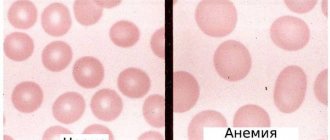
While carrying a child, the female body needs a large amount of useful substances that participate in the processes that occur during pregnancy and ensure the growth and development of the fetus. One of the most important microelements is iron. Unfortunately, 40% of pregnant women develop iron deficiency - this condition is called iron deficiency anemia. It is caused by a decrease in the level of hemoglobin, a complex iron-containing protein that binds oxygen and delivers it to tissues and organs. As a result of anemia, cells do not receive enough oxygen, which is dangerous for the health of both the woman and the child.
Why does iron deficiency occur during pregnancy, what are its signs and consequences?
Causes of iron deficiency in the female body during pregnancy
During the period of bearing a child, the volume of blood in the female body increases by 50%. At the same time, the amount of fluid increases, causing the blood to “thin out.” Therefore, a decrease in hemoglobin levels is natural: the lower limit of hemoglobin in the blood of pregnant women is set at 110 g/l. For comparison: the norm for non-pregnant women is from 120 to 140 g/l. It is worth considering that women often enter pregnancy with a deficient or borderline level of iron in the blood. Iron levels may be low due to heavy menstruation lasting more than 5 days, poor nutrition, problems with the gastrointestinal tract, in which this trace element cannot be fully absorbed in the body.
Iron deficiency anemia during pregnancy is indicated when the hemoglobin level drops below 110 g/l. There are three degrees of anemia:
- Mild severity (hemoglobin level - from 90 to 110 g/l).
- Moderately expressed (from 70 to 89 g/l).
- Heavy (from 40 to 69 g/l).
Treatment and prevention of anemia
If iron deficiency anemia is detected in a pregnant woman, the doctor prescribes a course of multivitamins with iron, or, less commonly, individual iron supplements. In addition, if you have anemia, it is recommended to follow a diet that involves consuming enough foods containing iron.
This group includes:
- red meat, liver;
- pomegranate and tomato juice;
- prunes, nuts;
- buckwheat, legumes, dried apricots, potatoes.
All of these foods contain iron, which is easily absorbed. It is worth noting that iron is better absorbed from animal products, so it is recommended to give preference to them when following a diet. To prevent anemia, gynecologists managing pregnancy prescribe iron supplements and vitamin complexes at the stage of pregnancy planning. In addition, it is recommended to consume large amounts of citrus fruits, since vitamin C supports the absorption of iron, while calcium, on the contrary, inhibits its absorption.
It is recommended to take iron supplements in the morning with water or orange juice. It is better to avoid tea and coffee, since the polyphenols contained in these drinks also interfere with the absorption of iron.
Symptoms of anemia during pregnancy
With iron deficiency during pregnancy, the following symptoms are observed:
- Constant weakness, possible fainting.
- Dizziness.
- Pale, dry, flaky skin.
- Pale mucous membranes (lips, eyelids, etc.).
- Depressed mood, irritability, drowsiness.
- Tachycardia (heart beats quickly - more than 90 beats per minute).
- Brittle nails with white spots.
- Brittle, dull hair with split ends.
- Non-standard taste preferences (for example, when you want to eat chalk or sand).
If the hemoglobin level decreases gradually, then the expectant mother may feel well for a long time, although the problem still exists. Therefore, it is important to regularly take all the tests prescribed during pregnancy. Anemia will be detected by a complete blood test.
Anemia: what is it?
Blood anemia during pregnancy (gestational) is a disorder in which hemoglobin decreases. It is designated in analyzes as Hb. Hemoglobin is a protein found in red blood cells (erythrocytes). The function is to bind with oxygen and deliver it to organs and tissues. In the capillaries of the lungs, hemoglobin binds with oxygen. The red blood cells are then distributed throughout the body through the bloodstream. After this, oxygen is freed from its connection with hemoglobin and enters the tissues, where it is spent on oxidative processes. Free hemoglobin picks up carbon dioxide in the tissues and “carries” it to the lungs.
When the concentration of hemoglobin decreases, the function of providing the body with oxygen and removing carbon dioxide is also disrupted.
What are the dangers of iron deficiency during pregnancy?
Anemia increases the risk of pregnancy complications. Women with iron deficiency are more likely to experience toxicosis. In 40% of pregnant women with anemia, gestosis is diagnosed, in which blood pressure rises, swelling appears, and protein is found in the urine. 15–42% of women with anemia experience miscarriages and labor begins prematurely.
Acute iron deficiency can lead to serious consequences:
- Premature birth.
- Weak labor.
- Premature placental abruption.
- Intrauterine growth retardation and fetal development.
- Bleeding after childbirth.
- Increased risk of inflammation after childbirth.
- Reduced milk supply during breastfeeding.
Children whose mothers experienced iron deficiency during pregnancy also often develop anemia by the first year of life. In addition, such babies are more susceptible to viral diseases. The fact is that iron is required for the proper formation of the immune system. If there was little iron during intrauterine development, then the child’s immunity will be weak.
G.N. Gorokhovskaya, Yu.O. Zimaeva, O.V. Yuzhaninova, M.M. Petina, V.I. Biryukov
Department of Hospital Therapy No. 1 MGMSU, Moscow
Iron deficiency anemia is one of the most common human diseases, affecting about 25% of the world's population. Anemia in pregnant women in at least 90% of cases is iron deficiency anemia. There is a relationship between the frequency of detection of iron deficiency anemia in pregnant women and the level of socio-economic development of the region. In general, the number of pregnant women with this pathology reaches 43.9 million people or 51% of the total number of pregnant women [7]. There are anemia observed before pregnancy and anemia diagnosed during gestation. Pregestational iron deficiency anemia negatively affects pregnancy, contributing to the threat of miscarriage, miscarriage, weakness of labor, postpartum hemorrhage and infectious complications. Anemia caused by pregnancy refers to a number of anemic conditions that occur during pregnancy, complicate its course and usually disappear soon after childbirth or termination of pregnancy. In the second half of pregnancy, anemia is diagnosed almost 40 times more often than in the first weeks. These are primarily the hormonal changes inherent in pregnancy: an increase in the production of estrogens, glucocorticoids, as well as immunological mechanisms. In practical work, such differentiation of iron deficiency anemia is not necessary, since the severity of the disease, clinical picture, frequency and severity of pregnancy complications are determined primarily by the severity of anemia, and not by the time of its onset. As for treatment, it is the same in both cases. The first report of anemia in pregnant women belongs to G. Andral, 1843. In 1823, he observed and described the condition of a pregnant woman who was anemic and died during childbirth. However, even after more than 180 years, there are many challenges in diagnosing and treating this condition. The high prevalence of anemia in pregnant women, and the adverse consequences for the pregnant woman and the fetus that they can lead to, make this problem extremely urgent and require improvement of the modern system of maternal and child health care. The presence of iron deficiency anemia leads to a disruption in the quality of life of patients, reduces their performance, and causes functional disorders in many organs and systems. Iron deficiency in pregnant women increases the risk of complications during childbirth, and in the absence of timely and adequate treatment, iron deficiency may also occur in the fetus.
Etiology and pathogenesis Food is a natural source of iron. A woman consumes 10-20 mg of iron daily with food, of which no more than 2 mg is absorbed. Up to 75% of healthy women lose 20-30 mg of iron during menstruation. This amount of iron cannot be absorbed even with a high content of it in food. An imbalance occurs, leading to the development of anemia [6]. The main part of iron (65%) is in hemoglobin, less in myoglobin (3.5%), a small but functionally important amount in tissue enzymes (0.5%), plasma (0.1%), the rest in the depot (liver , spleen, etc.) – 31%. The average iron content in the human body is 4.5-5 g. A reduction in iron reserves in the body affects not only the amount of hemoglobin. The role of iron in metabolism is much broader. Iron takes part in collagen synthesis, porphyrin metabolism, terminal oxidation and oxidative phosphorylation in cells, and the functioning of the immunocompetent system. The biological significance of iron is determined by its participation in tissue respiration. In this regard, iron deficiency anemia in pregnant women is characterized by tissue hypoxia and the pathology caused by it. With iron deficiency in pregnant women, progressive hemic hypoxia occurs with the subsequent development of secondary metabolic disorders [11]. Pregnancy predisposes to the occurrence of iron deficiency, since during this period there is an increased consumption of iron, necessary for the development of the fetus, associated with hormonal changes, the development of early toxicosis, which prevents the absorption in the gastrointestinal tract of iron, magnesium, phosphorus, necessary for hematopoiesis. During gestation, iron is intensively consumed due to intensified metabolism: in the first trimester, the need for it does not exceed the need before pregnancy and is 0.6-0.8 mg/day; in the second trimester it increases to 2-4 mg; in the third trimester it increases to 10-12 mg/day. Over the entire gestational period, 500 mg of iron is consumed for hematopoiesis, of which 280-290 mg is consumed for the needs of the fetus, and 25-100 mg for the placenta. By the end of pregnancy, iron depletion inevitably occurs in the mother's body due to its deposition in the fetoplacental complex (about 450 mg), an increase in the volume of circulating blood (about 500 mg) and in the postpartum period due to physiological blood loss in the third stage of labor (150 mg) and lactation (400 mg). The total loss of iron by the end of pregnancy and lactation is 1200-1400 mg. The process of iron absorption during pregnancy increases and amounts to 0.6-0.8 mg/day in the first trimester, 2.8-3 mg/day in the second trimester, and up to 3.5-4 mg/day in the third trimester. However, this does not compensate for the increased consumption of the element, especially during the period when bone marrow hematopoiesis of the fetus begins (16-20 weeks of pregnancy) and the blood mass in the maternal body increases. Moreover, the level of deposited iron in 100% of pregnant women decreases by the end of the gestational period. It takes at least 2-3 years to restore iron reserves lost during pregnancy, childbirth and lactation. Latent iron deficiency is detected in 20-25% of women. In the third trimester of pregnancy, it is detected in almost 90% of women and persists after childbirth and lactation in 55% of them. In the second half of pregnancy, anemia is diagnosed almost 40 times more often than in the first weeks, which is undoubtedly associated with impaired hematopoiesis due to changes caused by gestation [2, 4, 17]. Inappropriately low production of erythropoietin (EPO) is one of the most important pathogenetic mechanisms for the development of anemia in pregnant women. Excessive production of pro-inflammatory cytokines and, above all, TNF-α plays a role in suppressing the production of endogenous EPO, which can have several causes, the most important of which is latent infections (primarily urogenital). It was found that the placenta under hypoxic conditions is capable of producing proinflammatory cytokines in large quantities [9, 10, 13, 17]. In addition to states of overproduction of proinflammatory cytokines caused by pregnancy itself, their overproduction is possible with concomitant chronic diseases (chronic infections, rheumatoid arthritis, etc.), which can lead to anemia of chronic diseases. Starting from the 28-30th week of physiological pregnancy, there is an uneven increase in the volume of circulating blood plasma and the volume of erythrocytes [9]. Of interest are some indicators (Table 1) of peripheral blood depending on the duration of pregnancy [9]. Bleeding during pathological pregnancy can also cause the development of anemia in pregnant women, for example, repeated bleeding with placenta previa. It is important to take into account pre-pregnancy diseases that often lead to bleeding - uterine fibroids, endometriosis; Heavy and prolonged menstruation also causes significant losses - from 50 to 200 mg of iron. It is also necessary to take into account hidden bleeding from the gastrointestinal tract (peptic ulcer, hemorrhoids, etc.). Repeated bleeding disrupts the balance between iron intake and excretion and leads to the development of iron deficiency [9, 13]. Factors contributing to the development of iron deficiency anemia:
1. Reduced intake of iron into the body from food (vegetarian diet, anorexia). 2. Chronic diseases of internal organs. Particular attention should be paid to gastrointestinal bleeding. 3. The presence of diseases manifested by chronic nosebleeds (thrombocytopathies, thrombocytopenic purpura). 4. Gynecological diseases accompanied by heavy menstruation or uterine bleeding, endometriosis, uterine fibroids. 5. Complicated obstetric history: multiparous women; history of spontaneous miscarriages; Bleeding in previous births contributes to the depletion of iron stores in the body. 6. Complicated course of this pregnancy: multiple pregnancy; early toxicosis; young age of the pregnant woman (under 17 years); primigravidas over 30 years of age; arterial hypotension; exacerbation of chronic infectious diseases during pregnancy; gestosis; placenta previa; premature placental abruption [9].
Pregnancy is contraindicated in the following forms of diseases of the blood and hematopoietic system: chronic iron deficiency anemia of III-IY degree; hemolytic anemia; bone marrow hypo- and aplasia; leukemia; Werlhof's disease with frequent exacerbations. If pregnancy occurs due to these diseases, it is advisable to terminate the pregnancy before 12 weeks. Some researchers consider iron deficiency anemia as a total pathology, leading to functional and morphological changes in all organs and tissues. Constantly regenerating tissues are especially severely damaged: the epithelium of the skin, respiratory tract, gastrointestinal tract, as well as the immune system and brain [11].
Clinic Clinical symptoms of iron deficiency anemia usually appear with moderate severity of anemia. In mild cases, the pregnant woman usually does not make any complaints, and only laboratory indicators serve as objective signs of anemia. The clinical picture of iron deficiency anemia consists of general symptoms caused by hemic hypoxia (general anemic syndrome) and signs of tissue iron deficiency (sideropenic syndrome). General anemic syndrome is manifested by pallor of the skin and mucous membranes, weakness, increased fatigue, dizziness, headaches (usually in the evening), shortness of breath during exercise, a feeling of palpitations, fainting, flashing “flies” before the eyes with a low level of anemia in pregnant women. Often a pregnant woman suffers from drowsiness during the day and complains of poor sleep at night, irritability, nervousness, tearfulness, decreased memory and attention, and loss of appetite. Sideropenic syndrome includes the following:
• Changes in the skin and its appendages (dryness, peeling, slight cracking, pallor). Hair is dull, brittle, splits, turns gray early, and falls out rapidly. In 20-25% of patients, changes in the nails are observed: thinning, brittleness, transverse striations, sometimes spoon-shaped concavity (koilonychia). • Changes in the mucous membranes (glossitis with atrophy of the papillae, cracks in the corners of the mouth, angular stomatitis). • Damage to the gastrointestinal tract (atrophic gastritis, atrophy of the esophageal mucosa, dysphagia). • Predilection for unusual odors (gasoline, kerosene, acetone). • Distortion of taste and olfactory sensations. • Sideropenic myocardial dystrophy, tendency to tachycardia, hypotension, shortness of breath. • Disturbances in the immune system (the level of lysozyme, B-lysines, complement, some immunoglobulins, the level of T- and B-lymphocytes decreases), which contributes to a high infectious morbidity in iron deficiency anemia. • Functional liver failure (hypoalbuminemia, hypoprothrombinemia, hypoglycemia occurs).
Signs of iron deficiency anemia: hemoglobin below 110 g/l; red blood cells less than 3.5 million; color index less than 0.8-0.85; hematocrit less than 0.30-0.33; serum iron less than 10 µmol/L (10 µg/L); increase in iron-binding capacity; average erythrocyte volume 3 (normal 90 ± 10 µm3). Differential diagnosis is carried out primarily with physiological blood dilution associated with an increase in circulating blood volume. Since the plasma volume increases by approximately 1000 ml, and the volume of red blood cells by only 300 ml, a relative “anemia” occurs, which reaches a maximum in the third trimester. In multiple pregnancies, the increase in blood volume is more pronounced - 2000-3000 ml. This leads to a drop in hemoglobin to approximately 110 g/l and hematocrit to 0.30. Some authors consider the lower limit of physiological hemodilution to be 100 g/l hemoglobin and 3.0 million red blood cells. Assessing the severity of anemia. According to the degree of decrease in hemoglobin, anemia is divided into three degrees of severity: mild - 110-91 g/l; medium-heavy – 90-81 g/l; heavy – below 80 g/l. Bleeding in the postpartum and early postpartum periods is proportional to the severity of anemia. In most countries, anemia in pregnant women is considered to be with a hemoglobin level below 100-96 g/l and erythrocytes of 3.0 million, and severe with a level of 60 g/l. M.V. Khitrov (2002) also proposes, from a practical point of view, that a pregnant woman should be considered anemic with the hemoglobin and hematocrit indicators given in Table 2. However, to more reliably confirm the diagnosis of iron deficiency anemia with the indicated hemoglobin and hematocrit indicators, it is advisable to assess serum iron, average erythrocyte volume and differential diagnosis with physiological hemodilution. Megaloblastic anemia associated with folic acid deficiency accounts for 1% of all anemias in pregnant women and most often develops in the third trimester of pregnancy, before childbirth and in the early postpartum period. An adult needs 50-100 mcg of folic acid daily. Folic acid, like iron, plays an important role in many physiological processes. Folic acid is a group of vitamins, the main representative of which is pteroylglutamic acid (synonym folacin). This acid is involved in the synthesis of a number of amino acids (for example, serine, glycine, histidine, methionine) and, most importantly, methidine, a component of DNA. It also plays a key role in cell division processes. Tissues with a high rate of cell division, such as bone marrow and intestinal mucosa, are characterized by a high need for folic acid. Folic acid deficiency in the body occurs due to: insufficient content in the diet; increased need for folic acid (pregnancy, prematurity, hemolysis, cancer); impaired absorption and increased excretion from the body (some skin diseases, liver diseases). During pregnancy, when intensive new cell formation occurs, the value of folic acid increases sharply. Its participation in purine metabolism determines its importance for normal growth, development and proliferation of tissues, in particular for the processes of hematopoiesis and embryogenesis. Folic acid is involved in hematopoiesis. Hematological pathology as a result of depletion of this acid is manifested by impaired maturation of both erythrocytes and myeloid cells, which leads to anemia and leukopenia. Thrombocytopenia is sometimes possible. During pregnancy, a negative balance of folic acid is often formed, due to its intensive utilization for the needs of cellular reproduction in the growing fetus. Moreover, it is used to ensure the growth of the uterus, placenta, as well as continuously increasing erythropoiesis in the woman’s hematopoietic organs. Therefore, during pregnancy, a progressive decrease in the level of folic acid is observed not only in plasma, but primarily in erythrocytes [11, 15]. The fetus absorbs mainly the active form of folic acid, necessary for its development, and thereby depletes the mother's blood. To cover these losses during pregnancy, there is an increased need for folic acid. This need for multiparous pregnant women is greater than during the first pregnancy. A particularly high concentration of folic acid is needed during pregnancy with twins, placental abruption, and preeclampsia. It is the insufficient supply of folic acid that causes disturbances in the decidual and chorionic cells. The placenta may also be a source of higher levels of folic acid in the blood of pregnant women compared to non-pregnant women. With the loss of such a powerful storage organ as the placenta by the body, the concentration of folic acid in the blood of postpartum women sharply decreases. Lactation is accompanied by increased utilization of folic acid [15, 22]. The daily requirement of a pregnant woman's body for folic acid increases to 400 mcg, and by the time of delivery - up to 800 mcg; the need for folic acid during lactation is 300 mcg. Folic acid deficiency adversely affects the course of pregnancy and fetal development; it is detected in the second trimester in 67% of pregnant women and in the third trimester in 87% of pregnant women. Hidden folic acid deficiency is observed in up to 1/3 of the total number of pregnant women. A sufficient level of folic acid is necessary primarily for the normal development of the fetus. Full formation of the fetal nervous system is impossible if there is a deficiency of folic acid in a woman’s body before pregnancy and in its early stages. The neural tube is formed already on the 18th day after conception, and its closure occurs in the 4th week of embryogenesis. The influence of any harmful factors, including folate deficiency, can lead to the development of neural tube defects, which results in anencephaly, encephalocele or spina bifida. Another important fact confirming the role of folic acid during pregnancy is the close relationship between the level of folic acid in the mother's body and the birth weight of the child. Several weeks before birth, the fetus uses the mother's folic acid to increase its own weight and replenish its folate reserves. As a result, in women with folic acid deficiency, the likelihood of having a child with malnutrition and a reduced supply of folic acid increases significantly [2, 15, 20, 22, 23]. Iron deficiency anemia is accompanied by numerous complications during pregnancy and childbirth for the mother and fetus. Due to the fact that during pregnancy, oxygen consumption increases by 15-33%, pregnant women with iron deficiency anemia are characterized by severe tissue hypoxia with the subsequent development of secondary metabolic disorders, which may be accompanied by the development of dystrophic changes in the myocardium and a violation of its contractility. Iron deficiency anemia is characterized by disturbances in protein metabolism with the occurrence of protein deficiency in the body, which leads to the development of edema in a pregnant woman. With iron deficiency anemia, degenerative processes develop in the uterus and placenta, which lead to disruption of its function and the formation of placental insufficiency. In this case, the developing fetus does not receive sufficient quantities of the nutrients and oxygen it needs, resulting in delayed fetal development. The main complications of pregnancy with iron deficiency anemia are: threat of miscarriage (20-42%); gestosis (40%); arterial hypotension (40%); premature placental abruption (25-35%); delayed fetal development (25%); premature birth (11-42%). Childbirth is often complicated by bleeding. In the postpartum period, various inflammatory complications can occur (12%) [7, 9, 11, 17]. In children during the neonatal period, there is a large loss of body weight and a slower recovery, delayed loss of the umbilical cord and delayed epithelization of the umbilical wound, and a long course of physiological jaundice. Iron deficiency in the mother during pregnancy affects the growth and development of the child's brain, causes serious deviations in the development of the immune system, and in the neonatal period of life causes a high risk of infectious diseases.
Treatment Pregnant women with iron deficiency anemia need medication and dietary treatment. It is impossible to reverse iron deficiency anemia without iron supplements with just a diet consisting of iron-rich foods. However, pregnant women with iron deficiency anemia are prescribed a special diet. 2.5 mg of iron per day is absorbed from food, while 15-20 times more from medications. The greatest amount of iron is found in meat products. The iron they contain is absorbed by the human body by 25-30%. The absorption of iron from other products of animal origin (eggs, fish) is 10-15%, from plant products - only 3-5%. The largest amount of iron (in mg per 100 g of product) is found in pork liver (19.0 mg), cocoa (12.5 mg), egg yolk (7.2 mg), heart (6.2 mg), veal liver ( 5.4 mg), stale bread (4.7 mg), apricots (4.9 mg), almonds (4.4 mg), turkey meat (3.8 mg), spinach (3.1 mg) and veal ( 2.9 mg). A pregnant woman with iron deficiency anemia should adhere to a balanced diet. Protein products are recommended: beef, bovine liver, tongue, liver and heart, poultry, eggs and cow's milk. Fats are found in: cheese, cottage cheese, sour cream, cream. Carbohydrates should be replenished by: wholemeal rye bread, vegetables (tomatoes, carrots, radishes, beets, pumpkin and cabbage), fruits (apricots, pomegranates, lemons, cherries), dried fruits (dried apricots, raisins, prunes), nuts, berries ( currants, rose hips, raspberries, strawberries, gooseberries), cereals (oatmeal, buckwheat, rice) and legumes (beans, peas, corn). Fresh herbs and honey must be included in your diet. Treatment of iron deficiency anemia should be carried out with iron supplements: Treatment with iron supplements should be long-term. The hemoglobin content increases only at the end of the third week of therapy for iron deficiency anemia. Normalization of red blood counts occurs after 5-8 weeks of treatment. It is most preferable to take iron supplements orally rather than by injection, since in the latter case various side effects may occur more often. In addition to iron, medications for the treatment of iron deficiency anemia contain various components that enhance iron absorption (cysteine, ascorbic acid, succinic acid, folic acid, fructose). For better tolerability, iron supplements should be taken with meals. It must be taken into account that under the influence of certain substances contained in food (phosphoric acid, phytin, tannin, calcium salts), as well as with the simultaneous use of a number of medications (tetracycline antibiotics, almagel), the absorption of iron in the body decreases. It is preferable for pregnant women to prescribe iron supplements in combination with ascorbic acid, which is actively involved in the processes of iron metabolism in the body. The content of ascorbic acid should be 2-5 times higher than the amount of iron in the preparation. Currently, a number of effective drugs are used to treat anemia in pregnant women. The question of prescribing a specific drug, as well as its single dose, frequency of use and duration of treatment is decided only by the attending physician on an individual basis. Treatment with iron supplements should not be stopped after normalization of hemoglobin levels and red blood cell counts in the body. Normalizing hemoglobin levels in the body does not mean restoring iron reserves in it. Iron deficiency anemia should be treated mainly with drugs for internal use. In the early stages of iron deficiency anemia, oral iron preparations - di- and trivalent iron compounds - are used. Numerous drugs for oral use are widely presented in any drug reference book [16]. Even the far from complete list of ferrous preparations for oral administration demonstrates the difficulty of choosing the optimal remedy (Table 3). Since ionized iron is absorbed from the gastrointestinal tract only in divalent form and ascorbic acid plays a great role in this process, its presence in the preparation is very important. A significant role in hematopoiesis belongs to folic acid, which enhances nucleic acid metabolism. For the normal metabolism of folic acid, cyanocobalamin is necessary, which is the main factor in the formation of the active form from it. Deficiency of these substances, often occurring in anemia associated with blood loss, leads to disruption of DNA synthesis in hematopoietic cells, while the inclusion of these components in the drug increases the active absorption of iron in the intestine, its further utilization, and also releases additional amounts of transferrin and ferritin. All this significantly increases the rate of hemoglobin synthesis and increases the effectiveness of therapy for iron deficiency conditions and iron deficiency anemia. All these requirements are met by the complex antianemic drug Ferro - Folgamma, containing 100 mg of ferrous sulfate, 5 mg of folic acid, 10 mcg of cyanocobalamin and 100 mg of ascorbic acid. The active components of the drug Ferro-Folgamma are in a special neutral shell, which ensures their absorption, mainly in the upper part of the small intestine. The absence of local irritation on the mucous membrane of the gastrointestinal tract contributes to good tolerability of the drug. Ferro-Folgamma is prescribed 1-3 capsules per day. The best effect is obtained by taking the drug before meals. For mild anemia, it is recommended to take 1 capsule 3 times a day for 3-4 weeks; for moderate cases, 1 capsule 3 times a day for 8-12 weeks; in severe cases, 1 capsule 3 times a day for 16 weeks or more. The good clinical effect of the drug is confirmed by data from clinical studies. In an open controlled study carried out over three years, the effectiveness and tolerability of Ferro-Folgamma and a number of other iron-containing drugs were compared (V.V. Gorodetsky et al., 2004). It has been shown that this drug is really well tolerated by patients, and according to this characteristic it is included in the group of drugs with the lowest incidence of side effects. In this study, the patients did not have dyspeptic symptoms or other complaints that could be considered as a result of taking Ferro-Folgamma. As a result of the therapy, subjective and more objective clinical signs of iron deficiency anemia quickly resolved - general weakness, dizziness, shortness of breath during exercise, pallor of the mucous membranes, tachycardia. In this case, clinical improvement preceded the normalization of red blood counts. This drug provided the highest average rate of increase in hemoglobin, and rapid normalization of the number of red blood cells and serum iron levels was noted. Within a month after stopping taking the drugs, patients receiving Ferro-Folgamma did not experience a repeated decrease in hemoglobin, and there was even a tendency for its continued increase, which was combined with a pronounced decrease in the total iron-binding capacity, which indicated the continued normalization of ferrostatus and increased absorption of food iron (due to the rapid and complete restoration of enterocyte function against the background of the complex influence of Ferro-Folgamma). As studies show (Maev I.V. et al., 2003, 2004), Ferro-Folgamma is a highly effective remedy both in therapeutic practice for chronic bleeding (one of the most common causes of iron deficiency anemia) and in the treatment of posthemorrhagic anemia in surgical practice . There is also evidence that in patients with chronic inflammatory bowel diseases, the most suitable drug for the treatment of iron deficiency is Ferro-Folgamma (Gracianskaya A.N. et al., 2003). A special area of application of ferrodrugs, especially Ferro-Folgamma, is iron deficiency anemia in pregnant women. The importance of this problem is due to a number of factors: the prevalence of iron deficiency anemia in pregnant women, the increased need for iron during pregnancy, the danger of this condition for the fetus, the danger of this condition for the mother. Treatment of iron deficiency anemia in pregnant women has additional difficulties:
• gastric dyspepsia that often accompanies pregnancy (nausea, changes in taste preferences); • frequent multivitamin deficiency, including deficiency of folic acid, which poses an additional threat to the fetus; • the possibility of developing folic acid deficiency against the background of successful therapy with ferrodrugs. As studies have shown (Petrukhin V.A., Grishin V.L., 2002), Ferro-Folgamma is well tolerated by women, providing a rapid increase in hemoglobin, red blood cells, hemoglobin content and concentration in red blood cells.
There is convincing evidence (Sopoeva Zh.A. et al, 2002, 2003) that Ferro-Folgamma has a positive effect on the general condition of pregnant women, hematological parameters, ferrostatus and serum levels of folic acid and cyanocobalamin not only in isolated iron deficiency anemia, but also in combination with gestosis. In another study (Murashko L.E. et al., 2002), against the background of combined therapy with the inclusion of Ferro-Folgamma, convincing results were obtained in the treatment of iron deficiency anemia in pregnant women with preeclampsia. Thus, the results of the conducted studies suggest that the combined drug Ferro - Folgamma, in terms of effectiveness and tolerability, can be considered the drug of choice for the treatment and prevention of iron deficiency anemia in pregnant women. In case of iron deficiency anemia, one should not resort to blood transfusions without vital indications: the risk of infection with viral hepatitis is too great. In addition, red blood cell transfusion immunizes the patient with antigens she does not have. In subsequent pregnancies, this can lead to miscarriages, stillbirths, and hemolytic disease of the newborn. Iron from transfused red blood cells is poorly utilized. The criterion for vital indications for blood transfusion is not the level of hemoglobin, but the general condition of the patient, the state of hemodynamics. Indications for blood transfusion may occur 1-2 days before delivery when the hemoglobin level is 40-50 g/l. Prevention of anemia is primarily required for pregnant women with a high risk of developing anemia. These may include:
• women who previously suffered from anemia; • women with chronic infectious diseases or chronic diseases of internal organs; • multiparous women; • pregnant women with a hemoglobin level in the first trimester of less than 120 g/l; • pregnant women with multiple pregnancies; • pregnant women with symptoms of toxicosis; • women who have had periods of more than 5 days for many years.
Prevention consists of prescribing a small dose of iron supplements (1-2 tablets per day) for 4-6 months, starting from the 12-14th week of pregnancy. At the same time, patients are recommended to increase the content of meat products in their daily diet. Thus, iron deficiency anemia in pregnant women is an important problem related to both the health of the mother and her fetus. The use of new complex preparations with a balanced content of iron, folic acid, cyanocobalamin and ascorbic acid in one capsule (Ferro-Folgamma) allows one to achieve good results in the treatment of this pathology, and prophylactic use during pregnancy and lactation prevents the development of severe complications on the part of the mother and her child.
Literature 1. Burlev V.A., Konovodova E.N., Murashko L.E., Sopoeva Zh.A. Correction of iron deficiency conditions in pregnant women with gestosis // Problems of reproduction 2002; 6:30-34. 2. Burlev V.A., Ordzhonikidze N.V., Sokolova M.Yu., Suleymanova I.G., Ilyasova N.A. Compensation for iron deficiency in pregnant women with bacterial and viral infection. 2006. 3. Gorodetsky V.V., Godulyan O.V. Iron deficiency conditions and iron deficiency anemia: diagnosis and treatment. 2005. 4. Demikhov V.G. Anemia in pregnant women: differential diagnosis and pathogenetic rationale for therapy. Author's abstract. dis. ... Doctor of Medical Sciences, Ryazan, 2003. 5. Zakharova I.N., Zaplatnikov A.L., Malova N.E. Selection of drugs for ferrotherapy of iron deficiency anemia in children // RMZh 2003; 11: 1. 6. Kazyukova T.V., Samsygina G.A., Kalashnikova G.V. and others. New possibilities for ferrotherapy of iron deficiency anemia // Clinical Pharmacol and Therapy 2000; 2: 88-91. 7. Kasabulatov N.M. Iron deficiency anemia in pregnant women // Breast Cancer 2003. 8. Konovodova E.N., Burlev V.A., Kravchenko N.F., Karibdzhanov O.K., Murashko L.E., Sopoeva Zh.A. Transferrin saturation coefficient with iron in pregnant women // Problems of reproduction 2002; 6: 45-47. 9. Makarov I.O. Anemia and pregnancy // Med Journal SonoAce-International 2007. 10. Petrukhin V.A., Grishin V.L. Treatment of anemia in pregnant women using the drug Ferro-Folgamma. // Problems of reproduction 2002; 6. 11. Podzolkova M.A., Nesterova A.A., Nazarova S.V., Sheveleva T.V. Bulletin of Siberian Medicine 2006; 3. 12. Pukhalskaya T.G. Study of the effectiveness and safety of the drug Ferlatum. Gynecology, Extra Issue 2005; 11-15. 13. Smirnov A.N., Chesnokova N.P., Mikhailov A.V. Iron deficiency anemia in pregnant women. Etiology and pathogenesis of metabolic and functional disorders. Saratov 1994. 14. Serov V.N., Orzhonikizhze N.V. Anemia - obstetric and perinatal aspects // RMJ 2004; 12: 1. 15. Khitrov M.V., Okhapkin M.B., Ilyashenko I.N. A manual for doctors and interns. Yaroslavl 2002. 16. Chuchalina A.G., Belousov Yu.B., Yasnetsova V.V. Federal guidelines for the use of drugs. 2006. 17. Shekhtman M.M. Iron deficiency anemia and pregnancy. Pharmacoter in Obstetrics 2000; 6:2:17-25. 18. Shekhtman M.M., Nikonov A.P. Iron deficiency anemia in pregnant women and its treatment. 2000. 19. Breymann C. Iron deficiency and anemia in pregnancy: modern aspect of diagnosis and therapy. Blood Cells Mol Dis 2002; 29:3:506-516. 20. Crichton R, Danielson Bo.G, Gaisser P. Iron therapy with special emphasis on intravenous administration / 2nd edition. Bremen: UNI-MED, 2005. 21. Margaret PR et al. Abnormal iron parameters in the pregnancy syndrome preeclampsia. Am J Obstet Gynecol 2002; 187: 412-418. 22. 42nd Annual Meeting of the American Society of Hematology December 1-5, 2000, San Francisco, CA. 23. Recommendations to Prevent and Control Iron Deficiency in the United States MMWR 47 (RR-3); 1-36.
Risk group for anemia in pregnant women:
- Pregnancy in adolescence.
- Pregnancy and lactation during the previous 3 years, many births (more than 3 with a short interval).
- Excessive menstrual blood loss (monthly blood loss more than 100 ml).
- Gynecological diseases, especially uterine fibroids and endometrial diseases, inflammatory diseases of the pelvic organs.
- Diets low in animal protein (vegetarianism).
- Regular blood donation.
- Diseases of the gastrointestinal tract.
- Low socio-economic status.
- Obesity.
At the same time, WHO recommends that all menstruating women be considered at risk, provided that the prevalence of anemia in non-pregnant women in the region exceeds 20%.
Drugs for treatment
What should women take to restore hemoglobin? It is recommended to take medications containing divalent or trivalent forms of iron. The dosage and specific medicine are selected individually, depending on the severity of the disease and existing complications:
When a woman has difficulty taking tablets or capsules, absorption through the mucous membrane of the digestive tract is impaired, there is microelement intolerance, or there is a gastric ulcer, duodenal ulcer, drugs for parenteral use are prescribed.
Taking vitamin C at the same time improves the absorption of iron. It is also recommended to take folic acid if anemia is associated with a deficiency of this substance. Vitamin B12 is prescribed when a woman has a cyanocobalamin deficiency.