The article was checked by rheumatologist Borodin O.O. , is for general informational purposes only and does not replace specialist advice. For recommendations on diagnosis and treatment, consultation with a doctor is necessary.
- At the Yauza Clinical Hospital, laboratory (coagulogram, increased levels of the enzyme antistreptolysin-O, IgA) and instrumental (biopsy) research methods are used to diagnose hemorrhagic vasculitis (Henoch-Schönlein disease, purpura).
- Based on the results of the examination, as well as taking into account the clinical picture of the disease, the rheumatologist will develop an individual treatment regimen for the patient, if necessary, using innovative methods of extracorporeal hemocorrection.
- 140 cases per 1 million population - incidence rate of hemorrhagic vasculitis
- More than 60% of cases of hepatitis in adults are accompanied by involvement of the joints, 50% of the kidneys, and 65% of the digestive tract.
- In 95% of cases, timely treatment of Henoch-Schenelein disease contributes to the patient’s complete recovery
sign up for a consultation
About the development of the disease
Hemorrhagic vasculitis or Schenelein-Henoch disease is a disease in which autoimmune damage to small arteries occurs - they become fragile, their permeability increases, which causes impaired microcirculation, microthrombosis, multiple small hemorrhages (hemorrhages) as in the skin (hemorrhagic rashes on the skin and mucous membranes) , and in internal organs (gastrointestinal tract, kidneys, joints).
Most often the disease develops in childhood (6-7 years), but can also affect adults. Boys get sick 1.5 times more often than girls.
Diagnostic methods
Since in children the disease manifests itself with bright, acute symptoms from the very beginning, there are, as a rule, no problems with making a diagnosis. Diagnosis of hemorrhagic vasculitis in adults is much more difficult, especially in the absence of a characteristic rash at the onset of the disease. As a rule, it is based on laboratory tests, which include:
- blood tests - general, biochemical, coagulogram;
- urine examination for hematuria, proteinuria, cylindruria, Nechiporenko and Zimnitsky tests, biochemical analysis;
- stool test for the presence of blood.
An important stage of diagnosis, which allows us to establish the degree of damage to internal organs, is instrumental studies - ultrasound of the abdominal cavity and kidneys, ultrasound of the renal vessels, gastroscopy. In severe cases of the disease, a biopsy of the skin and kidneys is prescribed to determine the size of immunoglobulin deposits and the permeability of the vascular wall.
Causes
The exact cause of hemorrhagic vasculitis (HV) has not yet been clarified, however, most scientists are inclined to the multi-etiological theory of the development of pathology. The leading factors provoking the development of the disease are:
- viral and bacterial infections,
- chronic infections,
- food or drug allergies,
- vaccines.
The mentioned reasons provoke a malfunction of the immune system, which begins to produce pathogenic immune complexes (IgA) that affect the inner lining of small vessels and contribute to the development of inflammation and microthrombosis.
List of sources
- Lyskina G. A. Systemic vasculitis. In the book: Pediatric rheumatology. Guide for doctors / Ed. A. A. Baranova, L. K. Bazhenova. M.: Medicine, 2002. pp. 221–270.
- Kulaga V.V., Romanenko I.M., Afonin S.L. Allergic diseases of the blood vessels of the skin. Lugansk: “Etalon-2”, 2006. 168 p.
- A practical guide to childhood diseases, edited by prof. Kokolina V.F. and prof. A.G. Rumyantsev, volume IV. Hematology/oncology of childhood (edited by Rumyantsev A.G. and E.V. Samochatova). Medical practice – M. Moscow 2004 Zinovieva G.A., Frolkova E.V. Hemorrhagic vasculitis. Clinic and treatment // ros. pediatrician, journal — 1998. -N12. P.24-26.
- Krivosheev O.G., Gulyaev CB, Semenovykh A.G. Modern principles of treatment of Henoch-Schönlein purpura // Doctor. 2007. No. 4. -P.54-55.
Symptoms of hemorrhagic vasculitis
There are several forms of hepatitis B:
- Skin or simple : characterized by the appearance of a specific itchy rash on the lower extremities and buttocks (small pinpoint hemorrhages that rise above the skin and do not disappear with pressure). Over time, the red rash darkens and disappears, leaving areas of increased pigmentation.
- Joint: patients complain of pain in the area of large joints (knees, elbows, hips), their swelling and dysfunction.
- Abdominal : nausea and vomiting, severe abdominal pain (often cramping), possible intestinal bleeding, development of intestinal gangrene (due to thrombosis).
- Renal : urine becomes pink or red due to the admixture of red blood cells, its quantity decreases, protein appears in tests, which are signs of the development of glomerulonephritis and the threat of developing chronic renal failure.
- Fulminant : characterized by the development of DIC syndrome and high blood loss.
Often the disease begins with an increase in body temperature to 38-390C, and patients also note general weakness and increased fatigue. Characteristic wave-like course of the disease.
Diet
Hypoallergenic diet
- Efficacy: therapeutic effect after 21-40 days
- Timing: constantly
- Cost of products: 1300-1400 rubles. in Week
Diet Table No. 1
- Efficacy: therapeutic effect after 3 weeks
- Terms: 2 months or more
- Cost of products: 1500 - 1600 rubles. in Week
Diet 7 table
- Efficacy: therapeutic effect after a week
- Terms: 1 month or more
- Cost of products: 1200-1300 rubles per week
A hypoallergenic diet is prescribed, which involves excluding obligate allergens from the diet: milk, fish, citrus fruits, chocolate, cocoa, orange and red vegetables/fruits, as well as extractive substances. For abdominal syndrome, a modified Table No. 1 according to Pevzner is indicated until it is completely relieved. For nephritis - dietary Table No. 7 with a gradual transition to a hypochloride diet.
Diagnosis of hemorrhagic vasculitis
At the Yauza Clinical Hospital, patients with suspected Henoch-Schönlein disease are prescribed the following set of examinations:
- general blood analysis;
- general urine analysis;
- coagulogram;
- determination of the level of antistreptolysin-O, IGA in peripheral blood;
- tissue biopsy of the affected organ or part of the body, followed by histological examination of the biopsy.
To make a diagnosis of hemorrhagic vasculitis, the patient must have two or more diagnostic criteria:
- specific rashes not associated with low platelet levels;
- manifestation of the disease before the age of 20 years;
- widespread abdominal pain that worsens after eating, intestinal bleeding;
- granulocytic infiltration of the walls of microvasculature vessels, which is confirmed histologically.
YOU can call us: 8 (8452) 98-84-68 and +7-967-500-8468 or
Hemorrhagic vasculitis (synonyms: Henoch-Schönlein purpura, Henoch-Schönlein disease, rheumatic purpura, allergic purpura) is the most common disease from the group of systemic vasculitis. It is based on aseptic inflammation of the walls of microvessels, multiple microthrombotic formation, affecting the vessels of the skin and internal organs (most often the kidneys and intestines).
The main reason that causes this disease is the circulation of immune complexes and activated components of the complement system in the blood. In a healthy body, immune complexes are removed from the body by special cells - cells of the phagocytic system. Excessive accumulation of circulating immune complexes under conditions of predominance of antigens or insufficient formation of antibodies leads to their deposition on the endothelium of the microvasculature with secondary activation of complement system proteins along the classical pathway and secondary changes in the vascular wall.
As a result, microthrombovasculitis develops and changes occur in the hemostatic system: activation of platelets, circulation of spontaneous aggregates in the blood, pronounced hypercoagulation, decrease in plasma antithrombin III, thrombopenia, increased level of von Willebrand factor, depression of fibrinolysis.
In 1837, the famous German physician JL Schönlein described “anaphylactic purpura.” In 1874 his compatriot E.N. Henoch published a valuable work on the same disease.
The name “ hemorrhagic vasculitis ,” used only in Russia, was introduced in 1959 by the outstanding rheumatologist V. A. Nasonova. Henoch-Schönlein purpura still prevails .
Etiology
In the majority of patients (66-80%), the development of the disease is preceded by an upper respiratory tract infection.
The manifestation of the disease after typhus, paratyphoid A and B, measles, and yellow fever is described.
Other potential triggers for the disease may include:
- medications (penicillin, ampicillin, erythromycin, quinidine, enalapril, lisinopril, chlorpromazine)
- food allergy
- insect bites
- hypothermia
Sometimes hemorrhagic vasculitis complicates the development of pregnancy, periodic illness, diabetic nephropathy, liver cirrhosis, and malignant neoplasms.
Classification
By form
- cutaneous and skin-articular:
- simple
- necrotic
- with cold urticaria and swelling
- abdominal and cutaneous-abdominal
- renal and cutaneous-renal
- mixed
With the flow
- fulminant course (often develops in children under 5 years of age)
- acute course (resolved within 1 month)
- subacute (allowed up to three months)
- prolonged (allowed up to six months)
- chronic.
By degree of activity
- I degree of activity - the condition is satisfactory, body temperature is normal or subfebrile, skin rashes are not abundant, all other manifestations are absent, ESR is increased to 20 millimeters per hour.
- II degree of activity - a state of moderate severity, severe skin syndrome, body temperature rises above 38 degrees (fever), severe intoxication syndrome (headache, weakness, myalgia), severe articular syndrome, moderate abdominal and urinary syndrome. In the blood, the number of leukocytes, neutrophils, eosinophils is increased, ESR will be increased to 20-40 millimeters per hour, albumin content decreases, dysproteinemia.
- III degree of activity - the condition will be severe, symptoms of intoxication are pronounced (high fever, headache, weakness, myalgia). Skin syndrome, articular, abdominal (paroxysmal abdominal pain, vomiting, mixed with blood), severe nephritic syndrome will be expressed, and there may be damage to the central nervous system and peripheral nervous system. In the blood there is a pronounced increase in leukocytes, an increase in neutrophils, an increase in ESR above 40 millimeters per hour, there may be anemia, a decrease in platelets.
Clinical picture As a rule, hemorrhagic vasculitis is benign. Usually the disease ends in spontaneous remission or complete recovery within 2-3 weeks from the moment the first skin rash appears. In some cases, the disease becomes relapsing. Severe complications due to damage to the kidneys or intestines are possible.
There are several clinical forms of hemorrhagic vasculitis:
Simple (cutaneous) form; Articular (rheumatoid) form; Abdominal form; Kidney form; Lightning form; Combined lesion (mixed form). Clinically, the disease manifests itself with one or more symptoms:
Skin lesions are the most common symptom[7] and are one of the diagnostic criteria for the disease. A characteristic hemorrhagic rash is observed - the so-called palpable purpura, the elements of which rise slightly above the surface of the skin, which is invisible to the eye, but is easily identified by touch. Often individual elements merge and can form continuous fields of significant area. Sometimes individual elements become necrotic. At the onset of the disease, the rash may be petechial in nature.
At the onset of the disease, the rashes are always localized in the distal parts of the lower extremities. Then they gradually spread to the thighs and buttocks. Very rarely the upper limbs, abdomen and back are involved in the process.
After a few days, the purpura in most cases fades, acquires a brown color due to pigmentation and then gradually disappears. With a recurrent course, areas of pigmentation may persist. There are never scars (with the exception of isolated cases with necrotization of elements and the addition of a secondary infection).
Joint syndrome - often occurs together with skin syndrome, occurs in 59-100% of cases[5]. Joint damage develops more often in adults than in children.
The favorite localization is the large joints of the lower extremities; the elbow and wrist joints are less often involved.
Characterized by migrating pain in the joints, occurring simultaneously with the appearance of skin rashes. In about a quarter of cases (especially in children), joint pain or arthritis precedes skin lesions.
A combination of articular syndrome with myalgia (muscle pain) and swelling of the lower extremities is possible.
The duration of articular syndrome rarely exceeds one week.
Abdominal syndrome, caused by damage to the gastrointestinal tract, occurs in approximately 2/3 of all patients. It manifests itself as spastic abdominal pain, nausea, vomiting, gastrointestinal bleeding (moderate, non-dangerous bleeding occurs frequently - up to 50% of cases; severe - less often, life-threatening - in no more than 5% of cases). Severe complications such as intussusception, perforation, and peritonitis are possible. An endoscopic examination reveals hemorrhagic or erosive duodenitis, less often erosion in the stomach or intestines (any localization is possible, including the rectum).
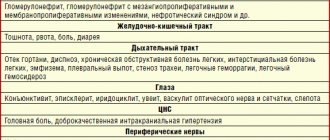
Renal syndrome: the prevalence has not been precisely established; there is a significant range of data in the literature (from 10 to 60%). More often it develops after the appearance of other signs of the disease, sometimes one to three weeks after the onset of the disease, but in isolated cases it may be its first manifestation. The severity of renal pathology, as a rule, does not correlate with the severity of other symptoms. Clinical manifestations of kidney damage are varied. Usually isolated micro- or macroglobulinuria is detected, sometimes combined with moderate proteinuria. In most cases, these changes pass without a trace, but some patients may develop glomerulonephritis[7]. Nephrotic syndrome may develop.
Morphological changes in the kidneys range from minimal to severe nephritis with crescents. Electron microscopy reveals immune deposits in the mesangium, subendothelium, subepithelium, and glomeruli of the kidneys. They include IgA, mainly the 1st and less often the 2nd subclass, IgG, IgM, C3 and fibrin.
Lung damage: occurs in isolated cases. Patients with pulmonary hemorrhage and pulmonary hemorrhages are described. Damage to the nervous system: occurs in isolated cases. Patients with the development of encephalopathy, with minor changes in mental status, are described; there may be severe headaches, seizures, cortical hemorrhages, subdural hematomas and even cerebral infarction. The development of polyneuropathy has been described. Damage to the scrotum: occurs in children, no more than 35%, and boils down to swelling of the scrotum (which is associated with hemorrhages in its vessels). Lightning form. It is based on a hyperergic reaction, the development of acute necrotizing thrombusculitis. The disease most often develops in the first or second year of life, 1-4 weeks after a childhood infection (chickenpox, rubella, scarlet fever, etc.). Characterized by symmetrical extensive hemorrhages, necrosis, and the appearance of cyanotic areas of the skin (hands, feet, buttocks, face), which are confluent in nature. In the future, gangrene of the hands and feet, coma, and shock may develop.
Features of hemorrhagic vasculitis in children:
The severity of the exudative component; Tendency to generalize; Limited angioedema; Development of abdominal syndrome; Acute onset and course of the disease; Tendency to relapsing course.
Laboratory signs Nonspecific. An important sign to suspect the disease is an increase in the concentration of IgA in the blood serum.
RF is detected in 30% - 40% of patients. In children, an increase in ASL-O titer is observed in 30% of cases. Increases in ESR and CRP correlate with the degree of vasculitis activity.
Diagnostic criteria[edit | edit wiki text] There are classification criteria for hemorrhagic vasculitis recognized by the international community of rheumatologists, which have been successfully used in diagnosis for many years (since 1990)[8].
There are four of them, each given a clear definition.
Palpable purpura. Slightly raised hemorrhagic skin changes not associated with thrombocytopenia. Age less than 20 years. The age of onset of the disease is less than 20 years. Stomach ache. Diffuse abdominal pain, worse after eating. or intestinal ischemia (there may be intestinal bleeding). Detection of granulocytes during biopsy. Histological changes revealing granulocytes in the wall of arterioles and venules. The presence of 2 or more of any criteria in a patient allows a diagnosis to be made with a sensitivity of 87.1% and a specificity of 87.7%.
Other systems of classification and differential diagnostic criteria have also been proposed [9] [10].
Treatment First, a diet is necessary (allergenic foods are excluded). Secondly, strict bed rest. Thirdly, drug therapy (antiplatelet agents, anticoagulants, corticosteroids, immunosuppressants - azathioprine, as well as antithrombotic therapy). The following drugs are used:
disaggregants - chimes 2-4 milligrams/kilogram per day, trental intravenous drip. heparin in a dosage of 200-700 units per kilogram of body weight per day subcutaneously or intravenously 4 times a day, gradually withdrawn with a decrease in the single dose. activators of fibrinolysis - nicotinic acid. In severe cases, plasmapheresis or glucocorticosteroid therapy is prescribed. In exceptional cases, cytostatics such as Azathioprine or Cyclophosphamide are used. In general, the course of the disease is favorable, and immunosuppressive or cytostatic therapy is rarely used (for example, in the development of autoimmune nephritis).
Children must be registered at a dispensary. Conducted over 2 years. For the first 6 months, the patient visits the doctor monthly, then once every 3 months, then once every 6 months. Prevention is carried out by sanitation of foci of chronic infection. Regularly examine stool for helminth eggs. Such children are contraindicated in sports, various physical procedures and exposure to the sun.
Therapeutic measures
At the Yauza Clinical Hospital, treatment of hemorrhagic vasculitis is aimed at achieving the following goals:
- elimination of clinical signs of pathology;
- reducing the risk of complications;
- preventing damage to vital organs;
- complete recovery of the patient or achievement of stable long-term remission.
To do this, our rheumatologist develops an individual treatment regimen for each patient, which includes:
- bed rest for at least 3 weeks;
- avoiding contact with allergens;
- diet therapy;
- prescribing enterosorbents, antihistamines, antispasmodics, hemostatic agents and antiplatelet agents;
- in some cases, the use of hormones and cytostatics is justified.
To reduce the destructive influence of circulating immune complexes and enhance the effectiveness of drug therapy, patients with hepatitis B undergo extracorporeal hemocorrection.
Forms, varieties, and symptoms
The symptoms of the disease depend on the form of vasculitis and the variety.
Early symptoms are similar to those of most infectious and inflammatory diseases: fever, weakness, headache, fatigue, muscle pain. As the process progresses, symptoms of the primary and secondary forms of the disease appear. The primary form is an independent disease, which consists of inflammation of a vessel of immune origin, autoimmune vasculitis. The secondary form is a consequence and symptom of a systemic disease, as well as a consequence of infections, helminth infections, exposure to toxins, chemicals, and radiation. Among the systemic diseases, the symptoms of which can be vasculitis, are diabetes mellitus, lupus erythematosus, and sarcoidosis.
Cutaneous
Cutaneous vasculitis affects the vessels of the dermis of small or medium diameter, but does not affect the vessels of the internal organs. It is diagnosed by biopsy, since skin vasculitis is similar in external symptoms to some diseases:
- capillary effusions of the skin - purpura;
- damage to skin capillaries - petechiae;
- urticaria, nodules;
- reticular levedo due to stagnation of blood in the capillaries.
Skin vasculitis can develop against the background of systemic diseases, and then the symptoms are supplemented by fever and joint pain.
Allergic
Manifested by the following symptoms:
- nodules, hemorrhagic, erythematous spots and rashes;
- skin infarction - formation of a black crust in the area of the rash;
- hemorrhages under the toenails;
- pain in joints and muscles;
- burning, squeezing pain or itching in areas of rash;
Allergic vasculitis most often manifests itself as a rash on the thighs, legs, feet, and in the generalized form, rashes are added on the forearms and torso.
The group of allergic vasculitis includes erythema induratum of Bazin, acute and chronic erythema nodosum, Behcet's disease, temporal angiitis, which have specific symptoms.
Acute erythema nodosum is characterized by large size nodes and a change in the color of the skin underneath them from red to greenish.
Behcet's disease mainly affects the mucous membranes of the eyes, mouth and skin with the formation of erosions and ulcers.
With temporal or senile angitis, older women suffer from severe and prolonged pain in the temple area.
System
Occurs when immune mechanisms are disrupted in various systemic diseases, which are characterized by damage to connective tissue (rheumatism, granulomatosis, lupus erythematosus, etc.)
With Wegener's granulomatosis, the disease manifests itself with the following symptoms:
- destructive changes in the walls of blood vessels in the respiratory tract and kidneys;
- ulcerated granulomas on the mucous membrane of the nose, mouth, bronchi;
- glomerulonephritis;
- severe complications on internal organs, skin, nervous system, and organs of vision.
With rheumatism, it spreads to the entire body and manifests itself depending on the stage of development of the disease. In addition to the skin, the vessels of internal organs and the brain are affected, with the risk of internal bleeding.
Cryoglobulinemic
One of the varieties of the systemic variety of the disease is cryoglobulinemic vasculitis, in which cryoglobulin proteins appear in blood cells, depositing on the walls of blood vessels and destroying them.
The disease has a progressive form, and its characteristic symptom (except for those common to all types of the disease) is damage to peripheral nerves and impaired sensitivity. If not adequately treated, cryoglobulinemic vasculitis can cause speech loss and motor paralysis.
Urticarial vasculitis
Urticarial vasculitis, or angiitis, is one of the types of allergic forms of the disease, which is characterized by chronic inflammation of the superficial vessels of the skin.
At the initial stage of development, it is often diagnosed as chronic urticaria. The disease is characterized by the following symptoms:
- wave-like current;
- the appearance of hemorrhagic spots, nodules, blisters on the skin;
- burning sensation in the affected areas;
- headache, in joints, lower back, muscles, stomach;
- elevated temperature;
- glomerulonephritis.
Diagnosed by immunofluorescence and histological examination of the affected areas of the dermis.
Mechanism of vascular damage
The main factor of damage in hemorrhagic vasculitis is special complexes formed from immune cells. They are called anaphylotoxins for their destructive properties. Under normal conditions they disintegrate. In a sick person, complexes accumulate and become antigens.
Deposition on the inner wall of blood vessels with a change in permeability causes blood circulation problems:
- platelets are activated;
- the plasma content of specific antithrombin decreases;
- the process of fibrinolysis is blocked.
As a result, a mass of microthrombi is formed in small vessels against the background of allergic inflammation and reduced blood clotting.
Clinical classification
Clinicians distinguish the following forms of the disease:
- simple or cutaneous - the whole process is limited to skin manifestations;
- skin-articular - in addition to the characteristic skin rashes, there are signs of inflammation of the joints;
- skin-abdominal - against the background of skin changes, symptoms of dysfunction of the stomach and intestines appear;
- renal - rare, accompanied by damage to the renal vessels with impaired filtration and urine excretion;
- mixed (combined) - there are changing symptoms of different forms.
Based on the type of disease, the following are distinguished:
- fulminant form - characterized by a rapid course, lasts several days, occurs in children under 5 years of age;
- acute - the disease has a sudden onset and lasts up to 30 days;
- subacute - lasts up to three months;
- protracted - clinical manifestations last for six months;
- recurrent - characterized by the repetition of symptoms at least four times in the next few years;
- chronic - the clinical picture of the disease lasts several years with periodic exacerbations.
How does the disease progress depending on the degree of activity?
To choose the correct therapy for hemorrhagic vasculitis, the doctor needs to know the degree of activity of inflammatory phenomena in the blood vessels. According to the clinic and the simplest laboratory tests, it is customary to distinguish 3 degrees:
- Grade I - the patient’s condition is satisfactory, the temperature is not elevated or slightly above 37, there are moderate non-widespread skin rashes, the ESR in the blood is not higher than 20 mm/hour, there are no other manifestations.
- Stage II - the patient’s condition is moderate, skin manifestations are intense, body temperature is over 38 degrees, there are signs of intoxication (muscle and headaches, weakness), there are clear signs of articular syndrome, abdominal and kidney symptoms are moderate. In the blood test: leukocytosis with eosinophilia and neutrophilia, ESR increases to 40 mm/hour, the ratio of protein fractions is disturbed towards a decrease in albumin.
- Degree III - the patient’s condition is objectively assessed as severe, there is a constant high temperature, intense symptoms of intoxication. The patient suffers from the simultaneous manifestation of skin, articular, renal and abdominal syndromes. Possible brain damage. Blood test: high leukocytosis due to neutrophils, ESR exceeds 40 mm/hour, possible decrease in red blood cells, hemoglobin and platelets (anemic syndrome).
The ankle and knee joints are most often affected, rarely the elbows and wrists.