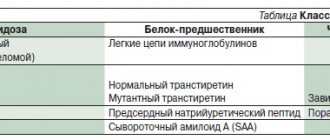
Characteristics of medicines
According to reviews of cardiologists involved in the treatment of primary or secondary hypertension, Lozap, Amlodipine, Lerkamen have proven themselves well, but not in every clinical case. Any of these pharmacological drugs can eliminate the following signs of high blood pressure within about half an hour:
- headaches localized in the temples and back of the head;
- attacks of nausea, sometimes ending in vomiting;
- weakness, fatigue;
- flickering of spots before the eyes, doubling of objects;
- hearing disorders;
- discomfort in the heart area, increased heart rate;
- swelling of the legs;
- redness of the face and neck.
When choosing an antihypertensive drug, cardiologists focus not only on the speed of symptom relief, but also on the list of contraindications and possible side effects. And also for the presence of other chronic diseases. After all, no matter how effective the drug is, safety always comes first.
Comparison of antihypertensive drugs
Patients who took Lozap, Lerkamen, Amlodipine speak differently about their therapeutic properties. Some people prefer the latter for its ability to quickly lower blood pressure. Others prefer to take imported drugs, appreciating them for their long-lasting positive effects on the cardiovascular system.
Cardiologists think a little more broadly when choosing the best remedy for the patient.
The fewer additional components in an antihypertensive drug, the less doctors worry about side effects.
An experienced cardiologist needs only to look at the composition of a drug to predict its effect on the heart muscle and coronary vessels of a particular patient. Pharmacological properties, which are somewhat different for the active components, are also important. Arterial hypertension is a dangerous pathology due to its complications, so it is important to quickly stop its exacerbations.
Features of the composition of the tablets
Amlodipine is produced by many pharmaceutical companies - Ozone, Vertex, Canonpharma, Teva. There is also Vero-amlodipine from Veropharm on pharmacy shelves. Many cardiologists like Amlodipine for its small amount of additional ingredients. To form its auxiliary composition, manufacturers used crospovidone, lactose monohydrate, calcium stearate and povidone.
Lozap is produced in a Slovak pharmaceutical factory. In addition to the active substance losartan, its composition is represented by the following ingredients:
- povidone;
- croscarmellose sodium;
- mannitol;
- magnesium stearate;
- hypromellose;
- talc;
- macrogol;
- dimethicone.
Lozap has more additional substances than other drugs. They act as stabilizers and preservatives, ensuring the gradual release of losartran from the tablet base and its most complete penetration into the general bloodstream.
Lerkamen is produced by the German pharmaceutical concern Berlin-Chemie. Its therapeutic activity is determined by lercanidipine.
And the auxiliary composition is formed from povidone, milk sugar, cellulose, magnesium stearate. Each tablet is coated with iron oxide, titanium dioxide, talc, opadry and macrogol. Auxiliary components are conductors of lercanidipine into the bloodstream.
Set of pharmacological properties
The general purpose of use of Lozap, Amlodipine, Lerkamen is to stabilize blood pressure in patients with hypertension. According to cardiologists, they cope with this task well. But the mechanism of pressure rise is different, so the selection of drugs is made taking into account their principles of action.
| Antihypertensive drug | pharmachologic effect |
| Amlodipine | Blocks calcium channels, helps slow down the transmembrane transition of calcium ions into cells, dilates arterioles, peripheral and coronary arteries |
| Lozap | Provides a decrease in total peripheral vascular resistance, reduces the load on the heart muscle, has a diuretic effect, normalizes the levels of the neurotransmitters adrenaline and aldosterone in the blood |
| Lerkamen | Inhibits the penetration of calcium ions into the smooth muscles of coronary vessels, has a direct relaxing effect on smooth muscle cells, and helps reduce peripheral resistance |
The complex mechanism of action of drugs determines their inclusion in patients’ therapeutic regimens. It depends on it how long it takes for the hypotensive effects to appear and for how long they will persist. And also how to cope with the pharmacological load on the patient’s body.
Amlodipine tablets - reviews
Tatiana
Maybe the information will be useful. I will not describe the events before. Too much and intense. Before that, I took amlodipine 0.5 + more. I was admitted to the hospital with severe nosebleeds. After discharge, I took amlodimine in the morning 1 mg 'at around 5 o'clock in the afternoon (i.e., during the period of maximum concentration in the blood), the pressure steadily rose to 200. And before that, the pressure was very low for me - 130. I analyzed - for my body the pressure is 120 - 130 is almost dangerous and my body saved me by raising my blood pressure. I started taking 0.5 again. The five o'clock phenomena disappeared. Our body is smarter than us. The trouble is that we do not always understand it. What’s interesting is that I’ve had blood pressure since the time when I weighed 48 kg (now, alas, 75). I have three children. As soon as I became pregnant, without any medications, my blood pressure was always normal. Be healthy!
Eteri
Maybe I have a thyroid problem. ? Get checked
Alina Bolshakova
I read some reviews and am surprised... I stopped drinking for two weeks, then the doctor told me to start drinking again... Almost all antihypertensive drugs have a cumulative effect. Fortunately, a stable decrease begins after approximately 3 - 4 weeks of constant use at the same time of day (preferably). And if you drink today and don’t drink tomorrow, it will cause even more harm to your health. All doctors have different opinions about amlodipine, some say that it is a drug with a minimum number of side effects, others say the opposite. Everything is individual.
Lessa-LP
https://otzovik.com/review_4490650.html
Advantages:
- effective remedy
- low price
Flaws:
- severe swelling of the legs
Greetings to the Authors and Readers of the Otzovik site!
Our grandfather is almost eighty years old. Of course, at his age you have to constantly monitor your blood pressure. Our grandfather is “advanced” and gets a lot of useful information from the Internet. He uses many different methods against hypertension, ranging from special breathing exercises, a la Yoga, to taking ASD 2. Last summer, before going to the hospital for a full examination (he has problems with his joints), he stopped taking ASD 2 so as not to spoil the clinical picture.
The doctor at the hospital prescribed Amlodipine tablets for hypertension. Grandfather did not resume taking ASD 2 (there are some “regime” requirements when taking it that I didn’t want
The doctor told me to take two tablets - 20 mg, once a day, before bed. A pack of sixty tablets was enough for a month. With a pack price of 173 rubles. Grandfather honestly took Amlodipine for half a year (from August 2016 to January 2017), but... Gradually he began to notice that his legs were swelling. At the beginning a little, then more. We read “side effects”, the second item indicates “swelling of the ankles and feet.”
Of course, having reached this stage, the grandfather decided to stop taking Amlodipine and return to ASD 2. The rest of the pack of Amlodipine went into the trash.
Conclusion:
Amlodipine is a truly effective medicine against hypertension. But this barrel of honey has its own fly in the ointment - swelling of the legs.
I note that the degree of swelling shown in the photo was achieved only in January. But a fact is a fact. We do not recommend taking this drug, but advise you to choose something else.
I wish you all excellent health! Thank you for reading my review.
Anonymous565624
https://otzovik.com/review_2328044.html
Advantages:
normalizes blood pressure
Flaws:
causes swelling of the legs
I have been taking it for only 4 days, but there is already an effect - the pressure does not exceed 140x80. However, severe swelling of the legs immediately began in the area of the foot and ankle (this had never been observed before). After carefully reading the instructions, it became clear that this is a common side effect of amlodipine. In addition, amlodipine affects liver function, and my gallbladder was removed and stones formed in the bile ducts. I already had to say goodbye to Enap, because it ultimately led to terrible spasms in the throat until I stopped breathing. Also a side effect, which was not immediately clear. Now you need to decide with your doctor what to do next. Most likely, you will have to refuse, no matter how sad it is.
Natalia
https://www.otzyvua.net/amlodipin/review-215309
After 2.5 months of taking amlodipine, my feet and ankles began to swell terribly. To its credit, the blood pressure has returned to normal. I don’t know what to do now and which device to switch to.
Byrin M. S.
https://protabletky.ru/amlodipine/#otzivi
Availability and price.
Questionable effectiveness and quality of the drug itself.
A well-known drug for the treatment of arterial hypertension, a constant member of the medicine team of every second pensioner. I can’t say that I prescribe him often; to be honest, I don’t trust him. Yes, if a patient cannot afford something of better quality or is simply greedy about his health, that’s his right, but if a person really wants to be treated and does not put his health in last place, I prescribe more modern drugs, even if they are more expensive.
Elena
https://www.piluli.ru/product/Amlodipin/review
This drug was recommended by a doctor for the treatment of hypertension. The medicine acts gently, does not cause drowsiness, and is not at all expensive. But the pressure does not decrease immediately, but somewhere after 6-8 hours, then it stabilizes and lasts for another 10-12 hours, then you need to take more. So when my blood pressure jumped, Capoten was recommended to me. Amlodipine must be taken. who smokes. to prevent atherosclerosis and strengthen the heart and coronary vessels.
Londina
https://citykey.net/review/nedorogoe-lekarstvo-ot-davleniya-no-pobochka-est
Advantages:
- Reduces blood pressure
- inexpensive drug
Flaws:
- Pressure jumps
- there are side effects
Oh, this hypertension! My grandmother, my mother, and my father are suffering from her, but she is getting younger and younger, and has already reached my husband. And he seemed to live without stress, happy with life, and here you go!
When my husband’s hypertension just started, the doctor prescribed him different pills, checking the effect and a sheet with blood pressure readings in order to choose the right medicine and dose. But my husband either took or didn’t take the pills, and the results were not so great. After all, for hypertension, you need to choose a drug and take it every day without skipping, because it does not cure, but only supports. As a result, the doctor prescribed the antihypertensive drug Amlodipine.
My husband started taking it every day at rare intervals, when he went fishing, drank there, and taking the drug was out of the question. I will also note that along with the pills, my husband also took beer, and occasionally something stronger. I kept a sheet of his measurements. And we both didn’t like that the pressure was fluctuating: after the pill it was ideal, but before the pill it was critical. The doctor promised that in a month everything would level out, but it never did.
After two weeks, my husband began to complain that he was getting sleepy more often, and physical and mental retardation appeared. It's all from these pills. It’s a pity that they are appointed for life, the husband is already turning into an old man. But you can’t not take it either: then the risk of stroke and heart attack increases.
(Anna22.04) Anna
https://www.imho24.ru/recommendation/53513/#review74118
The drug is good at reducing high blood pressure, but it can have dangerous side effects.
Advantages:
- Low price.
Flaws:
- Tachycardia may occur.
Doctors do not prescribe the drug Amlodipine as often as some other drugs against high blood pressure. This is primarily due to the fact that this drug has a lot of side effects, as well as a lot of strict contraindications for use. At one of the appointments, the cardiologist prescribed this medicine to my grandfather at a dosage of 10 mg. Due to the fact that this drug belongs to the group of slow calcium channel blockers, it can cause or worsen existing heart failure. That is why it is recommended to start taking it with minimal doses. You especially need to be careful in the first days of use for older people and those who have kidney problems. Indeed, in this category of patients, the drug may take longer to be eliminated from the body, which means that with an incorrectly selected dosage, a sharp drop in blood pressure is possible, which will last longer than in patients who do not have such problems. My grandfather was prescribed this drug by a cardiologist at a dosage of 10 mg. At a fairly low price, to save money, it is still recommended to buy a dosage of 20 mg and, if necessary, divide the tablet in half. For older people like my grandfather, this is an important factor.
After the first dose, a few hours later, the pressure dropped to critically low levels and lasted for about 12 hours. The next day the dosage was reduced to 5 mg, and the pressure was already normal. Also, this remedy is not suitable for relieving a hypertensive crisis, since it does not begin to act immediately, and the pressure may begin to decrease only a few hours after administration.
Unfortunately, the drug has a lot of side effects. And the most common is tachycardia, as well as the occurrence of various arrhythmias, including atrial fibrillation. Also, this drug very often causes peripheral edema. Therefore, it is better for people suffering from this problem to stop taking it. Elderly people are more likely to suffer from edema. When my grandfather's ankles became swollen, it became clear that this was due to this remedy. When I stopped taking the pills, everything immediately returned to normal, and, unfortunately, this cheap drug had to be replaced with another, but more expensive one.
(oksy36) Oksana
https://www.imho24.ru/recommendation/53513/#review73807
An effective drug for the treatment of angina pectoris and arterial hypertension
Advantages:
- Reduces vascular tone in angina and cardiac ischemia
- Normalizes heart rhythm
- Reduces the load on the heart during arterial hypertension
- Has a diuretic effect
- Has antioxidant abilities
Flaws:
- Severe side effects
- A number of contraindications
Good afternoon
In my review, I will share useful information about the drug Amlodipine. It was prescribed to my dad for angina pectoris and exacerbation of coronary heart disease. My dad has had heart problems for many years and periodically, exacerbations occur, especially if he gets nervous or it’s too hot outside.
In the complex treatment of angina pectoris, my father was prescribed this drug to regulate blood pressure and reduce attacks of angina pectoris. When the next attack begins, dad can’t breathe, there’s a stake in his heart, his blood pressure rises, he has tinnitus, and dizziness.
The principle of action of this drug is very simple.
This drug belongs to the category of calcium channel blockers. It blocks the passage of calcium ions through the membrane and prevents an increase in intracellular calcium concentration. Due to this, vascular tone decreases and blood pressure decreases.
The long-term effect of these tablets does not cause tachycardia, there is no fluctuation in blood pressure. Under the influence of this medicine, the blood vessels of the arteries dilate, the ischemia of the heart muscle decreases, and the course of angina pectoris is alleviated. As a result, the load on the heart is reduced and the heart's need for oxygen is reduced.
Amlodipine is used for arterial hypertension, angina pectoris, and chronic cardiac ischemia.
Dad took 1 tablet of 10 mg per day for 10 days. The first improvement in heart function was observed 3 hours after taking the drug.
After the course of treatment, my dad’s heart pain disappeared, his shortness of breath went away, and his blood pressure became close to normal.
The side effects are very strong. Dad developed insomnia, nausea, stomach pain, nervousness, and abnormal bowel movements.
Tablets with a dosage of 10 mg were prescribed to my dad by a cardiologist. If side effects are too pronounced, the dosage should be reduced to 5 mg per day.
In case of overdose, tachycardia may be observed.
At the moment, my dad takes this medicine only when absolutely necessary.
The drug is very effective, but has a negative effect on overall well-being. I advise you to take it only under the supervision of a doctor.
Nina
https://www.medcentre.com.ua/amlodipin.html
I took Amlodipine for high blood pressure. He helped me very well, but after a couple of weeks my legs began to swell and there was pain in the bones of my feet. And this led to skin rashes. I thought that these were side effects from the drug Amlodipine. I went to the doctor and he stopped this drug. Of course, I was very upset, since he helped me well with blood pressure. But such side effects are also not good. In general, I had to be treated for dermatitis and cope with swelling of the legs.
Svetik
https://zhivizdorovim.ru/lekarstva/serdechno-sosudistie/741-amlodipin.html#comment-839
With long-term use of the drug Amlodipine, the skin on the hands and face turns red, peels and irritates so that creams do not help. It keeps my blood pressure down, but I can’t drink all the time! When discontinued, peeling on the face goes away in 3 days, on the hands it takes longer.
Informative reviews from doctors
Not only patients share their opinions about the effectiveness of a particular drug on forums. Which is better according to doctors' reviews - Lozap or Amlodipine, Lerkamen - you can find out from the opinions left on specialized sites:
- V. Sokolov: “Amlodipine is usually the first choice drug
. It acts in approximately 30 minutes, and the maximum therapeutic concentration of the active substance is created in the bloodstream after 3 hours. Patients say that after taking even one tablet, their blood pressure does not rise for 24 hours.” - G. Mironenko: “Compared to Amlodipine, Lozap acts more slowly - maximum hypotensive activity is observed only after six hours, and also lasts for a day
. But with a course of taking it, it is possible to avoid surges in blood pressure for a month and a half after discontinuation.” - E. Vasiliev: “I noticed that Amlodipine and Lerkamen have a lot in common in terms of duration of action
. Both drugs quickly accumulate in the bloodstream and penetrate to target organs. And their pharmacological effects persist throughout the day.”
When prescribing a drug to a patient, the cardiologist also focuses on the method of eliminating metabolites. For example, if he has kidney problems, then Lozap is preferable.
Difference in instructions for use
According to the instructions for use attached to the packages of Lozap, Lerkamen, Amlodipine, there are no clear instructions at what pressure to take them. The cardiologist is guided not by the values of the tonometer, but by the severity of the symptoms of hypertension. The fact is that there is no general concept of “normal blood pressure”. Many people feel quite comfortable throughout their lives at 130/90 Hg. Art. and even higher. If such a condition is physiological for a person, then taking antihypertensive drugs is not required.
Doctors try to choose drugs that are easy to use. And Amlodipine, and Lozap, and Lerkamen fully meet this requirement:
- Amlodipine
is taken once a day, 50 mg per day, in complicated cases - 100 mg; - Lerkamen
take once every 24 hours, if the pressure does not decrease enough, then after two weeks the dose is doubled; - Lozap
is taken 5 mg once a day, if necessary, the dose is doubled, and in some cases reduced to 2.5-5 mg to maintain pressure at an optimal level.
Only Lerkamen is advisable to use before meals for rapid penetration of the active substance into the systemic bloodstream. The therapeutic effects of Amlodipine and Lozap do not depend on the presence of food in the stomach. All tablets cannot be crushed or chewed - they must be swallowed whole with clean water.
Place of amlodipine in cardiological practice
Calcium antagonists (CAs) have been used in clinical practice for about four decades and are currently one of the most commonly prescribed drugs in cardiology. Such widespread use of AKs in clinical practice is associated with their high antihypertensive efficacy, metabolic neutrality and good tolerability [1, 14]. In recent years, calcium antagonists of the dihydropyridine, phenylalkylamine and benzothiazepine series have been present on the Russian pharmaceutical market, but dihydropyridine derivatives have found the most widespread use in clinical practice: nifedipine, amlodipine, isradipine, nitrendipine, lacidipine, felodipine, lercanidipine.
Today, the most prescribed representative of the calcium antagonists of the dihydropyridine series is amlodipine (Amlovas, Amlotop, Vero-Amlodipine, Kalchek, Cardilopin, Cordi Cor, Norvasc, Normodipin, Omelar Cardio, Stamlo, Tenox).
Amlodipine is a third-generation dihydropyridine calcium channel antagonist that blocks slow calcium channels (L-type channels) and prevents intracellular hypercalcemia and smooth muscle cell contraction, exerting a vasodilatory effect. It has a long-lasting effect, which allows it to be used once a day.
Pharmacokinetics
When taken orally, amlodipine is slowly and almost completely absorbed from the gastrointestinal tract, regardless of food intake. The bioavailability of amlodipine is high and ranges from 60 to 80%. The volume of distribution of the drug is on average 20–21 l/kg body weight, which is significantly more than that of other representatives of the dihydropyridine series. In serum, 95–98% of the drug dose is bound to plasma proteins. The maximum concentration in the blood is reached 6–12 hours after administration. The duration of action is due to its slow release from connection with receptors. Biotransformation to inactive metabolites occurs in the liver. The drug is excreted in the urine (about 10% unchanged and about 60% in the form of inactive metabolites) and in feces. The half-life is 35–50 hours. A stable equilibrium concentration (steady-state) is achieved after 7–8 days of taking the drug. With impaired liver function, the elimination time of amlodipine increases, which is also typical for other dihydropyridine calcium antagonists. Amlodipine does not cause impaired glucose tolerance and can be used in patients with diabetes mellitus.
Pharmacodynamics
Effect on blood pressure (BP) and heart rate (HR)
The effect of amlodipine (in the form of blocking slow calcium channels and reducing intracellular hypercalcemia) is 80 times more pronounced in relation to vascular smooth muscle cells compared to contractile myocardium. Thus, the decrease in blood pressure under the influence of amlodipine occurs precisely due to peripheral vasodilation. Amlodipine has a pronounced hypotensive effect on both systolic (SBP) and diastolic blood pressure (DBP).
Amlodipine has a long-term hypotensive effect due to its long half-life (35–50 hours), which allows it to control blood pressure evenly throughout the day, including preventing early morning rises in blood pressure, regardless of the time of taking the drug (morning or evening once a day) [8, 19]. In a study by Hayduk K. et al. during a break in treatment, blood pressure remained within normal values even on the second day of drug withdrawal [11]. The maximum hypotensive effect during therapy with 5 mg of amlodipine occurs only on the 6th week of drug use, which makes early dose increases inappropriate in case of incomplete control of blood pressure levels [30]. The drug has a dose-dependent effect on blood pressure levels and is characterized by a linear dose-concentration relationship in blood plasma. Thus, in a study on healthy volunteers, DBP decreased when measured while standing by 1.1; 4.8 and 8.0 mm Hg. Art., when using 2.5; 5 and 10 mg of amlodipine, respectively [17].
With the development of the hypotensive effect of amlodipine, there is no change in heart rate, which sets the drug apart from other representatives of the dihydropyridine series. In addition, the drug is well tolerated by patients. Side effects include swelling of the legs and hyperemia, which is characteristic of all AKs of the dihydropyridine series.
Effect on myocardial ischemia
The antianginal effect is determined by the peculiarity of the mechanism of action and is due to the coronary-lytic effect of the drug, which also determines the most preferable patient population. The effect of the drug is maximum in patients with severe vasospasm [21]. However, amlodipine is also widely used for the treatment of stable angina pectoris, significantly reducing the frequency, duration and severity of episodes of myocardial ischemia [16, 27]. One of the possible beneficial protective effects of amlodipine on the state of the myocardium after an episode of ischemia is considered to be its ability to reduce calcium overload of cells, which is the cause of myocardial damage [10]. An advantageous difference between amlodipine and earlier calcium antagonists is its lack of influence on heart rate, an increase in which during physical activity is one of the triggers for ischemia.
The CAPE study [3] studied the anti-ischemic properties of amlodipine in patients with coronary artery disease. During control 48-hour ECG monitoring, a decrease in the number of episodes of myocardial ischemia was observed. When amlodipine was added to traditional therapy with b-blockers and nitrates, no increase in episodes of arrhythmias was observed.
Effect on the sympathetic autonomic nervous system and plasma renin activity
Activation of the sympathetic component of the autonomic nervous system is an undesirable side effect of dihydropyridine calcium antagonists due to their direct mechanism of action. However, a peculiarity of the action of amlodipine is the lack of activation of the sympathetic nervous system and the development of reflex tachycardia. Thus, when determining norepinephrine in the blood of patients taking amlodipine, there was no increase in its level compared to the baseline [23]. During spectral analysis, no increase in LF/HF was observed [24]. The lack of effect of amlodipine on plasma renin activity and norepinephrine levels in patients with arterial hypertension (AH) was shown in a study by Susaguri et al. [24].
Effect on left ventricular myocardial mass
The cardioprotective effect and ability of amlodipine to reduce left ventricular myocardial mass were demonstrated in the randomized, double-blind, placebo-controlled TOMHS study, which compared 5 antihypertensive drugs: a diuretic (chlorthalidone), a β-blocker (acebutolol), a calcium channel antagonist (amlodipine), ACE inhibitor (enalapril), α-adrenergic receptor antagonist (doxazosin). When studying the dynamics of changes in left ventricular myocardial mass, it turned out that the most pronounced decrease was observed in the amlodipine and chlorthalidone groups, compared with the acebutolol and placebo groups, and led to a decrease in the risk of developing cardiovascular complications in hypertensive patients with left ventricular hypertrophy.
Effect on the progression of vascular atherosclerosis
The beneficial effect of AA on the state of the vascular endothelium was confirmed in the multicenter, prospective, randomized, double-blind, placebo-controlled PREVENT study [22], which assessed changes in the degree of atherosclerotic lesions of the coronary arteries and the thickness of the intimomedial layer of the carotid arteries during the administration of amlodipine. There was a pronounced effect of amlodipine on the progression of atherosclerosis in the carotid arteries, detected using ultrasonography. At the same time, in the amlodipine group, regression of the intimomedial layer was observed by 0.046 mm, and in the control group, a thickening of 0.011 mm was observed. Currently, a correlation has been proven between the degree of thickening of the intimomedial layer of the carotid arteries and the incidence of myocardial infarction (MI) and cerebral stroke.
Clinical experience
Arterial hypertension
Antihypertensive effect
Amlodipine effectively reduces SBP and DBP levels both in monotherapy and as part of combination therapy. Amlodipine is a competitive drug when compared with other calcium antagonists and drugs from other classes of antihypertensive drugs [9].
When comparing the effect of amlodipine with the effect of other calcium antagonists, its greater effectiveness in relation to blood pressure levels is shown in comparison with verapamil and diltiazem. Thus, in a study by Watts RW et al. [29] compared amlodipine (5–10 mg) and controlled-release diltiazem (180–360 mg), and mean daily blood pressure decreased with amlodipine to 137/84 mmHg. Art., and when using diltiazem - up to 143/86 mm Hg. Art. In numerous comparisons of amlodipine with other dihydropyridine calcium antagonists, it had a comparable but significantly longer antihypertensive effect [8, 13]. At the same time, the advantageous advantage of the drug over other dihydropyridine calcium antagonists is the lack of its effect on heart rate, which allows it to be prescribed to patients with tachysystole.
In terms of reducing the risk of developing cardiovascular complications and improving the prognosis for hypertension (the main goal in the treatment of this disease), amlodipine, according to studies such as ALLHAT [25] and VALUE [12], was comparable in effectiveness to ACE inhibitors and angiotensin receptor blockers, and in some respects even better. Compared with valsartan, an antihypertensive therapy regimen based on amlodipine significantly reduced the incidence of MI by 19% in hypertensive patients with numerous concomitant risk factors.
Organoprotective effects
The angioprotective effects of amlodipine were demonstrated in the PREVENT study [22]. It was shown that in patients with coronary heart disease (CHD), amlodipine contributed to a decrease in the intima-media thickness index compared to a group of patients with CHD who received placebo. Perhaps it is the slowdown in the progression of carotid artery atherosclerosis that explains the data obtained in many studies indicating a particularly pronounced reduction in the incidence of cerebrovascular accidents during treatment with calcium antagonists [28]. The results of the CAMELOT study [18] allow us to judge the antiatherosclerotic effect of amlodipine in relation to the coronary arteries.
The most important element of organ protection in the treatment of patients with hypertension is the prevention of stroke. The ASCOT study compared the effectiveness of antihypertensive therapy based on the use of the calcium antagonist amlodipine followed by the addition of the ACE inhibitor perindopril with therapy based on the use of the beta-blocker atenolol and the thiazide diuretic bendroflumethiazide. Both groups showed a comparable reduction in blood pressure, but in the amlodipine and ACE inhibitor group the relative risk of stroke was 23% lower than in the atenolol and diuretic group (p = 0.0003) [4]. The results of the ASCOT study suggest that, in addition to their hypotensive effects, calcium antagonists and ACE inhibitors have additional properties that may reduce the risk of cerebrovascular complications.
The most important characteristic of an antihypertensive drug is its metabolic effects, in particular, the effect on carbohydrate metabolism [26]. Since the development of diabetes in hypertensive patients significantly increases the risk of cardiovascular complications [7], the selection of antihypertensive therapy must be carried out taking into account its effect on the risk of diabetes. Calcium antagonists reduce the incidence of new cases of diabetes compared to diuretic therapy [12, 25]. In the ALLHAT study, depending on the frequency of new cases of diabetes in the comparison groups, the tested drugs were distributed as follows: chlorthalidone > amlodipine > lisinopril [25]. However, the beneficial effect of amlodipine was especially evident in the ASCOT study [4], where, during treatment with amlodipine in combination with perindopril, the likelihood of developing new cases of diabetes was 30% less than in the group of patients receiving therapy with atenolol and the thiazide diuretic bendroflumethiazide.
The results of major studies (PREVENT, INSIGHT, ELSA, CAMELOT, etc.) served as a prerequisite for expanding the indications for the use of AC in patients with hypertension and introducing into the new recommendations the presence of atherosclerosis of the carotid and coronary arteries in patients with hypertension as one of the indications for the primary use of AC dihydropyridine group [26]. In addition, in the 2007 European recommendations, calcium antagonists from the group of dihydropyridine derivatives (amlodipine) are indicated as the drugs of choice in elderly patients with isolated systolic hypertension, angina pectoris, left ventricular myocardial hypertrophy, peripheral vascular diseases, pregnancy, atherosclerosis of the carotid and coronary arteries.
Cardiac ischemia. Angina pectoris
Amlodipine has a pronounced coronary effect due to its high selectivity for smooth muscle cells of arterioles. The steal syndrome that occurs when using short-acting AKs is much less pronounced in long-acting drugs, in particular amlodipine. Amlodipine is widely used for the treatment of stable angina pectoris, both in monotherapy and (more often) and as part of combination therapy. Amlodipine also has a beneficial effect when used in patients with a pronounced dynamic component of coronary obstruction [3].
The anti-ischemic effects of amlodipine, its ability to reduce the frequency of episodes of ST segment depression, the total ischemic time (as measured by ECG), as well as the frequency of painful ischemic episodes and the frequency of additional use of short-acting nitrates, have been demonstrated in a number of studies, including the multicenter CAPE study [5, 6].
The effect of amlodipine on the prognosis of patients with coronary artery disease was assessed in the PREVENT study [22]. There was a decrease in the number of hospitalizations caused by destabilization of the course of angina pectoris and chronic heart failure (CHF); reduction in the number of myocardial revascularization operations (53 compared with 85 in the placebo group), regardless of the use of beta-blockers, nitrates or lipid-lowering therapy.
In a meta-analysis, Kloner RA et al. [15] assessed the safety of calcium channel antagonists. Comparative and non-comparative studies of amlodipine and nifedipine GITS were included. It was shown that in patients receiving amlodipine, overall cardiovascular mortality, the incidence of acute myocardial infarction and progression of coronary artery disease were significantly lower than similar indicators for other calcium antagonists.
According to the CAMELOT study, amlodipine compared with placebo by 31% (p < 0.003) reduced the incidence of adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, coronary revascularization, the need for hospitalization due to angina, heart failure, fatal or non-fatal stroke or peripheral arterial disease) mainly due to a decrease in the rate of revascularization [18].
Chronic heart failure
The randomized, double-blind, placebo-controlled study PRAISE I [20] studied the effects of amlodipine in patients with CHF. The study included 1153 patients with an ejection fraction of less than 30% and CHF of ischemic and non-ischemic origin. Amlodipine vs placebo led to a 9% reduction in the total number of cardiovascular complications and a 16% reduction in the risk of sudden death. Moreover, the change concerned exclusively patients with non-ischemic heart failure, who experienced a 31% reduction in the total number of cardiovascular complications and a 46% reduction in the risk of sudden death when using amlodipine. The PRAISE II study showed a reduction in clinical symptoms and plasma norepinephrine levels with amlodipine in patients with dilated cardiomyopathy. A number of authors associate this effect of amlodipine with inhibition of NO hyperproduction and a decrease in myocardial damage.
Conclusion
The antagonist of slow L-type calcium channels from the group of dihydropyridines, amlodipine, is effective in mono- and combination therapy in patients with hypertension, coronary artery disease with severe coronary spasm, both in monotherapy and in combination with other antianginal and antihypertensive drugs [2]. The effect of amlodipine on cardiovascular risk is confirmed by the results of a large number of large international multicenter randomized, placebo-controlled clinical trials (
.).
Amlodipine is a long-acting drug, which neutralizes the sharp hemodynamic changes characteristic of the initial period of absorption of short-acting AA.
An important feature of the action of amlodipine is the lack of influence on heart rate, which expands the possibilities of using the drug.
Amlodipine has a good range of safety and tolerability; the percentage of adverse reactions when using it does not significantly exceed the placebo effect.
For questions regarding literature, please contact the editor.
T. E. Morozova , Doctor of Medical Sciences, Professor V. L. Zakharova , Candidate of Medical Sciences MMA named after. I. M. Sechenova , Moscow
Spectra of therapeutic effects
Amlodipine is prescribed by cardiologists to patients with arterial hypertension as part of complex therapy or as monotherapy, stable and vasospastic angina. It is used to eliminate severe symptoms of acute or chronic coronary artery disease, heart failure, including swelling of the face and legs.
Another indication for treatment with Amlodipine is bronchial asthma, during attacks of which negative reactions from the cardiovascular system are noted.
The narrowest list of indications for Lerkamen is essential hypertension of I and II severity.
Lozap is the most popular drug in cardiology practice. It is included in therapeutic regimens for patients suffering from the following diseases:
- arterial hypertension;
- chronic heart failure;
- diabetic nephropathy, the course of which is complicated by hypercreatininemia and proteinuria.
Cardiologists especially value Lozap for its ability to be used not only for therapeutic purposes, but also for preventive purposes. Thus, with its help it is possible to avoid the development of complications in hypertension or left ventricular hypertrophy.
Amlodipine: leader of medical recommendations in the treatment of patients with cardiovascular diseases
AKs are a large group of drugs, the main property of which is the ability to reversibly inhibit the flow of calcium through slow calcium channels. These drugs have been used in cardiology since the late 70s of the last century and have now gained such wide popularity that in most developed countries they occupy one of the first places in terms of frequency of prescription among drugs used to treat CVD. This is due, on the one hand, to the high clinical effectiveness of calcium antagonists, on the other hand, to the relatively small number of contraindications to their use and the relatively small number of side effects they cause. Among AKs, amlodipine (Amlotop, Makiz-Pharma CJSC) occupies a special place. Amlotop is the leader in prescription by both cardiologists and therapists in the entire C08C group (selective blockers of “slow” calcium channels), according to the analytical company Comcon Pharma, Medi-Q, (2010). Amlotop has the most long-lasting effect (both antihypertensive and anti-ischemic) and has been successfully studied in many clinical studies. Amlodipine was introduced into clinical practice in 1992 for the treatment of arterial hypertension and coronary heart disease. By selectively blocking the flow of calcium ions through slow channels of vascular smooth muscle cells, amlodipine reduces vascular peripheral resistance without affecting cardiac contractility. The decrease in blood pressure is not accompanied by reflex tachycardia due to the slow development of the hypotensive effect, and there is no increase in the release of catecholamines. Amlodipine does not affect sinus node conduction and intracardiac conduction. Experimental and clinical data have been obtained on its beneficial effect on platelet aggregation and the ability to slow down the rate of development of atherosclerosis. The peculiarities of the action of amlodipine are determined by its pharmacokinetic parameters. It is quickly and completely absorbed from the gastrointestinal tract and is significantly bound to protein (95–98%). The maximum concentration of the drug in the blood is observed after 6–12 hours, the half-life is 35–50 hours, while a constant concentration in the blood is achieved on the 7–8th day of administration. The drug is well tolerated, causing few side effects. Used in combination with other antianginal and antihypertensive drugs [1–4]. Classification of calcium antagonists Based on their chemical structure, they are distinguished: dihydropyridine calcium antagonists (nifedipine, amlodipine, nicardipine, felodipine, lacidipine, etc.), benzothiazepine derivatives (diltiazem) and phenylalkylamines (verapamil) (Tables 1 and 2). The use of amlodipine in arterial hypertension Currently, AKs are one of the main classes of drugs used to treat hypertension. The decrease in blood pressure under the influence of Amlotop (amlodipine) occurs due to peripheral vasodilation, which is the result of blocking slow calcium channels and a decrease in the level of intracellular calcium in vascular smooth muscle cells. According to comparative studies (ALLHAT, TOMHS, VALUE), amlodipine demonstrated an antihypertensive effect equal to the antihypertensive activity of ACE inhibitors, angiotensin II antagonists, diuretics and β-blockers. Amlotop has a pronounced hypotensive effect on both systolic and diastolic blood pressure. However, the degree of blood pressure reduction varies, according to different authors. Thus, in a study by Horwitz LD et al. [2] when using 5–10 mg of amlodipine for 10 weeks, the decrease in systolic pressure was 13.1 mm Hg, diastolic pressure was 12.2 mm Hg, and in the study by Habeler G. et al. [5] when using the same dose of amlodipine for 27 months, systolic blood pressure decreased by 30.5 mm Hg, and the decrease in diastolic blood pressure was 20.7 mm Hg. (Table 3). Amlotop has a long-term hypotensive effect due to its long half-life (35–50 hours), which allows it to control blood pressure evenly throughout the day. This leads to a relatively greater effectiveness of the drug in controlling the early morning rise in blood pressure, regardless of the time of administration (morning or evening once a day) [3–6]. In a study by Leenen FH et al. during a break in treatment, blood pressure remained within normal limits even on the second day after discontinuation of the drug. The maximum hypotensive effect during therapy with 5 mg of Amlotop occurs only in the 6th week of drug use, which makes early dose increases inappropriate in case of incomplete control of blood pressure levels. The drug has a dose-dependent effect on blood pressure levels and is characterized by a linear dose-concentration relationship in blood plasma. Thus, in a study on healthy volunteers, diastolic blood pressure decreased when measured while standing by 1.1; 4.8 and 8.0 mm Hg, when using 2.5, 5 and 10 mg of amlodipine, respectively [10–12]. Amlotop, in doses usually used to treat hypertension, has a very beneficial effect on renal function. The use of Amlotop in renal failure is therefore not contraindicated. With the development of the hypotensive effect of Amlotop, there is no change in the heart rate, which sets the drug apart from other representatives of the dihydropyridine series [29]. The use of amlodipine for coronary heart disease The antianginal effect of Amlotop is determined by the coronary-lytic effect of the drug, which is maximum in patients with a pronounced spastic component of coronary obstruction. An additional beneficial protective effect of Amlotop on the state of the myocardium during an ischemic episode is considered to be its ability to reduce calcium overload of cells, which is the cause of myocardial damage [2,7,22]. Amlotop is widely used for the treatment of stable angina, significantly reducing the frequency, duration and severity of ischemic episodes. An advantageous difference between amlodipine and earlier calcium antagonists is its lack of influence on heart rate, an increase in which during physical activity is one of the triggers of ischemia [2,9,24]. The CAPE study [8,18] assessed the effect of amlodipine on the duration and frequency of myocardial ischemic episodes in patients with coronary artery disease. During the control 48-hour ECG monitoring, a decrease in the number of ischemic episodes was observed. When assessing the possible proarrhythmogenic effect of the drug in patients with stable angina, when amlodipine was added to traditional therapy with β-blockers and nitrates, no increase in episodes of arrhythmia was observed. The effect of amlodipine therapy on the prognosis of patients with coronary artery disease was assessed in the PREVENT study. There was a decrease in the number of hospitalizations due to destabilization of angina pectoris and chronic heart failure (61 in the amlodipine group and 88 in the placebo group). Also, with the use of amlodipine, a decrease in the number of myocardial revascularization operations was observed (53 compared with 85 in the placebo group), regardless of the use of b-blockers, nitrates or lipid-lowering therapy. The frequency of anginal attacks decreased from 85 to 60 [2,23]. A comparative assessment of the effect on cardiovascular mortality of the angiotensin receptor antagonist valsartan and the calcium antagonist amlodipine is carried out in the VALUE study. 14,400 patients with arterial hypertension and additional risk factors (hypercholesteremia >6.5 mmol/l, serum creatinine >1.2 mg/dl, ECG signs of left ventricular hypertrophy, type 2 diabetes mellitus, coronary artery disease or stroke in history) were randomized. In the amlodipine group, blood pressure control was better throughout the observation period. The incidence of the study's main composite outcome did not differ between the two treatment groups. The incidence of heart failure and stroke, the level of overall mortality in the groups also did not differ significantly. However, the relative risk of myocardial infarction was 19% lower (p=0.02) in the amlodipine group. In the ALLHAT study, one of the directions was a comparative assessment of the effect of amlodipine on the incidence of non-fatal myocardial infarction and coronary death, comparing four classes of antihypertensive drugs: diuretics, calcium antagonists, a-blockers and ACE inhibitors in relation to the reduction of cardiovascular morbidity and mortality in patients hypertension with hypercholesterolemia [2]. The ALLHAT results justify an increased role for amlodipine in the treatment of patients with hypertension and a high risk of cardiovascular complications. In patients with hypertension who received the AC amlodipine or the diuretic chlorthalidone, regardless of gender, age, race, or the presence of diabetes mellitus, there were no differences in the incidence of primary outcomes (cases of fatal ischemic heart disease and nonfatal myocardial infarction) and in the incidence of each of secondary outcomes (overall mortality, fatal and non-fatal strokes, coronary artery disease in general and cardiovascular complications in general). In addition, when analyzing components of secondary outcomes, there were no differences between the amlodipine and chlorthalidone groups in the incidence of angina pectoris, peripheral artery disease, and coronary revascularization. In the double-blind, randomized study CAMELOT 1991, patients with coronary artery disease with angiographically confirmed stenoses in the coronary arteries and diastolic pressure below 100 mm Hg. Amlodipine was prescribed at a dose of 10 mg/day, enalapril 20 mg/day, or placebo. Over 2 years of observation, a significant decrease in blood pressure was noted in both groups of antihypertensive therapy (amlodipine by 4.8/2.5 mm Hg, enalapril by 4.9/2.4 mm Hg). Cardiovascular complications were reported in 23.1% of cases in the placebo group, in 16.6% of cases in the amlodipine group and in 20.2% of cases in the enalapril group. In the amlodipine group, the risk of cardiovascular complications (cardiovascular death, nonfatal myocardial infarction, coronary revascularization, the need for hospitalization due to angina pectoris, fatal or nonfatal stroke, peripheral arterial disease) decreased by 31% (p = 0.003), and in the amlodipine group enalapril - by 15%, but these differences were not statistically significant. The PREVENT study revealed a decrease in the number of hospitalizations due to worsening angina pectoris and chronic heart failure (61 in the amlodipine group and 88 in the placebo group), a decrease in the number of myocardial revascularization operations (53 in the amlodipine group and 85 in the placebo group), and a decrease in the frequency of anginal attacks (in the amlodipine group from 85 to 60) regardless of the use of β-blockers, nitrates or lipid-lowering drugs [23]. The results of the double-blind, placebo-controlled CAPARES study [2] demonstrated the high effectiveness of amlodipine in the prevention of restenosis after coronary angioplasty (Table 4). Amlotop has the ability to slow down platelet aggregation, which is important for the prevention of exacerbations of coronary artery disease. At the same time, it is of great importance that the aggregation ability of platelets is maximum in the morning, when the number of sudden deaths and myocardial infarctions reaches a peak level. Taking this into account, the use of amlodipine in the combination of arterial hypertension and coronary artery disease is most justified, because the drug helps slow down platelet aggregation within 24 hours (Selwyn et al., 1991). In a meta-analysis, Kloner RA et al. [16] assessed the safety of calcium channel antagonists. Comparative and non-comparative studies of amlodipine and nifedipine GITS were included. It was shown that in patients receiving amlodipine, overall cardiovascular mortality, the incidence of acute myocardial infarction and progression of coronary artery disease were significantly lower than similar indicators for other calcium antagonists. Effect of amlodipine on the autonomic nervous system and plasma renin activity Activation of the sympathetic component of the autonomic nervous system is an undesirable side effect of dihydropyridine calcium antagonists due to their mechanism of action (reflex activation). However, even with prolonged use of Amlotop in concentrations necessary for sustainable normalization of systolic and diastolic pressure, there are practically no changes in the concentration of norepinephrine, adrenaline, renin or atrio-natriuretic factor (ANF) in the blood plasma (Table 5). Thus, a feature of Amlotop’s action is the absence of activation of the sympathetic nervous system and the development of reflex tachycardia [28–29]. A small and unreliable increase in the level of aldosterone in the blood plasma is an effect inherent in other calcium antagonist drugs, but with Amlotop it is observed only in the elderly. Sometimes a small and unreliable increase in glycemia also occurs, blood plasma lipids do not change, and the concentration of total cholesterol and triglycerides decreases (Table 6). Effect of amlodipine on left ventricular myocardial mass In the randomized, double-blind, placebo-controlled study TOMHS [1,2], 5 antihypertensive drugs were compared: a diuretic (chlorthalidone), a β-blocker (acebutolol), a calcium channel antagonist (amlodipine), an ACE inhibitor (enalapril maleate) , an α-adrenergic receptor antagonist (doxazosin) and their possible effect on the mass of the left ventricular myocardium. The study was based on a proven connection between an increase in the size of the left ventricle and an increased risk of developing cardiovascular complications. The study was conducted for more than four years on 902 patients with mild hypertension of 1-2 degrees. At the first stage, patients were offered one of 5 antihypertensive drugs (including amlodipine at a dose of 5 mg/day) or placebo, and then at the second stage, if blood pressure control was inadequate, a second drug was added (chlorthalidone in 5 groups of patients and enalapril in the group previously receiving chlorthalidone). All drugs were prescribed once a day in the morning. Follow-up echocardiographic studies were performed at baseline, 3, 12, 24, 36 and 48 months. During the study, a significant decrease in blood pressure levels was observed, and in the acebutolol and amlodipine groups the percentage of changes in therapy was the smallest, i.e. Adequate blood pressure control was observed throughout the entire 4-year observation period at drug doses not exceeding the initial ones. When studying the dynamics of changes in left ventricular myocardial mass, it turned out that the most pronounced decrease was observed in the amlodipine and chlorthalidone groups compared with the acebutolol and placebo groups. During the entire observation, it turned out that amlodipine reduces the mass of the left ventricular myocardium, which may reduce the risk of developing cardiovascular complications in patients with arterial hypertension and left ventricular hypertrophy (Tables 7, 8). The effect of amlodipine on the progression of vascular atherosclerosis The PREVENT study assessed changes in the degree of atherosclerotic lesions of the coronary arteries and the thickness of the intima-medial layer of the carotid arteries during the administration of amlodipine. The study included 825 patients with coronary artery disease confirmed by coronary angiography [23]. Patients received amlodipine at a dose of 5 mg, which, if well tolerated, was increased to 10 mg. As a result of the study, no significant differences were obtained in both study groups (active treatment and control) in relation to the progression of atherosclerotic stenosis of the coronary vessels. In contrast, amlodipine significantly slowed the progression of atherosclerosis in the carotid arteries, detected by ultrasonography. At the same time, in the amlodipine group, regression of the intima-medial layer was observed by 0.046 mm, and in the control group, thickening by 0.011 mm. Currently, a correlation has been proven between the degree of thickening of the intima-medial layer of the carotid arteries and the incidence of myocardial infarction and cerebral stroke. Also, the PREVENT study showed good tolerability of the drug, which was previously noted by other researchers, with the frequency of adverse reactions comparable to the placebo group (79% for amlodipine and 83% for placebo). Additional prescription of angiotensin-converting enzyme inhibitors in the amlodipine group was observed half as often as in the placebo group. The CAMELOT study [2] additionally examined the effect of amlodipine and enalapril therapy on the progression of atherosclerosis using intravascular ultrasound in 274 patients. It turned out that in the amlodipine group there was no progression of atherosclerosis, in the enalapril group there was a tendency towards its progression (p=0.08), and in the placebo group there was a significant progression of atherosclerosis (p<0.0001). Moreover, when analyzing participants from the amlodipine group with initially elevated blood pressure, the slowdown in the progression of atherosclerosis was significant (p = 0.02). The use of amlodipine for chronic heart failure in a randomized double -blind placbo -controlled study of Praise I evaluate the influence of the new calcium amlodipine antagonist on patients with chronic heart failure. The study included 1153 patients with chronic heart failure of ischemic and non -ischemic genesis and an emission faction of less than 30%. The results of the study showed a decrease in the total number of cardiovascular complications by 9%, a reduction in the risk of sudden death by 16% in the amlodipine group in comparison with the placebo. The Praise II study evaluated the role of amlodipine in the therapy of chronic heart failure of nonsense (dilatation cardiomyopathy). A decrease in clinical symptoms and level of plasma norepinephrine when using amlodipine in patients with dilatation cardiomyopathy is shown. A number of authors associate this effect of amlodipine with inhibiting hyperproduction NO and a decrease in myocardial damage [2]. The drug interaction of some kind of dose of amlotope is not required when used with thiazide diuretics, β -adrenoisters, and ACE inhibitors. A favorable effect on the level of blood pressure is shown while the assignment of amlotope with A -adreno -blocking. The Schwartz JB study [27] assessed the effect of amlodipin on the pharmacological profile of digoxin in healthy volunteers. A change in the equilibrium concentration of digoxin (Steady - State), as well as blood pressure or heart rate when joint use of drugs, is not shown. The conclusion existing scientific data indicates that amlodipine retains the position of the main drug for the constant treatment of patients with hypertension, coronary heart disease and chronic heart failure. The studies prove the prolonged hypotensive effect of amlodipine, which provides very effective blood pressure control. The antianginal and protective properties in relation to the myocardium determine the beneficial effect of amlodipin on the forecast, the number of hospitalizations and the survival of patients with coronary heart disease and heart failure. Amlodipine reduces the mass of myocardial ventricular myocardium, slows down the progression of atherosclerosis, which reduces the risk of cardiovascular complications in cardiological patients. In addition, amlodipine does not affect the frequency of heart contractions, which levels sharp hemodynamic shifts. In numerous studies, good tolerance of amlodipine was observed, and the percentage of adverse reactions during its use did not significantly exceed a similar indicator in the control group. Such a favorable profile of amlodipine determines its active use in clinical practice. However, a special place in terms of purpose among all calcium antagonists is occupied by Amlotop Makiz -Farma CJSC, which has been the leader of medical recommendations for both cardiologists and therapists for several years in a row. This indicates the high efficiency of amlotope in cardiological patients. In addition, the drug has a minimum number of side effects and is available in price.
Literature 1. Zhelnov V.V. et al. Modern long-acting calcium antagonists in clinical practice. RMJ 2008, volume 16, no. 7 (317), pp. 487–491. 2. Nedogoda S.V. The role of amlodipine in the treatment of coronary heart disease. Consilium medicum 2008, vol. 10, no. 5, pp. 100–104. 3. Ajayi AA et al. The efficacy and tolerability of amlodipine and hydrochlorothiazide in Nigerians with essential hypertension. J Natl Med Assoc 1995 87(7) 485–8. 4. Broadhurst P. et al. Intra-arterial monitoring of the antihypertensive effects of once-daily amlodipine. J Hum Hypertens 1992 6 Suppl 1 9–12. 5. Brown MJ et al. Alpha-blockade and calcium antagonism: an effective and well-tolerated combination for the treatment of resistant hypertension. J Hypertens 1995 13(6) 701–7. 6. Burris JF et al. Double–blind comparison of amlodipine and hydrochlorothiazide in patients with mild to moderate hypertension. J Cardiovasc Pharmacol 1988 12 Suppl 7 98–102. 7. Chahine RA et al. Randomized placebo–controlled trial of amlodipine in vasospastic angina. L Am Coll Cardiol 1993 21(6) 1365–70. 8. Detry JM Amlodipine and the total ischemic burden: Circadian Anti–Ischemia Program in Europe (CAPE) trial – Methodology, safety and tolerance. Cardiology 1994 85 Suppl 2 24–30. 9. Deanfield JE et al. Amlodipine reduces transient myocardial ischemia in patients with coronary artery disease: double–blind Circadian Anti–Ischemia Program in Europe (CAPE Trial). J Am Coll Cardiol 1994 24(6) 1460–7. 10. Frishman WH et al. Amlodipine versus atenolol in essential hypertension. Am J Cardiol 1994 73(3) 50–4. 11. Habeler G. et al. Effectiveness and tolerance of amlodipine in treatment of patients with mild to moderate hypertension. Results of long–term study with a new calcium antagonist. Wien Klin Wochenschr 1992 104(1) 16–20. 12. Hayduk K. et al. Is initial dose titration of amlodipine worthwhile in patients with mild to moderate hypertension? Current Med Res Opinion 1999 15(1) 39–45. 13. Horwitz LD et al. Comparison of amlodipine and long-acting diltiazem in the treatment of mild or moderate hypertension. Am J Hypertens 1997 10(11) 1263–9. 14. Ishimitsi T. et al. Amlodipine, a long-acting calcium channel blocker, attenuates morning blood pressure rise in hypertensive patients. Clin Exp Pharmacol Physiol 1999 26(7) 500–4. 15. Khokhani RC et al. Amlodipine in mild and moderate hypertension: initial Indian experiment. J Assoc Physicians India 1993 41(10) 662–3. 16. Kloner RA et al. Safety of long-acting dihydropyridine calcium channel blockers in hypertensive patients. Am J Cardiol 1998 81(2) 163–9. 17. Lau CP et al. Relative efficacy and tolerability of lacidipine and amlodipine in patients with mild–to–moderate hypertension: a randomized double–blind study. J Cardovasc Pharmacol 1996 28(2) 328. 18. Lichtlen PR, Fisher LD Analysis of arrhythmias in the Circadian Antiischemia Program in Europe (CAPE) study. J Cardiovasc Pharmacol 1999 33(1) 135–9. 19. Leenen FH et al. Persistence of antihypertensive effect after missed doses of calcium antagonist with long (amlodipine) vs short (diltiazem) elimination half–life. British J Clin Pharmacol 1996 41(2) 83–8. 20. Minami J. et al. Effects of amlodipine and nifedipine retard on autonomic nerve activity in hypertensive patients. Clin Exp Pharmacol Physiol 1998 25(7–8) 572–6. 21. Nold G. et al. Morning versus evening amlodipine treatment: Effect of circadian blood pressure profile in essential hypertensive patients. Blood Press Monit 1998 3(1) 17–25. 22. Petkar S. et al. Amlodipine monotherapy in stable angina pectoris. Indian Heart J 1994 46(2) 85–8. 23. Pitt B. et al. Effect of amlodipine on progression of atherosclerosis and the occurrence of clinical events. PREVENT investigators. Circulation 2000 102(13) 1503–10. 24. Rinaldi CA et al. Randomized, double–blind crossover study to investigate the effects of amlodipine and isosorbide mononitrate on the time course and severity of exercise–induced myocardial stunning. Circulation 1998 98(8) 749–56. 25. Sethi KK et al. Amlodipine monotherapy in mild to moderate hypertension. Indian Heart J 1994 46(1) 17–20. 26. Siche JP et al. Effects of amlodipine on baroreflex and sympathetic nervous system activity in mild–to–moderate hypertension. Am J Hypertens 2001 14(5 Pt 1) 424–8. 27. Schwartz JB Effects of amlodipine on steady-state digoxin concentrations and renal digoxin clearance. J Cardiovasc Pharmacol 1988 12(1) 1–5. 28. Steffensen R. et al. Effects of amlodipine and isosorbide dinitrate on exercise–induced and ambulatory ischemia in patients with chronic stable angina pectoris. Cardiovasc Drug Ther 1997 11(5) 629–35. 29. Susaguri M. et al. Amlodipine lowers blood pressure without increasing sympathetic activity or activating the rennin–angiotensin system in patients with essential hypertension. Eur J Clin Pharmacol 1997 53(3–4) 197–201. 30. Videbaek LM et al. Crossover comparison of the pharmacokinetics of amlodipine and felodipine ER in hypertensive patients. Int J Clin Pharmacol Ther 1997 35(11) 514–8.
About drug safety
Doctors prescribe drugs to patients taking into account the severity of the disease, stage, nature and intensity of accompanying symptoms. Lerkamen is quickly evacuated from the body, which means that the likelihood of accumulation of its components is relatively low.
But its auxiliary ingredients in combination enhance and prolong the effect of the main substance. This explains the wide list of restrictions of Lerkamen. All drugs have the following limitations for treatment:
- age under 18 years;
- pregnancy;
- lactation period.
Amlodipine has a smaller list of contraindications, which determines its high demand in the complex treatment of cardiovascular pathologies.
Compared to Amlodipine, Lozap has more restrictions for patients with individual intolerance to one or another component.
Doctors try not to prescribe Lozap to patients with bilateral renal artery stenosis, or renal artery stenosis of a single kidney. It should be used with caution in case of disturbances in electrolyte-water metabolism. Cardiologists must monitor its use by patients with severe liver diseases.
What can replace medications with?
If after 2-3 days the severity of symptoms of primary or secondary hypertension does not decrease, you should inform your doctor. He will prescribe additional medications and adjust the dosage regimen. The doctor can also replace Amlodipine, Lozap, Lerkamen with an analogue that is more effective for a particular patient. Most often, cardiologists prescribe the following antihypertensive drugs:
- angiotensin-converting enzyme inhibitors (ACEIs) - Captopril, Zofenopril, Enalapril, Ramipril, Quinapril, Perindopril, Lisinopril, Benazepril, Fosinopril;
- angiotensin-1 receptor blockers (ARBs) - Valsartan, Irbesatran, Candesatran;
- renin inhibitors - Aliskiren, Rasilez;
- diuretics - Trigrim, Veroshpiron, Diakarb.
The cardiologist does not necessarily replace the drug with an active analogue - a drug with a different active substance, but a similar effect. In their opinion, such adjustments to the therapeutic regimen are not always justified. In many cases, replacing it with a drug with the same main ingredient, but from a different manufacturer, helps. For example, instead of Amlodipine, doctors prescribe Normodipine, Norvasc, Emlodin.
Amlodipine-Prana
Amlodipine can be safely used for the treatment of hypertension together with thiazide diuretics, alpha-blockers, beta-blockers or ACE inhibitors. In patients with stable angina, the drug can be combined with other antianginal agents, for example, long- or short-acting nitrates, beta-blockers.
Amlodipine can be used concomitantly with non-steroidal anti-inflammatory drugs (NSAIDs) (especially indomethacin), antibacterial agents and oral hypoglycemic agents.
It is possible to enhance the antianginal and hypotensive effect of BMCC when used together with thiazide and loop diuretics, verapamil, ACE inhibitors, beta-blockers and nitrates, as well as enhance their hypotensive effect when used together with alpha 1-blockers, antipsychotics.
Although negative inotropic effects have not generally been observed in amlodipine studies, some CBMCs may enhance the negative inotropic effects of antiarrhythmics and QT prolonging agents (eg, amiodarone and quinidine).
A single dose of 100 mg of sildenafil in patients with essential hypertension does not affect the pharmacokinetic parameters of amlodipine.
Repeated use of amlodipine at a dose of 10 mg and atorvastatin at a dose of 80 mg is not accompanied by significant changes in the pharmacokinetics of atorvastatin.
Ethanol (drinks containing alcohol): amlodipine with single and repeated use in a dose of 10 mg does not affect the pharmacokinetics of ethanol. Antiviral agents (ritonavir) increase plasma concentrations of BMCC, incl. amlodipine.
Neuroleptics and isoflurane - enhance the hypotensive effect of dihydropyridine derivatives.
Calcium supplements may reduce the effect of BMCC.
When amlodipine is used together with lithium preparations, it is possible to increase the manifestation of neurotoxicity (nausea, vomiting, diarrhea, ataxia, tremor, tinnitus).
Amlodipine does not change the pharmacokinetics of cyclosporine.
Does not affect the serum concentration of digoxin and its renal clearance.
Does not have a significant effect on the effect of warfarin (prothrombin time).
Cimetidine does not affect the pharmacokinetics of amlodipine.
In in vitro studies, amlodipine does not affect the binding of digoxin, phenytoin, warfarin and indomethacin to blood proteins.
Grapefruit juice: simultaneous single administration of 240 mg of grapefruit juice and 10 mg of amlodipine orally is not accompanied by a significant change in the pharmacokinetics of amlodipine.
About the effectiveness of medications
Doctors take into account the composition, dosage form, pharmacokinetics and pharmacodynamics. As well as the likelihood of developing adverse reactions, both local and systemic, when recommending this or that drug to the patient. Amlodipine, Lozap, Lerkamen are the most commonly prescribed antihypertensive drugs. Their main advantage is a one-time dose during the day. By swallowing a pill at breakfast, a person does not have to worry that stress or physical activity will lead to a sharp jump in blood pressure. Therefore, such drugs will be useful for forgetful people or those who are busy with tasks throughout the day.