToDate, 2004.
- Widemann HP Cor pulmonale //UpToDate, 2004.
A. V. Emelyanov , Doctor of Medical Sciences, Professor of St. Petersburg State Medical University, St. Petersburg