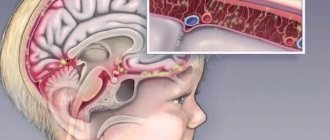
What is the DPT vaccine for?
DTP vaccination is an adsorbed pertussis-diphtheria-tetanus vaccine. All three diseases that it protects against are caused by bacteria that produce toxins and attack the human body. Vaccination cannot protect against bacterial infection - it is aimed at neutralizing toxins.
Vaccine composition
The DPT vaccine contains components of three bacteria: Bordetella pertussis (causes whooping cough), Corynebacterium diphtheriae and Clostridium tetani (causes diphtheria and tetanus, respectively).
The pertussis component of the vaccine is represented by whole microbial cells, previously “killed” by formaldehyde. To protect against diphtheria and tetanus, the vaccine includes separate purified diphtheria and tetanus toxoids, which are obtained from the bacteria that cause these diseases. Thus, DTP is an inactivated vaccine. It may not provide as much protection as live, attenuated vaccines such as the measles vaccine, so it must be given multiple times.
Aluminum salts are added to DPT as an immune response enhancer (adjuvant). Antigens adsorbed on them provoke the development of humoral immunity.
Many people are afraid of the DPT vaccine because of its high reactogenicity. This is due to its pertussis component – whole cells of Bordetella pertussis. If for some reason your child cannot receive DPT, vaccination against diphtheria and tetanus can still be done. For this purpose, there are separate preparations of toxoids: AS - tetanus toxoid, AD - diphtheria toxoid and ADS - diphtheria and tetanus toxoids without pertussis component. Of course, ADS vaccination is more convenient, because then you will have to give fewer injections when receiving subsequent doses.
HOW Vaccination AFFECTS THE SPREAD OF INFECTIONS
Before the advent of the DTP vaccine in the 1950s, infections such as tetanus, diphtheria and whooping cough caused very serious illness and even death. According to statistics, 20% of children suffered from diphtheria, and by the age of two years, almost half of the cases were fatal. Child mortality from tetanus was even higher and reached 95%. And whooping cough was almost as common as ARVI - almost 100% of children suffered from it, with varying degrees of severity. The WHO estimates that since the start of a large-scale pertussis vaccination campaign in the 1950s and 1960s, the number of cases has dropped by 90%!
In Russia, statistics also show positive figures: in 2016, there were only two cases of diphtheria infection and three of tetanus. Only about 8,000 people had whooping cough - 1.7 cases per 100,000 people. When you compare this to 1958, when there were 475 reported cases of whooping cough per 100,000 people, the statistics speak for themselves: the vaccine has indeed helped minimize the spread of the infection.
The anti-vaccination campaign that began in the 1980s led to a decrease in vaccination coverage of the Russian population to 60%, and this almost immediately affected the incidence of many infections, including whooping cough. By 1993, the number of reported cases had increased 13-fold. After the 2000s, when active public education led to an increase in the number of people vaccinated, especially children, the picture changed again.
Vaccination schedule
DTP vaccination is included in the National Preventive Vaccination Calendar. The vaccination course consists of three vaccinations:
- at 3 months,
- at 4.5 months,
- at 6 months.
Then at 18 months, revaccination is carried out. If the schedule was violated, the doctor waits 12–13 months after the last DPT vaccination. If the DPT vaccine was not administered at all, the age of the child matters:
- if the child is under 3 years 11 months 29 days, DPT is administered;
- if older, but not yet 6 years old, the pertussis component is excluded and ADS toxoid is administered;
- for children over 6 years of age, ADS-M toxoid is used, in which the content of diphtheria toxoid is reduced.
Important! According to the vaccination schedule, children at 6-7 and 14 years of age must undergo a second and third revaccination against diphtheria and tetanus using toxoid preparations with a reduced content of the diphtheria component (ADS-M). In the future, revaccination against these diseases is carried out for all adults once every 10 years.
Revaccination of older children and adults against whooping cough is not carried out in Russia, although vaccination with acellular whooping cough vaccines is widely practiced abroad in children and adolescents, as well as pregnant women, starting from the 26th week of pregnancy, which helps protect infants under 3 months from the disease (for vaccination of older children age and adults use special preparations with a reduced content of diphtheria toxoid).
Vaccination against diphtheria, whooping cough, tetanus
- A little history
- Composition, properties of vaccines
- Vaccine effectiveness
- Vaccine administration technique
- Vaccine administration schedule
- Preparing for DPT vaccination
- Contraindications: true and false
- Adverse reactions
- Complications
- Storage
- DPT (international abbreviation DTP) is a combination vaccine against diphtheria, tetanus and whooping cough. Such vaccines include the Russian DPT vaccine and the French Tetrakok, which, in addition to the listed infections, also protects against polio. In a number of CIS countries, the French vaccine “D.T. Kok" is identical in set of components to DPT. In some CIS countries, the Belgian vaccine Tritanrix-HB is used, which contains, in addition to DTP, a vaccine against hepatitis B.
- ADS (DT) - vaccines against diphtheria and tetanus (Russian "ADS" and French "D.T. Vac"), used in the presence of certain contraindications to DTP vaccines, including previous whooping cough.
- ADS-M (dT or Td) - vaccines for the prevention of diphtheria and tetanus in children over 6 years of age and adults, with a reduced content of the diphtheria component. Such vaccines include the Russian ADS-M and the French Imovax D.T. Adultery."
- AC (T) is a monovaccine for the prevention of tetanus.
- AD-M (d) is a monovaccine for the prevention of diphtheria.
Currently, for the prevention of diphtheria, tetanus and whooping cough in Russia and other CIS countries, the following are used:
Monovalent (individual) vaccines against whooping cough have been developed abroad and in Russia, but until now they have not entered into everyday vaccination practice due to the presence of a combined vaccine and a number of conditions limiting their use. Next, we will mainly talk about DTP vaccines, which are the “backbone” of vaccination against diphtheria, tetanus and whooping cough.
A little history
The first pertussis vaccine appeared in the USA in 1941, and the first combined DPT vaccines were introduced into vaccination practice abroad in the late 40s of the 20th century. DTP vaccines are included in the mandatory set of vaccines recommended by the World Health Organization. Currently, vaccination against whooping cough is carried out in all countries of the world. Attempts to cancel vaccination against pertussis in some countries led to a sharp increase in incidence and, as a result, vaccination was resumed.
Composition and properties of vaccines
Modern DPT vaccines typically contain 30 international units (IU) of diphtheria toxoid, 40 or 60 IU of tetanus toxoid, and 4 IU of pertussis vaccine. Such significant dosages of diphtheria and tetanus toxoids are administered in order to achieve a response of the required intensity from the child’s still imperfect, weakly responsive immune system. In children over 6 years of age and adults, significantly lower dosages are used, in particular for the diphtheria and tetanus components, due to the higher degree of development of the immune system and the increased risk of allergic reactions.
It is no secret that with diphtheria and tetanus, what is dangerous is not the very presence of bacteria in the body, which can only cause purulent inflammation, but their release of toxic waste products, toxins that block a number of functions of the human body.
Diphtheria and tetanus toxoids are chemically inactivated (neutralized) toxins of diphtheria and tetanus bacilli that are not capable of causing intoxication, but are capable of forming an immune response. From an immunological point of view, toxoids are not ideal antigens, which again justifies the use of large dosages in young children and explains the high risk of allergic reactions to them when using equally large dosages in older children and adults.
The whooping cough vaccine is a suspension of whole inactivated (killed) whooping cough bacilli. This means, on the one hand, the greater effectiveness of such vaccines, due to the fact that the body “gets an idea” of a practically unchanged bacterium. The other side and disadvantage of whole-cell vaccines is the greater risk of adverse reactions, since, along with the antigens necessary for the development of immunity, whooping cough bacteria also contain a number of toxic substances.
In those developed in the recent past, the so-called. Acellular, or acellular, pertussis vaccines use only a few pertussis antigens. It is quite logical that such vaccines, i.e., vaccinations with them, are much better tolerated, but at the same time somewhat less effective. By the way, another reason for refusing to use DTP vaccines in children over 6 years of age and adults is the higher risk of adverse reactions to the pertussis vaccine.
All vaccines for the prevention of diphtheria, tetanus and whooping cough are inactivated (killed), that is, they do not contain anything living. It is known that individual antigens in their pure form and inactivated vaccines are inferior in effectiveness to live vaccines.
In this regard, aluminum hydroxide is used as an amplifier (so-called adjuvant) for vaccines against diphtheria, tetanus, whooping cough (and a number of other infections). The point of using this substance is to enhance the inflammatory reaction at the site of vaccine administration and, as a result, intensify immune reactions and increase the effectiveness of vaccinations in general.
Vaccine effectiveness
All components of DPT vaccines are capable of forming immunity in almost 100% of those vaccinated. Vaccines against diphtheria and tetanus, upon completion of the primary course of vaccinations, form immunity lasting about 10 years, which explains the need for revaccination after this period of time.
Vaccines against whooping cough, according to foreign data, form immunity lasting about 5-7 years, but revaccination is hampered by the high reactogenicity of whole-cell vaccines in older children, adolescents and adults, as well as the lack of mass production of combined vaccines for children over 6 years of age and adults based on acellular pertussis vaccine.
Vaccine administration technique
All vaccines against diphtheria, tetanus and whooping cough are administered intramuscularly. This is caused by the presence of aluminum hydroxide in them, which, when administered subcutaneously, accumulates in fatty tissue, forming persistent lumps that dissolve over many months, sometimes disturbing the child (itching).
In addition, part of the vaccine is deposited in fatty tissue and does not enter the body immediately, which leads to fragmentation of the immunizing dose and a decrease in the effectiveness of the vaccine. In the United States, there are recommendations according to which subcutaneous administration of vaccines against diphtheria, tetanus and whooping cough is considered incorrect, is not accepted, and the vaccination is repeated.
In addition, subcutaneous administration of DTP vaccines may increase the risk and duration of adverse reactions because the vaccine is absorbed more slowly. The risk of widespread swelling of the limb increases, which is due to poorer blood supply and “washing” of fiber compared to muscle tissue.
In children under 3 years of age, the recommended site for administration of any vaccines is the anterolateral surface of the thigh, in its middle third. In children over 3 years of age and adults, vaccines are recommended to be injected into the deltoid muscle of the shoulder (muscle protrusion on the shoulder, in the upper third, the injection is done from the side).
Administration of any vaccine into the gluteal region is strongly discouraged, especially in young children, due to the high risk of mechanical or inflammatory damage to the sciatic nerve (and possible disability) and great vessels.
In adults, the subcutaneous layer is pronounced in the buttock area, which is why such “intramuscular” vaccination is essentially subcutaneous, that is, incorrect.
Vaccine administration schedule
The standard regimen for using DTP vaccines consists of 4 vaccinations: three with an interval of 1–2 months, starting at the age of 2 or 3 months, the fourth is administered 12 months after the third vaccination. The first three vaccinations are the primary course, the fourth is the first (and last, in the case of whooping cough) revaccination. The minimum interval between the first three vaccinations is 1 month, between the third and fourth it is 6 months. Thus, the complete scheme, with minimal intervals, looks like: 0 - 1(2) - 2 (4) - 12 (6) months.
Options are possible when an interval of 1.5 months (6 weeks) is used between the first three vaccinations, as in the Russian vaccination calendar since 2002.
In a number of countries (usually economically backward), vaccination against whooping cough consists of 3 vaccinations. Conversely, in a number of highly developed countries, 5-dose vaccination is practiced using whole-cell or acellular DTP, with the last dose administered at 6 or 7 years of age (to protect against whooping cough at school age). The possibility of revaccination of adolescents aged 15–16 years using acellular vaccines is also being considered.
The use of the Russian DTP vaccine has a number of features. Thus, this vaccine, according to the current instructions for it, can only be vaccinated in children up to 4 years of age. The incomplete course of DTP vaccination when the child reaches 4 years of age is completed using the ADS vaccine (up to 6 years) or ADS-M (after 6 years). This restriction does not apply to foreign DPT vaccines. The administration regimen of ADS differs from DPT and consists of two vaccinations with an interval of 1 month and the first revaccination, which is carried out 9–12 months after the second vaccination (the remaining revaccinations are carried out using ADS-M).
One of the indications for the use of ADS is whooping cough in a child. If a child who has had whooping cough has already received two DTP vaccinations, then the course of vaccination against diphtheria and tetanus is considered completed, and revaccination is carried out after 9–12 months. If a child received only one DTP vaccine before contracting whooping cough, then another dose of DTP is administered, and a third after 9–12 months.
The ADS-M administration regimen, in cases where a person over the age of 6 years has not been vaccinated against diphtheria and tetanus, consists of two vaccinations with an interval of 1 month and the first revaccination after 6–9 months. All other revaccinations with ADS-M, regardless of when the person was first vaccinated, are carried out every 10 years.
The course of vaccinations with vaccines against diphtheria and tetanus is never started again due to the absence of a clear need for this and the high probability of severe adverse reactions. That is, even in the case of gross violations of the vaccination schedules, only the missing vaccinations are carried out, but the vaccination course should in no case be started anew. For example, if 12 months have passed since the administration of the 2nd dose, then you simply need to administer the third dose and revaccinate after 6-12 months.
Of course, the effectiveness of the formed immunity with highly modified vaccination regimens may be somewhat lower than that when using a standard regimen, however, this difference, as studies show, is not so great as to expose the child to a high risk of adverse reactions when repeating certain (not done on time) or all vaccinations already done. The only exception is in cases where a particular vaccination was given with gross violations of the administration technique, i.e., for example, subcutaneously and not intramuscularly.
Preparing for DPT vaccination
DTP vaccines are among the most reactogenic (i.e., capable of causing adverse reactions) drugs. This is explained both by the high content of antigens and their properties - the most reactogenic components of DTP vaccines are pertussis and, to a lesser extent, diphtheria. For this reason, before vaccination with the DTP vaccine, medicinal preparation of the child is recommended.
Without exception, all (whole cell) DPT vaccines should be administered against the background of antipyretics (antipyretics). This allows, on the one hand, to prevent a possible uncontrolled increase in temperature, on the other hand, to eliminate the risk of febrile (temperature) seizures in young children that occur against a background of high fever, regardless of what caused it.
In addition, all antipyretic drugs have anti-inflammatory and analgesic properties. The latter is especially important, on the one hand, to prevent pain at the injection site, which can be quite severe, and on the other, to protect the child from severe swelling at the site of vaccine administration.
If a child has allergic disorders (most often atopic dermatitis, i.e. diathesis), the use of antiallergic drugs is also recommended.
Neither antipyretics nor antihistamines affect the development of immunity, i.e., the effectiveness of vaccination.
The general principles of using the listed drugs in preparation for vaccination are as follows:
- when purchasing medications, pay attention to the fact that this form of release is suitable for the child’s age, ask the pharmacist if this medicine is suitable for the age of your child,
- when choosing forms of release of antipyretics, you should opt for rectal suppositories, since flavorings in syrups can provoke allergic reactions,
- do not wait for the temperature to rise after vaccination, administer antipyretics in advance, since the temperature may rise too quickly to be controlled later,
- In children, aspirin (acetylsalicylic acid) should never be used; if the maximum permissible dosage of an antipyretic is exceeded and the effect is not achieved, then switch to a drug with another active ingredient (for example, from paracetamol to ibuprofen),
- if a child had no reactions to a previous vaccination, this does not mean that preparing the child for vaccination should be neglected - adverse reactions are more common after repeated vaccinations,
- In any doubtful cases, consult your doctor. Do not hesitate to call an ambulance - they may not come if the situation is not critical, but they will definitely provide advice over the phone. If the vaccination was done at a paid vaccination center, do not hesitate to take the doctor’s contact information in case of adverse reactions - in good vaccination centers, doctors themselves leave contact information or call back to find out about the child’s condition.
Approximate scheme* of preparing a child for vaccination with DTP vaccines:
- Day −2, −1. If the child has diathesis or other allergic disorders, give antihistamines in a maintenance dosage
- Day 0: Immediately after returning home, administer an antipyretic suppository. This will prevent some reactions that develop in the first hours after vaccination (prolonged crying, swelling at the injection site, etc.). If the temperature rises during the day, introduce another suppository. A candle at night is a must. If the baby wakes up at night for feedings, check the temperature and if it rises, introduce another suppository. Continue taking your antihistamine.
- Day 1. If the temperature is elevated in the morning, introduce the first suppository. If the temperature rises during the day, introduce another suppository. You may need to introduce another suppository at night. Continue taking your antihistamine.
- Day 2. Antipyretic is administered only if there is a fever. If its increase is insignificant, you can refuse antipyretics. Continue taking your antihistamine.
- Day 3. The appearance on the 3rd day (and later) of an increase in body temperature and reactions at the vaccination site is not typical for inactivated vaccines. If the temperature does rise, you should look for another reason (teething, acute respiratory infections, etc.).
*—This chart is provided as a guideline and reflects general approaches that may not take into account your child's specific health conditions. Exact dosages, dosage regimens, list and names of specific drugs can and should be recommended only by the treating pediatrician who directly examined your child.
Contraindications: true and false
In addition to general contraindications to vaccination, such as acute illness, allergy to vaccine components and severe immunodeficiency (in which the formation of immunity is impossible), DPT vaccines are temporarily or absolutely contraindicated (true contraindications) if the child has a progressive pathology of the nervous system, or convulsions were observed not against the background of an increase in temperature. In this case, children are vaccinated with a vaccine without a pertussis component (PVC).
Temporary and relative contraindications are diathesis (vaccinations can be carried out outside of exacerbations), recent acute respiratory infections (vaccinations can be carried out immediately after recovery). It should be noted that in the United States, mild acute respiratory infections are not a contraindication and vaccinations can be carried out, including against the background of a slight increase in temperature, cough, or runny nose.
Febrile (i.e., occurring against the background of an increase in temperature) convulsions observed during acute respiratory infections or other diseases (excluding DPT vaccinations) are not a contraindication, however, in this case, careful preparation of the child for vaccination is required in order to prevent temperature reactions.
A history of perinatal encephalopathy in itself is a false contraindication, since this term denotes (by the way, it is used only in the CIS countries) unclassified, a variety of (including acceptable) deviations in the development of the nervous system, registered in the first months of a child’s life . As a rule, all these manifestations disappear by the age of the start of DTP vaccinations, which can be guaranteed by a neurologist’s opinion before the start of vaccinations. Prematurity is also a false contraindication.
False contraindications to DPT vaccinations include: taking antibiotics, allergic disorders (except allergies to vaccine components), allergies in relatives, a history of seizures in relatives, severe adverse reactions to DTP in relatives.
Contraindications to vaccination with drugs against diphtheria and tetanus are only allergic or neurological reactions to previous administrations of such vaccines.
Adverse reactions
DTP vaccines are the most reactogenic, “heavy” childhood vaccines. On average, adverse reactions occur in a third of vaccinated people, and not with every vaccine. The peak frequency of reactions is observed, as a rule, on the third and fourth injections of the vaccine, which coincides with the peak rates of immunity development.
In a sense, the occurrence of adverse reactions to vaccination is natural, as a “by-product” of the process of developing immunity. The fact is that during an immune reaction, special mediator substances, internal immunostimulants of the body, enter the bloodstream, which, among other things, have properties that provoke inflammatory processes.
On the other hand, when creating vaccines, every opportunity is used to minimize, albeit natural, but still unpleasant side effects, which is achieved by minimizing the content of ballast substances and a special balance between the quantity and quality of antigens.
In general, the presence of mild adverse reactions is a favorable sign, indirectly indicating the correct formation of the child’s immune system and the effectiveness of the immunity being formed. On the other hand, as a result of efforts to minimize the risk of adverse reactions, their absence should not be taken as an alarm signal or interpreted as a defect in the immune system.
Reactions at the site of vaccine administration (in general, observed in 15–25% of vaccinated people, without taking into account the preparation of the child for vaccination):
- redness (1–2%) and swelling (1–2%) caused by immune inflammation at the injection site and the action of the adjuvant (see above).
- pain at the injection site (probability about 15%, manifested by the fact that when moving the child “protects” the leg and cries) is also a consequence of the inflammatory reaction.
General reactions (on average observed in 20% of vaccinated people, excluding the preparation of the child for vaccination):
- increase in body temperature (up to 30%),
- others (anxiety or vice versa, lethargy, vomiting, diarrhea, appetite disturbances).
As a rule, all adverse reactions to DPT vaccines develop no later than 24 hours after vaccination and last no more than 24 hours.
Reactions that occur later and last longer cannot be caused by the vaccine and in such cases another cause should be sought. As a rule, these are teething, acute respiratory infections, and intestinal infections.
In some cases, the cause of a late rise in temperature may be serious illnesses, such as otitis media and meningitis, so do not rush to conclude that such a reaction is related to the vaccine and consult your doctor to rule out serious illnesses.
To avoid confusion between adverse reactions to vaccination and food allergies, at least for the day before vaccination and the day after it, you should not introduce new complementary foods or change the mother's diet if breastfeeding. In addition to normal, severe adverse reactions may occur , the frequency of which is subject to accounting and monitored by regulatory organizations in order to prevent low-quality batches of vaccines from entering practice. If certain values are exceeded (to exclude cases of individual reactions of individual children), specific series of vaccines may be withdrawn from circulation or recalled by the manufacturer.
Severe adverse reactions:
- Prolonged unusual crying, when a few hours after vaccination the child begins to cry loudly, and the crying is more like a squeal. The cause of this reaction is pain at the injection site and, presumably, a headache. The frequency of such a reaction is 1 in 200 vaccinations.
- Increased body temperature (measured in the axillary region) above 39 °C.
- Significant swelling at the site of vaccine administration, covering an area greater than 8 cm in diameter.
Such reactions can (and should) be avoided through the prophylactic administration of antipyretics (in preparation for vaccination), which have, among other things, analgesic and anti-inflammatory effects.
Complications
As with the administration of any other vaccine, in rare cases, allergic reactions to the components of the vaccine are possible in the form of a rash, urticaria, Quincke's edema (specific swelling that covers a large area at the site of vaccine administration), anaphylactic shock, etc. These complications are not associated with the properties of the vaccine , but with the amount of ballast substances in specific preparations, the child’s allergy to them and, in some cases, non-compliance with vaccination rules.
It is significant that, according to statistics of post-vaccination complications in the United States, even severe allergic reactions to DTP vaccines have not led to serious consequences in any case since 1978, taking into account the fact that about 80 million vaccinations were given during this period.
The connection between vaccination against whooping cough and neurological complications (with the exception of temperature cramps) is now questioned and neurological syndromes, previously considered unambiguous complications of DTP vaccine, are classified as “possibly related to vaccination”. There are several reasons for this:
- There are no neurological complications that could be associated with DPT vaccines due to their high specificity;
- There are no laboratory tests or other means of proving a link between neurological syndromes and vaccination;
- DTP vaccination “passes” through the entire first year of a child’s life, being an additional reason for visits to the doctor, which leads to improved diagnosis of any problems of the child’s nervous system;
- DTP is the first temperature stimulus, i.e., in fact, a provocateur, against the background of which hitherto hidden neurological symptoms may worsen;
- Symptoms of epilepsy that appear in the first year of life were previously almost always attributed to DPT vaccines.
Possible specific complications of DTP vaccines include neurological complications. It is assumed that they may be caused by the fact that toxins (even inactivated) pertussis bacillus tend to irritate, in an extremely small proportion of susceptible children, the meninges. Manifestations of neurological complications following vaccination may include:
- Convulsions without fever (0.3–90 per 100 thousand vaccinations). The child may make involuntary sudden movements in the form of nodding, twitching of individual limbs.
- Short-term encephalopathy (literally (Greek) - brain damage, 0.1–1.0 per 100 thousand), manifested by non-temperature convulsions and short-term impairment of consciousness.
The listed complications are an absolute contraindication to continued vaccination against whooping cough, regardless of whether their connection with the vaccine has been proven or not.
False complications that are sometimes attributed to DTP include prolonged encephalopathy, convulsions that occur over a long period of time, and encephalitis. The syndrome of sudden death of children after vaccination is currently not considered even in the category of probable complications due to the fact that among unvaccinated children, as studies have shown, this syndrome is registered either with the same frequency as in vaccinated children, or more often.
Storage
Vaccines against diphtheria, tetanus and whooping cough do not require different storage conditions than other vaccines. Like all vaccines, they must be stored at a temperature of 2 to 8 ° C (refrigeration conditions in a household refrigerator).
When vaccines are frozen or overheated, the component that undergoes visible changes is aluminum hydroxide.
If the drug contains insoluble and unbreakable flakes, sediment, changes in transparency or color appears, the drug is unsuitable for use.
Normally, DTP and other vaccines look like a transparent, slightly whitish, slightly opalescent, perhaps slightly cloudy, homogeneous suspension.
Preparing a child for vaccination
Before vaccination, children are always examined by a pediatrician.
Photo: AllaSerebrina / Depositphotos The vaccine is administered intramuscularly; the procedure does not require any special preparation. However, DPT has contraindications. Some are worth paying attention to, others only create false impressions about the vaccine.
True contraindications include:
- allergy to vaccine components, which manifests itself in a strong general reaction or complications after the previous administration. These include: the first two days, temperature above 40 ℃, swelling more than 8 cm in diameter, developed Guillain-Barré syndrome (autoimmune disease);
- severe immunodeficiency;
- convulsions/fits and other diseases of the nervous system in a progressive process.
What conditions cannot be exempt from vaccination?
False contraindications to DTP vaccination:
- acute diseases (4 weeks after recovery), mild respiratory diseases (2 weeks after);
- chronic diseases (the main thing is to wait for remission);
- diathesis (beyond exacerbation);
- weight loss, prematurity;
- allergic diseases: local rashes, spasm of the respiratory tract with cough (bronchospasm);
- taking antibiotics;
- convulsions/allergic reactions to DTP in relatives.
DTP analogues
Due to the frequency and severity of side effects associated with DTP, new, acellular drugs (ACDs) became widespread in the mid-1990s. All of them, like DPT, are combined with diphtheria and tetanus toxoids, but instead of whole pertussis bacteria they contain only individual pertussis antigens. Such vaccines are better tolerated and have completely replaced the DPT vaccine in many countries with a low risk of whooping cough infection. Many of the new cell-free drugs protect against 5 or even 6 infections at once:
- Infanrix hexa (6 infections, including hepatitis B, polio and Haemophilus influenzae),
- Pentaxim (5 infections, including polio and hemophilus influenzae),
- Tetraxim (4 infections, including polio).
Among the three-component BCVs: Infanrix for children and Adasel for adults (this vaccine has a reduced amount of diphtheria toxoid).
However, experts believe that the whole-cell vaccine protects better - there are more antigens, and the immune response is closer to natural infection. If we compare acellular vaccines, those with more pertussis antigens protect better.
When choosing between whole-cell drugs, in addition to DPT, you can pay attention to four-component ones, which also protect against hepatitis B.
What vaccinations are there for whooping cough, diphtheria and tetanus?
- DTP is the most widely used vaccine in our country. It includes toxoid (neutralized toxin) of tetanus and diphtheria, as well as killed pertussis bacteria. In addition to the main components, the vaccine includes adjuvants, antiseptics and preservatives, as well as the main medium - a diluent.
- ADS and ADS-M are vaccines without a pertussis component. The ADS-M vaccine contains a reduced amount of diphtheria toxoid. These vaccines are used for revaccination in children after 7 years of age and in adults when whooping cough vaccination is no longer indicated.
- “Bubo-Kok” - in addition to the DTP components, this vaccine contains part of the hepatitis B viral protein. This is done in order to avoid giving the baby two injections at the same time, because Vaccinations according to the calendar are done together.
- "Bubo-M" is a vaccine without a pertussis component.
- "Pentaxim" - contains tetanus, diphtheria and pertussis toxoids, particles of the pertussis microbe. Additionally, polio has been added to this vaccine for ease of use. According to the vaccination calendar, the DTP and polio vaccination schedules coincide. A component against Haemophilus influenzae can be added to this vaccine from a separate vial. The decision about the need to administer it is made by the doctor. The vaccine is distinguished by the absence of whole pertussis cells - this causes fewer side effects.
- "Infanrix" is identical in composition to "Pentaxim", with the exception of the polio component - it is absent in it.
- "Infanrix hexa" - in addition to the components of "Infanrix", includes inactivated polio viruses and part of the hepatitis B virus protein.
- "Adasel" - includes: diphtheria, tetanus, pertussis toxoids and fragments of pertussis bacteria.
Which vaccine is better to choose?
Both domestic and foreign vaccine preparations against whooping cough are presented on the Russian market.
Photo: TTK TV channel In Russia, people are vaccinated with whole-cell DPT produced by the Federal State Unitary Enterprise NPO Microgen of the Russian Ministry of Health. Foreign acellular vaccines are also available:
- Belgian "Infanrix"
- French "Tetraxim" from SANOFI PASTEUR,
- French "Pentaxim" from SANOFI PASTEUR.
The Russian inactivated combined vaccine “Bubo-Kok” produced by CJSC NPK “Combiotech” also protects against hepatitis B. The first Russian 5-valent vaccine “aDTaP-HepB+Hib” or pentovaccine produced by FSUE “NPO Microgen” is already available. It protects against five common childhood infections: diphtheria, whooping cough, tetanus, hepatitis B and Haemophilus influenzae.
Pertussis vaccine for adults
Until recently, there were no pertussis vaccines for adults in Russia.
However, in 2022, the drug “Adasel” produced by SANOFI PASTEUR appeared on the domestic market (Fig. 1). This is an acellular vaccine with a reduced content of diphtheria component. The US Centers for Disease Control and Prevention (CDC) recommends giving Adasel to adults as a booster dose to re-prime the body's immune response. The drug can also be administered to children, but again for revaccination, and not as a first dose. Pregnancy is not a contraindication for vaccination. The CDC offers pregnant women the same acellular Adasel. It is introduced at the beginning of the third trimester. In Russia, such vaccination is not practiced, although studies indicate there is no evidence of a risk to pregnancy. In America, this drug is administered before each pregnancy, even if there is a year or two between them. Children in the first months of life are susceptible to whooping cough; if the mother has not been vaccinated, they are defenseless against infection.
Figure 1. Adasel vaccine. Source: NSW Health
What to do after vaccination
It is important to monitor the condition of the body after vaccination. Their parents do this for their children. Mild side effects are more likely a good sign that the body has begun to work on its immune response. It is necessary to spend at least half an hour near the vaccination room in case of unexpected severe reactions.
The main thing is not to panic when normal passing reactions appear. You can ask your doctor in advance about antipyretic and antihistamine medications for children. On the 3rd day after vaccination, the appearance of any reactions is uncharacteristic.
DPT vaccine
Dear Parents! Today we will talk once again about vaccinations, in particular about DTP. Our doctors have collected detailed information for you: what kind of vaccination this is, why it is needed, when and how it is done.
Hearing the phrase “DPT vaccination,” many young mothers fall into real horror, because this vaccination is considered the most dangerous and difficult to tolerate for the baby. Such opinions are also supported by gossip and rumors, various scary stories from the World Wide Web, due to which many women refuse vaccination altogether. Of course, our country's healthcare system gives us the opportunity to make a choice and refuse vaccination. BUT:
As a result of parents' refusal to vaccinate, cases of children contracting measles, diphtheria, whooping cough and even polio have increased noticeably in Russia. However, timely vaccination would allow us to avoid such depressing statistics. First of all, you should not give in to mass panic. It is important to take into account the compelling arguments “FOR”: Vaccination will protect the child from numerous viruses, developing immune bodies in his body to resist the disease. Mass vaccination makes it possible to avoid serious outbreaks of epidemics, but it is the fragile child’s body that becomes their first victim. There are a huge number of unsafe bacteria “walking” in the world around us, immunity to which is possible only through vaccination. Despite the fact that the vaccine does not protect 100%, vaccinated children tolerate the disease more easily.
THE THREAT AND RISK COMING FROM THE DISEASE IS MUCH HIGHER THAN FROM VACCINATION!!!
Almost all vaccines have a low risk/high benefit ratio. Massive refusal to vaccinate could lead to epidemics in the future.
SO, WHAT IS THE DTP VACCINE REALLY?
DTP (international name DTP) is a vaccine that produces immunity to three diseases at once - whooping cough, diphtheria and tetanus.
WHOOPING COUGH is a dangerous disease caused by a bacterium called Bordatellapertussis. Its main symptom is attacks of severe spasmodic cough. Whooping cough is especially dangerous for one-year-old children, as it is fraught with respiratory arrest and complications such as pneumonia. The disease is transmitted from an infected person or carrier of the infection through airborne droplets. Read more about whooping cough disease here.
DIPHTHERIA is even more difficult , the causative agent of which is a special bacterium (diphtheria bacillus), which, among other things, is capable of releasing a toxin that destroys cells of the heart muscle, nervous system and epithelium. Diphtheria in childhood is VERY SEVERE, with high fever, inflammation of the lymph nodes and characteristic films in the nasopharynx. It should be noted that diphtheria IS A DIRECT THREATEN TO THE LIFE OF A CHILD, and the younger the child, the more dangerous the situation becomes. It is transmitted through the air (by coughing, sneezing, etc.), or through household contact with an infected person.
Finally, TETANUS is a very dangerous disease for both children and adults; In addition, immunity is not formed in people who have had tetanus, so there is a possibility of re-infection. The causative agent of the disease is the tetanus bacillus, which can exist in the environment for a very long time and is very resistant to antiseptics and disinfectants. IT PENETRATES THE BODY THROUGH WOUNDS, CUTES AND OTHER DAMAGES TO THE SKIN, while producing toxins dangerous to the body. The only way to protect yourself from the above diseases is vaccination, after which a person develops stable long-term immunity.
MECHANISM OF ACTION OF THE VACCINE.
Once in the body, the drug releases weakened microorganisms that stimulate infection and cause an appropriate protective reaction in the body. Thanks to this, antibodies are formed and, as a result, immunity to the disease.
WHAT VACCINE IS VACCINED WITH?
In our country, for vaccination within the framework of the state program, we use adsorbed tetanus vaccine of domestic production, as well as a foreign drug, Infarix.
WHERE IS IT ENTERED?
Any DTP vaccine is administered intramuscularly, but if injections into the buttock were previously practiced, now it is recommended to administer the drug into the thigh. Vaccination in the buttock has a high risk of suppuration, and there is also a danger that the vaccine will get into the fat layer and its effectiveness will be reduced to zero. For older children, the injection is given in the upper arm, and some vaccines (such as ADS-M and ADS) are given under the shoulder blade using a special needle.
VACCINATION SCHEME.
All DTP vaccines have one feature - after a certain time after routine vaccination, immunity gradually weakens, so a person needs revaccination, that is, a second injection. In the absence of contraindications, the DPT vaccination schedule is as follows: I vaccination – 3 months; II vaccination – 4–5 months; III vaccination – 6 months. Mandatory condition: the first three doses of the drug must be administered at intervals of at least 45 days. When administering subsequent doses, the minimum interval between them should be 4 weeks. IV vaccination – 18 months; V vaccination – 6–7 years; VI vaccination – 14 years. Further vaccination is carried out approximately once every ten years. If the schedule is violated, vaccine doses are administered in compliance with the rule described above: that is, three vaccinations are administered after 45 days each, and the next one no less than a year later.
DTP VACCINES.
At Medical, we use several types of registered DPT vaccines from both domestic and foreign manufacturers for vaccination. The RUSSIAN-MADE vaccine is a whole-cell vaccine that consists of dead pertussis pathogens and diphtheria and tetanus toxoids. The drug can only be administered to children who have not yet reached the age of four. Adults and children over 4 years of age, as well as those who have had whooping cough, are vaccinated with ADS or ADS-m preparations that do not contain whooping cough microorganisms. INFANRIX (Manufacturer – Belgium, England). Refers to acellular vaccines that produce minimal side effects. There are several types of Infarix vaccine: * vaccine, the components of which are similar to the DTP vaccine, * InfarixGexa (DPT infections + polio, hepatitis B and Haemophilus influenzae infection). PENTAXIM (Manufacturer – France). An acellular vaccine that protects the body against DPT infections, Haemophilus influenzae and polio. Due to the minimal number of side effects, Pentaxim is considered an excellent alternative to domestic whole-cell vaccines.
VACCINE SAFETY.
Like any other medications and vaccines, DPT can cause adverse reactions. It should be noted that acellular vaccines, which contain microbial particles, are considered safer and more easily tolerated than whole-cell vaccines, which contain whole microorganisms. That is why the main task of the pediatrician is to select the type of vaccine that will be as safe as possible for your baby.
IMMUNE RESPONSE
The body's immune response to the DPT vaccine is quite strong, so it is considered the most serious vaccination in the calendar. As a result of vaccination, approximately 92–96% of vaccinated patients develop antibodies to the corresponding infectious diseases. In particular, a month after three vaccinations, the level of antibodies to diphtheria and tetanus toxins in 99% of vaccinated children is more than 0.1 IU/ml.
HOW LONG DOES POST-VACCINATION IMMUNITY LAST?
Post-vaccination immunity to infectious diseases largely depends on the type and characteristics of the vaccine. Usually, after scheduled vaccinations, it lasts for about 5 years, after which the child requires revaccination. Subsequently, immunization is sufficient to be carried out approximately once every 10 years. Generally speaking, almost every child after vaccination with DTP is considered well protected from whooping cough, tetanus and diphtheria viruses.
PREPARATION FOR VACCINATION
Since the DPT vaccine represents a serious burden on the body, it is very important to properly prepare the baby for immunization. Before routine immunization, you must: 1. visit pediatric specialists, in particular a neurologist, since most often complications after this vaccination occur in children with disorders of the nervous system. 2. It is best to take blood and urine tests to make sure there are no diseases that could complicate the child’s condition after the injection. 3. If the baby has suffered any infection (for example, ARVI), then at least two weeks should pass from the moment of absolute recovery until the moment the drug is administered. 4. Children who are prone to allergic reactions should begin to be given antihistamines in a maintenance dosage approximately three days before vaccination. 5. Immediately before vaccination, the child should be examined by a pediatrician and adequately assess his condition.
BODY REACTIONS
The reaction to the vaccine appears within three days after the vaccine is administered. It should be noted that any symptoms that appear after this period are in no way related to vaccination. NORMAL REACTIONS to the injection, which disappear within two to three days after taking antipyretics and antihistamines, are the following: * Increase in temperature. The temperature after DTP vaccination can rise to 38.5°, so about two to three hours after the injection, doctors recommend giving the child a small dose of an antipyretic. If the temperature rises again in the evening, you need to repeat taking the antipyretic. * Changes in behavior. The child may be restless, whine and even scream shrilly for several hours: this reaction is usually associated with pain after the injection. In other cases, the baby, on the contrary, may look lethargic and slightly inhibited. * Redness and swelling at the injection site. A normal reaction is swelling of less than 5 cm and redness of less than 8 cm. In this case, the child may feel pain at the injection site, and as if protecting the leg from other people’s touches. After the vaccine is administered, it is recommended to sit with the child in our Center for 20-30 minutes to avoid severe allergic reactions.
CONTRAINDICATIONS.
Of course, there are contraindications to DTP vaccination. These contraindications are determined only by doctors: a pediatrician or a neurologist. To rid yourself of doubts about vaccination, if any, you must: 1. Go to an appointment with a pediatrician at the Children's Health Medical Center, who, taking into account all the characteristics of the child, will draw up an individual vaccination plan. 2. Mom and dad take a deep breath and exhale.)) 3. Tune in only to a positive outcome of vaccination. 4. Prepare for vaccination strictly as prescribed by your pediatrician. 5. Be healthy before vaccination. 6. Get vaccinated and be calm. PLEASE stay healthy! And we are always ready to help you with this. Come see us for vaccinations. You have your choice of both domestic and imported vaccines. Make an appointment by the same phone numbers: 200-20-44; 200-50-44.
What not to do after DTP vaccination
It is better not to engage in physical activity, because an enemy has entered the body, albeit inactivated. The body’s task is to develop cells that will resist this enemy. Therefore, in the first few days you should ensure yourself peace. However, if the child feels well, then walking is not contraindicated.
It is also not recommended to change the diet of a child or a nursing mother. This can lead to additional stress on the intestines, and therefore on the entire body.
Complications after vaccine administration
DTP vaccination can cause prolonged crying in children.
Photo by Laura Garcia: Pexels Complications after vaccination that require seeking medical attention include:
- allergic rash (not local),
- more than 3 hours of uncontrollable screaming and crying,
- swelling of the face and throat,
- labored breathing,
- cardiopalmus,
- dizziness, nausea and weakness.
In the 1970s, the use of whole-cell DTP vaccine was associated with encephalopathy in children. However, numerous studies have proven the absence of this connection.