Psychiatry is often “mystified”, as a result of which the treatment of mental illness seems to most to be something extremely extraordinary, unknown and complex. And very often this is exactly what happens: the process of treating psychiatric patients really does cause a lot of problems and difficulties.
A psychiatrist is the same doctor as a therapist, cardiologist, ENT specialist, etc.
Society has developed a very specific attitude towards psychiatry, and it is unfounded and even absurd. Treatment by a psychiatrist, unfortunately, is condemned by people, considered shameful and often hidden from family and friends.
It is important to understand that mental health therapy is a routine treatment for an unusual illness. Nowadays, there are not so many differences between the principles of treatment in psychiatry and, say, therapy (although some “unusual” procedures are still used).
A person should not be more afraid of a visit to a psychiatrist than a visit to a therapist, cardiologist or ENT specialist. This, in many ways, is the key to the mental health of the population. Let's look at what a consultation with a psychiatrist can be like using the example of obsessive-compulsive neurosis, the treatment of which is very important due to its wide distribution.
Indications
◊ Recommendations of the Russian Ministry of Health
F32 Depressive episode
F33 Recurrent depressive disorder
F40.0 Agoraphobia
F41.0 Panic disorder (episodic paroxysmal anxiety)
◊ FDA recommendations
- Major depressive disorder (adults and children over 12 years of age)
- GTR
◊ Recommendations from UK Medicines and Healthcare Products Regulatory Agency
- Major depressive episode
- Panic disorder with/without agoraphobia
- Social phobia
- GTR
- OCD
◊ Using Off-label
- Vasomotor symptoms during menopause
- Insomnia
- Dysmorphophobia
- Bulimia [5].
Mechanism of action and pharmacokinetics
Escitalopram is the S-isomer of citalopram. Selectively inhibits the reuptake of serotonin, increasing the concentration of this neurotransmitter in the synaptic cleft. Escitalopram, like other antidepressants from the SSRI group, practically does not bind to dopamine (D1 and D2) receptors, α-adrenergic and m-cholinergic receptors, as well as benzodiazepine and opioid receptors [4]. Long-term use of escitalopram leads to desensitization of somatodendritic 5-HT1A and terminal autoreceptors.
- Bioavailability – 80%.
- Half-life 27-32 hours
- Stable concentration in the blood is maintained for one week
- Metabolized by CYP3A4, CYP2C19; inhibits CYP2D6
Manifestations of obsessional neurosis
The most common manifestation of obsessional neurosis is fear, which is very difficult and sometimes almost impossible to overcome. Phobias make social contacts, work and all other aspects of life very difficult.
Another version of neurosis is, in fact, obsessive thoughts that a person cannot “drive” out of his head. These thoughts interfere with learning, concentration and greatly tire the patient. An important criterion: a person with obsessional neurosis never realizes his thoughts. The last type is compulsive. It manifests itself through obsessive movements and excessive ritualism.
Treatment regimen
◊ Dosage and dose selection
- Optimal dose for treating depression, OCD and GAD: 10-20 mg/day
- Start with 10 mg/day, increase to 20 mg if necessary
- Take once daily, morning or evening
- 10 mg escitalopram is comparable to 40 mg citalopram, but without side effects
- A dose of 30-40 mg is suitable for some patients [1]
- To relieve vasomotor symptoms during menopause, 10 mg/day is sufficient, but if ineffective within 4 weeks, the dose may be increased to 20 mg/day
- If anxiety, insomnia, agitation, or akathisia occur at the beginning of treatment or after interruption of treatment, the possibility of bipolar disorder should be considered and switched to a mood stabilizer or an atypical antipsychotic
◊ How quickly it works
- Begins to act after 2-4 weeks
- If there is no effect after 6-8 weeks, you need to increase the dose or switch to another drug
- To prevent relapse, it can be taken for many years.
◊ Expected result
- Complete remission.
- After the symptoms of depression disappear, you should continue taking it for 1 year if this was the treatment of the first episode. If this is to treat a recurrent episode, treatment can be extended indefinitely.
- Use in the treatment of anxiety and chronic pain may be indefinite.
◊ If it doesn't work
- Change the dose, switch to another medicine or add an auxiliary drug;
- Connect psychotherapy;
- Review the diagnosis by identifying comorbid conditions;
- In patients with undiagnosed bipolar affective disorder, the effectiveness of treatment may be low, in which case it is necessary to switch to a mood stabilizer [1].
- In the acute phase of severe depressive disorder, which is accompanied by psychotic or catatonic symptoms, as well as in patients with current suicidal ideation, electroconvulsive therapy should be considered [7].
◊ How to stop taking it
It is usually not necessary to reduce gradually, but to be sure to avoid withdrawal symptoms, you can reduce it gradually. Gradual reduction scheme: dose reduced by 50% - 3 days, again reduced by 50% - 3 days, complete cessation. If withdrawal symptoms appear, increase the dose, wait for withdrawal symptoms to subside, and continue decreasing [1].
◊ Treatment combinations
- For insomnia: trazadone
- For fatigue, drowsiness, loss of concentration: modafinil [3].
- Combinations with other antidepressants may activate bipolar disorder and suicidal ideation
- For bipolar depression, psychotic depression, treatment-resistant depression, treatment-resistant anxiety disorder: mood stabilizers, atypical antipsychotics
- For anxiety disorder: gabapentin, tiagabine
The effectiveness of the drug escitalopram (Cipralex) in the treatment of panic attacks
Escitalopram (Cipralex) is a highly selective serotonin reuptake inhibitor (SSRI) with proven effectiveness against panic disorders. Due to the selectivity of their action, antidepressants of the SSRI group have a significantly lower number of side effects and the degree of their severity in comparison with drugs of the previous generation - tricyclic antidepressants. The antidepressant effect of escitalopram has been demonstrated in clinical trials, including placebo-controlled ones, mainly in patients with depressive disorders.
Table 1. Patient population
Table 2. Previous diagnoses
Table 3. Groups of drugs used as therapy
Table 4. Main complaints during an attack of PA
Table 5. First Panic Score
Table 6. What, according to the patient, is associated with the development of the disease
Table 7. Characteristics of attacks
Table 8. Dynamics of attacks
Rice. 1. Weekly self-assessment according to VAS for 10 weeks
Table 9. Dynamics of test indicators over 10 weeks
Table 10. Subjective assessment of escitalopram therapy in patients with PsA
Escitalopram is the S-enantiomer of the SSRI citalopram, a racemic compound consisting of two isomers (S- and R-). It has been established that the ability of the S-isomer to inhibit serotonin reuptake is more than 100 times higher than that of the R-isomer. S-citalopram was isolated as an independent drug, which is superior to citalopram in the speed of development of the clinical effect and the degree of its severity.
Thus, in previous studies, using escitalopram at a fixed dose of 10 mg/day, the same improvement in key parameters of antidepressant efficacy was observed as when using 40 mg citalopram. The early and persistent antidepressant effect of escitalopram is achieved using doses in the range of 10–20 mg/day. with exceptionally good tolerability [11]. According to multicenter studies conducted in the United States, escitalopram was well tolerated in 76% of cases, regardless of dose. Discontinuation of escitalopram due to side effects was recorded in 4.2% of those taking the drug at a dose of 10 mg/day. and in 10.4% - at a dose of 20 mg/day. [16]. The severity of adverse events that occurred during therapy does not exceed 2 points on the scale of side effects of therapy (UKU), which indicates the absence of a significant impact on the patient’s condition and functioning. The dynamics of adverse events are regressive in nature, i.e., by the end of the 2nd week of treatment, most manifestations are mild and lose both objective and subjective significance [3].
Panic attacks (PA) are the most severe form of anxiety disorders, leading to severe maladjustment [14], having a chronic course with exacerbations and remissions [4]. PAs are discrete periods in which there is a sudden onset of intense anxiety, fear or terror, often associated with a feeling of impending doom. These attacks are characterized by symptoms such as shortness of breath, throbbing, chest pain or discomfort, a feeling of suffocation, and fear of “going crazy” or “losing control” [5]. Diagnostic criteria for a panic attack (PA) are paroxysmalness, polysystemic vegetative symptoms, the presence of emotional disorders, the severity of which can range from “a feeling of discomfort” to “panic.”
Purpose of the study
The effectiveness and tolerability of a 10-week course of escitalopram (Lundbeck) at a dose of 5–10 mg/day were assessed. in the treatment of panic disorders according to the dynamics of clinical characteristics and psychometric indicators, as well as identifying predictors of therapy effectiveness. The main assessment of effectiveness was made by the frequency of panic attacks in the 10th week of treatment compared with baseline indicators (before the start of treatment) and the effect of the drug on comorbid conditions. The effectiveness of escitalopram was verified by a statistically significant reduction in panic attacks, a decrease in the level of anxiety, and depression.
Research material
Forty outpatients fulfilling DSM-IV (1994) and ICD-10 (1995) criteria [13, 17] for panic disorder with or without agoraphobia. All subjects had typical PAs – the typicality index was 0.68 [3]. Among the examined patients, there were 27 (67.5%) women and 13 (32.5%) men. The average age of patients in the whole group at the time of treatment was 35.9 ± 9.1 years (from 24 to 61 years). The average age of onset of PA was 33.8 ± 8.1 years (from 23 to 57 years), with 33.3% being within the age limit of 25–35 years, 33.3% within the age limit of 35–40 years, and 14 .8% – within 30–35 years. That is, all the examined persons were of active, working age. The average duration of the disease in the group was 1.1 ± 1.1 years (from 1 month to 4 years). The patient population is presented in Table 1.
Among the examined patients, 29.6% suffered from agoraphobia. These patients were unable to travel on the subway on their own or drive their own car (only when accompanied by loved ones). 25.9% had restrictive behavior, which included poor tolerance of hypermarkets, markets, and other public places that provoke attacks of PA due to “flashing before the eyes of people and a lot of goods.” Among the observed patients, 11 are car owners, but due to attacks of PA they were forced to give up driving a car independently. During therapy, patients began to drive again without any subjective difficulties, which indicates good tolerability of escitalopram against the backdrop of a pronounced effect of increasing concentration.
Professional representation
In the groups of patients there were representatives of different professions, among them 81.5% had a permanent job (manager, head of construction operation, company administrator, doctor, deputy general director of the enterprise, leading specialist in regional supplies, accountant, director of the company, economist, bank employee, businessman, pharmacist, supermarket salesman, curtain designer, personal chef) and 18.5% did not work (housewife, pensioner). Only one patient left work due to the onset of her illness, the rest - due to somatic diseases or age. 51.8% had higher education, 48.2% had specialized secondary education. As can be seen from the list of professions, the vast majority of the patients studied occupy leadership and responsible positions that require maximum internal stress.
It turned out that more than half of the patients had a combination of clinical syndromes: autonomic dysfunction, algic manifestations, motivational and insomnia disorders.
Headaches were observed in 30% of cases. The characteristics of headaches in patients with PA had some signs of tension headaches (localization in the fronto-parieto-temporal region, of a pressing nature, the average intensity on the VAS reached 4-5 points) and differed from the latter in the accompanying symptoms: a feeling of “heaviness in the head”, “ deterioration of hearing”, the feeling that “one can hear the heartbeat”, “something is tense in the head.” Since headaches occurred only in association with other symptoms, these characteristics may indicate that headache was part of a psycho-vegetative complex.
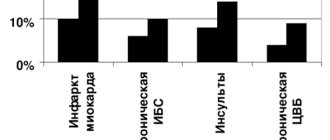
The majority of patients (63%) who sought help had previous diagnoses that either reflected failure in the somatic sphere or did not have a clear nosological focus; 37.5% had no diagnosis at all and only 15% had a corresponding diagnosis of PA (Table 2). The data obtained indicate that panic disorder is underdiagnosed in general somatic practice.
Previous treatment
All patients unsuccessfully or insufficiently effectively (the effect lasted for several days or, less often, 1 month) took a number of drugs without receiving the proper therapeutic effect.
Study design and methods
The patients were examined during the 2nd, 4th, 6th and 10th weeks of continuous therapy with escitalopram. The following methods were used to assess the status of patients:
- clinical and neurological examination according to the survey protocol for patients with PA with assessment of the panic attack typicality index [5];
- psychometric testing using the Sheehan Anxiety Scale (Sheehan, 1983), Beck Depression Inventory (Beck, 1961) [2] and quality of life for panic attacks [5], Holmes TM Life Events Scale [18], 10-point visual analogue scale (VAS) for self-assessment of general well-being (where 0 points are the worst, 10 points are the best idea of the state of health) (according to S. Walker, R. Roser, 1993) [2];
- subjective assessment of the effectiveness of escitalopram therapy on a 5-point scale (where 0 points is no effect, 5 points is a pronounced effect).
Background indicators
During the initial examination, patients in the study group complained of rapid heartbeat, fluctuations in blood pressure, respiratory distress (hyperventilation, “attacks of suffocation,” “inability to inhale,” “lump in the throat”), tension-type headaches, increased anxiety and internal trembling, fixation on the state of one’s health, decreased performance and a feeling of helplessness, lipothymia (“blackout before the eyes”), sleep disturbance (difficulty falling asleep, early awakenings), “ringing in the ears.” During the attack, each patient had several symptoms. The main symptoms accompanying the attack are presented in Table 4.
At the onset, 9 patients had such severe anxiety and fear of death that they had to call an ambulance or were repeatedly hospitalized. The assessment of the “first panic” is presented in Table 5.
Neurological status
In the vast majority of patients, the following features were revealed in their neurological status: revival of tendon reflexes from the arms and legs with expansion of reflexogenic zones, with unstable pathological hand signs (Rossolimo, Hoffman rivers), dissociation of reflexes along the axis (more vividly from the legs than from hands), Khvostek's sign of I–II degree, wetness of the hands, nystagmus in the extreme abductions, slight asymmetry (smoothness) of the nasolabial folds.
An analysis of patients’ opinions regarding the provoking factor in the development of the disease showed that the majority of patients (37.5%) indicated stressful situations at home and/or at work as the main factors that provoked the development of the first attack of PA (Table 6). But it should be noted that there was often a combination of several factors.
Treatment results
The study results showed that out of 40 patients, 33 (82.5%) completed the full 10-week course of escitalopram therapy. Subjectively, the frequency (from 14 to 0–1 attacks per week) and intensity of attacks (from high, with an ambulance call, to complete absence), the duration of one episode (from 24 hours to several minutes), and the number of symptoms in an attack (from 13 to 1) at the end of the course of therapy.
At the initial stage, only a small proportion of patients used therapy correctors: anaprilin, sonopax, alprazolam, fluanxol.
We assessed the effectiveness of therapy based on the qualitative characteristics of the attack and their dynamics, using objective rating scales; we compared the effectiveness in groups of patients who had previously taken and had not taken antidepressants (Table 3). Table 7 presents the qualitative characteristics of the attack.
Noteworthy is the long duration of the attack, which in some patients reached several hours. This circumstance is due to the fact that for the duration of the attack, patients took a combination of events that included the attack itself, a post-attack state in the form of asthenia, anxiety, irritability, headaches, etc., or a series of attacks with short time intervals.
All patients (100%) had daily both full-blown and abortive attacks before starting therapy. In the process of taking the drug, there was the following dynamics: a gradual decrease in attacks and shortening their duration, a decrease in intensity until complete cessation, and an increase in self-control during an attack. The dynamics of attacks are presented in Table 8.
In the background study, all patients (100%) had both spontaneous and situational (100%) attacks of PA. At the end of therapy, spontaneous attacks were not observed in any patient, situational ones persisted in 6 patients and were abortive in nature (a single monosymptomatic attack of low intensity, quickly resolving). In connection with this circumstance, these patients continued taking escitalopram after a 10-week course of therapy.
The drug prescription regimens for those patients (n=33) who completed the full course of therapy were as follows:
- The initial dose is 1.25 mg/day. for 10 days, the next 10 days at 2.5 mg/s, the remaining days at 5 mg/day. (n=1);
- The initial dose is 2.5 mg/day. for 2–3 weeks, followed by a transition to a dose of 5 mg/day. (n=3);
- The initial dose is 5 mg/day. for 3 weeks, followed by a transition to 10 mg/day. (n=2);
- The initial dose is 5 mg/day. for 1 week, followed by a transition to 10 mg/day. (n=27).
Most patients used the 4th treatment regimen and the drug was well tolerated. However, when prescribing escitalopram, it should be taken into account that some patients require a specific individual treatment regimen 1, 2 or 3.
The reasons why non-standard treatment regimens were prescribed are as follows. In a patient treated according to regimen 1, after a single dose of 5 mg, severe weakness, dilated pupils, and increased blood pressure were observed - the dose was reduced to 2.5 mg, which also led to increased symptoms of panic. It was decided to further reduce the dose to 1.25 mg, which was well tolerated by the patient. Subsequent dose increases did not cause any side effects. Patients transferred to regimen 2 also turned out to be sensitive to a dose of 5 mg; a dose of 2.5 mg was well tolerated by them. The patient taking the drug according to regimen 3, after a week's course, was unable to switch to a dose of 10 mg; she required a longer adaptation period.
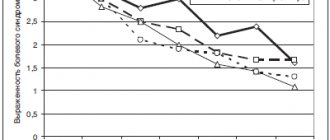
Tolerability of the drug was generally rated by patients as good. Subjectively, within 2 weeks, the following was noted: a decrease in attacks and a decrease in their intensity, an increase in self-assessment of general well-being according to VAS (Fig. 1), improved mood, and normalization of sleep. Objectively, all test indicators reliably changed for the better (Table 9).
Subjective assessment data (on a 5-point scale) of escitalopram therapy by patients who completed a 10-week course of treatment are presented in Table 10. Most patients rated the drug at 5 points. The average sum score was 4.57.
Tolerability of the drug included side effects, paradoxical reactions, and drug refusal. On days 1–3, almost all patients reported side effects of varying severity: dizziness, “drowsiness,” decreased concentration, and increased anxiety. Paradoxical reactions developed, as a rule, during the first week (on days 3-5-7 of therapy at a dose of 5 mg/day or when switching to a dose of 10 mg/day): severe weakness, rise in blood pressure, sharp worsening of all symptoms of PA, sleep disturbance (insomnia, drowsiness), leg cramps. This was the reason for refusal of escitalopram therapy in 7 (17.5%) patients (5 women, 2 men). The drug was well tolerated by most patients in the following days.
Conclusion
The study showed the high effectiveness of Escitalopram in the treatment of panic disorder over a 10-week course. Patients who completed the course of treatment subjectively highly rated both the effectiveness of the drug and its tolerability.
The anti-panic effect appears in the 2-3rd week of therapy; first of all, full-blown attacks undergo regression. The undeniable advantage of Escitalopram is its effectiveness against concomitant agoraphobic and depressive disorders. The dynamics of the reverse development of depressive symptoms and symptoms of agoraphobia correspond to the regression of panic attacks. Symptoms of agoraphobia have proven to be the most resistant to treatment. In treated patients who retained PA at the end of the treatment course, only situational PA (a marker of agoraphobia) was observed. In the presence of severe agoraphobia and severe panic disorder, longer courses of treatment may be recommended - from 3 to 5 months.
Thus, escitalopram can be recommended as monotherapy or a basic drug in polytherapy for the treatment of panic disorder.
Special patient groups
◊ Patients with kidney problems
Use caution if the patient has severe kidney disease [1].
◊ Patients with liver disease
The recommended dose is 10 mg/day [1].
◊ Patients with heart disease
There are no systematic data on the use of escitalopram in people with pathology of the cardiovascular system. Supposedly safe. Useful in recovery after a heart attack [1].
◊ Elderly patients
For elderly patients, a dose of 10 mg is recommended [1].
◊ Children and teenagers
- Recommended for the treatment of depression aged 12-17 years
- It is necessary to regularly and personally check the patient's condition, especially in the first weeks of treatment.
- Use with caution due to the risk of undiagnosed bipolar disorder and suicidality.
- Inform adults about the risks.
◊ Pregnant women
- There have been no adequate studies in pregnant women [1].
- Not recommended for pregnant women, especially in the first trimester
- All risks should be weighed and compared
- Bleeding can be expected during childbirth
◊ Breastfeeding
- The medicine passes into breast milk.
- If the infant shows signs of irritation or sedation, discontinue feeding or escitalopram
- However, treatment after childbirth may be necessary, so the risks should be weighed.
What is obsessional neurosis, and does it need to be treated?
The main goal of treatment is to maximize the patient’s quality of life. If a disease interferes with life, then it definitely needs to be treated. Does obsessional neurosis interfere with normal life? To understand this, you need to find out what is commonly understood by this term.
Obsession is the appearance in a person of thoughts or actions that are perceived by him as something alien. A person cannot get rid of them: obsessions force him to perform certain actions, thereby becoming the cause of debilitating mental discomfort.
Side effects and other risks
◊ Mechanism of side effects
Side effects are caused by an increase in serotonin. Most side effects occur immediately after starting treatment and go away over time.
◊ Side effects
- Gastroenterological (reduced appetite, nausea, diarrhea, constipation)
- Insomnia, sedation, agitation, tremor
- Sweating
- Urinary dysfunction
- Dry mouth
- Dangerous side effects: seizures, mania, suicidal ideation
- Weight gain: very rare
- Sedation: very rare
- Sexual dysfunction: yes
◊ What to do about side effects
- Wait
- Switch to another antidepressant [1].
◊ Long-term use
Safely
◊Addiction
No.
◊ Overdose
- There are very few reports of overdose.
- Very rare cases of fatal overdoses.
- Vomiting, sedation, cardiac arrhythmia, dizziness, tremor.
Expert advice
- The best antidepressant in terms of tolerability
- Lowest sexual impact compared to other SSRIs
- Lack of response to escitalopram in elderly patients may indicate Alzheimer's disease
- In postmenopausal women, escitalopram works better in combination with estrogen [1]
- Escitalopram and fluoxetine show similar effects in the treatment of depression. The only difference noted is that escitalopram significantly improves microinflammation in the patient’s body [6].
Examples of obsessional neurosis
It is very easy to explain the essence of this phenomenon with examples. Let's say you believe that you shouldn't look in the mirror before leaving the house. However, if you accidentally look in the mirror, you will still leave the house without giving it much importance.
Or, for example, a black cat on the road will not force you to reschedule your business: you may be a little worried, but you will soon forget about it. A person with compulsive obsessions, looking in the mirror, will bolt the door and stay at home all day, and, having met a black cat, go to the pharmacy for sedatives.
As you can see, obsessional neurosis makes the patient’s life very difficult. This means that we can say confidently and definitely: this disease definitely needs treatment, and the treatment must be professional and complete.