IV GENERATION CEPHALOSPORINS
MODERN ANTIMICROBIAL CHEMOTHERAPY
MODERN ANTIMICROBIAL CHEMOTHERAPY
L.S. Strachunsky, S.N. Kozlov. Guide for doctors
| Content | ANTIBIOTIC.ru |
Antibacterial drugs / Beta-lactam antibiotics / Cephalosporins
IV generation cephalosporins include cefepime and cefpirome, which are similar in many properties. IV generation cephalosporins are characterized by greater resistance than all other cephalosporins to the action of chromosomal and plasmid β-lactamases of the AmpC class, which are common in nosocomial strains of Enterobacter and Citrobacter.
Compared to third-generation cephalosporins, they are more active against gram-positive cocci (but do not act on MRSA and enterococci), gram-negative bacteria of the Enterobacteriaceae
and against
P. aeruginosa
(including some strains resistant to ceftazidime).
CEFEPIM
Maxipim
Activity spectrum
| Gram(+) cocci: | streptococci (including penicillin-resistant pneumococci); staphylococci (except MRSA). Enterococci are resistant. |
| Gram(-) cocci: | N.gonorrhoeae, N.meningitidis, M.catarrhalis , including β-lactamase-forming strains. |
| Gram(-) sticks: | family Enterobacteriaceae ( E.coli, Proteus spp., Klebsiella spp., Enterobacter spp., Serratia spp., etc.), including a number of strains resistant to third-generation cephalosporins; H. influenzae ; P. aeruginosa (including some strains resistant to ceftazidime). |
| Anaerobes: | predominantly anaerobic cocci (peptostreptococci, etc.); no effect on B.fragilis . |
Pharmacokinetics
When administered intravenously, it is well distributed in the body and penetrates the BBB. It is excreted mainly unchanged by the kidneys. T1/2 is about 2 hours.
Indications
- Severe, mainly nosocomial, infections caused by multidrug-resistant microflora:
- nosocomial pneumonia;
- complicated urinary tract infections;
- intra-abdominal and pelvic infections (in combination with metronidazole);
- infections of the skin, soft tissues, bones, joints;
- sepsis.
Dosage
Adults
Parenteral 1-2 g every 12 hours; for life-threatening infections, 2 g every 8 hours.
Children over 2 months
Parenteral - 100 mg/kg/day in 2 administrations; for cystic fibrosis, neutropenic fever - 150 mg/kg/day in 3 doses.
Release forms
Bottles of 0.5 g, 1.0 g and 2.0 g of powder for the preparation of solution for injection.
Carbapenems are structurally similar to other β-lactam antibiotics, but unlike them, they are characterized by high resistance to ESBLs and a wider spectrum of activity, including P. aeruginosa
and non-spore-forming anaerobes.
The group of carbapenems includes imipenem and meropenem, which act on many strains of gram-negative bacteria resistant to cephalosporins of the III-IV generations.
Carbapenems are not active against MRSA and gram-negative bacteria such as B.cepacia
and
S. maltophilia
.
IMIPENEM/CILASTATIN
Tienam
It is a combination of imipenem with cilastatin in a 1:1 ratio. Cilastatin is an inhibitor of dehydropeptidase I, which is produced in the kidneys. When used without cilastatin, imipenem is destroyed by this enzyme, so therapeutic concentrations of the drug in the urine are not created.
Activity spectrum
| Gram(+) cocci: | streptococci, including most penicillin-resistant pneumococci; E.faecalis (but has no effect on S.faecium ); staphylococci (except MRSA). |
| Gram(-) cocci: | meningococci, gonococci, M.catarrhalis . |
| Gram(-) sticks: | E.coli , Salmonella, Shigella, Klebsiella, Enterobacter, Serration, Providence, Proteus, Citrobacter, Acinetobacter, P. aeruginosa . |
| Anaerobes: | spore-forming (clostridia, except C.difficile ) and non-spore-forming, including B.fragilis . |
Pharmacokinetics
When administered parenterally, it is well distributed in the body and passes through the BBB during inflammation of the meninges. Not metabolized in the liver. Excreted through the kidneys. T1/2 - 1 hour.
Adverse reactions
- Allergic reactions (in rare cases, cross-allergy with penicillins is possible).
- Gastrointestinal tract: nausea, vomiting (more often with rapid intravenous administration), in rare cases, diarrhea.
- Neurotoxicity: seizures (with rapid intravenous administration in patients with severe central nervous system diseases, renal failure).
Indications
- Severe infections, including nosocomial ones, caused by multidrug-resistant microorganisms, as well as mixed microflora:
- NDP (nosocomial pneumonia, lung abscess);
- profit center;
- intra-abdominal and pelvic infections;
- skin, soft tissues, bones and joints;
- sepsis;
Warning
Pseudomonas aeruginosa can quickly develop resistance to imipenem, therefore, when using it, it is necessary to repeatedly determine the sensitivity of P.aeruginosa
.
Dosage
Adults
Intravenous drip (over 30 minutes) - 0.5 g every 6 hours or 1.0 g every 8 hours per 100 ml of 5% glucose or saline sodium chloride solution. Intramuscularly - 0.5-0.75 g every 12 hours.
Children
Newborns - see Appendix I.
Children over 1 month - 15-25 mg/kg/day every 6 hours, intravenously.
The maximum daily dose is 2.0 g.
Release forms
Bottles of 0.5 g of powder for the preparation of solution for injection. Vials for intravenous and intramuscular administration are produced separately.
MEROPENEM
Meronem
In many characteristics it is close to imipenem, including T1/2 (1 hour).
Differences from imipenem:
- more active against gram-negative flora ( H.influenzae, P.aeruginosa, Klebsiella
spp.,
Enterobacter
spp., etc.); - less active against staphylococci and streptococci, has no effect on E.faecalis
; - is not destroyed by renal dehydropeptidase I, therefore it is used without its inhibitor (cilastatin);
- does not have convulsive activity, which is why it is used for meningitis;
- can be administered either intravenously by drip or by stream, but is not administered intramuscularly.
Indications
- Severe infections, including nosocomial ones, caused by multidrug-resistant microorganisms, as well as mixed microflora:
- NDP (nosocomial pneumonia, lung abscess);
- MVP (acute pyelonephritis);
- intra-abdominal and pelvic infections;
- skin, soft tissues, bones and joints;
- bacterial meningitis.
- sepsis.
Dosage
Adults
Intravenously (stream over at least 5 minutes or drip over 15-30 minutes) - 0.5 g every 6 hours or 1.0 g every 8 hours; for meningitis - 2.0 g every 8 hours.
Children over 3 months
Intravenously - 10-12 mg/kg every 8 hours; for meningitis - 40 mg/kg every 8 hours (no more than 6 g/day).
Release forms
Bottles of 0.5 g and 1.0 g of powder for preparing a solution for injection.
They are represented by one drug - aztreonam.
AZTREONAM
Azaktam
Has a narrow spectrum of activity, has a bactericidal effect on gram-negative flora, including P.aeruginosa
, however, similarly to penicillins and cephalosporins, ESBLs are destroyed. In addition, it is inactivated by β-lactamases, which are produced by staphylococci and bacteroides.
Despite the structural similarity of monobactams to penicillins and cephalosporins, cross-allergy with these groups of antibiotics is not observed.
Activity spectrum
| Gram(-) sticks: | E.coli , Salmonella, Shigella, Enterobacter, Klebsiella, Proteus, Serration, Citrobacter, Providence P.aeruginosa, H.influenzae , etc. Acinetobacter - resistant. |
| Gram(-) cocci: | gonococcus, meningococcus. |
Does not affect gram-positive flora (staphylococci, pneumococci) and anaerobes.
Pharmacokinetics
It is well distributed in the body, penetrating into many organs, tissues and environments. It penetrates through the BBB during inflammation of the meninges. Excreted by the kidneys. T1/2 is 1.5-2 hours.
Adverse reactions
- Local: phlebitis and thrombophlebitis - with intravenous administration, pain and swelling - with intramuscular administration.
- Dyspeptic and dyspeptic disorders.
- Hepatotoxicity (jaundice, hepatitis).
- Neurotoxicity.
Indications
The main clinical significance of aztreonam is its effect on aerobic gram-negative bacteria, including P. aeruginosa
; in some cases it acts as an alternative to aminoglycosides.
- NPD infections (nosocomial pneumonia), including cystic fibrosis.
- UTI infections.
- Intra-abdominal and pelvic infections (in combination with antianaerobic drugs).
- Infections of the skin, soft tissues, bones and joints.
- Sepsis.
Dosage
Adults
Parenteral - 1.0-2.0 g every 6-8 hours; for pseudomonas infection - up to 12 g/day; for UTI infections - 1.0 g every 8-12 hours.
Children
Parenteral - 30 mg/kg every 6-8 hours; for cystic fibrosis - 50 mg/kg every 6 hours (no more than 8 g/day).
Release forms
Bottles of 0.5 g and 1.0 g of powder for the preparation of solution for injection.
| Copyright © 2000-2007 ANTIBIOTIC.ru Posted: 05/15/2004 |
The address of this page: https://www.antibiotic.ru/books/mach/mac0107.shtml
Last modified date: 05/24/2004 18:56
Newspaper "News of Medicine and Pharmacy" Antimicrobial therapy (343) 2010 (thematic issue)
The history of the creation of antibacterial drugs was directly related to the solution of certain clinical problems: the search for drugs with high natural activity to suppress streptococci (penicillin, ampicillin), staphylococci (oxacillin), gram-negative flora (aminoglycosides); overcoming side effects (allergy to natural penicillins); increased penetration of antibiotics into tissues and cells (macrolides, fluoroquinolones). However, the use of antibiotics has led to the activation of microflora protection processes against them. Therefore, when developing drugs that are currently widely used in the clinic, the task of overcoming the natural and acquired resistance of nosocomial flora has become urgent. The most prominent representatives of this relatively new generation of drugs are carbapenems.
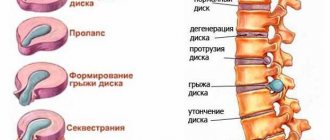
Development of carbapenems and their structural and functional features
Like penicillins and cephalosporins, carbapenems are naturally occurring. The first carbapenem, thienamycin, is a product of Streptomyces cattleya. The basic structure of thienamycin and subsequent carbapenems, like penicillins, is a five-membered β-lactam ring. The chemical feature of carbapenems that distinguishes them from penicillins is the replacement of carbon with nitrogen in the 1st position and the presence of double bonds between 2 and 3 carbon atoms, high resistance to hydrolysis of the β-lactam ring in the 6th position and the presence of a thio group in the 2nd position five-membered ring. It is believed that the last of these differences is associated with the increased antipseudomonal activity of carbapenems.
The first of the carbapenems, imipenem, appeared in clinical practice in 1986. To increase the stability of this drug against renal dihydropeptidase-1, imipenem was combined with an inhibitor of this enzyme, cilastatin, which significantly improved its pharmacokinetics in the kidneys.
Meropenem appeared in clinical practice in 1996. The main chemical difference from imipenem was the presence of a transhydroxyethyl group in the 6th position, which determined the stability of the drug to the action of various β-lactamases and the unique microbiological and pharmacological characteristics. The appearance of a side dimethylcarbamylpyrrolidinethio group in the 2nd position of the five-membered ring sharply increased the activity of the drug against Pseudomonas aeruginosa and other important gram-negative bacteria. The methyl group in the 1st position created stability of the drug against the action of renal dihydropeptidase-1, which made it possible to use the drug without cilastatin.
Ertapenem became the third drug in the carbapenem family in 2001. Like meropenem, it is stable to renal dihydropeptidase-1 and various β-lactamases. The chemical difference of this drug was the replacement of the methyl group with a benzoic acid residue in the 2nd position of the five-membered ring, which sharply increased its binding to plasma proteins. This figure reaches 95%, for imipenem - 20% and 2% for meropenem. As a result, the half-life of the drug from plasma increased, and it became possible to administer it once a day. Modification of the chemical structure had a negative impact on its activity against non-fermentative Gram-negative bacteria such as Pseudomonas aeruginosa and Acinetobacter baumannii [4–6]. In Psedomonas aeruginosa, it is suggested that a significant change in charge, increase in molecular weight and lipophilicity impaired the penetration of ertapenem through the membrane porin channel (OprD), which is a critical portal for the penetration of carbapenems [7, 8].
In 2010, a new carbapenem appeared - doripenem. Its chemical structure resembles meropenem and ertapenem, differing in the presence of a sulfammonylaminomethylpyrrolidinethio group in the 2nd position of the five-membered ring. This change led to increased activity against Staphylococcus aureus, while activity against gram-positive flora did not change significantly compared to meropenem [4–6, 9].
Mechanism of action and significance of penicillin-binding proteins
Carbapenems, like other β-lactam antibiotics, are bactericidal inhibitors of cell wall synthesis due to their binding to penicillin binding proteins (PBPs). PBPs are cytoplasmic cell wall proteins that complete the synthesis of peptidoglycan, the skeleton of the cell wall. Carbapenems bind to all major PBPs of Gram-negative bacteria. The main difference between the binding of carbapenems and other β-lactams to PBP is the high affinity for PBP-1a and -1b of Pseudomonas aeruginosa and E. coli, which leads to rapid killing of bacteria and increases the number of dead bacteria. Among carbapenems, in turn, there are differences in affinity for PSB-2 and -3 gram-negative bacteria. Imipenem has a greater affinity for PSB-2 compared to PSB-3. This causes the bacteria to acquire a spherical or ellipsoidal shape before lysis occurs. However, the affinity for Pseudomonas aeruginosa PSB-2 and -3 is the same. The affinity of meropenem and ertapenem for PSB-2 and -3 E. coli is significantly higher than that of imipenem. Similarly, the affinity for Pseudomonas aeruginosa PBP-2 is higher for meropenem than for imipenem, but for Pseudomonas aeruginosa PBP-3 it is 3- to 10-fold higher. Meropenem and doripenem have the same affinity for PSB-2, -3 [10, 11]. At the same time, there are individual differences between microbial strains in the affinity of PBP to various carbapenems.
Pharmacodynamic features of carbapenems
They depend more on the frequency of drug administration than on the concentration in the blood, which distinguishes them from aminoglycosides and fluoroquinolones, the effectiveness of which is directly related to the concentration of the drug in plasma. The maximum bactericidal effect of carbapenems is observed when plasma concentrations exceed the minimum inhibitory concentration (MIC) by 4 times [12]. Unlike carbapenems, the effectiveness of aminoglycosides and fluoroquinolones increases in proportion to their plasma concentration and can be limited only by the maximum permitted single dose of the drug [13].
The most important pharmacodynamic indicator of carbapenems is the ratio of the time when the drug concentration exceeds the MIC to the time between drug administrations. This indicator is expressed as a percentage (T > MIC%). Theoretically, it would be ideal to maintain carbapenem concentrations throughout 100% of the dosing interval. However, this is not necessary to achieve optimal clinical outcome [14–16]. Moreover, this interval varies among different β-lactam antibiotics. To achieve the bacteriostatic effect of an antibiotic, a figure of 30–40% is required for penicillins and cephalosporins and 20% for carbapenems. To achieve the maximum bactericidal effect, it is necessary to achieve 60–70% for cephalosporins, 50% for penicillins and 40% for carbapenems [13, 17]. Although penicillins, cephalosporins, and carbapenems kill bacteria by the same mechanism, differences in T > MIC reflect differences in the rate of killing, which is slowest for cephalosporins and fastest for carbapenems [13]. The molecular reasons for the difference in this process between cephalosporins and carbapenems may be the different affinities of these drugs for PBP-1a and -1b.
Another important characteristic of these drugs is the duration of the postantibiotic effect (PAE). PAE is the effect of a drug that continues after it is removed from the system. Among β-lactams, PAE is most often observed in carbapenems. PAE of imipenem against some microbes, including P. aeruginosa, lasts 1–4.6 hours [18–21]. It should be noted that this indicator can vary significantly among strains belonging to the same genus. Meropenem has a PAE similar to imipenem [22]. The duration of PAE of ertapenem against gram-positive bacteria is 1.4–2.6 hours. In doripenem, PAE against S.aureus, K.pneumoniae, E.coli and P.aeruginosa was observed for about 2 hours, and only against strains of S.aureus and P.aeruginosa [23].
Spectrum of activity and clinical efficacy
Carbapenems have the widest spectrum of activity among all antibacterial drugs. They are active against gram-positive and gram-negative microbes, including aerobes and anaerobes. The MIC50 indicator allows one to evaluate their natural activity and resistance; in this indicator they are similar to fluoroquinolones and aminoglycosides. Some bacteria lack natural sensitivity to carbapenems, such as S. maltophila, B. cepacia, E. faecium and methicillin-resistant staphylococci [4, 5, 9, 24–26]. There are certain differences between carbapenems in natural activity, which may be due to impaired penetration of drugs through the cell membrane and the activity of efflux pumps. Data on the comparative activity of all 4 drugs against the same clinical strains of microbes are very limited. However, there are experimental data from global comparative studies of the activity of these drugs, which are also not exhaustive [4, 6]. For example, in one of them there is no comparative assessment of certain MIC values: the minimum concentration for doripenem and meropenem was 0.008 μg/ml, for ertapenem - 0.06 μg/ml, and for imipenem - 0.5 μg/ml, so 3023 strains E. coli comparison of MIC90 was possible only with the above indicators. However, there are data from direct comparisons of the MICs of doripenem, meropenem and imipenem against enterobacteria, P. aeruginosa, Haemophylus influenza and Bordetella pertussis, which indicate their similar natural activity in terms of MIC50, which was similar or differed by one to twofold dilution [27 , 28]. Only against Proteus mirabilis, the activity of meropenem was 4 times higher than the activity of doripenem, and both drugs turned out to be significantly more active than imipenem; the same trends persisted with respect to MIC90. All three drugs were equally active against penicillin-sensitive and penicillin-resistant S. pneumoniae. Resistance associated with modification of penicillin-binding proteins had a significant effect on the activity of carbapenems: MIC50 and MIC90 of penicillin-resistant strains were 32–64 times higher than those of sensitive strains, while MIC90 remained below 1 μg/ml. Doripenem had similar activity to imipenem against S. aureus and E. faecalis. Against ceftazidime-sensitive Enterobacteriaceae that do not produce extended-spectrum β-lactamases (ESBLs), the activity of ertapenem, meropenem and doripenem was equal to or superior to that of imipenem. However, the activity of ertapenem was significantly lower against non-fermenting gram-negative flora (P. aeruginosa, A. baumannii) [4–6]. Against S. pneumoniae, S. aureus, S. epidermidis and E. faecalis, the activity of carbapenems was approximately the same, including ertapenem. Against gram-positive and gram-negative anaerobes, the activity of carbapenems was also the same with an MIC50 of 1 μg/ml and lower.
Carbapenems and resistance mechanisms
Resistance to β-lactams is present in gram-negative and gram-positive microorganisms. Gram-positive bacteria do not have resistance mechanisms associated with changes in the properties of the outer membrane, or enzymes capable of destroying carbapenems. The emergence of resistance in Gram-positive bacteria is associated with changes in penicillin-binding proteins (PBPs), such as the emergence of PBP-2a with low affinity for all β-lactams in methicillin-resistant S. aureus (MRSA). In gram-negative bacteria, the presence of an outer membrane and various β-lactamases led to the emergence of resistance associated with the production of inactivating enzymes (β-lactamases), disruption of the PBP structure, and decreased accumulation of the drug in the periplastic space due to a decrease in the permeability of outer membrane porin proteins or efflux pumps , removing various antibiotics from microbial cells. Of these, the production of β-lactamases and a decrease in cellular permeability are of greatest importance.
Extended spectrum and AmpC class beta-lactamases
The production of β-lactamases is the most common mechanism of resistance in Gram-negative bacteria. The location of the hydroethyl group at position 6 determines the high stability of carbapenems compared to cephalosporins and penicillins to hydrolysis by β-lactamases [29, 30], especially cephalosporinases (ESBLs and AmpC). Therefore, the real difference between carbapenems and other β-lactam antibiotics is their stability to the action of ESBLs and AmpC.
AmpC is a cephalosporinase with a broad spectrum of activity that destroys penicillins (including protected ones) and most cephalosporins. A necessary condition for the destruction of antibiotics is a high level of production of this enzyme by the microbe. In P.aeruginosa and many enterobacteria (E.coli, K.pneumoniae), the chromosomes contain information about the synthesis of AmpC, but synthesis begins under certain conditions - upon contact with an antibiotic. This nature of the formation and release of the enzyme is called inducible. However, if there is a congenital predisposition to hyperproduction of the enzyme, its depression may occur as a result of mutation [31]. Cephalosporinases AmpC are present on plasmids of some enterobacteriaceae; they are most often found in K. pneumoniae and E. coli [32–34]. Some plasmid-borne AmpC may have an inducible phenotype. Regardless of whether AmpC is chromosomal or plasmid, its overproduction in Enterobacteriaceae and P. aeruginosa leads to resistance to almost all β-lactams. However, many Enterobacteriaceae - hyperproducers of AmpC remain sensitive to cefepime and carbapenems, and most P.aeruginosa - hyperproducers of AmpC are sensitive to imipenem, meropenem and doripenem.
ESBL production is a second mechanism of β-lactam resistance. The production of these enzymes leads to resistance to penicillins and cephalosporins [25, 36]. The source of these enzymes for enterobacteria turned out to be Kluyvera spp. [37]. It should be noted that this type of β-lactamases can be suppressed by β-lactamase inhibitors (sulbactam, tazobactam, clavulanic acid), so protected penicillins and cephalosporins can retain their activity against ESBL producers. However, carbapenems are considered the drugs of choice for the treatment of infections caused by ESBL-producing Enterobacteriaceae [38]. It was shown that E. coli and K. pneumoniae remain sensitive to all carbapenems, with the exception of ertapenem, and MIC90 does not change significantly. The MIC90 of ertapenem in ESBL producers is approximately 4 times higher than in “wild” strains [39].
Carbapenemases
In addition to ESBLs and AmpC, some bacteria have enzymes (carbapenemases), information about which is encoded on the chromosome or plasmids [40]. Such enzymes can be produced by some enterobacteria, P.aeruginosa and Acinetobacter spp. Carbapenemases pose a challenge to the treatment of severe infections with carbapenems, but a direct correlation between carbapenemase production and carbapenem resistance has not been identified. One explanation for this fact is the difference in the hydrolytic activity of carbapenemases towards different substrates, such as various carbapenem preparations [41]. Other reasons may be a simultaneous decrease in penetration through the bacterial wall (changes in the structure of porin proteins) or the inaccessibility of target penicillin-binding proteins (presence of carbapenemases in the periplastic space). If carbapenemase production is present in clinical situations, carbapenems should not be used to treat infections caused by such microbes.
Porin-associated resistance
Reduced penetration into the bacterial cell is one of the mechanisms of resistance to carbapenems in enterobacteriaceae [41–45, 58]. The most well studied resistance in P.aeruginosa is associated with changes in the structure of the porin OprD, which passively captures basic amino acids and short peptides, but also serves as a channel for carbapenems [46, 47]. It is this mechanism of resistance that is characteristic of carbapenems and does not affect sensitivity to other β-lactam ABs. In P.aeruginosa, this mechanism is associated with a number of genetic mechanisms and leads to an increase in the MIC of imipenem by 4–16 times, meropenem by 4–32 times, and doripenem by 8–32 times [48–51]. Despite the apparent benefit of imipenem, its MIC rises above the level considered sensitive (4 μg/ml), while the MICs of doripenem and meropenem remain below 4 μg/ml [52].
P. aeruginosa resistance associated with efflux
Potentially resistant P.aeruginosa has genes on its chromosome that encode information about several efflux pumps that remove various antibiotics from the cell. The most studied are Mex-OprM, MexCD-OprJ, MexEF-OprN and MexXY. These pumps are capable of pumping out various drugs from the cytoplasm and periplastic space of the cell. As a result of the study of these pumps, prospects have opened for the development of new antibacterial drugs that can control the process of their operation. Taking this into account, it became clear that it was necessary to separately consider their role in resistance to imipenem, meropenem and doripenem in P.aeruginosa.
The pumps that remove imipenem are not exactly installed. However, it has been shown that with high expression of two efflux pumps (MexCD-OprJ and MexEF-OprN), there is a significant decrease in the sensitivity of P.aeruginosa to imipenem. It was shown that this mechanism is not associated with a combination of the β-lactamase activity of AmpC and OprD [53]. At the same time, high expression of MexCD-OprJ and MexEF-OprN leads to a significant decrease in sensitivity to imipenem due to decreased expression of OprD [50, 54, 55].
Unlike imipenem, meropenem is a suitable substrate for efflux pumps: it has been shown to be cleared from cells by MexAB-OprM, MexCD-OprJ and MexEF-OprN [57]. According to other studies, only overproduction of MexAB-OprM determines resistance to meropenem [8]. The influence of this mechanism explains the difference in resistance to imipenem and meropenem in P. aeruginosa strains that have such pumps. It is important to note that increased production of MexAB-OprM does not necessarily lead to a rise in BMD above the sensitivity level [56], but does indicate a likely interaction of this mechanism with others (eg, OprD-associated resistance) and is therefore of important clinical significance. With regard to doripenem, it was shown that it is a substrate for MexAB-OprM, MexCD-OprJ and MexEF-OprN efflux pumps; more detailed information is not available in the literature [57]. Thus, the interaction of mechanisms related to clearance, permeability impairment, β-lactamase activity, and PBP availability leads to clinically significant carbapenem resistance.
Dosing and clinical pharmacokinetics
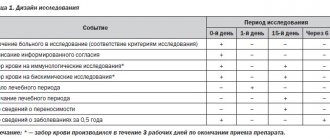
All carbapenems are water-soluble substances and are administered intravenously or intramuscularly due to low absorption from the gastrointestinal tract. The main dosages of drugs are presented in table. 1.
The amount of protein binding is an important indicator of the pharmacokinetics and antibacterial activity of drugs. Pharmacodynamic analysis of antibacterial drugs requires taking into account protein binding and discussing the kinetics of the “free” drug. As shown in table. 1, protein binding of imipenem (20%), doripenem (8%) and meropenem (3%) varies significantly [57, 58]. Changing the structure of ertapenem significantly increased dose-dependent protein binding: up to 95% at plasma concentrations below 100 mg/l and 85% above 300 mg/l. High protein binding results in longer elimination: the half-life of ertapenem is 4 hours compared to 1 hour for other carbapenems. The pharmacokinetic profile of the “free” drug after administration of a 500 mg dose shows its equivalence with imipenem, meropenem and ertapenem. In this case, predominantly renal clearance of the drug is observed in imipenem, meropenem and doripenem.
Due to its long half-life, ertapenem is the only carbapenem that is administered once daily (500 mg or 1 g) [58]. Meropenem is administered at 500 mg or 1 g after 8 hours, and imipenem at 500 mg or 1 g after 6-8 hours. A decrease in renal clearance requires a reduction in drug dosage, however, when using ertapenem, this clearance should be below 30 ml/min, when using meropenem - below 51 ml/min. The convulsive potential of imipenem requires special attention when choosing the dosage of the drug, taking into account renal function and body weight. Imipenem dosage reduction should begin after clearance decreases below 70 ml/min and in patients weighing less than 70 kg.
As stated earlier, the effectiveness of carbapenems depends on the duration of the intervals between drug administrations when its concentration is above the MIC. Optimization of pharmacodynamic parameters can be achieved by administering a higher dose, shortening the period between doses and increasing the duration of drug infusion [59]. The most attractive method is to increase the duration of infusion, because... this makes it possible to optimize pharmacodynamic parameters without significantly increasing economic costs. However, the duration of infusion is limited by the stability of the drug in solution: meropenem and imipenem at room temperature should be administered within 3 hours; The stability of doripenem reaches 12 hours [58, 60]. Currently, continuous infusion of carbapenems may be considered for meropenem and doripenem. However, the maximum permitted dosage for meropenem is 6 g of the drug per day, and for doripenem - 1.5 g/day. To optimize pharmacodynamic parameters, it is necessary to use the maximum dose and prolonged infusion of the drug. Pharmacodynamic modeling showed that the use of meropenem at a dose of 6 g per day and a 3-hour infusion creates conditions for the suppression of flora, which is interpreted in microbiological testing as resistant (up to 64 μg/ml). The possibility of using doripenem in such situations is limited by its low permitted daily dose (1.5 g).
Carbapenems and seizures
All β-lactams have the potential to cause seizures, especially when inappropriately dosed in settings with impaired renal function or low body weight, certain chronic pathologies, or increased seizure activity [61–64]. An increase in seizure activity was identified during the phase III clinical trial of imipenem, and later - of meropenem and ertapenem [42, 58, 65]. Various mechanisms can lead to seizures, but for carbapenems the main mechanism is inhibition of GABAa receptors [66, 67]. The side chain at position 2 of the 5-membered ring of carbapenems has been shown to be responsible for this complication. Moreover, at the highest concentration (10 mmol/l), imipenem suppresses 95% of GABA receptors that bind 3H-muscimol, meropenem suppresses 49%, and doripenem suppresses 10% [68]. This mechanism explains the occurrence of seizures in 1.5–6% of patients receiving imipenem [61, 69, 70]. A retrospective dose-response study suggested that low body weight, decreased renal function, a history of seizures, the presence of other central nervous system pathology, and high doses of imipenem/cilastatin should be considered risk factors for seizures [61]. An excess dose of imipenem/cilastatin is one that exceeds the recommended daily dose by 25% and the usual dose in patients with impaired renal function or concomitant CNS pathology. Careful dosage control of the drug has reduced the incidence of seizures to the level observed with meropenem and ertapenem (~0.5%) [70–72].
Conclusion
Carbapenems currently remain the most reliable drugs for the treatment of nosocomial infections in severely ill patients, especially in cases of infections caused by resistant flora. Taking into account current trends in the growth and spread of resistance in nosocomial flora, carbapenems are the main drugs for the treatment of infections caused by resistant gram-negative microbes (enterobacteria, P. aeruginosa, Acinetobacter spp.). The permitted daily doses and the possibility of prolonged infusion allow us to consider meropenem as the only drug whose pharmacodynamics can be optimized to suppress flora, which, from a microbiological point of view, is determined to be resistant to meropenem and other carbapenems.
First published in the Russian Medical Journal. - 2010. - Volume 18, No. 17.
Antibiotics-carbapenems
Home Medical encyclopedia Medicines Antimicrobial and antiparasitic medicines
ANTIBIOTICS-CARBAPENEMS
MEROPENEM (Mcropenem)
Synonyms: Meronem.
Pharmachologic effect. Broad-spectrum carbapenem antibiotic. It acts bactericidal (destroys bacteria), disrupting the synthesis of the bacterial cell wall. Active against many clinically significant gram-positive and gram-negative aerobic (developing only in the presence of oxygen) and anaerobic (capable of existing in the absence of oxygen) microorganisms, including strains producing beta-lactamases (enzymes that destroy penicillins).
Indications for use. Bacterial infections caused by pathogens sensitive to the drug: infections of the lower respiratory tract and lungs; infections of the genitourinary system, including complicated infections; abdominal infections; gynecological infections (including postpartum); skin and soft tissue infections; meningitis (inflammation of the membranes of the brain); septicemia (a form of blood infection by microorganisms). Empirical therapy (treatment without a clear definition of the cause of the disease), including initial monotherapy (treatment with one drug) for suspected bacterial infection in patients with weakened immunity (body defenses) and in patients with neutropenia (decreased number of neutrophils in the blood).
Method of administration and dose. Before prescribing a drug to a patient, it is advisable to determine the sensitivity to it of the microflora that caused the disease in this patient. The drug is administered intravenously every 8 hours. The single dose and duration of therapy are set individually, taking into account the location of the infection and the severity of its course. Adults and children weighing more than 50 kg for pneumonia (pneumonia), genitourinary tract infections, gynecological infections,
including endometritis (inflammation of the inner lining of the uterus), infections of the skin and soft tissues are prescribed in a single dose of 0.5 g. For pneumonia, peritonitis (inflammation of the peritoneum), septicemia, as well as if a bacterial infection is suspected in patients with neutropenia, a single dose of 1 g ; for meningitis - 2g. For children aged 3 months to 12 years, a single dose is 0.01-0.012 g/kg. In patients with impaired renal function, the dosage regimen is set depending on the values of creatinine clearance (the rate of blood purification from the final product of nitrogen metabolism - creatinine). Meropenem is administered as an intravenous injection over at least 5 minutes, or as an intravenous infusion over 15-30 minutes. For intravenous injections, the drug is diluted with sterile water for injection (5 ml per 0.25 g of the drug, which provides a solution concentration of 0.05 g/ml). For intravenous infusion, the drug is diluted with 0.9% sodium chloride solution, 5% or 10% glucose solution.
Side effect. Hives, rash, itching, abdominal pain, nausea, vomiting, diarrhea; headache, paresthesia (feeling of numbness in the limbs); development of superinfection (severe, rapidly developing forms of infectious disease caused by drug-resistant microorganisms that were previously in the body, but do not manifest themselves), including candidiasis (fungal disease) of the oral cavity and vagina; at the site of intravenous administration - inflammation and pain, thrombophlebitis (inflammation of the vein wall with its blockage). Less commonly - eosinophilia (increased number of eosinophils in the blood), thrombocytopenia (decreased number of platelets in the blood), neutropenia (decreased number of neutrophils in the blood); false-positive direct or indirect Coombs test (a test that diagnoses autoimmune blood diseases). Cases of reversible increases in serum bilirubin (bile pigment), enzyme activity: transaminases, silk phosphatase and lactate dehydrogenase have been described.
Contraindications. Hypersensitivity to the drug, to carbapenems, penicillins and other betalactam antibiotics.
Meropenem is prescribed with caution to patients with diseases of the gastrointestinal tract, especially colitis (inflammation of the colon), as well as to patients with liver diseases (under monitoring the activity of transaminases and the concentration of bilirubin in the blood plasma). You should keep in mind the possibility of pseudomembranous colitis (intestinal colic, characterized by attacks of abdominal pain and the release of large amounts of mucus in the stool) if diarrhea develops while taking an antibiotic. Coadministration of meropenem with potentially nephrotoxic (kidney damaging) drugs should be used with caution.
The drug should be prescribed with caution to patients with a history of allergic reactions.
The use of meropenem during pregnancy and lactation is possible only in cases where the potential benefit from its use, in the opinion of the doctor, justifies the possible risk to the fetus or child. In each case, strict medical supervision is required. There is no experience with the use of meropenem in pediatric practice in patients with neutropenia or secondary immunodeficiency. Efficacy and tolerability of the drug in children under 3 months of age. has not been established, and therefore it is not recommended for repeated use in this category of patients. There is no experience of use in children with impaired liver and kidney function.
Release form. Dry substance for intravenous administration in bottles of 0.5 g and 1 g.
Storage conditions. List B. In a dry place, protected from light.
| print version | This information is not a guide to self-treatment. A doctor's consultation is required. |