Aneurysm and aortic dissection
Symptoms of aneurysm and aortic dissection
Aortic aneurysms, which appear as a result of congenital, hereditary or transferred pathology and are not associated with dissection of the vascular wall, in most cases do not have obvious clinical signs and represent an incidental finding.
Large aneurysms may be accompanied by a feeling of fullness, dull pain in the back, and symptoms of compression of neighboring organs may occur.
A dissecting aortic aneurysm has a more vivid and characteristic clinical picture. When the internal aortic wall is torn, sharp pain occurs in the chest, back or lower back (depending on the location of the damage). This pain is short-lived, but can cause a reflex drop in blood pressure and fainting.
After some time, the patient begins to experience burning pain in the chest spreading to the arms, neck, under the shoulder blades, this pain cannot be relieved by nitroglycerin, a dry cough appears, a feeling of lack of oxygen, blood pressure drops, and collapse occurs.
If the dissection occurs in the lower parts of the aorta, then pain is noted in the lower back with irradiation to the pelvis and legs. If the dissection affects the mouth of the branches extending from the aorta, symptoms of circulatory disorders in the corresponding organs are observed.
Typically, at this stage, patients are hospitalized and undergo emergency surgery.
In case of complete rupture of the aortic wall, massive bleeding and terminal shock occurs. Unfortunately, more than 90% of such patients die.
Diagnostics
Initial aortic dissection can be determined using transthoracic or transesophageal echocardiography.
One of the most reliable methods for diagnosing the entire aorta is aortography. This method allows you to see in real time defects in the aortic walls, the secondary lumen and aneurysm cavity formed as a result of dissection. If the site of the tear is closed by a blood clot, then aortography may give a false negative result.
This deficiency can be corrected by performing a vascular contrast-enhanced computed tomography scan, which can be performed at K+31.
Treatment of aneurysm and aortic dissection
For a small aneurysm that does not bother the patient, it is enough to observe. Large aneurysms are subject to planned removal followed by aortic repair .
In the case of a dissecting aortic aneurysm, the patient is given morphine for pain relief to prevent painful shock and emergency surgical treatment is performed, which usually consists of excision of the affected area of the aorta and installation of a synthetic vascular prosthesis in its place.
After such severe operations, the K+31 Clinic helps you undergo a course of rehabilitation treatment. We keep health in focus and offer patients our active participation in the prevention of recurrent aortic dissection and the occurrence of aneurysms.
Diagnostic measures
Symptoms are not enough to make an accurate diagnosis, as they often mimic symptoms of other diseases. The doctor will prescribe a full examination, which includes:
- ultrasound examination - allows you to study all parts of the vessel, you can detect dissection of the aortic arch on ultrasound;
- chest x-ray – necessary for differential diagnosis of aortic dissection with other pathologies of the chest organs (for example, tuberculosis);
- ECG for thoracic aortic dissection – allows to exclude myocardial infarction;
- aortography is an x-ray examination of the aorta filled with a contrast agent.
The most informative will be the diagnosis of aortic dissection using CT, because it allows not only to confirm the presence of pathology, but also to assess its prevalence and the depth of the dissection.
Treatment methods
This pathology requires immediate emergency medical care already at the diagnostic stage, followed by transfer of the patient to the intensive care unit. The intensive care protocol contains the following algorithm:
- pain relief – narcotic analgesics (morphine);
- pressure correction (dopamine, mesaton for collapse, sodium nitroprusside for elevated);
- infusion therapy to maintain blood volume and kidney function;
- oxygen therapy.
Further treatment of aortic dissection is usually surgical; conservative therapy is indicated only in cases of mild chronic forms.
The operation consists of eliminating the false channel and suturing or prosthesizing the walls of the vessel. If necessary, aortic valve repair is performed. There are two options - open heart intervention and endovascular technique. Anticoagulants and glucocorticoids are used to prevent complications.
In the future, the patient requires long-term rehabilitation and dynamic observation.
Maintenance drug therapy is prescribed - cardiotonics, antihypertensive and antisclerotic drugs.
The following recommendations reduce the risk of relapse:
- moderate physical activity;
- rejection of bad habits;
- avoiding junk food;
- physiotherapeutic procedures.
conclusions
Dissecting aortic aneurysm is a dangerous cardiovascular disease, which in most cases is fatal and requires immediate medical attention.
The prognosis is very disappointing - without treatment, about 70% of patients die in the first day, and within a month - 90%. Operative mortality is 10%, and in the first 5 years after surgery, about 40% die. This disease is easier to prevent than to treat.
The following sources of information were used to prepare the material.
Causes of aortic enlargement
Congenital systemic connective tissue diseases: Marfan syndrome, Ehlers-Danlos syndrome, caused by genetic changes in which the aortic wall has an abnormal structure, can cause the development of an aneurysm.
Acquired diseases that cause aneurysmal changes in the aortic wall: most often this is atherosclerosis. About 80% of all complicated aortic aneurysms are aneurysms caused by an atherosclerotic process, which leads to weakening of the vessel wall and the inability to withstand normal blood pressure, and as a result, to its expansion.
Less commonly, an aortic aneurysm develops in inflammatory diseases caused by external agents (syphilis, fungal infection, tuberculosis) or in autoimmune diseases (nonspecific aortoarteritis).
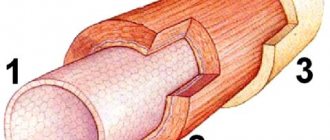
How this happens: pathophysiology of the process
Typically, delamination occurs at the site of the damaged area of the inner wall. Most often, there is already an aneurysm there - an expansion of the lumen of the aorta. Naturally, the inner wall of the vessel is significantly thinned. Another important factor is high blood pressure (especially during a hypertensive crisis). In this case, under strong pressure, the damaged intima ruptures.
Blood then enters the muscle layer and pushes the fibers apart, spreading proximally and distally from the rupture site. This creates a so-called false flow. In some cases, it may stop in places where healthy tissue is located. If the aorta is affected over a significant area, the process spreads further, spreading to other arteries, which significantly worsens hemodynamics. In some cases, the protrusion formed due to false flow leads to the closure of the lumen of the outgoing arteries.
In cases where the outer wall also ruptures, massive internal bleeding occurs, which in 90% of cases leads to death.
Types of open surgical operations for aortic aneurysms:
- Bentalla-De Bono operation (replacement of the ascending aorta with a valve-containing conduit with a mechanical prosthetic aortic valve);
- David's operation (replacement of the ascending aorta while preserving the native aortic valve);
- Supracoronary aortic replacement;
- Prosthetics of the ascending aorta and its arch (Borst technique, the use of oblique aggressive anastomosis and other techniques);
- Thoracic aortic replacement;
- Abdominal aortic replacement.
Diagnosis of aortic aneurysm
In the diagnosis of aortic aneurysms, the so-called imaging techniques (ultrasound, MRI, CT, AG) are of greatest importance. In the ascending aorta, its arch and in the abdominal section, an aneurysm can be detected using ultrasound methods (ultrasound). To diagnose an aneurysm of the descending (thoracic) aorta, X-ray methods (x-ray, computed tomography) are required. To establish a final diagnosis and select a treatment method, contrast research methods are performed. Currently, the optimal diagnostic method, which provides the most complete information about the location, extent, diameter of the aneurysm and its relationship to nearby organs, is multislice computed tomography - aortography.
Endovascular interventions
They allow you to dramatically reduce the amount of surgical trauma, shorten hospitalization periods and reduce the inevitable suffering of the patient associated with surgical approaches. One of the main disadvantages of the method is the need for repeated interventions.
Types of endovascular operations for aortic aneurysm:
- implantation of a stent graft into the abdominal aorta,
- implantation of a stent graft into the ascending (thoracic) aorta.
The most modern method of treating aortic aneurysm is a hybrid method, which allows achieving optimal treatment results with the least surgical trauma.
Hybrid surgeries combine the advantages of open and endovascular interventions.
To prevent the development of aortic aneurysms, the most important thing is the need to control risk factors, namely arterial hypertension. In addition to arterial hypertension, the most significant risk factors are age (over 55 years), male gender, smoking, the presence of aneurysms in direct relatives, and high cholesterol levels.
Symptoms of aortic aneurysm
Unfortunately, the diagnosis of aortic aneurysm cannot always be established during the “cold period” (before complications develop), since this disease is usually asymptomatic. Most often, it is discovered accidentally during fluorography, ultrasound or tomography studies performed in connection with other diseases. Treatment of an aneurysm of the ascending aorta before complications develop is much safer for the patient, therefore, in the early diagnosis of an aortic aneurysm, routine medical examination is important.
It is worth noting that every hundredth patient who died suddenly dies from aortic dissection.
Complaints usually appear when the aneurysm begins to stratify or, enlarging, compresses surrounding organs and tissues. Pain or dysfunction of those organs located in the area of the aneurysm appears. At first, this is not of a bright nature and, therefore, does not alarm either the patient or the doctor.
However, the pain intensifies as these deadly complications of an aortic aneurysm develop—it is some of the most severe pain a person can experience. It is localized in the chest if the aneurysm is located in the ascending, descending sections or in its arch, or in the abdomen if it formed in the abdominal section. Characterized by severe weakness, pallor, and often the person loses consciousness.
Impaired blood supply to organs located in the area of aneurysm rupture or aortic dissection (brain or spinal cord, kidneys, intestines, upper or lower extremities) leads to loss of function of these organs, and a large volume of blood loss during aortic rupture represents the most serious danger. To save a life, minutes count. If early surgical treatment is not available, the first-day mortality rate for aortic dissection is 1% per hour (one person in a hundred dies every hour). Within the first 24 hours, 33% of patients die from aortic dissection, 50% of patients within 48 hours and 75% within two weeks. Only early surgical intervention makes it possible to save a significant proportion of patients.