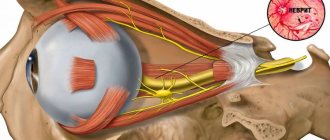
One of the common reasons why a person comes to see an ENT doctor is hearing loss. And often hearing loss is a consequence of damage to the nerve fibers in the inner ear.
The auditory nerve suffers under the influence of unfavorable factors - inflammatory processes in the peripheral part of the auditory system, toxic substances, injuries, etc. This disease is called neuritis of the auditory nerve (cochlear neuritis, sensorineural hearing loss).
The disease can occur in both acute and chronic forms. And depending on the degree of nerve damage, it leads to disturbances in auditory perception from moderate hearing loss to complete deafness. Therefore, it is so important to diagnose the disease in time and begin treatment.
Why does cochlear neuritis occur?
Otolaryngologists often name the main causes of the disease:
- infectious diseases;
- inflammation in the outer or middle ear;
- pathologies of the cardiovascular system, including hypertension;
- endocrinological diseases, metabolic diseases;
- traumatic injuries of the skull;
- poisoning by toxins;
- prolonged noise or vibration exposure;
- tumor diseases.
Sensorineural hearing loss is most often diagnosed in men over 50 years of age, as well as in residents of large cities.
Diagnostics
Diagnosis of acoustic neuritis, as a rule, does not cause significant difficulties and is based on a thorough history, examination and additional examination of the patient. Treatment is conservative and depends on the etiological factors, clinical picture, and nature of the disease. It must be remembered that the success of treatment measures and the prognosis in general depend on the time of initiation of proper treatment. In acute conditions, first aid consists of emergency measures aimed at relieving intoxication, inflammation, vascular disorders, etc. In addition to emergency specific treatment, ENT doctors also carry out complex vitamin therapy, the introduction of neuroprotectors, and symptomatic treatment of the underlying disease that caused the occurrence of auditory neuritis.
Symptoms of acoustic neuritis
The main symptom of the disease is hearing loss. Both complete and partial: for example, some patients stop hearing sounds of a certain frequency, perceive the speech of the interlocutor as unintelligible, and note noise or ringing in the ears.
Other symptoms include:
- general weakness,
- temperature increase,
- earache,
- problems with the vestibular system - imbalance, dizziness, nausea or vomiting.
4.Treatment
Effective etiotropic therapy is possible only in cases where the causes of nerve damage are identified and when these causes are reversible. In different situations, neurological, antibiotic, antiviral, and physiotherapeutic treatment is prescribed (the role and possibilities of the latter are very large and have not been sufficiently studied to date). In some cases, hearing is restored after surgery, which eliminates, for example, the factor of mechanical pressure on the nerve.
According to data published today, significant improvement or complete restoration of hearing function can be achieved in approximately 80% of cases. If all measures taken are ineffective, a hearing aid is selected; The characteristics and design of modern high-tech digital models can radically reduce the psychological, social and professional limitations caused by hearing loss.
Slüder syndrome – Neurosurgery Kyiv
Ganglionitis of the pterygopalatine ganglion (Slüder syndrome) is an inflammatory neuralgia that affects the peripheral nerve endings of the pterygopalatine ganglion.
The main reason for the development of pathology is inflammation in the paranasal sinuses, but the risk of ganglionitis in the presence of extensive caries and inflammatory processes in the nasopharynx cannot be excluded.
Depending on which part of the pterygopalatine node is affected by inflammation, three types of pathology are distinguished:
- destruction of somatic nerve fibers carrying innervation from the mucous membranes of the mouth, cheeks, and gums;
- pathology of parasympathetic fibers responsible for the perception of taste and secretion of the salivary glands;
- destruction of sympathetic fibers.
Causes
Ganglionitis of the pterygopalatine node occurs, in most cases, as a consequence of pathological processes in the ENT organs, for example, sinusitis or frontal sinusitis. Considering the fact that the pterygopalatine ganglion is located close to the ethmoidal nasal labyrinths, their inflammation can also affect it.
Ganglionitis of odontogenic type occurs due to dental diseases:
- caries;
- periodontitis;
- pulpitis;
- Therefore, dentists often begin to treat pathology first of all, removing teeth affected by caries in order to relieve pain.
- Maxillofacial injuries are another common cause of ganglionitis, especially if there is a fracture of the cheek bones.
- People at risk of developing pathology include:
- alcohol abusers;
- smokers a lot;
- subject to constant stress.
Factors provoking inflammatory neuralgia of the pterygopalatine ganglion:
- chronic fatigue syndrome;
- constant lack of sleep;
- frequent presence in very noisy rooms (for example, in production).
All these factors lead to the imbalance between the processes of inhibition and excitation of the central nervous system, which is often the cause of neuralgia.
Ganglionitis of the pterygopalatine ganglion develops in the presence of oncological tumors that are located behind the jaw, due to injuries to the nasal septum, leading to its curvature. Diseases such as syphilis, viral pathogenic microflora, purulent tonsillitis, and jaw abscesses provoke the development of ganglionitis of the pterygopalatine node.
Symptomatic picture of ganglionitis of the pterygopalatine ganglion
The main and very first sign of pathology, which is characteristic of all types of neuralgia, is severe pain.
Reasons not related to neurology
Most often, ears become blocked due to infectious inflammation of the mucous membrane of the Eustachian tube (eustachitis) or the outer, middle, inner ear (otitis). Diseases develop against the background of acute respiratory viral infections, sinusitis, laryngitis, pharyngitis, tonsillitis.
Shpidonov Gennady Stanislavovich
Neurologist
Rostov State Medical University (neurology)
10 years of experience
Ear congestion and decreased hearing quality occur with traumatic brain injuries, damage to the eardrum, and intracranial tumors of cerebral tissue.
Natural factors that cause discomfort in the ear canals are the entry of water or a foreign body, cerumen plug, intensive release of mucus from the nose (blowing the nose). Many people experience ear congestion when climbing to a height. This is a normal physiological response to pressure changes. Unpleasant sensations go away on their own and, usually, without consequences.
Diagnosis of ear congestion in neurology
When the ear becomes clogged, pain and extraneous noise appear in the ear canal, people turn to an otolaryngologist. ENT diagnostics includes:
- instrumental examination - otoscopy;
- assessment of hearing indicators - audiometry (speech, tonal and threshold, suprathreshold);
- specific tests (Toynbee, Valsalva, empty throat);
- identification of infectious pathogens - bacterial culture of discharge from the external auditory canal.
If, during the examination, the ENT doctor establishes (suggests) a neurological etiology of the symptoms, the patient is referred to a neurologist. To make a diagnosis:
- Questioning the patient. It is necessary to find out the nature and duration of pain, their initial localization and area of irradiation, as well as the factors causing a painful attack and accompanying symptoms.
- Examination of the patient. The doctor pays attention to palpation of specific pain areas on the head - the areas where the branches of the trigeminal nerve exit and the auricular ganglion joins it (Balle's point, Richet's point). Normally, pressing on them causes moderate pain; in neurological cases, it causes sharp, piercing pain.
- Ultrasound of the parotid salivary gland. Evaluates structural changes (if any).
- Magnetic resonance imaging. Neuroimaging allows us to exclude other causes of pain and the presence of neoplasms.
- Electroneuromyography. Performed to determine the sensitivity threshold of trigger zones and the degree of nerve damage.
If the cause of neuralgia is not related to diseases of the ENT organs, a dental examination is necessary.
If signs of a tumor are detected on MRI, a consultation with an oncologist or neurosurgeon is prescribed.
Risk factors
- Genetic factor, family history of hearing loss
- Fetal hypoxia
- Low fetal weight at birth <1500g
- Premature birth, threat of miscarriage during pregnancy
- Gilbert's syndrome (congenital liver disease)
- Neurological disorders (Charcot-Marie-Tooth syndrome, Friedreich's ataxia)
- Neurofibromatosis type 2 (genetic disease of the nervous system)
- Infectious diseases (influenza, mumps)
- Exposure to chemicals or drugs (aminoglycosides, loop diuretics) that are ototoxic
Auditory neuropathy
TABLE OF CONTENTS
1. Levels of damage to the structures of the auditory organ in SSN 2. Symptoms of auditory neuropathy syndrome 3. Causes of auditory neuropathy syndrome 4. Prevalence of auditory neuropathy syndrome 5. Auditory screening (detection) of auditory neuropathy syndrome 6. Comprehensive diagnosis of auditory neuropathy syndrome 7. Clinical manifestations of SSN 8. Rehabilitation of children with auditory neuropathy syndrome 9. Experience of the AURORA™ Medical Center in the diagnosis and rehabilitation of children with auditory neuropathy syndrome 10. Description of clinical cases 11. In what cases should you contact the AURORA™ Medical Center for diagnosis of auditory neuropathy syndrome
Objectively, audiometrically, SSN is characterized by the presence of otoacoustic emissions (OAE) and/or microphone potential (MP) of the cochlea of the inner ear and the absence or greater impairment of short-latency auditory evoked potentials (SLEP).
What does the presence of OAE and/or MP and the absence of KSVP indicate? Recall that outer hair cells (OHCs) ( Figure 1 ) amplify vibrations of the basilar membrane of the cochlea of the inner ear and, in the process of amplification, generate otoacoustic emissions (OAEs), which are conducted from the cochlea through the oval window, the ossicles, and the basilar membrane into the external auditory canal. Internal hair cells (IHC), under the influence of vibrations of the basilar membrane, produce electrical potentials that cause the release of a special chemical substance (transmitter) into the synapses (contacts) between the IHC and the short processes (dendrites) of nerve cells (neurons) of the auditory nerve. The transmitter causes electrical excitation in the dendrite and neuron body of the auditory nerve, located in the spiral ganglion. Further, the electrical excitation spreads along the long process (axon) of the auditory nerve to the cochlear nucleus and from it - through the nerve structures of the hearing organ of the brain stem and subcortical structures - into the auditory zone of the cerebral cortex.
Figure 1. Diagram of the organ of Corti of the cochlea. Adapted by E.V. Sokolova.
It follows that objective audiometric data on OAE, MP and SEP indicate the following characteristics of auditory neuropathy:
- The presence of OAEs and MPs of the cochlea indicates normal functioning of the middle ear and external hair cells (OHC) of the cochlea of the inner ear.
- The absence or severe impairment of CVEP indicates a violation of: (a) the generation of nerve impulses by the internal hair cells (IHCs) of the cochlea of the inner ear, (b) the transmission of nerve impulses through synapses (contacts) between the IHCs and auditory nerve fibers, and (c) the conduction of nerve impulses auditory nerve fibers.
Levels of damage to the structures of the hearing organ in SSN
The occurrence of SSN can be caused by damage to various structures of the auditory analyzer, in particular:
- inner hair cells (IHC);
- synapses between the VVC and short processes (dendrites) of auditory nerve neurons;
- dendrites and axons of the auditory nerve, spiral ganglion cells;
- brainstem sections of the hearing organ;
- a combination of the above localizations.
Manifestation of auditory neuropathy syndrome
The clinical manifestations of SHF are varied and may differ between patients. These include:
- Hearing impairment from slight to profound hearing loss and deafness.
- Instability of hearing thresholds – temporary improvements and deterioration of hearing.
- Discrepancy between speech perception impairment and tonal hearing thresholds.
- Impaired speech perception in noise compared with speech perception in sensorineural hearing loss with the same hearing loss.
- Impaired speech perception with normal thresholds of hearing tones.
- Delayed speech development.
The severity of manifestations varies - from a complete lack of reaction to sound to minor hearing impairment and speech perception.
When conducting a comprehensive audiometric examination of children with SSN, one sign is revealed that is common to all children suffering from this pathology - the results of audiometric tests indicate normal function of the outer hair cells and a gross disruption of the conduction of nerve impulses by the auditory nerve.
Characteristic signs of SSN are the presence of normal evoked otoacoustic emissions (OAE) and microphonic potential (MP) of the cochlea, indicating preserved function of the outer hair cells. The presence of caused OAE is a variable diagnostic feature, as in approximately 30% of children with SUD, OAE eventually ceases to be detected for as yet unknown reasons. At the same time, the microphone potential (MP) of the cochlea of the inner ear is preserved and is a persistent diagnostic sign of SSN.
Figure 2. Microphone potential (MP) recorded in a child with auditory neuropathy during recording of CVEP. The microphone potential (MP) of the cochlea of the inner ear is recorded, but the SEP waves are not recorded. Adapted by E.V. Sokolova from Guidelines for Cochlear Microphonic Testing. Ver. 2.0. 20 Sept. 2011. NHSP Clinical Group.
Another important diagnostic feature of SSN is a gross disruption of the conduction of nerve impulses along the auditory nerve and subcortical structures of the auditory analyzer, which manifests itself in the absence or significantly altered SEP. In most cases, the results of CVEP show a complete absence of characteristic peaks. In some cases, at high levels of stimulation (above 70 dB nHL), it is possible to register the fifth wave of SEP (wave V) with low amplitude and greatly extended latency - with a long delay compared to the latency in sensorineural hearing loss with the same hearing loss.
The acoustic reflex of the intraaural muscles is most often not recorded. This is explained by the fact that in auditory neuropathy syndrome, the conduction of a nerve impulse along the afferent arc of the acoustic reflex is blocked or desynchronized. In some cases, the acoustic reflex is recorded at high levels of stimulation (Berlin C et al., 2010).
The results of subjective audiometry are characterized by a variety of hearing loss - from normal hearing thresholds to deafness. Speech intelligibility is impaired to varying degrees - from slight to complete lack of understanding of speech. Speech-tone dissociation is characteristic - according to G. Rance (2007), in more than half of cases of SSN, speech intelligibility is worse than expected based on the results of threshold pure-tone audiometry. Speech intelligibility in noise is impaired - there is a significant difficulty in understanding speech against the background of even slight noise.
Causes of auditory neuropathy syndrome
SHF is a multi-etiological disease, that is, it has various causes. It has been established that risk factors for SHF in children are:
- heredity, genetic changes;
- prematurity;
- anoxia;
- low birth weight;
- intrauterine infection;
- hyperbilirubinemia (newborn jaundice);
- congenital absence/aplasia of the auditory nerve;
- delay in anatomical and physiological maturation of the hearing organ.
Genetically determined hearing loss in SSN can be isolated or syndromic. Isolated genetic SUDs include disorders caused by mutations in the otoferlin and peivakin genes. Syndromic genetic disorders, one of the symptoms of which is SSN, may include Friedrich's ataxia, Charcot-Marie-Tooth disease, and Refsum disease.
One of the leading pathogenetic factors in the development of SHF is hyperbilirubinemia (jaundice) in newborns. Hyperbelirubinemia in newborns leads to pathological changes at the level of the brainstem nuclei with an intact (intact) cochlea of the inner ear.
SSN is diagnosed when the auditory nerve is underdeveloped or absent in the presence of a normally developed and normally functioning cochlea of the inner ear. In a computed tomography study, hypodevelopment or absence of the auditory nerve was found in 9 of 51 children with audiological signs of SUD (Buchman C., et al 2006).
In some newborns, auditory neuropathy may be temporary and a sign of immaturity or incomplete myelination (myelin coating) of neurons in the auditory system. In such cases, SSN goes away on its own and hearing becomes normal by 12–24 months of life.
Prevalence of auditory neuropathy syndrome
Studies in many countries around the world have identified auditory neuropathy syndrome in:
- 3% of newborns who fail hearing screening (screen positive)
- 19% of newborns with irreversible hearing impairment identified as a result of screening,
- 40% of newborns in the neonatal intensive care unit,
- 14.5% of children with hearing impairment,
- 8% of children with severe hearing loss.
Auditory screening (detection) of auditory neuropathy syndrome
In the late 1990s and early 2000s, the most widely used newborn hearing screening method in the United States and several other countries was otoacoustic emissions (OAE). But by the mid-2000s, the high prevalence of auditory neuropathy syndrome in newborns, in which OAE is present, began to become clear. Therefore, already in the 2007 Joint Committee on Infant Hearing Position Statement, it was prescribed that auditory screening in neonatal intensive care units and with risk factors for auditory neuropathy must be performed using short-latency auditory evoked potentials (SLEP). To avoid the risk of missing hearing loss during screening, many newborn hearing screening programs in the United States, Canada, Great Britain, the European Union, Turkey, and other countries began to use the HFRS hearing screening method for all newborns by the late 2000s.
This is what happened at the AURORA™ Medical Center: having begun to use UAE for auditory screening of newborns in the mid-2000s, as medical data on SHF accumulated by the end of the 2000s, AURORA™ completely switched to auditory screening of children using CVS.
Comprehensive diagnosis of auditory neuropathy syndrome
As noted above, the main feature of SSN is the combination of intact outer hair cell (OHC) function and impaired or absent auditory nerve function. To diagnose the condition of these structures, it is necessary to conduct appropriate examinations.
The scope of methods for diagnosing SSN was widely discussed by specialists from many countries around the world and was generally adopted at a special Symposium on auditory neuropathy syndrome as part of the International Conference on Hearing in Newborns in 2008 in Como (Italy) and continues to develop as data from evidence-based medicine accumulates.
Currently, the examination package for diagnosing SHF includes the following methods.
Audiological (audiological) diagnostics
Studies of the function of external hair cells (OHC) by recording the microphone potential (MP) of the cochlea of the inner ear using the method of recording CVEP and/or electrocochleography (ECoG) and evoked otoacoustic emissions (EOAE). Registered MP and VOEA indicate preserved function of the NVK.
Study of the function of the auditory nerve and subcortical structures of the auditory analyzer by recording SEP. SSN is characterized by the absence of CVEP or registration of abnormal CVEP (a single low-amplitude V wave can be recorded at high stimulation levels - above 80 dB nHL).
Study of conduction pathways by recording the acoustic reflex (AR) of the intraauricular muscles . A characteristic diagnostic sign of SSN is the absence of ipsi- and contralateral AR.
Determination of the degree of tonal hearing impairment . If possible, subjective audiometry is performed according to the child's age. Hearing thresholds may not differ from the norm or indicate varying degrees of hearing loss - from mild to deafness. Hearing thresholds may be unstable with repeated examinations. Therefore, when diagnosing SHF, it is advisable to perform repeated audiometry.
Identification of anatomical features of the structures of the cochlea, auditory nerve, brainstem structures of the auditory analyzer
The structural features of the cochlea of the inner ear, the auditory nerve and the brainstem structures of the hearing organ are determined using imaging - studies using computed tomography (CT) and magnetic nuclear resonance (MNR) . These studies allow, in particular, to identify congenital absence/aplasia of the auditory nerve.
Imaging studies are mandatory for children with suspected SHF and are carried out in specialized healthcare institutions upon the referral of doctors from the AURORA™ Medical Center.
Identification of concomitant diseases
Consultation of related specialists . Children with diagnosed SSN need to be examined by a neurologist (neurologist) to assess the function of peripheral and cranial (cranial) nerves. If necessary, a consultation with an ophthalmologist, endocrinologist, or cardiologist is also carried out.
For these examinations, children with SUD are referred to specialized healthcare institutions by doctors from the AURORA™ Medical Center.
Clinical manifestations of SHF
Delayed maturation of the auditory analyzer. SSN detected in infants and newborns may be a sign of delayed maturation of the hearing organ. In this case, after a thorough diagnosis and exclusion of severe pathology of the auditory nerve, hearing aids and monitoring of the child’s hearing condition are recommended, in particular, periodic examination of CVEP and behavioral audiometry every three months - until the age of 24 months , which is determined by the child’s individual rehabilitation plan at the AURORA™ Medical Center .
In the case of an individual delay in maturation of the auditory analyzer, hearing may normalize or improve by the age of 18-24 months. During this period, it is advisable to stimulate the auditory system with the help of hearing aids with mandatory monitoring of the state of the auditory system by objective methods (OAE, KSVP, AR) and auditory-speech development by a teacher of the deaf every three months.
Compensated form of SSN . Children with this form of CH develop the ability to adequately perceive speech and respond to non-speech signals in silence. But significant difficulties may arise in understanding speech against the background of even slight noise. Such children may be candidates for the use of FM systems, which increase the speech-to-noise ratio and significantly facilitate speech perception for such children.
Varying degrees of speech intelligibility impairment combined with impaired hearing thresholds . For mild to moderate speech intelligibility impairment, hearing aids can be effective. But in cases of severe speech intelligibility impairment, cochlear implantation is recommended - in the absence of contraindications.
There is no response to sound and is not restored . As a rule, this is due to the absence or severe damage to the auditory nerve. In this case, hearing aids and cochlear implantation are not effective. Such children should be integrated into the environment of the deaf and learn sign language.
Rehabilitation of children with auditory neuropathy syndrome
Hearing-speech rehabilitation of children with SSN is complicated by the following factors:
- Hearing thresholds cannot be determined from the results of the CVEP, since there are no CVEP.
- Hearing thresholds are not an indicator of speech intelligibility; There are frequent cases of speech-tonal dissociation (discrepancies between tonal thresholds and speech perception).
- The level of damage to the auditory system cannot always be determined during clinical audiological diagnostics.
- The success of auditory-verbal rehabilitation cannot be predicted by the results of threshold audiometry.
Established evidence-based medicine methods of auditory-speech rehabilitation of children with SSN are hearing aids and cochlear implantation . In particular, the results of an extensive study by Rance G. (2007) showed that hearing aids for children with SSN can improve speech intelligibility in 50% of prosthetized children. The AURORA™ Medical Center has also accumulated positive experience in providing hearing aid to children with SUDs.
The choice of rehabilitation method for children with SUD depends on the results of subjective (behavioral) audiometry. Children with elevated hearing thresholds should be advised to have a trial of hearing aids . Because hearing may change in young children with SLI, regular hearing monitoring is necessary to adjust the electroacoustic parameters of hearing aids. The child’s auditory-speech development should also be regularly assessed by a teacher of the deaf through questionnaires of parents and observation of the child.
Observation is especially important since hearing aids for children with SSN do not always lead to significant progress in the child’s auditory-speech development. Children with hearing aids who do not show progress in auditory-speech development are candidates for cochlear implantation. VERY IMPORTANT: the question of the advisability of cochlear implantation, which is an irreversible intervention, should be decided only after trial hearing aid and classes on the development of hearing and speech. Moreover, cochlear implantation of children with SSN does not provide a 100% guarantee of successful auditory-speech rehabilitation of children, especially in cases of hypoplasia of the auditory nerve and damage to the brainstem structures of the hearing organ.
Experience of the AURORA™ Medical Center in the diagnosis and rehabilitation of children with auditory neuropathy syndrome
The AURORA™ Medical Center for Auditory Rehabilitation has accumulated experience in diagnostics and auditory-speech rehabilitation of 45 children with SSN. The age of these children at the time of diagnosis ranged from 6 months to 10 years. Hearing loss, determined based on the results of subjective (behavioral) audiometry, ranged from hearing loss of the first degree to deafness according to the classification accepted in Ukraine. SHF was diagnosed using the methods described above. Observations were carried out every three months.
Three of these 45 children (7%) had normalized hearing to a socially adequate level and did not require further auditory rehabilitation.
Hearing replacement was provided to 24 of 45 children with SSN (53%) with modern digital hearing aids with an extended frequency range from Oticon (Denmark). Monitoring of children's hearing and speech development was carried out by a teacher of the deaf. The children's reaction to speech and non-speech sounds, speech understanding, comfort with hearing aid amplification, and speech development were assessed.
Hearing results . 19 children (42% of the entire SSN group and 79% of hearing aided children in this group) constantly use hearing aids. Of these, 17 children (38% of the entire SSN group and 71% of hearing aided children in this group) have a satisfactory level of auditory-speech development.
22 children out of 24 hearing aided children in the group with SSN have reached the appropriate age and are receiving education in the following way:
- seven children (16% of the group with SUD) attend public kindergarten,
- four children (9%) study in a comprehensive school,
- six children (13%) are raised at home,
- one child (2%) attends a kindergarten for the hearing impaired.
- one child (2%) is studying at a school for the deaf,
- two children (4%) are engaged in an individual plan due to the presence of concomitant diseases.
Thus, our experience indicates that hearing aids for children with SLI can lead to improved speech intelligibility (in our case in 71% of hearing aided children) and contribute to their successful social adaptation.
The experience of diagnosis and rehabilitation of children with SHF at the AURORA™ Medical Center was reported by the Chief Physician of the Medical Center, otolaryngologist-audiologist Elena Mikhailovna Khomenko at the Second Conference of the Ukrainian Association of Otiatrists, Otoneurosurgeons and Otoneurologists, held in Kyiv on September 13-14, 2012.
Description of clinical cases
The data was obtained by the Chief Physician of the AURORA™ Medical Center, otolaryngologist-audiologist Elena Mikhailovna Khomenko.
To maintain patient confidentiality, children's initials have been changed and dates of birth are not provided.
Child L.A.
The child’s parents contacted the AURORA™ Medical Center when the child was five years old.
History : The child was born premature, birth weight 900 grams.
Main complaint : Delay in speech development, the child’s speech is incomprehensible, does not pronounce many speech sounds.
Hearing test results ( Figure 3 ):
- No otoacoustic emissions were recorded in either the right or left ear.
- Acoustic reflexes were not recorded on both sides.
- When studying the KSEP recording method, the microphone potential (MP) of the cochlea of the inner ear was recorded, but there were no KSEP peaks.
- Children's play audiometry: bilateral damage to the sound-receiving apparatus, III degree hearing loss.
Diagnosis : Auditory neuropathy syndrome.
Auditory rehabilitation : The child received binaural hearing aids from Oticon Vigo BTE Power (Denmark). I took a course of classes with a teacher of the deaf on the development of hearing and speech. There has been significant progress in auditory-speech development.
Education : The child attends a public school.
Figure 3. Results of the child LA study. 1 – Examination using the KSVP method; Microphone potential (A) was recorded, VSEP peaks were not recorded. 2 - hearing thresholds determined using children's play audiometry. Observation of doctor E.M. Khomenko.
Child V.A.
The parents contacted the AURORA™ Medical Center when the child was 18 months old.
History : suffered hyperbilirubinemia (jaundice) of newborns, bilirubin level was 489 mmol/l.
Main complaint : Delayed speech development, poor response to sounds.
Hearing test results ( Figure 4):
- No otoacoustic emissions (OAE) were recorded in either the right or left ear.
- Acoustic reflexes (AR) were not recorded on both sides.
- When studying the CVEP recording method, the microphone potential (MP) of the cochlea of the inner ear was recorded; there were no CVEP peaks.
- Children's play audiometry: bilateral severe damage to the sound-receiving apparatus.
Diagnosis: Auditory neuropathy syndrome.
Auditory rehabilitation: The child received binaural hearing aids Oticon Safari 300 SP (Denmark). I took a course of classes with a teacher of the deaf on the development of hearing and speech. There has been significant progress in auditory-speech development.
Figure 4. Results of the VA child hearing test. The designations are the same as in Figure 3. Observation by doctor E.M. Khomenko.
In what cases should you contact the AURORA™ Medical Center for diagnosis of auditory neuropathy syndrome?
ATTENTION, PARENTS! An audiological (audiological) examination of children to identify SUDs is recommended in the following cases:
Children with delayed speech development.
Children of any age with risk factors for SUD:
- perinatal asphyxia of the child (breathing disorder) during childbirth;
- baby hypoxia (low oxygen levels in the blood) during childbirth;
- long-term artificial ventilation of the child;
- prematurity of the child;
- low birth weight of the child - less than 1500 grams;
- the child’s stay in the intensive care unit for five or more days;
- hyperbilirubinemia (jaundice) of newborns;
- diseases of demyelination of nerve fibers;
- heredity, genetic hearing impairments or suspicion of their presence, in particular peripheral neuropathies:
- Friedrich's ataxia, - Charcot-Marie-Tooth disease, - Refsum disease,
- traumatic brain injury of a child.
References:
1. Berlin C., Hood L., Morlet T., Wilensky D., Li L., Mattingly KR, Tailor-Jeanfreau J., Keats B., St. John P., Montgomery P., Shallop J., Russell B., Frisch S. Multi-site diagnosis and management of 260 cases with Auditory Neuropathy Auditory Dys-synchrony (Auditory Neuropathy Spectrum Disorder). Int. J. of Audiology 2010; 49, 30-43.
2. Rance G. Speech perception in noise for children with auditory neuropathy/dys-synchrony type hearing loss / G Rance, E. Barker, R. Dowell et al.// Ear. Hear. – 2007. – Vol. 28, N. 3. – P. 351-360.
Privatdozent Dr. Parvis Mir-Salim
Otorhinolaryngology
Head of the Department of Otorhinolaryngology
Specialization
- Ear surgery
- Functional endoscopic sinus surgery, head and neck surgery
- Extensive experience in cochlear implantation in children
- Master of Medicine degree at University Hospital Kigali, Rwanda
- Cochlear Implant Training in Nairobi, Kenya and Tartu, Estonia
- Video consultation
Show doctor's personal profile