Pharmacological properties of the drug Andriol tk™
Pharmacodynamics. Testosterone, the main androgenic hormone necessary for the normal development of male genital organs and secondary sexual characteristics, maintaining normal function of the testicles, prostate and seminal vesicles, to maintain libido and potency. Oral administration of Andriol TK provides physiological levels of testosterone in the blood serum in men with hypogonadism. In addition, the use of the drug leads to a clinically significant increase in plasma concentrations of dihydrotestosterone and estradiol, as well as a decrease in the level of sex hormone binding globulin (SHBG). Treatment with the drug in men with primary (hypergonadotropic) hypogonadism normalizes gonadotropin levels. Androgens influence the processes of anabolism in the body, the development of skeletal muscles and the distribution of subcutaneous fat on the body, are responsible for the end of linear growth of the body and stimulate erythropoiesis, increasing the production of erythropoietin. When taking them, salt and water retention may occur in the body. The effect of testosterone on target organs is enhanced after the peripheral conversion of testosterone to estradiol, which binds to estradiol receptors in the nucleus of the target cell. This process occurs in the pituitary gland, adipose tissue, brain, osteocytes and testicular granulocytes. The use of exogenous androgens, depending on the dose, delays the release of endogenous testosterone. The use of exogenous androgens in high doses can inhibit spermatogenesis. Pharmacokinetics. After oral administration, a significant portion of testosterone undecanoate, together with the lipophilic solvent, is absorbed in the small intestine and enters the lymphatic system, thus bypassing the initial passage through the liver. When testosterone is absorbed, undecanoate is partially reduced to form dihydrotestosterone undecanoate. From the lymphatic system it enters the blood plasma. As a result of hydrolysis in the blood plasma and tissues, testosterone undecanoate and dihydrotestosterone undecanoate are converted into natural androgens - testosterone and dihydrotestosterone. A single dose of 80–160 mg of Andriol TK leads to a clinically significant increase in the level of total plasma testosterone concentration, the maximum value of which, Cmax, is about 40 nmol/l and is achieved 4–5 hours after oral administration. The increased concentration of testosterone in the blood plasma persists for at least 8–12 hours. It is excreted mainly in the urine in the form of conjugates (ethiocholanolone and androsterone).
Obesity is understood as a chronic metabolic disease manifested by excessive development of adipose tissue [1]. This pathology increases the incidence of cardiovascular diseases, type 2 diabetes mellitus, joint diseases (osteoarthrosis), malignant neoplasms of various localizations (kidney, colon, lung cancer , breast and female genital area) [2-5]. In addition to its overall health consequences, obesity reduces quality of life, including physical and psychosocial activity, and significantly affects life expectancy and increases overall mortality [3–5].
Literature data indicate that deterioration in the quality of life in overweight men is also associated with sexual dysfunction in the form of erectile dysfunction, low sexual satisfaction, and decreased libido [6-9]. The limited number of studies of sexual function in obese men indicates the need for further research in this area.
Goal of the work:
- to study changes in the level of sex hormones in patients with excess body weight;
- explore the relationship between the quality of sexual life and body mass index (BMI);
- to evaluate the effectiveness of androgen replacement therapy as an additional method of treating obesity.
MATERIALS AND METHODS
The object of the study was men who consulted a nutritionist about excess weight.
In the period from January to June 2012, we observed 30 men aged from 37 to 54 years (average age 45 years), with varying degrees of obesity. 10 men were found to have low levels of testosterone in the blood (<12 mmol/l). They were included in the study group. The control group included 20 men with normal testosterone levels.
All patients underwent the following examinations:
- determination of BMI;
- waist circumference (WC) measurement;
- determination of the level of five sex hormones: testosterone (Tst), luteinizing hormone (LH), prolactin, sex steroid binding globulin (SSBG) and estradiol;
- assessment of erectile function on the IIEF-5 scale.
Both groups were comparable in age, BMI, WC, hip volume (HF), % fat tissue
As androgen replacement therapy, patients used testosterone gel 1% - the drug "AndroGel"
The degree of significance of the difference (p) was determined using the Fisher-Student table. The difference was considered significant if p<0.05.
RESULTS
According to the result of measuring BMI, the majority of patients in both groups had class II before treatment. obesity (BMI 35 39.9 kg/m2), the distribution of adipose tissue was according to the “male type”, i.e. in the abdominal area, while WC in all patients was more than 100 cm, which is one of the indirect signs of a disorder of gonadal function.
It was noted that patients in the study group with a higher BMI had lower testosterone levels. Despite the low level of testosterone in the blood in the morning, the remaining hormones studied (LH, prolactin, CVS and estradiol) were within the physiological norm. When studying erectile function in patients, the average score on the IIEF scale was 14.2±5.0 (Table 1).
Table 1. Results of the study of patients in the main group
| Before treatment | 5 months after treatment | |
| BMI (kg/m2) | 38,2 ± 5,7* | 30,2 ± 2,6 |
| Waist circumference (cm) | 127,4 ± 19,7* | 103,4 ± 9,4 |
| % fat tissue | 37,7± 11,7* | 25,8± 7,3 |
| IIEF-5 | 14,2 ± 5,0 | 20,2 ± 4,7* |
| Tst (mmol/l) | 9,3± 2,1 | 18,3± 5,7* |
| Prolactin (mIU/l) | 270 ± 49,7* | 240 ± 40,9 |
| LH(IU/l) | 3,4± 1,7* | 2,1 ± 1,1 |
| SSSG(nmol/l) | 45,2± 6,3 | 43,1± 5,9 |
| Estradiol (pmol/l) | 63,2± 15,7* | 51,1± 12,5 |
Statistically significant difference before and after treatment, p<0.05
In order to restore and maintain the physiological level of testosterone in the blood, patients in the study group received the drug “AndroGel” - testosterone gel 1%, at a dose of 50 mg per day, for three months. After starting the use of AndroGel, patients in the study group experienced an increase in the rate of weight loss; by the 5th month of therapy, the same results as the control group were achieved.
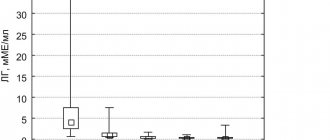
At the same time, patients in the study group had a slower rate of weight loss during the weight loss process compared to patients with normal testosterone levels (Fig. 1).
Rice. 1. Dynamics of decrease in body mass index when taking Androgel
When assessing sexual function after 5 months of treatment, the average score on the IIEF-5 scale in the study group receiving androgen replacement therapy exceeded that of the control group (20.2 ± 4.7 versus 18.2 ± 5.5, p < 0.05) .
Thus, obese men often experience a decrease in blood testosterone levels, while, despite testosterone deficiency, the levels of other sex hormones (LH, prolactin, CVS and estradiol) remained within the physiological norm. In obese men, there is a significant prevalence of ED, associated with both secondary hypogonadism and dysmorphophobia. The severity of ED also correlated with the degree of obesity. The additional administration of the gel testosterone preparation “AndroGel” contributed to a significant improvement in the quality of erectile function of patients and was an effective adjuvant to the main treatment of obesity in men.
LITERATURE
1. Controlling the global epidemic obesity. World Health Organization, 2002. // URL: https://www.who.int/nut/obs.htm.
2. Tritos N, Mantzoros CS. Leptin: Its role in obesity and beyond. // Diabetologia. 1997. Vol. 40. P. 1371-1379.
3. Jeguer E, Tappy L. Regulation of body weight in humans. // Physiol Rew. 1999. Vol. 79, N 2. P. 451-475.
4. Baile CA, Delle-Fera MA, Martin RJ. Regulation of metabolism and body fat mass by leptin. //Ann Rev Nutr. 2000. Vol. 20. P. 105-127.
5. Morales A, Lunenfeld B. Androgen replacement therapy in aging men with secondary hypogonadism. Draft recommendations for endorsement by ISSAM. // Aging Male. 2001. Vol. 4, N 3. P. 151-162
6. MoralesA, Heaton JPW. Hormonal erectile dysfunction: evaluation and management. // UrolClin North Amer. 2001. Vol. 28, N 2. P. 279-288/
7. Alexander GM, Swerdloff RS, Wang C, Davidson T, McDonald V, Steiner B, Hines M. Androgen behavior correlations in hypogonadal and eugonadal men: cognitive abilities. // Hortn Bekav. 1998. Vol. 33, N 2. P. 85-94.
8. Urban RJ, Bodenburg Gilkison C, Fowworth J, Coggan AR, Wolfe RR. Testosterone administration to elderly men increases skeletal muscle strength and protein synthesis. // Am J Physiol. 1995. Vol. 269, N 5. P. 820-826.
9. Morales A, Johnston B, Heaton JWP, Lundie M. Testosterone supplementation for hypogonadal impotence: assessment of biochemical measures and therapeutic outcomes. // J Urol 1997. Vol. 157, N 3. P. 849-854
| Attached file | Size |
| 155.11 kb |
‹ Our experience in retroperitoneoscopic treatment of purulent-inflammatory diseases of the kidneys and retroperitoneum Up Report on the X All-Russian scientific and practical conference with international participation “Rational pharmacotherapy in urology” ›
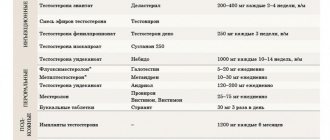
Use of the drug Andriol tk™
The dose is selected individually depending on the clinical effect. Typically, an initial dose of 120–160 mg/day for 2–3 weeks, followed by a maintenance dose of 40–120 mg/day, is adequate. Andriol TK capsules are taken orally during meals without chewing, if necessary, with a small amount of liquid. It is advisable to take half the daily dose in the morning and the rest in the evening. If an odd number of capsules is taken, the higher dose is taken in the morning.
Special instructions for the use of the drug Andriol tk™
In prepubertal boys, androgens should be used with caution to avoid premature closure of the epiphyses and accelerated sexual development. Regular monitoring of skeletal development is necessary. Patients with latent or severe heart failure, impaired renal function, hypertension (arterial hypertension), epilepsy or migraine (either currently or in history) should be under constant medical supervision, since sometimes deterioration or exacerbation of these diseases is possible. Androgens should be prescribed with caution to patients with benign prostatic hyperplasia. If androgen-dependent adverse reactions develop, treatment should be discontinued. After the disappearance of side effects, treatment with the drug should be resumed at lower doses. Taking steroids may affect the results of certain laboratory tests.
Andriol
Release form, composition and packaging
Capsules 1 capsule. testosterone undecanoate 40 mg.
Clinical and pharmacological group: Androgenic drug.
Pharmacological action Andriol is a testosterone preparation that is active when taken orally. The active ingredient is testosterone undecanoate, an ester of natural testosterone. Testosterone in its pure form is inactive when taken orally.
In contrast, testosterone undecanoate, due to its high fat solubility, as well as the presence of a special solvent - oleic acid, is absorbed with chylomicrons through the lymphatic system of the small intestine, enters the thoracic lymphatic duct and then immediately enters the systemic bloodstream through the superior vena cava system.
Thus, a sufficient amount of testosterone bypasses the initial passage through the liver and inactivation in it, and therapeutic concentrations of this hormone are quickly achieved in the systemic circulation. When using Andriol in plasma, the level of both testosterone and its active metabolites increases, which causes a lasting therapeutic effect. Andriol, unlike orally active C-17-methylated testosterone derivatives, does not affect liver function.
Pharmacokinetics
Suction
After oral administration, 45-48% of the dose is absorbed from the small intestine. Cmax in plasma is achieved between 2.5 hours and 5 hours after a single dose.
Metabolism
Testosterone undecanoate is hydrolyzed to form testosterone, the action of which is similar to that of endogenous testosterone. Subsequently, active testosterone metabolites are formed: 5-alpha-dihydrotestosterone, androstenedione and estradiol, which, by binding to the corresponding receptors, determine the full spectrum of androgenic activity of Andriol. Excretion T1/2 - 3-4 hours. Excreted mainly in urine in the form of metabolites (glucuronides and sulfates); in the first 24 hours - about 40%, and within one week - 50-70%.
A small amount of the active substance is excreted in the feces.
Indications
Hormone replacement therapy for disorders associated with testosterone deficiency:
- post-castration syndrome;
- eunuchoidism;
- hypopituitarism;
- endocrine impotence;
- menopausal disorders in men, such as decreased libido and decreased mental and physical activity.
In addition, testosterone therapy may be indicated for osteoporosis.
Dosage regimen
As a rule, the dose should be adjusted individually depending on the clinical effect. The recommended initial dose is 120-160 mg/day for 2-3 weeks. Maintenance dose - 40-120 mg/day. Andriol capsules should be taken after meals with a small amount of liquid; swallow whole without chewing. It is advisable to take half the dose in the morning and the other half in the evening. If the patient is taking an odd number of capsules, the higher dose should be taken in the morning.
Side effect
From the reproductive system: priapism, increased sexual arousal; premature puberty in boys, increased frequency of erections, increased penis size, oligospermia, decreased ejaculate volume. From the side of water-electrolyte balance: sodium and water retention. Other: premature closure of bone growth zones, dizziness, nausea.
Contraindications
- verified or suspected prostate or breast carcinoma.
special instructions
If androgen-dependent side effects occur, treatment should be discontinued. After their disappearance, treatment should be resumed with lower doses.
Treatment of patients with latent or severe heart failure, impaired renal function, arterial hypertension, epilepsy or migraine (or with indications of these conditions in the anamnesis) should be carried out under constant supervision, since androgens can in some cases cause sodium and water retention. A decrease in the level of protein-bound iodine may occur, but this is not clinically significant.
Use in pediatrics
In prepubertal boys, androgens should be used with caution to avoid premature closure of the epiphyses and accelerated sexual development.
Overdose
Currently, no cases of overdose of Andriol have been reported.
Drug interactions
Drug interactions with Andriol have not been described.
Storage conditions and periods
The drug should be stored in a dry place, protected from light.
Shelf life when stored at room temperature is 90 days. Shelf life when stored at a constant temperature from 2° to 8°C is 3 years.