Quick transition Treatment and prevention of recurrent cystitis
Recurrent cystitis is cystitis that occurs at least 3 times a year or at least 2 times within six months.
The most common causative agent of recurrent cystitis, as well as acute cystitis, is E. coli. Moreover, if E. coli is cultured, the likelihood of developing a repeat episode of the disease over the next 6 months is much higher than with cystitis, the causative agent of which is another bacterium.
The mechanism of development of recurrent cystitis is similar to the development of sporadic infection, that is, single episodes of acute cystitis.
Pathogenic bacteria from the rectal flora colonize the paraurethral zone and urethra and then enter the bladder.
Causes
The main role in the occurrence of recurrent cystitis is played by behavioral factors:
- frequent sexual intercourse;
- the use of antibiotics that negatively affect the intestinal and vaginal flora;
- the appearance of a new sexual partner within the last year.
The following are likely to develop recurrent cystitis:
- women who use a diaphragm with spermicide as contraception (the use of spermicidal-coated condoms by a partner also increases the risk of relapse);
- Postmenopausal women (often suffer from urinary tract infections).
Possible causes of recurrent cystitis:
- the presence of residual urine after urination associated with genital prolapse;
- a decrease in estrogen levels, leading to changes in the vaginal microflora, a decrease in the number of lactobacilli and an increase in the colonization of E. coli in the vagina;
- anatomical features of the location of the woman’s urethra (some women have a lower location of the urethra or increased mobility of the external opening of the urethra, causing its displacement into the vagina during sexual intercourse and the reflux of vaginal flora into the bladder, which causes so-called postcoital cystitis).
For doctors
Comparative analysis of the effectiveness of treatment of painful bladder syndrome/IC with intravesical instillations of sodium hyaluronate alone and in combination with oral administration of chondroitin sulfate 13.12.2018
Previous article
Aboyan I.A., Aboyan V.E., Pavlov S.V., Zinkovskaya O.V., Pavlov D.S.
Aboyan V.E. - Ch. doctor professor, doctor of medical sciences, Clinical Diagnostic Medical Institution, Rostov-on-Don, [email protected]
Painful Bladder Syndrome/ Interstitial Cystitis (BPS/IC)
is a chronic bladder condition. Modern studies and meta-analyses in recent years report an increase in the incidence of BPS/IC, currently amounting to 300 cases per 100,000.
Epidemiological studies clearly indicate the prevalence of BPS/IC in women - 2.7% of cases versus 1.7% in men.
Meanwhile, the etiology of BPS/IC still remains poorly understood. Researchers have proposed a large number of hypotheses. One of the most widely accepted theories is based on damage to the protective glycosaminoglycan (GAG) layer of the urothelium
.
The main chemical components of the GAG layer are hyaluronic acid (HA), heparin sulfate, chondroitin sulfate (CS), dermatan sulfate and keratin sulfate
. Disruption of the function of the GAG layer of the urothelium can lead to the penetration of both normal and pathological components of urine into the suburothelial lining, causing an inflammatory response that prevents the timely healing of the damaged urothelium.
This lesion can serve as a trigger for the subsequent cascade of inflammatory and neurogenic responses, leading to the appearance of pain, urination disorders and persistent changes in the structure of bladder tissue.
Based on the latest theory, to restore the protective properties of the damaged GAG layer
Various chemical agents are used, such as pentosan polysulfate, heparin sulfate, HA, CS or a combination of the above drugs.
HA is considered one of the main components of the GAG layer, and a number of studies show the effectiveness of instillation of HA into the bladder for BPS/IC. In addition, intravesical instillation of HA is recommended as one of the main types of therapy for BPS/IC in the latest versions of urological guidelines. At the same time, cholesterol is also used in the treatment of BPS/IC quite widely and with good results.
Unlike GC, CS is available both in the form of intravesical instillations and as an oral preparation. The bioavailability of oral cholesterol is low, however, taking the drug does not require a patient visit to a medical facility, which makes such therapy more convenient for the patient and reduces the cost of its use.
In the available literature there is a sufficient number of studies comparing the effectiveness of the use of HA and cholesterol in the form of instillations, both individually and in combination. However, we did not find any indications of the effectiveness of GC instillations in combination with oral administration of cholesterol.
In this regard, in this study we compared the effectiveness of GC instillations in patients with BPS/IC alone and in combination with long-term oral administration of cholesterol (poCS).
Materials and methods. The study included 59 women diagnosed with BPS/IC.
. The main inclusion criterion was the presence of pain in the patient, localized in the projection of the bladder and associated with the filling of the bladder.
All had at least one of the following symptoms: frequency of urination more than 8 times a day, urination 2 or more times at night, or persistent urgency for at least 12 weeks
.
In addition, inclusion criteria were age over 18 years
,
a negative pregnancy test
, and
negative urine culture results
.
Patients with current urinary tract infection, sexually transmitted diseases, chemical or radiation cystitis, urolithiasis, malignancy, urethral diverticulum, or breastfeeding women were not included in the study.
All patients underwent a comprehensive urodynamic study and cystoscopy to confirm the diagnosis of BPS/IC and exclude other bladder diseases. Standard hydrodistension was not performed.
All patients before the start of the study, as well as 1 week after completion of treatment, filled out a visual analogue scale (VAS), the O'Leary questionnaire and the Interstitial Cystitis Problem Index (IPPI) and a voiding diary for 3 days.
Patients were randomized into two groups: receiving only instillations of the HA drug in the form of a viscoelastic solution of sodium hyaluronate 50 ml ( Urolife®
, Riviera Biotech) once a week for 12 weeks (n=30) and received complex therapy in the form of the above instillations together with oral administration of cholesterol 0.39 g (
Urolife® capsules
, Riviera Biotech) 2 capsules 3 times a day for 12 weeks ( n=29).
Intravesical instillations were performed using a Nelaton 10 Ch catheter, and patients were instructed to try to abstain from going to the toilet for at least one and no more than two hours after drug administration.
Data were collected prospectively followed by retrospective analysis. Statistical analysis was carried out using the MS Excel program with the calculation of Student's t-test. A P level of <0.05 was accepted as a significant difference.
results
From July 2022 to September 2022
The study included
59 women, randomized into 2 groups
.
The average age of the 30 patients
included in the group who received only GC instillations was
57.1 years
;
in the second group (HA + cholesterol) the average age was 58.63 years
.
When performing cystoscopy in all patients, bladder stones, tumors and other conditions that were criteria for excluding the diagnosis of BPS/IC were excluded. Using a urodynamic study, the presence of neurogenic dysfunction of the lower urinary tract in patients was excluded.
Before treatment, the average VAS score was 7 in both groups.
The average ISIC was 17 in the GC group and 18 in the GC + cholesterol group (p>0.1)
.
The average PICI was the same in both groups and amounted to 15
.
The frequency of urination on average for the groups was 11.4 and 11.6 micturitions per day
in the GC and GC+poCS groups, respectively (p>0.1).
The average volume of urination before treatment was 138±24.6 ml and 131±18.6 ml by group
.
After 12 weeks
therapy in both groups there was a significant improvement in VAS, ICIC, ICIC and frequency and volume of urination. However, in the group of GC + cholesterol, the improvement in almost all studied parameters was more significant than in the group receiving only GC instillations. In particular, the VAS score was 4 versus 5 (p<0.05), ICPI – 9 versus 11 (p<0.01), PICI – 7 versus 8 (p<0.05), and urination frequency decreased to 6.9 versus 8.3 times a day (p<0.05) in the group of GC+poCS versus GC only, respectively (Fig. 1).
Rice. 1. The value of the studied indicators in both groups before and after treatment
The only exception was the volume of urination, which was 189±44.3 ml in the GC group and 213±29.4 ml in the GC+poCS group (Fig. 2). Despite a significant increase in capacity in both groups after therapy, the difference in the result between the groups themselves turned out to be statistically insignificant (p>0.05).
Rice. 2. Average volume of urination before and after treatment in both groups.
No significant adverse effects were observed in any of the patients in either group. In 8 patients
(3 in the GC group and 5 in the GC+poCS group) the appearance of minor pains was noted within 1-2 days after the instillations, however, we associate this side effect not with the effect of the administered drug, but with the catheterization itself.
Discussion
Treatment of BPS/IC is a known challenge for urologists due to unclear etiology and poor predictability of the effectiveness of therapy, including oral medications, intravesical instillations, or surgical manipulation.
. In this regard, researchers continue to search for the most optimal type of treatment or combination thereof.
The theory proposed by Hurst that defects in the GAG layer can lead to BPS/IC is now generally accepted. GC in the form of intravesical instillation was the first glycosaminoglycan proposed for the treatment of BPS/IC.
The first study on the effect of GCs on BPS/IC symptoms was published in 1996 by Morales et al.
, who found improvement in 71% of patients after 12 weeks of therapy.
Subsequently, a number of studies were carried out, showing the effectiveness of intravesical GC therapy from 30% to 80%
.
On the other hand, in two more studies from 2003 and 2004
There was no statistically significant difference in the effectiveness of GC compared to placebo in patients with BPS/IC. However, patient selection conditions and improvement parameters from these sources remain unclear.
At the same time, a number of studies show that cholesterol deficiency in the superficial layer of the lining of the bladder can play a significant role in the pathogenesis of BPS/IC. In this regard, it has been proposed to use intravesical administration of cholesterol for the treatment of patients with BPS/IC. Steimhoff et al assessed the effectiveness of cholesterol use for 12 months
, and the study showed improvement in symptoms in 67% of patients. However, there are other studies reporting low or even comparable to placebo effectiveness of intravesical administration of cholesterol for 12 weeks.
The good effectiveness of intravesical use of a combination of GC and cholesterol has also been shown in a number of studies. In particular, Porru et al reported significant improvements in VAS score, voiding volume and frequency, and ICIC with combination therapy in 20 patients with BPS/IC. Similar results were reported by Cervigni et al, with the authors also reporting improvements in symptoms and quality of life over a 3-year follow-up period.
Despite a considerable number of publications devoted to the intravesical use of GCs and cholesterol, there are very few studies on the effectiveness of oral use of GAGs in the available literature. Thus, Torella et al report the effectiveness of oral administration of GC, cholesterol, curcumin and quercetin in postmenopausal women with frequent relapses of chronic urinary tract infection.
Theocharides et al describe in their study a 48% improvement in BPS/IC symptoms after 12 months
therapy with an oral drug containing GC, cholesterol, glucosamine sulfate, quercetin and rutin. However, we did not find any published data on the effectiveness of the combined use of intravesical and oral GAG for BPS/IC.
Our work, taking into account the available literature, is the first study of its kind to compare the effectiveness of intravesical therapy alone in combination with oral administration of GAGs, in particular polycholesterol. In addition, we found statistically significant differences in treatment outcome between these two treatments.
We compared the effectiveness of intravesical administration of GC alone and its combination with oral administration of cholesterol.
, while significant differences were revealed with the advantage of combined therapy in VAS, ISIC, ICPI and urination frequency. In terms of urinary volume, the difference was not significant.
The normal GAG layer of MP consists of sulfated GAGs (such as CS and dermatan sulfate) and non-sulfated GAGs, such as HA. About 80-90% of the total GAG surface is associated with integral membrane proteins, in particular, 55% of proteins are associated with heparan sulfate, 26% with cholesterol, the remaining with unidentified GAGs or dermatan sulfate. Thus, the use of only non-sulfated GAG - HA - cannot ensure complete restoration of the GAG layer of the bladder mucosa, and therefore will not allow for maximum effectiveness in treating the symptoms of BPS/IC.
Despite the rather low bioavailability of oral administration of cholesterol, not exceeding 13%, the results of our study show the undoubted effectiveness of its use together with GC instillations. In addition, oral administration does not require the patient to visit a medical facility, which reduces the cost of treatment and makes it possible to replenish GAG deficiency continuously over a long period of time.
In this case, the drug we use is Urolife
is the most convenient product, as it is available both in the form of a viscoelastic solution for instillation, the main component of which is HA, and in the form of capsules containing cholesterol.
The disadvantage of our study is the lack of comparison of the effectiveness of the use of GC in the form of instillations and GC together with polycholesterol with placebo. However, from our point of view, it is unethical to use a obviously ineffective drug in patients with BPS/IC, most of whom suffer from fairly intense pain and are desperate to get relief from treatment.
The duration of observation and the number of patients included in our study are also relatively small, although sufficient for statistical evaluation and comparable to the group sizes in similar studies available in the literature.
Conclusion
Literature data on comparative studies of the treatment of patients with BPS/IC using various GAGs, as well as their combinations, are quite limited. In addition, we did not find data on the effectiveness of using a combination of intravesical agents and simultaneous oral administration of GAGs, in particular GC and poCS. In our study, intravesical administration of GC in combination with polycholesterol showed an advantage over the use of intravesical GC alone, both in terms of pain and urinary frequency.
In order to obtain more accurate data on the benefits of certain GAGs in the treatment of BPS/IC, it is necessary to conduct longer studies on large groups of patients, preferably multicenter, studying the effectiveness not only during and immediately after treatment, but also in the long-term period.
Diagnostics
The diagnosis is confirmed by bacteriological examination of urine and identification of pathogenic pathogens in the analysis.
Ultrasound and cystoscopy are not used to make a diagnosis because they have low diagnostic value. However, it is advisable to carry out these studies in case of atypical symptoms and manifestations of cystitis, the presence of repeated episodes of hematuria (blood in the urine) - in order to exclude other pathologies of the bladder, such as tumors and bladder stones.
Treatment of recurrent cystitis and preventive measures
Treatment and prevention of recurrent urinary system infections are based on the possible elimination of negative factors that cause recurrent diseases, and also include lifestyle changes, adequate antibacterial therapy and antibacterial prophylaxis.
The concept of “lifestyle change” includes:
- washing after defecation from front to back, avoiding wearing tight synthetic underwear, avoiding vaginal douching, forced urination immediately after sexual intercourse (in modern studies, the role of these measures in reducing the risk of relapse of the disease has not been convincingly proven, but it is believed that their use is possible);
- Drink plenty of fluids: 2 to 3 liters per day (in a recent randomized trial of 140 women with recurrent cystitis who were drinking little fluid initially, 1.5 liters of water was added to their diet, which resulted in a 50% reduction in the rate of recurrent cystitis).
In postmenopausal women, local estrogen replacement therapy is effective. The use of estrogen suppositories allows you to restore the number of lactobacilli in the vagina, which helps eliminate the growth of pathogens. Since a common cause of relapses in this category of women is the presence of genital prolapse (prolapse or prolapse of the pelvic organs through the vagina), correction of prolapse is necessary - conservative or surgical.
The effectiveness of prophylaxis with immunoactive drugs (Uro-Vaxom, StroVac) has been proven. Uro-Vaxom is a medicine registered in Russia. The active ingredient is a lyophilized lysate of Escherichia coli bacteria. The drug is used for recurrent cystitis, can be prescribed in conjunction with antibacterial drugs, and has a small number of side effects. Course admission - up to 3 months.
It is possible to use antibiotic prophylaxis, which differs in dosage regimens: continuous and postcoital. Both regimens have proven effective in the treatment of recurrent cystitis. Numerous studies have shown that continuous prophylaxis reduces relapses by up to 95% compared to placebo. Fosfomycin, Nitrofurantoin, Ciprofloxacin can be used as a prophylactic drug.
Postcoital prophylaxis may be the method of choice in patients with exacerbations clearly associated with sexual intercourse. This also applies to women who want to prevent episodes of cystitis during pregnancy. However, in this case, the choice of medications is limited; it is possible to take Nitrofurantoin and a cephalosporin antibiotic.
Recently, D-mannose, a natural type of sugar that is a compound that mimics the receptors in the bladder wall, has been gaining popularity. It can competitively bind to bacteria and reduce the number of bacteria adhering to the bladder lining. This reduces the likelihood of developing cystitis. However, existing data regarding the effectiveness of the drug are not yet convincing enough and are few in number. It is also not very clear exactly what doses of D-mannose are effective, how and in what quantities they should be used. A number of studies have shown that D-mannose at a daily dose of 2 g is superior to placebo and comparable in effect to 50 mg of Nitrofurantoin (Furamaga). Produced in the form of a dietary supplement, it is not officially produced in Russia. May serve as an alternative for patients with postcoital cystitis along with postcoital antibacterial prophylaxis.
If conservative treatment is ineffective and a clear connection between the symptoms of cystitis and sexual activity is identified, it is possible to perform surgical treatment - surgical correction of the anatomical location of the external urethral opening (transposition of the distal urethral opening). The essence of the operation is to isolate the final section of the urethra and move it above the entrance to the vagina.
Intravesical instillations of hyaluronic acid (Uro-hyal, Urolife) are used to restore the protective glycosaminoglycan layer and are effective in the treatment of interstitial, post-radiation cystitis, and can also be used for the treatment and prevention of recurrent cystitis. There are methods for submucosal administration of hyaluronic acid into the urethra and bladder, the effectiveness of which is still being studied.
How is recurrent cystitis treated at the Rassvet Clinic?
Treatment of recurrent cystitis in Rassvet is carried out in accordance with the recommendations of leading foreign urological associations and medical communities. To diagnose urological diseases, our specialists use the latest generation digital urography, computer uroflowmetry, and expert-level ultrasound. Urologists at Dawn adhere to the principles of evidence-based medicine, do not prescribe unnecessary examinations or ineffective medications, and conduct extensive consultations aimed at preventing diseases of the genitourinary system.
Author:
Loktev Artem Valerievich urologist
Chronic cystitis. Immunoprophylaxis of relapses. Gadzhieva Z.K.
Oksana Mikhailovna Drapkina , professor, doctor of medical sciences:
– We move on to the next message from Professor Gadzhieva Zaida Kamaludinovna “Chronic cystitis and immunoprevention of relapses.” Please.
Zaida Kamaludinovna Gadzhieva , professor, doctor of medical sciences:
– In fact, on the one hand, my task was made easier, since I knew that Grigory Georgievich would speak, so fully and comprehensively he would present the problem of both acute and recurrent cystitis, and on the other hand, let’s say, I need to present as thoroughly as possible that small part, that seemingly small part of prevention, and specifically the immunoprophylaxis of cystitis, which we will talk about today.
In my speech, perhaps I will allow myself to repeat some points, because this is very important, and we must emphasize this, and we must remember this, because without such basic things, unfortunately, cystitis was the most important thing and the first among urological diseases in women, so, unfortunately, it will probably remain so. This is a kind of scourge. There are many such sufferers. They were, are and will be. But, in fact, I love such patients, because it is interesting to invest your knowledge, your experience in them, when you really see the effect of your work, but, unfortunately, as Grigory Georgievich said, there are a lot of recurrent cystitis, and these women do not - no they return.
The slide, which probably should have been the first, was for me to emphasize how common cystitis is - it accounts for 30% of all urological diseases. If we are talking today about chronic recurrent cystitis, we mean, of course, two or more exacerbations in six months and three or more exacerbations in a year. And, as Grigory Georgievich already said, it is believed that on average 20-30% of women have a relapse attack within 3-4 months after the first exacerbation, and about 20% of women face chronic urinary tract infections in their lives.
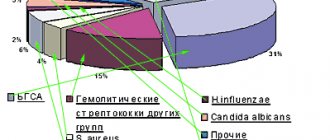
But I presented slightly earlier information than what Grigory Georgievich spoke about; he mentioned Aresk’s research. Here is a fairly large study that was carried out in Canada and several European countries. You see that almost 5,000 women took part in this study. And, despite the grandeur of this study, the result is, in principle, identical to what was presented by Professor Krivoborodov, that is, Escherichia coli as the main uropathogen accounts for the same 78-79%. A little less for other uropathogens. But we must pay attention to the fact that recently we are faced with the fact that the frequency of occurrence of the same Proteus, Klebsiella, Staphilococcus is growing. In recent years there have been more of them.
If we are talking about bacteriuria in general, then, of course, we must understand that the detection of the main uropathogens in the urine, just detection, does not give us the opportunity to make a final diagnosis. That is, in order for us to talk about true bacteriuria, we must prove that the number of these bacteria is really large. And according to all possible Guidelines, you see that clinically significant bacteriuria with a titer of monocultures of Escherichia coli and staphylococcus of 103 or more CFU/ml; monocultures of other bacteria are 104 CFU/ml and mixed cultures of two bacteria are 105 CFU/ml of urine.
A very important issue before the issue of prevention is the issue of urinary tract infections and bacteriuria in pregnant women. It is believed that about 6% of pregnant women have asymptomatic bacteriuria, despite the fact that it does not clinically cause any symptoms, which is why it is called asymptomatic bacteriuria, but what can it lead to? Look at the terrible complications: premature birth; to anemia of a pregnant woman; to preeclampsia; to malnutrition of the newborn; intrauterine fetal death. And it is believed that the risk of having children with low body weight in pregnant women who have asymptomatic bacteriuria and who have not received appropriate therapy is 1.5-2 times higher than in women without it.
As Grigory Georgievich said, what are the main goals we pursue when we talk about the treatment of uncomplicated urinary tract infection? This, of course, is the rapid elimination of clinical symptoms, eradication of the pathogen, and this is the very prevention of reinfections that we will talk about today.
Speaking about recurrent infection, as has already been emphasized, this is very important; it is a serious medical, socio-economic problem. There are different approaches to the problem of preventing this condition. Not all antibiotics are suitable for us to prevent infection. Moreover, if we are talking about antibiotics, then the questions regarding bacterial resistance, compliance, and adverse reactions are completely different. Therefore, we need to search and develop some other alternative approaches to this problem.
I found interesting data and I always try to show it, especially when I meet with other specialists, doctors of other specialties, because, fortunately or unfortunately, cystitis is, one might even say, in some way an interdisciplinary problem. Look what's happening? Who treats cystitis here? In first place, oddly enough, are not health workers at all (neighbors, friends). What was the advice? What dose was recommended? This is a big question. In second place, unfortunately, is self-medication. Patients do not reach specialists because even our elderly women have learned to use the Internet. What are they buying for themselves? This is also a big question. Today Grigory Georgievich spoke about the cost, it is desirable that the drug be of low cost. But in my practice there was a patient who found Ciprofloxacin for 28 rubles. What can you expect from this "Ciprofloxacin"? She really wanted to save money, apparently, but ended up saving on her treatment. In third place are our fellow gynecologists, because, as I already said, not at the dawn, but at the height of the 21st century, our women think that urologists are only male doctors, and do not reach a specialist in the appropriate field. Well, perhaps it is believed that it is easier for a woman to tell a gynecologist, combining all possible other problems. Well, in fourth place, finally, we are urologists, the matter has come to us. But then there are therapists, pharmacists, nephrologists - all those specialists who, willy-nilly, meet with these patients, so I believe that doctors of various specialties are probably obligated to know about what is happening in this section of medicine, because that they sometimes take the first blow. But at least you just need to send to a urologist, knowing, for example, what primary examination methods are needed to be carried out, so that the same urologist can quickly and easily make the correct diagnosis and prescribe the correct therapy.
I will periodically refer to the recommendations of the European Association of Urology, which we try to follow. There are some features that are presented in our Russian recommendations, which came out in 2012. But, for example, everything related to the prevention of recurrent urinary tract infections is here, both in our recommendations and in European ones, in principle, we follow the same rules.
As Grigory Georgievich said in his previous speech, in the first place is, of course, long-term prophylaxis using low doses of antibiotics. But, for example, if we are talking about women with postcoital cystitis, then we prescribe antibacterial drugs only when all possible behavioral methods of prevention have been exhausted. We always recommend that such women immediately after sexual intercourse urinate, after an hour it is possible to urinate again, be sure to wash themselves in order to wash away all those microorganisms that entered the external opening of the urethra during sexual intercourse with a current of urine, a stream of urine.
For women in menopause, since the main pathogenesis of the development of urinary tract infections in this category of patients is estrogen deficiency and urogenital atrophy, then the basis of pathogenetic therapy for such patients is hormone replacement therapy, be it systemic, but more often local; these are probiotics; this is nonspecific prevention in the form of acidifying urine with cranberry preparations or, as we have always used cranberry juice since ancient times, and immunoactive prevention, which we will talk about today.
But if you notice, on this slide, after each statement, let's say, after each recommendation, there is a level of recommendation. Everything that concerns antibacterial drugs, then the level of recommendation is A, and as for probiotics and nonspecific prophylaxis, then, accordingly, the level of recommendation is C, and if we are talking about immunoactive prophylaxis, then we mean the level of recommendation B. What is this?
When we mean level A recommendation, we have the right to use these recommendations based on the results obtained from all kinds of large clinical trials, at least one of which must be randomized. If we talk about level B recommendation, then, of course, we use the knowledge that has been obtained as a result of studies, well-designed clinical trials, not necessarily randomized. If we are talking about level C, then clinical studies of the required quality have not been conducted on these drugs or in this area.
As for immunoprophylaxis, from this slide I can clearly say that this is how the song says, if we say immunoprophylaxis, we mean “Uro-Vaxom”; if we say “Uro-Vaxom”, then we mean form of immunoprophylaxis. Because today this is the only drug that is recommended, accordingly, indicated in the recommendations of the European Association of Urology. And you see the translation, accordingly, from the Guidelines, from these recommendations: “...Immunoactive prophylaxis and the effectiveness of Uro-Vaxom compared to placebo have been proven even in several randomized studies. And it can be recommended for immunoprophylaxis in women with uncomplicated recurrent urinary tract infections.”
The same thing, I specifically gave a link to our Russian national Recommendations for antimicrobial therapy and prevention. Treatment of recurrent infections with low doses of antibiotics. If we are talking about alternative methods of treatment and recurrent infections, then the schemes, accordingly, include the same “Uro-Vaxom”.
What is Uro-Vaxom? What he really is? Today these are capsules that contain lyophilized strains of Escherichia Coli, 18 strains. More than 2000 patients have undergone various studies. More than 1 million, respectively, have been treated over the past 5 years.
How does Uro-Vaxom work? Its action literally begins from the gastrointestinal tract. Once in the gastrointestinal tract, the cells of the immune system are stimulated, namely Peyer's patches, which make up 25% of the surface of the entire gastrointestinal tract. Previously, it was believed that such drugs could not act in the human body; let’s say, they were not absorbed. But it was realized that the action occurs precisely through Peyer’s patches. Activation of T- and B-lymphocytes occurs, that is, our T-lymphocyte is responsible for cellular immunity, and our B-lymphocytes, respectively, are responsible for humoral immunity. Circulation of protective cells - their entry into the bloodstream and lymphatic channel, respectively, integration of T- and B-lymphocytes into the urinary tract. And already the production of protective and specific antibodies in the mucous membrane of the bladder itself. In principle, probably 20 years ago, it was believed that through the mucous membrane we could not achieve such an effect of these drugs until it was discovered that immunoglobulin A can be produced through Peyer's patches - the same immunoglobulin A that works well in the mucous membrane. For example, in other organs or in the circulatory system, immunoglobulin G mainly acts, which in the mucous membrane, accordingly, works worse than immunoglobulin A.
If we are talking about strengthening antimicrobial protection in the genitourinary tract under the influence of "Uro-Vaxom", then it goes in two directions - this is the implementation, respectively, of a specific immune response and an increase in nonspecific resistance, that is, through macrophages, NK-phagocytosis, synthesis immunoglobulins A, as I already said.
It is believed that the amount of immunoglobulins A and immunoglobulins G in those patients who take Uro-Vaxom is almost 2-2.5 times higher than in those patients who do not take this immunoactive drug, Uro-Vaxom.
Moreover, it was previously believed that if this drug contains only lyophilisates of Escherichia Coli, then it should act accordingly in patients whose urine cultures revealed Escherichia Coli. No, in fact, studies have been performed on the basis of which we can say that Uro-Vaxom provides protection against a wider range of pathogens that cause urinary tract infections, and not just against those used in its , let's say, composition.
How can we use Uro-Vaxom? Starting with treatment together with an antibiotic, for 10 days together with an antibiotic, 1 capsule per day, and then continue, respectively, one capsule per day for 3 months. That is, we use the drug, starting from the treatment stage, and then for 3 months in order to carry out, accordingly, immunoactive prophylaxis.
What do we expect from this immunoactive prophylaxis? Of course, a decrease in the level of bacteriuria. Of course, a decrease in symptoms. Reducing the need to use antibacterial drugs. And, of course, either an increase in the intervals between exacerbations, that is, an increase in the interval of relapse-free course, or a decrease, complete disappearance of relapses of the disease.
Look, if the drug is used together with an antibiotic, then after 3 months of treatment the level of bacteriuria is 3 times lower than, for example, among those patients who took only an antibiotic. Moreover, if we want and pursue the goal of reducing the need to use antibiotics, look, if we use Uro-Vaxom, that is, a drug for active immunotherapy, it reduces the duration of antibiotic use by 36%. In total, after 6 months of using it, the need to use antibiotics is reduced by even 67%. Moreover, the drug reduces the number of relapses by 36% in those patients in whom the level of bacteriuria was quite high and reached, respectively, 104 CFU/ml/
A very large number of patients get rid of urinary tract infections when using Uro-Vaxom. You see that 65% is quite high for such a disease. The difference in the number of patients with relapses was about 21% in favor of this drug. We have one for the use of active immunoprophylaxis. Therefore, in general, there is no advertising of the drug here. In this case, we are advertising the same immunoactive prophylaxis.
Moreover, since we are pursuing the most long-term need and the possibility of a long relapse-free period, then, you see, even after 12 months, that is, 1 year after stopping the drug, 55% of patients get rid of relapses of this disease.
A lot of research has been done on this matter. But Kurt Nabert, for urologists this is a fairly well-known name, in matters relating to urinary tract infections, he conducted a fairly large meta-analysis, collecting the results of many studies on this issue, and it was revealed that against the background of such active immunoprophylaxis, a decrease in the number recurrence of urinary tract infections is about 40%.
Moreover, using active immunoprophylaxis, we improve laboratory parameters. Leukocyturia decreases, as you can see, by almost 2 times, bacteriuria by 33%. The incidence of dysuria after 6 months decreases by more than 50%, that is, almost 2.5 times.
Moreover, the drug is quite well tolerated. So I collected data from various studies specifically. And you see that despite the fact that a lot is used there, all kinds of side effects are presented, the percentage of their occurrence is so low that, in general, we can safely recommend to patients, saying that this immunoprophylaxis is practically without side effects. In my practice, patients mostly complain about this feeling of nausea, some kind of slight nausea, and even then not always.
If we are talking, accordingly, about the clinical effectiveness of immunoactive prophylaxis using Uro-Vaxom, then, as a summary, the number of relapses is reduced; the frequency of bacteriuria, dysuria, leukocyturia decreases; and, accordingly, the need to use antibiotics is reduced; reliable protection from 3 to 12 months; and, as I already said, the drug is very well tolerated.
At the beginning of my speech, I said that asymptomatic bacteriuria occurs quite often in pregnant women. This is a very complex group of patients, to whom the approach can sometimes even be difficult, let’s say. We always consult with gynecologists on this issue. Despite the fact that the annotation for this drug, Uro-Vaxom, states that no clinical studies have been conducted on pregnant women, at the same time, animal studies have not revealed any negative effects during pregnancy, including including the development of the embryo, fetus, respectively, and postnatal development. If we talk about the lactation period, then such studies have not been conducted; accordingly, there is no data on this condition.
But we still have a question. Is it possible to use Uro-Vaxom in pregnant women? To date, several such studies have been carried out, and I will try to present the data. It is quite possible that, given such indicators, the annotation for this drug may someday include the possibility of using it in pregnant women.
Against the background of immunoactive prophylaxis, there is a significant decrease in urinary tract relapses, you see, a significant decrease in the frequency of dysuria - 87% at the starting point and 22.8%, which is almost 3.5 times. Moreover, there is a significant reduction in the need for antibiotic use. For pregnant women, this is a very important issue, because for a pregnant woman, antibiotics, even though some antibiotics can be used in certain trimesters of pregnancy, it is better to bypass them. And, naturally, the duration of the required course of antibiotic therapy is reduced by almost 40%.
Last slide. I always voice it and show it when I talk about lower urinary tract infections. Their treatment must be comprehensive. Today we spoke with Grigory Georgievich that no, no, these women are still coming back. Why? Because in addition to antibiotics, in addition to anti-inflammatory drugs, in my practice I always try to use drugs to improve the functions of the lower urinary tract. At one time, our clinic carried out work to study the functions of the lower urinary tract in patients suffering from chronic recurrent cystitis. Almost 50% of them have dysfunction of the urethra, the so-called instability of the urethra, causing this functional obstruction, which in itself is a provocateur of the development, casting, let’s say, of those bacteria that are located in the distal part of the urethra, maximum casting, which in should not be the norm. This is the same overactive bladder. We must identify and treat any dysfunctions using appropriate medications along with antibiotics and uroseptics. And, of course, the drug for systemic immunoprophylaxis, what we talked about today, the drug “Uro-Vakson”, is the only one we have today. Protection of the urothelium from recurrent infection. This may also be local therapy. Now there are drugs that improve the condition of the bladder mucosa. But perhaps this is the topic of some of our other meetings and speeches.
I thank you for your attention. And like Grigory Georgievich, I always try to tell you that in our clinic of the First Moscow Medical University. THEM. Sechenov, at the Research Institute of Uronephrology and Human Reproductive Health on Bolshaya Pirogovskaya we are always ready to meet you and help you. Welcome. Thank you.