Adenomyosis is a type of endometriosis, a disease in which the glandular tissue of the uterus (endometrium) grows into the underlying layers of the uterine wall. It usually develops in women of reproductive age, but can also be found in very young girls. During menopause it disappears on its own.
- Causes of adenomyosis
- Classification and forms of the disease
- Symptoms of adenomyosis
- How is adenomyosis diagnosed?
- How is adenomyosis treated?
- Postoperative period
- Pregnancy with adenomyosis
- Complications of adenomyosis
- Prevention
- Forecast
The disease is manifested by heavy menstrual bleeding, pain in the lower abdomen, acyclic bleeding and severe premenstrual syndrome. Also, one of the significant manifestations of adenomyosis is infertility, but a direct connection has not yet been established.
Causes of adenomyosis
As with many diseases, the causes of adenomyosis are not completely clear. Therefore, various theories have been put forward that could explain the emergence and development of pathology. Almost all of them are associated with the following risk factors:
- Hormones. This includes hormonal disorders, taking hormone replacement therapy, and oral contraceptives.
- Motherhood, especially complicated childbirth.
- Surgeries on the uterus - abortions, curettage and even installation of an IUD.
Other risk factors include early and late onset of menstruation, obesity, and immune disorders.
Expert recommendations
It has been proven that being overweight significantly increases the risk of developing adenomyosis. The reason is that in obese women the balance of hormones is shifted. The processes of metabolism and cellular regeneration are disrupted. The endometrium grows and affects muscle tissue. The greatest danger is obesity during menopause: excess weight complicates already complex natural processes.
Therefore, we recommend that our patients love themselves, take care of their bodies, watch their weight and eat right. From a young age, pay attention to your own health, and then adenomyosis during menopause will not be scary for you.
Classification and forms of the disease
Depending on the morphological picture, the following types of adenomyosis are distinguished:
- Focal adenomyosis. In this case, endometrial cells form separate foci in the dividing plate or myometrium.
- Nodular adenomyosis. In this case, endometrioid lesions form nodes (they are also called adenomyomas), which are surrounded by connective tissue and contain cavities inside filled with blood. As a rule, such foci are multiple in nature.
- Diffuse adenomyosis. In this case, endometrial cells are implanted into the underlying tissues without forming clear foci.
- Mixed diffuse-nodular adenomyosis - has features of diffuse and nodular adenomyosis.
Depending on the depth of implantation of endometrioid cells, the following degrees of adenomyosis are distinguished:
- 1st degree - only the submucosal layer of the uterine wall is affected.
- 2nd degree - the muscular layer of the uterine wall is affected, but not more than half its thickness.
- 3rd degree - the muscle layer is affected by more than half.
- Grade 4 - the entire myometrium is affected, and surrounding organs and tissues may be involved in the process.
Definition of disease
In a healthy uterus, the wall is strictly demarcated into layers, there are three in total:
- The muscle layer - the myometrium is sensitive to hormonal effects, especially to prostaglandins and oxytocin. It consists of three layers: the middle circular or vascular (the thickest), the internal longitudinal or submucosal (the thinnest), and the subserosal (outer).
- Serous - in addition to the uterus, the perimeter covers the abdominal cavity, bladder, and rectum.
- The endometrium is the membrane that covers the inside of the uterus. It is she who plays the main role in the development of adenomyosis.
The endometrium consists of two layers:
- deep basal, performing a regenerating function after menstruation
- functional, rejected during menstruation.
If it is not completely excreted with menstrual blood, and its fragments remain in the uterus, growing into its thickness, then adenomyosis occurs. The remaining tissue continues to function as usual, thickening of the uterine wall and other changes appear, and the cycle is disrupted.
What is adenomyosis?
Symptoms of adenomyosis
Symptoms of the disease are very varied, but the two most common manifestations are abnormal uterine bleeding (including menstrual bleeding) and dysmenorrhea (pain during menstruation).
The causes of abnormal menstruation are considered to be an increase in the endometrial surface, increased blood supply to the endometrial lining, abnormal contractions of the uterus and increased secretion of prostaglandins and estrogens.
Menstruation can be very heavy. 2-3 days before they begin and 2-3 days after they end, brown spotting is noted. Some patients may experience spotting of varying intensity outside of menstruation.
The appearance of symptoms of dysmenorrhea is associated with the number of adenomyotic foci, the depth of their invasion, swelling of the endometrium in the thickness of the muscle wall and increased synthesis of prostaglandins. The pain usually begins a few days before menstruation. Their severity is determined by the localization of foci of adenomyosis and the degree of damage to the uterus. The most severe pain occurs when the lesions are located in the area of the pharynx and cervix, and the pain syndrome is severe with multiple lesions. Some patients report pain during sexual intercourse, which intensifies towards the onset of menstruation.
But in many women, adenomyosis can be asymptomatic, which makes diagnosis and timely treatment difficult.
Prices for services
Initial appointment with a gynecologist + ultrasound (assessment of complaints, medical history, examination in a gynecological chair, pelvic ultrasound, consultation)
Primary appointment – visiting a doctor of a specific specialty for the first time. Make an appointment
1800 ₽
Repeated appointment with the gynecologist
With the exception of repeated appointments with doctors: Blatsios N.D., Dzhashiashvili M.D. Make an appointment
1200 ₽
Ultrasound of the pelvis in women (uterine cavity, ovaries)
Make an appointment
1500 ₽
During the first stage of the disease, endometrial cells slightly penetrate into the next layer of the uterus - the myometrium (the muscular layer of the uterus).
The second stage indicates the growth of the endometrium deeper into the muscle tissue of the uterus.
The third stage of the disease is the most unpleasant; endometrioid tissue penetrates into all layers of the uterus, including the serous membrane located on the side of the peritoneum. Unfortunately, this tissue can grow far beyond the uterus and pelvic organs. Foci of endometriosis can be located almost throughout the body, in the abdominal cavity, intestines, in the lungs, bladder, diaphragm, and even in the eyes and during menstruation, and sometimes before and after it begin to bleed, causing severe discomfort, pain, and the development of inflammatory diseases. and as a consequence of adhesive processes in the body. To date, medicine has not found ways to reverse this process and rid the patient of these changes completely and forever; we can only alleviate the symptoms and stop the process of proliferation and further degeneration of cells.
How is adenomyosis diagnosed?
To make a diagnosis of adenomyosis, a comprehensive examination is carried out, including anamnesis, gynecological examination, instrumental and laboratory tests.
It is best to perform a gynecological examination before menstruation, since at this time endometrioid formations “swell” and lead to an increase in the size of the uterus and its shape. With the diffuse type of adenomyosis, the uterus has a spherical shape, and with a widespread process, its size can reach 10-12 weeks of pregnancy. Nodular adenomyosis is manifested by tuberosity of the uterus.
The main method of instrumental research is transvaginal ultrasound. It is also recommended to be performed before the onset of menstruation. Using ultrasound, the size of the uterus is more accurately determined, the thickness of the layers of its wall is visualized, and cystic neoplasms are detected, provided that their size is more than 3 mm.
Does ultrasound detect endometriosis? Answered by ultrasound doctor E.V. Kwaktoon
For diffuse adenomyosis, a more informative research method is hysteroscopy. This diagnostic procedure allows not only to examine the endometrium from the inside, but also to take material for morphological examination, which will allow differential diagnosis with other diseases. The disadvantage of hysteroscopy is its invasiveness, and as a consequence the risks of infectious complications and the need for anesthesia.
Additional diagnostic methods can be laboratory tests, which determine the level of hormones, inflammatory markers and other indicators.
Expert advice
If a woman with endometriosis cannot become pregnant for a long time, in vitro fertilization is performed. The doctor should be aware of the presence of endometrial proliferation and the prevalence of endometriotic formations. The chance of getting pregnant using in vitro fertilization is higher if the disease is at stages 1-2. If the IVF procedure was successful, the pregnant woman should be under the supervision of a specialist throughout the entire gestation period.
To avoid risks to the patient's health, the obstetrician may decide to prohibit natural childbirth. A cesarean section is discussed taking into account possible contraindications, sensitivity to the drugs used, and the condition of the child.
Bani Odekh Elena Yurievna
Obstetrician-gynecologist, gynecologist-endocrinologist, ultrasound diagnostics doctor, Candidate of Medical Sciences Experience 23 years
How is adenomyosis treated?
Historically, the diagnosis of adenomyosis involved removal of the uterus. However, this method of treatment is not suitable for women who would like to preserve fertility or for patients for whom surgery cannot be performed due to the presence of concomitant pathologies. Therefore, adenomyosis is currently treated both surgically and with medication. The choice of treatment tactics is determined depending on the symptoms of the pathology, the presence of concomitant gynecological diseases, the patient’s age and her desire to preserve reproductive function.
Conservative treatment of adenomyosis
The cornerstone in the conservative treatment of adenomyosis is hormone therapy. There are 4 groups of drugs that can be used here:
- Estrogen-gestagen drugs. They are used for initial types of adenomyosis.
- Gestagens. They can treat adenomyosis of any type. The essence of the action is to suppress the production of estrogen and ovulation.
- Antigonadotropic drugs. They suppress the synthesis of gonadotropins in the hypothalamic-pituitary system. Prescribed in courses over several months to patients with hyperandrogenic status.
- Gonadotropic releasing hormone agonists. The advantage of these drugs is that they need to be taken once a month and have no significant side effects.
In addition to hormonal treatment, antispasmodics, analgesics and anti-inflammatory drugs are used.
Surgical treatment of adenomyosis
As we have already said, historically adenomyosis involved removal of the uterus. But nowadays, the possibilities of surgical treatment have expanded and organ-preserving treatment has become possible.
Radical operations include:
- Panhysterectomy.
- Hysterectomy.
- Supravaginal amputation of the uterus.
Indications for radial operations are:
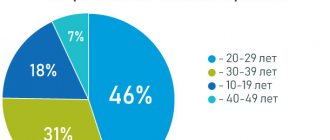
- Progression of the disease in patients over 40-45 years of age.
- Adenomyosis grade 3.
- Adenomyosis in combination with fibroids.
- Threat of malignant transformation of lesions.
- Lack of effect from conservative therapy and organ-preserving surgical methods of treatment.
In most cases, organ-preserving treatment is performed, which involves removing pathologically changed lesions and preserving reproductive function.
All methods of organ-preserving operations for adenomyosis are divided into the following groups, depending on the trauma to the healthy myometrium:
- Complete removal of adenomyotic lesions. These include adenomyometomy (nodular adenomyosis is removed) and cystectomy (used for cystic forms of the disease).
- Partial adenomyomectomy - involves incomplete, cytoreductive removal of the pathological focus. Such operations are performed for diffuse forms of adenomyosis. According to clinical studies, it alleviates dysmenorrhea in 81.8% of patients, menorrhagia in half of patients and allows approximately 47% of patients to become pregnant.
- Non-incisional methods. In this case, pathological foci are removed not surgically, but, for example, using ablation or electrocoagulation.
In general, organ-preserving treatment is more effective for focal forms of adenomyosis. For diffuse forms, its implementation presents difficulties associated with functional and anatomical features:
- Infiltrative growth.
- Damage to all layers of the uterine wall or all parts of the uterus.
- Lack of a demarcation line between pathological foci and healthy endometrium.
In general, recent developments in the surgical treatment of adenomyosis can effectively eliminate painful symptoms, improve the quality of life of patients and restore their reproductive health.
Treatment
Treatment approaches for adenomyosis depend on the severity of dysmenorrhea and menorrhagia. Patients with minimal symptoms near menopause can receive symptomatic treatment with non-steroidal anti-inflammatory drugs, analgesics, cyclic or continuous oral contraceptives, and progestins. For symptomatic alenomyosis, GnRH agonists can be used.
But severe, symptomatic adenomyosis usually does not respond to hormonal therapy (the basal layer of the endometrium is resistant to hormonal stimuli). So, the definitive treatment for adenomyosis can only be hysterectomy (vaginal, laparoscopic or abdominal). An important medical option before surgical treatment is to perform an endometrial biopsy (to exclude concomitant endometrial cancer) and a differential diagnosis with uterine fibroids. Thus, a surgeon may intend to perform a conservative myomectomy with a preliminary diagnosis of uterine fibroids, but if diffuse enlargement of the uterus is detected during surgery, he will be forced to perform a hysterectomy.
Postoperative period
Features of the postoperative period depend on the volume of intervention and the method of its implementation. The easiest way for patients to tolerate laparoscopic or hysteroscopic organ-preserving operations. The pain syndrome in the postoperative period is moderate, activation is possible already on the first day if there are no contraindications from the anesthesiologist.
In the first few weeks, bloody discharge from the genital tract is characteristic, which gradually decreases. During this time, it is recommended to avoid excessive physical activity and sexual activity.
In general, most patients feel satisfactory after surgery and even note an improvement in their quality of life, as pain during menstruation decreases, PMS is easier and the amount of bleeding decreases.
Prevention
To reduce the likelihood of developing uterine adenomyosis, you need to engage in prevention. Following the recommendations is useful for everyone who is at risk: patients over 30 years old, with reduced immunity and hormonal imbalances.
The main preventive measure is regular visits to the gynecologist. You should consult a doctor at least once every 6-12 months, even in the absence of alarming symptoms. This will allow us to identify most possible pathologies at an early stage, when they can be treated much faster and easier.
Moderate physical activity is required. It is believed that both severe overexertion and lack of physical activity are harmful to the female body. After training, a woman should feel slightly tired, but not exhausted. It is useful to lead an active lifestyle: spend more time in nature, walk in the fresh air, take an afternoon promenade.
The psycho-emotional state has a serious impact on health. If possible, it is necessary to avoid severe stress, nervous tension, quarrels and scandals. If there are signs of depression or other disorders, you should seek psychotherapeutic help.
It is useful to learn various relaxation techniques. Choose your option: yoga classes, swimming in the pool or a relaxing massage. This will help relieve physical and psycho-emotional stress.
To prevent various diseases of the reproductive system, you need to avoid solariums. A natural tan should be obtained during safe hours using sunscreen. A long stay on the beach can negatively affect the state of the hormonal system.
Follow the rules of personal hygiene. The state of the reproductive system largely depends on this factor, since the environment of the genital organs is highly sensitive to pathogenic microorganisms. You should exclude casual sex and use barrier contraception, even if you are confident in your partner.
You should not self-medicate. Even herbal medicine and folk recipes for medicinal preparations can affect the state of health, aggravate or provoke the development of diseases. To select a herbal complex, you need to contact a specialist.
Prevention of adenomyosis is largely nonspecific: it is aimed at strengthening the general condition of the body and strengthening its natural defense mechanisms.
Pregnancy with adenomyosis
Approximately one third of patients with adenomyosis experience infertility. There is no consensus on why this happens, but there are a number of factors that prevent the normal, natural occurrence of pregnancy in the presence of adenomyosis:
- Hormonal disorders that interfere with normal ovulation.
- Increased myometrial contractility, which prevents implantation of the fertilized egg.
- Inflammatory processes in the uterine cavity.
- Violation of the structure of the endometrium.
- The presence of adhesions in the uterine area.
- Violation of the transport function of the fallopian tubes.
- Often adenomyosis occurs against the background of another gynecological pathology, for example, fibroids.
In such patients, there is an increased risk of spontaneous abortion and even multiple miscarriages. In general, the possibility of pregnancy depends on the degree of damage to the uterus and the presence of other genital pathologies. You should plan to conceive no earlier than six months after the end of conservative therapy or endoscopic surgery. In this case, in the first trimester of pregnancy, hormonal support with gestagens is prescribed.
It is worth noting that while carrying a child, many patients experience regression of adenomyosis, since pregnancy is a “physiological menopause,” during which deep hormonal changes occur that have a beneficial effect on this disease.
Diagnostics
A preliminary diagnosis of adenomyosis is made based on medical history, characteristic complaints and gynecological examination. Pathology is indicated by palpation of a spherical or tuberous enlarged uterus, polymenorrhea, pain and signs of anemia. The diagnosis is confirmed by instrumental examination methods:
- Ultrasound of the pelvic organs. It is advisable to perform it at the end of the menstrual cycle with a vaginal sensor. Echo signs: the size of the uterus is larger than normal, the thickness of the walls is uneven, the echogenicity of the myometrium is increased, the presence of a “honeycomb” symptom: dense areas alternate with small cystic inclusions, the presence of passages from the endometrium into the thickness of the organ. Adenomyotic nodes are visualized as rounded areas of increased echogenicity without clear contours and capsules.
- Hysterography. The introduction of X-ray contrast into the uterine cavity makes it possible to identify its enlargement, deformation and jagged edges of the contour in the photographs.
- Hysteroscopy. Allows you to confirm adenomyosis and determine its degree. Grade 1 is characterized by unchanged wall relief and the presence of endometriotic ducts (dark bluish “eyes” or open bleeding wounds). For degree 2 – unevenness of the uterine walls, poor distensibility of the uterine cavity, the presence of endometriotic ducts. For grade 3 - bulging into the uterine cavity without clear contours, rigidity of its walls, open/closed passages.
- MRI. An increase in the size of the uterus, thickening of its walls, disrupted myometrial structure, endometriotic ducts.
- Curettage of the uterine cavity and cervical canal. Performed after hysteroscopy, histological examination of the scraping allows one to confirm the presence of endometrioid heterotopias, exclude/confirm hyperplasia, and endometrial cancer.
Laboratory tests include CBC (confirms anemia), TAM, blood test for sex hormones and tumor marker CA-125 (with endometriosis its level increases).
Differential diagnosis
Adenomyosis is differentiated with the following pathologies:
- Uterine fibroids. The combination with adenomyosis reaches 85%. The symptoms of uterine fibroids and uterine endometriosis are similar. With small fibroids, pain syndrome is usually absent; menstrual cycle disorders are more common when the node is located submucosally. A gynecological examination reveals an enlarged, dense uterus with nodes, palpation is painless, and mobility is preserved. With adenomyosis, the mobility of the organ is limited, there is pain on palpation and a connection between the size of the uterus and the phase of the cycle. The final diagnosis is confirmed by instrumental research methods.
- Hyperplastic processes of the endometrium (hyperplasia, polyp). Pain, as a rule, is absent; cycle disorders are noted in the form of prolongation of menstruation and an increase in the volume of blood loss and intermenstrual discharge. Pre- and postmenstrual discharge is not typical for endometrial polyp/hyperplasia. On ultrasound: the increase in the thickness of the M-echo is diffuse (hyperplasia) or focal (polyp/polyposis), the contours of the uterus are smooth, the dimensions are normal.
- Endometrial cancer. It is characterized by the occurrence of acyclic uterine bleeding and spotting, which is often accompanied by an unpleasant odor and discharge of pus. In the absence of bloody discharge, there is profuse, watery leucorrhoea, sometimes mixed with blood the color of “meat slop.” Pain occurs at an advanced stage and is not associated with the phase of the cycle. The diagnosis is confirmed by ultrasound, hysteroscopy, hysterography, and curettage of the uterine cavity.
Complications of adenomyosis
The most common complication of adenomyosis is anemia. It develops due to heavy menstrual bleeding and is accompanied by pale skin, weakness, dizziness, fatigue and even fainting.
Severe pain, severe PMS, and prolonged menstruation can lead to a decrease in psychological stability and the development of neuroses or depression. In such situations, patients are advised to undergo psychological counseling and, if necessary, drug treatment.
Forecast
Adenomyosis is a chronic disease prone to relapsing. The return of the disease is diagnosed in approximately every fifth fertile patient after conservative therapy or organ-saving surgery. In this regard, gynecologists can prescribe hormonal contraceptives for prevention.
In premenopausal patients, the disease is milder and during menopause it completely disappears.
Book a consultation 24 hours a day
+7+7+78
Sources
- Clinical guidelines – Endometriosis – 2022 – Approved by the Ministry of Health of the Russian Federation.
- Unanyan A.L., Sidorova I.S., Kogan E.A. Active and inactive adenomyosis: clinical and morphological development options, differentiated approach to therapy. Scientific article – Journal of Obstetrics, Gynecology and Reproduction, 2012.
- Linde V.A., Reznik M.V., Tarasenkova V.A. Sadikhova E.E. Modern ideas about adenomyosis. Scientific article - Bulletin of the Ivanovo Medical Academy, 2022.
Share: