Pain is the leading reason for visiting a doctor worldwide
According to published data, chronic pain accounts for 50% of all cases in Europe. Most likely, this figure will increase in the future, especially in older people, whose general condition is aggravated by various concomitant pathologies and has a complex etiology. Consequently, the need for safe and effective pain management increases in these patients. Specialists cannot completely relieve pain unless its cause is determined [1]. The International Association for the Study of Pain (IASP) defines it as “…an unpleasant feeling and emotional experience associated with actual or possible tissue damage or potential damage” [2]. Each patient perceives pain differently - depending on the irritant, previous experience and current psychological and physical state. The factors that cause pain cannot be ignored. They affect our behavior and mental activity, causing anxiety and/or depression [3,4]. Management of mild to moderate pain has traditionally relied on the use of nonsteroidal anti-inflammatory drugs (NSAIDs) and the synthetic non-opioid analgesic paracetamol (acetaminophen). In cases of persistent syndrome and increased pain, it is possible to take weak opioids (such as codeine, dextropropoxyphene or tramadol) and even stronger opioids (such as morphine or fentanyl) together with NSAIDs or paracetamol. NSAIDs play a major role in the relief of pain in acute and chronic rheumatic diseases, as well as pain in the postoperative period (unlike paracetamol, these drugs can also relieve inflammation associated with these types of pain). The well-known gastrointestinal side effects of NSAIDs can be reduced by careful monitoring of dosages and duration of treatment, adequately prescribed treatment, and administered concomitantly with NSAIDs. On the other hand, to reduce side effects and complications from the gastrointestinal tract, selective cyclooxygenase-2 (COX-2) inhibitors have been developed. Unfortunately, large-scale studies have revealed that these substances have a potential even more serious side effect - cardiovascular complications. The European Medicines Agency (EMA) and the Food Supplement and Drug Administration (FDA) of the United States have developed standards regarding the need for caution and certain restrictions when prescribing COX-2 inhibitors, especially to patients with increased cardiovascular risk and for long-term use.
Lysine salt of ketoprofen
Ketoprofen is an NSAID of the family of propionic acid derivatives with analgesic, anti-inflammatory and antipyretic effects [5]. It is a racemic mixture, of which only the S isomer inhibits cyclooxygenase; the R-isomer has a much lower ability to do this [6,7]. Solification of ketoprofen with a lysine amino acid makes it possible to improve the pharmacological characteristics of the molecule [8,9]. In particular, the lysine salt of ketoprofen (LSK) has greater solubility than ketoprofen; this promotes accelerated and more complete absorption of the active substance. Consequently, a high peak concentration of the substance in the blood serum is achieved as quickly as possible - after 15 minutes. after oral administration of LSC (when taking ketoprofen this occurs after 60 minutes) (Fig. 1) [10–12]. Such a rapid increase in plasma LSC concentration further accelerates pharmacological activity. The pronounced analgesic effect of LSC appears within 30 minutes. after the first dose (statistically significant compared with placebo) [13]. In addition, the high solubility of LSC in aqueous media allows the administration of injectable drugs with a similar physiological pH level (without the need for preservatives) with a minimum of irritation reactions and tissue damage at the injection site. The main mechanism of the analgesic effect of LSC is the inhibition of cyclooxygenase (COX), and therefore a decrease in the production of prostaglandin E2 (PGE2). In addition to its effect on COX, ketoprofen inhibits the lipoxygenase pathway of the arachidonic acid cascade [14], leading to a decrease in the synthesis of leukotrienes. It is worth noting that the lysine salt of ketoprofen has both peripheral and central effects [15] due to the inhibition of PGE2 biosynthesis [16,17]. In this case, inhibition of nitric oxide synthase and COX occurs in the brain. Thus, the lysine salt of ketoprofen easily and quickly penetrates the central nervous system, passing the blood-brain barrier within 15 minutes. (due to the high level of lipophilicity) [18]. Recently, experts have demonstrated that the lysine salt of ketoprofen interacts with the 5-HT system. This suggests that this characteristic is a possible explanation for the high effectiveness of this drug compared to other NSAIDs [7,15,19]. These properties allow us to evaluate the lysine salt of ketoprofen as a means to reduce the symptoms of pain during inflammation of the musculoskeletal system that occurs in conditions of both acute and chronic disease [20]. As an NSAID, it is a powerful and highly effective agent for reducing pain in injuries, orthopedic and rheumatic pathologies due to its anti-inflammatory and analgesic properties [21].
Ketoprofen-Lor rinse solution 16 mg/ml bottle, 200 ml
Registration Certificate Holder
PHARMSTANDARD-LEKSREDSTVA (Russia)
Dosage form
Medicine - Ketoprofen-ENT (Ketoprofen-LOR)
Description
Rinse solution
transparent, bluish-green to green in color, with a characteristic mint odor.
1 ml
ketoprofen lysine salt 16 mg
Excipients
: glycerol - 200 mg, ethanol - 40 ml, methyl parahydroxybenzoate (nipagin) - 1.5 mg, levomenthol - 0.7 mg, sodium saccharinate - 2 mg, sodium hydrogen phosphate dodecahydrate - 0.78 mg, mint flavor - 2.4 mg, brilliant green - 0.016 mg, water purified - up to 1 ml.
150 ml - bottles (1) - cardboard packs. 200 ml - bottles (1) - cardboard packs.
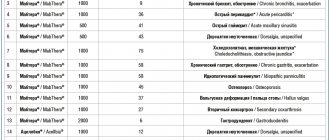
Indications
Articular syndrome (rheumatoid arthritis, osteoarthritis, ankylosing spondylitis, gout); symptomatic treatment of inflammatory and degenerative diseases of the musculoskeletal system (periarthritis, arthrosynovitis, tendonitis, tenosynovitis, bursitis, lumbago), pain in the spine, neuralgia, myalgia. Uncomplicated injuries, in particular sports injuries, sprains, sprains or ruptures of ligaments and tendons, bruises, post-traumatic pain.
As part of combination therapy for inflammatory diseases of the veins, lymphatic vessels, lymph nodes (phlebitis, periphlebitis, lymphangitis, superficial lymphadenitis).
Contraindications for use
Hypersensitivity to ketoprofen, as well as salicylates or other NSAIDs;
complete or incomplete combination of bronchial asthma, recurrent polyposis of the nose and paranasal sinuses and intolerance to acetylsalicylic acid or other NSAIDs (including a history); peptic ulcer of the stomach or duodenum in the acute phase; ulcerative colitis, Crohn's disease; hemophilia and other bleeding disorders; severe liver failure; severe renal failure (creatinine clearance less than 30 ml/min), confirmed hyperkalemia, progressive kidney disease; decompensated heart failure; postoperative period after coronary artery bypass surgery; gastrointestinal, cerebrovascular and other bleeding (or suspected bleeding); chronic dyspepsia; III trimester of pregnancy; breastfeeding period; children under 15 years of age; for rectal use - inflammatory diseases of the rectum and/or bleeding from the rectum; for external use - weeping dermatoses, eczema, infected abrasions, wounds. With caution:
history of peptic ulcer, presence of Helicobacter pylori infection; history of bronchial asthma; clinically significant cardiovascular, cerebrovascular and peripheral arterial diseases; dyslipidemia; moderate liver failure, hyperbilirubinemia, alcoholic cirrhosis of the liver; chronic renal failure (creatinine clearance 30-60 ml/min); chronic heart failure (II-IV FC according to NYHA classification); arterial hypertension; blood diseases; dehydration; diabetes; smoking; elderly age; long-term use of NSAIDs, simultaneous use of anticoagulants (including warfarin), antiplatelet agents (including clopidogrel), oral corticosteroids (including prednisolone), selective serotonin reuptake inhibitors (including fluoxetine, paroxetine, citalopram, sertraline).
pharmachologic effect
NSAID, propionic acid derivative. It has analgesic, anti-inflammatory and antipyretic effects. The mechanism of action is associated with inhibition of the activity of COX, the main enzyme in the metabolism of arachidonic acid, which is a precursor of prostaglandins, which play a major role in the pathogenesis of inflammation, pain and fever.
The pronounced analgesic effect of ketoprofen is due to two mechanisms: peripheral (indirectly, through suppression of prostaglandin synthesis) and central (due to inhibition of prostaglandin synthesis in the central and peripheral nervous system, as well as the effect on the biological activity of other neurotropic substances that play a key role in the release of pain mediators in the spinal cord). brain). In addition, ketoprofen has antibradykinin activity, stabilizes lysosomal membranes, and causes significant inhibition of neutrophil activity in patients with rheumatoid arthritis. Suppresses platelet aggregation.
Drug interactions
When ketoprofen is used simultaneously with other NSAIDs, the risk of developing erosive and ulcerative lesions of the gastrointestinal tract and bleeding increases; with antihypertensive drugs (including beta-blockers, ACE inhibitors, diuretics) - their effect may be reduced; with thrombolytics - increased risk of bleeding.
When used simultaneously with acetylsalicylic acid, it is possible to reduce the binding of ketoprofen to plasma proteins and increase its plasma clearance; with heparin, ticlopidine - increased risk of bleeding; with lithium preparations - it is possible to increase the concentration of lithium in the blood plasma to toxic levels due to a decrease in its renal excretion.
When used simultaneously with diuretics, the risk of developing renal failure increases due to a decrease in renal blood flow caused by inhibition of prostaglandin synthesis and against the background of hypovolemia.
When used simultaneously with probenecid, the clearance of ketoprofen and its binding to plasma proteins may be reduced; with methotrexate – the side effects of methotrexate may increase.
With the simultaneous use of warfarin, severe, sometimes fatal bleeding may develop.
Dosage regimen
Set individually depending on the clinical situation.
Used orally, intramuscularly, intravenously (as an infusion), rectally or externally in appropriate dosage forms.
Side effect
From the digestive system:
pain in the epigastric region, nausea, vomiting, constipation or diarrhea, anorexia, gastralgia, liver dysfunction; rarely - erosive and ulcerative lesions of the gastrointestinal tract, bleeding and perforation of the gastrointestinal tract.
From the side of the central nervous system:
headache, dizziness, tinnitus, drowsiness.
From the urinary system:
renal dysfunction.
Allergic reactions:
skin rash; rarely - bronchospasm.
Local reactions:
when used in the form of suppositories, irritation of the rectal mucosa and painful bowel movements are possible; when used in gel form - itching, skin rash at the site of application.
special instructions
With long-term use of NSAIDs, it is necessary to periodically evaluate a clinical blood test, as well as monitor kidney and liver function, especially in elderly patients (over 65 years), and conduct a stool test for occult blood. It is necessary to be careful and monitor blood pressure more often when using ketoprofen to treat patients suffering from arterial hypertension and cardiovascular diseases that lead to fluid retention in the body.
If visual disturbances occur, treatment should be stopped immediately.
Like other NSAIDs, ketoprofen can mask the symptoms of infectious and inflammatory diseases. If signs of infection or deterioration in health while using the drug are detected, the patient should immediately consult a doctor.
If there is a history of contraindications from the gastrointestinal tract (bleeding, perforation, peptic ulcer), in the case of long-term therapy and the use of ketoprofen in high doses, the patient should be under close medical supervision.
Because of the important role of prostaglandins in maintaining renal blood flow, particular caution should be exercised when using ketoprofen in patients with cardiac or renal failure, as well as in the treatment of elderly patients taking diuretics and patients who have a decrease in blood volume for any reason (eg , after surgery).
Effect on the ability to drive vehicles and machinery
During treatment, drowsiness, dizziness or other unpleasant sensations from the nervous system, including blurred vision, may occur. When using ketoprofen, patients should be careful when driving vehicles and engaging in other potentially hazardous activities that require increased concentration and speed of psychomotor reactions.
Use during pregnancy and breastfeeding
Restrictions during pregnancy - Contraindicated. Restrictions when breastfeeding - Contraindicated.
Contraindicated for use in the third trimester of pregnancy. In the first and second trimesters of pregnancy, the use of ketoprofen is possible in cases where the potential benefit to the mother outweighs the potential risk to the fetus.
If it is necessary to use ketoprofen during lactation, it is recommended to stop breastfeeding.
Use for renal impairment
Restrictions for impaired renal function - Contraindicated.
Contraindications for oral administration are severe renal dysfunction.
Use with extreme caution in patients with kidney disease. During treatment, systematic monitoring of renal function is necessary.
Use for liver dysfunction
Restrictions for liver dysfunction - Contraindicated.
Contraindications for oral administration are severe liver dysfunction.
Use with extreme caution in patients with liver disease. During treatment, systematic monitoring of liver function is necessary.
Use in children
Restrictions for children - Contraindicated.
Contraindicated under the age of 15 years (for retard tablets).
The use of ketoprofen in chronic rheumatic diseases
Osteoarthritis (OA) is the most common joint disease. In the study, 113 patients with symptoms of coxarthrosis underwent a 4-week course of comparative treatment with oral administration of ketoprofen or indomethacin. The study showed a significant effect in reducing pain and improving joint function, thereby improving the quality of life of patients. At the same time, taking ketoprofen turned out to be safer: fewer patients suffered from side effects or dropped out of the study [22]. Good effectiveness of oral administration of LSC has been shown in patients with OA: improvement was observed in 67.6% of patients [23]. Moreover, the analgesic effectiveness of LSC in acute conditions was higher than that of acetylsalicylic acid: the level of β-endorphin circulation in plasma was higher, and the level of substance P was lower. These data suggest that the rapid and continuous analgesic effect of the drug in patients with OA may be associated specifically with the level of β-endorphin and substance P in the circulatory system [24]. Rheumatoid arthritis (RA) is a chronic inflammatory disease of peripheral joints, often leading to tissue degradation and destruction of bone and cartilage [25]. Therapy is aimed at eliminating the inflammatory consequences of autoimmune activation using antirheumatic drugs that modulate the disease (“basic”). Systemic glucocorticoids are effective for short-term relief of pain and synovitis. Analgesics are used to reduce pain at all stages of the disease, often in combination with other treatments to control the inflammatory process. NSAIDs reduce pain and stiffness quickly without affecting the course of the disease. Numerous data indicate that both classical NSAIDs and those selective for COX-2 are better at relieving active signs and symptoms of RA than simple analgesics [26]. An open-label, 1-week study of 26 patients with RA and persistent synovitis of the knee demonstrated that treatment with LSC and naproxen (NA) significantly reduced pain and improved other clinical parameters [27]. Moreover, the level of synovial prostaglandin 2 (PGE2) decreased significantly, especially as a result of taking LSC, by 62.8% (for naproxen by 51.7%, respectively). The overall effectiveness and tolerability of both courses of treatment were almost identical (slightly higher for LSC). The authors concluded that the use of LSC should be recommended for the symptomatic treatment of RA, since this study confirms the pronounced analgesic and anti-inflammatory effect, as well as the active inhibitory effect of LSC on the level of PG in the joint fluid (even compared with naproxen). In another study involving 34 patients with rheumatic diseases (20 of them had RA), experts noticed that oral administration of LSC significantly reduced pain. There was a significant reduction in spontaneous pain (p<0.001), pressure tenderness, functional limitations and duration of morning stiffness within 10 days of treatment in all study patients [23]. Moreover, in 10 patients with persistent synovitis of the knee, LSC also successfully penetrated into the synovial fluid, significantly reducing the level of PGE2 in it (inhibition was about 73%). For elderly patients, these data are of particular importance. They often suffer from rheumatic diseases such as OA and RA, which are associated with various associated conditions, and usually require long-term use of NSAIDs. Therefore, the issue of long-term use is important regarding the safety of treatment. It should be said that ketoprofen has been evaluated in extensive studies involving a group of elderly patients. In particular, a prospective study conducted to determine the safety profile of ketoprofen over 12 months. involving 823 patients over 65 years of age (with OA and RA; taking ketoprofen orally), showed the following. At the end of the study, 521 (63.3%) patients remained on the same therapy. Oral ketoprofen is safe for elderly patients with arthritis over a long period of time. Pain reduction and safety rates were similar to those seen in younger patients [28]. The safety of ketoprofen for use in the elderly was assessed in a large open-label study involving approximately 20,000 elderly patients (over 60 years of age) suffering from various rheumatic diseases. Oral ketoprofen for 4 weeks provided overall effectiveness, rated by physicians as “excellent”/“good” in 74% of cases, with a “very good” risk-benefit ratio in older patients compared with the rest of the population [29]. Gout is an acute inflammatory joint disease that affects 1–2% of adults in industrialized countries. It occurs when uric acid crystals accumulate in joints and other tissues [30–32]. With gout, recurrent attacks of acute arthritis often occur. Sometimes this leads to chronic arthropathy, salt deposits and kidney disease. Gout is also associated with a number of comorbid conditions, such as cardiovascular disease, chronic kidney disease and metabolic syndrome [32]. Standard treatments for acute gout attacks include glucocorticoids, NSAIDs, and colchicine [32–34]. To study the effect of ketoprofen in gouty arthritis, several studies have been conducted, showing that intramuscular or oral administration of ketoprofen for 1 week. effectively, quickly and significantly reduces pain [35,36]. In a 7-day, multicenter, double-blind study conducted to compare the effects of oral ketoprofen and indomethacin in 59 patients with acute gouty arthritis, more than 90% of patients reported a decrease in pain within 1 day of taking the drug. At the end of the study period, the majority of patients in both groups showed significant improvement (assessed by both the investigators and the patients themselves). In addition, the researchers concluded that ketoprofen can relieve pain in acute gouty arthritis within 24 hours with the same effectiveness, but with fewer side effects, than indomethacin, which is routinely prescribed for this condition [37].
Taking lysine salt of ketoprofen for acute rheumatic and traumatic diseases
Acute rheumatic and traumatic diseases, soft tissue injuries are often accompanied by pain, swelling and inflammation. These include: sprains, tendonitis, bursitis (eg, lateral epicondylitis (tennis elbow), regional musculofacial pain syndrome, low back pain, and neurovascular impingement (eg, carpal tunnel syndrome and superior outlet syndrome). A double-blind clinical trial of oral LSA (80 mg/3 times daily) was conducted versus placebo in 120 patients with soft tissue disorders (tendonitis, bursitis and periarthritis). associated with pain, functional impairment and painful sensitivity to any touch, as well as a rapid and pronounced reduction in pain itself. The analgesic effect of LSC became significant within 30 minutes after administration (Fig. 2). Moreover, due to adverse reactions to the drug not a single patient dropped out. It was noted that the drug was truly safe - just like placebo. In conclusion, it is worth saying that for patients with soft tissue diseases, oral administration of LSC (as the study showed) is effective and safe [38]. Another comparative multicenter study aimed to determine the effectiveness and tolerability of ketoprofen and diclofenac sodium in acute rheumatic and traumatic conditions. In 180 patients who took ketoprofen or diclofenac for 15 days (first in the form of intramuscular injections, then orally), a decrease in pain symptoms was noted. Ketoprofen is recognized as more effective as an analgesic used in most pathological conditions. The study also showed that ketoprofen was better tolerated than diclofenac. It is rated “excellent/good” based on the results obtained in the largest percentage of patients [39]. To compare the analgesic effect of 1-week administration of ketoprofen (50 mg/3 times daily orally) and ibuprofen (600 mg/2 times daily orally), a multicenter, double-blind study was conducted involving 165 patients with sports injuries. In these patients, the resulting injuries have caused a range of painful lesions such as tendinitis or tenosynovitis, epicondylitis, traumatic bursitis, sprain, or contusion. The results obtained showed that after the first (oral) dose, ketoprofen reduces pain significantly faster (by 1.1 hours) compared to ibuprofen. It also turned out that the maximum pain reduction score for ketoprofen was much higher. Within 6 hours, 76% of patients taking ketoprofen experienced a 50% reduction in pain; for those taking ibuprofen, the rate was 58% (p<0.05). The maximum degree of pain reduction was achieved faster with ketoprofen than with ibuprofen (Fig. 3) [40].
Lower back pain
Low back pain is one of the most common conditions encountered in clinical practice. The main method of treatment is medication. In terms of duration, acute low back pain is usually defined as a symptom that persists for at least 6 weeks, subacute pain - from 6 to 12 weeks, chronic low back pain - from 12 weeks. and longer. For most patients, regardless of how long symptoms last, paracetamol (acetaminophen) and NSAIDs are the first choice pain reliever. The results of oral and intramuscular ketoprofen have been studied in a number of different clinical studies involving patients suffering from lumbago. A comparative 1-week study of the effectiveness and tolerability of intramuscular ketoprofen and indomethacin involved 115 patients with acute low back pain. The study results showed that ketoprofen significantly reduced overall pain and provided more durable pain relief than indomethacin. In addition, it should be noted that already 1 hour after administration, more patients in the ketoprofen group experienced a significant reduction in pain than in the group taking indomethacin (61 and 46.9%, respectively) [41]. Another study of 155 patients with chronic low back pain found that oral ketoprofen (150 mg twice daily) produced higher rates of improvement than diclofenac (75 mg twice daily) after 1 day. weeks after reception. This means that thanks to ketoprofen, pain relief occurred earlier than when taking diclofenac (in 71.4 and 62.36% of patients, respectively).




![Table 1. Bioavailability (absorption) of various organic forms of calcium within 2 hours after oral administration in the experiment [22]](https://laram-halal.ru/wp-content/uploads/tablica-1-biousvoyaemost-absorbciya-razlichnyh-organicheskih-form-kalciya-v-techenie-330x140.jpg)