Pancreatin is a cheap domestic product for improving the functioning of the pancreas and stimulating digestion.
The cost of the medicine depends on the region, the policy of the pharmacy organization, dosage and number of tablets, on average it varies from 25 to 130 rubles.
Pancreatin analogues differ in manufacturer and price-quality ratio. Before purchasing, consult your doctor and read the instructions for use.
pharmachologic effect
Manufacturer: AVVA RUS, Biosintez, Pharmproekt, Avexima, Pharmstandard, Irbitsky KhMZ, etc., Russia
Release form: tablets
Active ingredient: pancreatin
Synonyms: Ermital, Enzistal, Mezim, Pangrol, Creon, Panzinorm, Fermentozim, etc.
The drug contains the substance pancreatin, which contains three enzymes - amylase, protease and lipase.
The components help break down food into small particles. As a result, proteins, fats and carbohydrates are better digested and completely absorbed in the small intestine.
Indications for use of Pancreatin
The drug belongs to the group of drugs that compensate for the deficiency of pancreatic enzymes. Applicable in the following cases:
- chronic pancreatitis, cystic fibrosis and other conditions accompanied by impaired and insufficient functioning of the pancreas, deficiency of necessary enzymes;
- diseases of the gastrointestinal tract, inflammatory-dystrophic nature;
- diarrhea, dyspeptic disorders, flatulence, indigestion;
- postoperative period, rehabilitation after radiation;
- elimination of unpleasant symptoms (heaviness, abdominal pain, flatulence) caused by overeating, changes in usual food, lifestyle, impaired chewing function, insufficient physical activity or inactivity;
- preparatory stage before examinations, ultrasound and surgery.
Important! The medicine Pancreatin is sold freely from pharmacies and is often advertised as a remedy for heaviness and stomach pain. However, it should not be abused. With regular replenishment of the deficiency of pancreatic enzymes, the synthesis of its own substances is disrupted.
Pancreatin before or after meals
The medicine should be taken during or after meals three times a day if pancreatic function is impaired. The tablets must not be chewed. If you are concerned about heaviness and pain in the abdomen due to overeating, a sedentary lifestyle and other factors, the medication can be taken once.
Note! Cheap Pancreatin from domestic manufacturers must be stored in the refrigerator to preserve its medicinal properties in the pharmacy and at home. Detailed conditions are indicated on the medicine box and on the insert.
The course depends on the indications and varies from 2 days to several years.
Conservative treatment of chronic pancreatitis on an outpatient basis
Chronic pancreatitis unites a heterogeneous group of diseases characterized by structural (morphological) and/or functional changes, despite the cessation of exposure to the etiological factor, with further progression of pancreatic damage and the development of exocrine and/or endocrine insufficiency. The morphological substrate of chronic pancreatitis is varying degrees of edema, inflammation and focal necrosis of acinar tissue, developing against the background of strictures along the pancreatic ducts, protein plugs and calcifications in small ducts; pseudocysts that occur during an attack of acute pancreatitis. All this leads to disruption of the flow of pancreatic juice, intraductal hypertension, progression of acinar tissue necrosis with subsequent atrophy of the acini; intralobular and perilobular fibrosis of the pancreas. With the loss of 90% of the functioning parenchyma, pancreatic insufficiency develops due to maldigestion syndrome.
In the later stages of the disease, with obvious exocrine pancreatic insufficiency or the development of diabetes mellitus, the diagnosis of chronic pancreatitis does not cause serious difficulties; certain obstacles arise in the early stages of the disease, when functional changes prevail, manifesting themselves most clearly during the action of the etiological factor. Diagnosis of chronic pancreatitis is based on the study of risk factors for its development, clarification of possible etiological factors, and assessment of the clinical picture of the disease. Often, the diagnosis of chronic pancreatitis is formed after long-term observation of a patient who has clinical signs suggesting the presence of chronic pancreatitis.
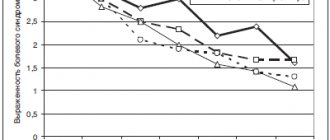
The etiological factors of chronic pancreatitis most often are 2 main causes - alcoholism and cholelithiasis, and 60-70% of all cases of chronic pancreatitis are caused by systematic, long-term (6-18 years) alcohol intake in a dose of more than 150 g per day before the development of obvious signs diseases (Table 1). The frequency of detection of chronic pancreatitis at autopsy in heavy drinkers reaches 45–50%. A high-protein diet and smoking exacerbate the damaging effects of alcohol. Alcohol-dependent pancreatitis develops predominantly in men and most often occurs between the ages of 35–45 years. A retrospective analysis of medical records and subsequent prospective observation of 372 patients made it possible to assess the course of chronic pancreatitis in idiopathic and alcoholic pancreatitis depending on the doses of alcohol consumed (less than 50 g/day and more than 50 g/day) [1]. It has been shown that in the group of patients with alcoholic pancreatitis, abdominal pain prevails at the onset of the disease. Patients from this group more often developed complications of chronic pancreatitis: fistulas, pseudocysts, abscesses, obstructive jaundice. It has been noted that in patients with the onset of chronic pancreatitis over the age of 35 years, drinking alcohol even in small doses (less than 50 g per day) leads to the early development of the disease, characterized by more frequent and intense abdominal pain, calcification of the pancreas and the presence of complications. Drinking large amounts of alcohol (50 or more grams per day) accelerates the formation of calcific pancreatitis and increases the incidence of fatal outcome in chronic pancreatitis.
Chronic pancreatitis, which develops with cholelithiasis (GSD), choledocholithiasis, is more common in women aged 50–60 years. As a rule, such patients show signs of metabolic syndrome: obesity, hyperlipidemia, a tendency to arterial hypertension, ischemic heart disease, impaired carbohydrate tolerance, hyperuricemia and/or hyperuricosuria, etc. In some patients with chronic pancreatitis, it is not possible to clarify the etiology of the disease - such pancreatitis is classified as to the group of idiopathic pancreatitis.
Recent studies have shown that the development of idiopathic pancreatitis may be caused by cholesterol microcrystals, bilirubinate granules and calcium microspherolites [2]. Dysfunction of the sphincter of Oddi (structural or functional) can also lead to the development of idiopathic pancreatitis, including due to the passage of microliths. Normally, the sphincter of Oddi performs 3 main functions: regulates the flow of bile and pancreatic juice into the lumen of the duodenum; prevents reflux of duodenal contents into the bile ducts and pancreatic duct; promotes filling of the gallbladder with hepatic bile. With dysfunction of the sphincter of Oddi, resistance to bile flow through the sphincter increases, as a result of which biliary colic develops in the absence of changes in the biliary system during a diagnostic examination (including ultrasound of the bile ducts (Fukuda, Aloka, Philips)); postcholecystectomy abdominal pain and chronic recurrent pancreatitis. Manometry (DSP-US, MTM-1, MA-4) of the sphincter of Oddi determines an increase in basal sphincter pressure in 15–57% of patients with a similar form of pancreatitis. The presence of biliary-type sphincter of Oddi dysfunction may be indicated by typical biliary-type pain, an increase in the level of aspartate aminotransferase and/or serum alkaline phosphatase by more than 2 times; prolongation of contrast transit time during endoscopic retrograde cholangiopancreatography (ERCP) by more than 45 minutes and dilatation of the common bile duct by more than 12 mm. With dysfunction of the sphincter of Oddi of the pancreatic type, there is a more than 2-fold increase in the level of pancreatic enzymes during successive attacks of pain, as well as an expansion of the pancreatic duct of more than 5 mm3.
Depending on the morphological changes in the pancreas, the following forms of chronic pancreatitis are distinguished (1989): calcifying, obstructive, fibrous-indurative pancreatitis, as well as cysts and pseudocysts of the pancreas. The group of calcifying pancreatitis includes alcoholic pancreatitis, pancreatitis that develops under the influence of organic solvents, certain chemical compounds, drugs, as well as pancreatitis that begins as a result of hyperlipidemia, hypercalcemia with hyperparathyroidism, chronic viral infections (including chronic HCV and HBV infections), congenital changes in the pancreatic ducts (doubling of the pancreatic duct - pancreas divisum). Hereditary pancreatitis with an autosomal dominant type of inheritance with incomplete penetration also belongs to the group of calcific pancreatitis and develops in children 10–12 years old or at the age of 30–40 years. It is indistinguishable from the usual forms of pancreatitis, is accompanied by recurrent attacks of abdominal pain; after 8–10 years, diabetes mellitus develops in 20% of patients and severe steatorrhea in 15–20% of patients. The absence of other etiological factors and indications of cases of pancreatitis in the family justify the suspicion of a hereditary form of chronic pancreatitis.
Chronic obstructive pancreatitis develops with obstruction of the main pancreatic duct by a pancreatic tumor, inflammation of the duodenal papilla or its stenosis, duodenitis due to Crohn's disease, closed abdominal trauma and surgical operations in the pyloroduodenal zone, the presence of pancreatic pseudocysts, congenital anomalies (pancreas divisum). Gallstone disease and choledocholithiasis, dysfunction of the sphincter of Oddi of the biliary and pancreatic types are the main causes of the formation of chronic obstructive pancreatitis.
Clarification of the etiological factor in the development of chronic pancreatitis allows for more effective prevention and treatment, which explains the appearance of the following classification of chronic pancreatitis according to the etiological principle, taking into account the morphological variant:
- alcoholic (calcific) pancreatitis;
- idiopathic juvenile and senile;
- tropical;
- hereditary;
- chronic obstructive pancreatitis.
Clinical signs of chronic pancreatitis are most clearly presented during the period of exacerbation (Table 2).
| Clinical signs of chronic pancreatitis |
Often the development of the painful form of chronic pancreatitis is preceded by a painless, latent stage of varying duration, masked by epigastric discomfort, flatulence, unstable stool with a tendency to diarrhea with the presence of undigested fiber in the stool or steatorrhea. Repeated attacks of the painful form of chronic pancreatitis form pancreatic insufficiency with predominant damage to exocrine or endocrine functions with the development of type 2 diabetes mellitus.
Pain syndrome - the most constant sign of acute and chronic pancreatitis - is observed in 70–80% of cases and has typical symptoms: localization in the epigastrium, “girdling” character with irradiation to the back, provoked and quickly intensifying after eating; the pain is relieved by sitting and bending forward. Often accompanied by nausea, vomiting, and fever. In 3–6% of patients, pain attacks can last several days; in 70–90%, episodes of pain are interspersed with a pain-free period. In some patients, the equivalent of epigastric pain may be back pain, sometimes comparable to the intensity of abdominal pain. In the genesis of abdominal pain syndrome in chronic pancreatitis, the main attention is paid to intraductal hypertension due to the persistent secretion of pancreatic enzymes by the inflamed gland under conditions of obstruction of the main or small ducts. Other factors - inflammation of the intrapancreatic nerve trunks, peripancreatic inflammation involving the duodenum, retroperitoneal space, stenosis of the distal common bile duct - also play a role in the development of pain. In 15% of patients, a painless form of the disease is observed, which manifests itself in 1/3 of patients with steatorrhea, most often this occurs with chronic calcific pancreatitis of alcoholic etiology. Endocrine function is most sensitive to the inflammatory process in chronic pancreatitis and is manifested in 2/3 of patients by impaired glucose tolerance and diabetes mellitus. In most cases, both exocrine and endocrine functions are affected; signs of pancreatic insufficiency develop with the loss of 80–90% of the functioning pancreatic parenchyma. In some cases, a progressive decrease in exocrine function leads to a decrease and even complete disappearance of pain.
Data on the effect of abstinence on the course of alcoholic pancreatitis are contradictory: in some patients, giving up alcohol leads to a decrease in the severity and frequency of pain attacks, signs of exo- and endocrine insufficiency, while others experience increased pain after 12–24 hours of abstinence. The course of chronic pancreatitis can be unpredictable - progressive, despite strict abstinence, and quite stable, regardless of continued alcohol intake. In one observation, 45% of patients who abused alcohol did not have clinical symptoms of pancreatitis, but had signs of chronic pancreatitis at autopsy.
Nausea, vomiting, anorexia, and weight loss are common in chronic pancreatitis. One of the main reasons for weight loss is a decrease in the caloric intake of food intake due to increased abdominal pain, as well as the developing malabsorption syndrome due to maldigestion and uncompensated diabetes mellitus. During chronic pancreatitis, malabsorption syndrome with diarrhea and steatorrhea develops relatively late, usually against the background of less than 20% of functioning acinar tissue. In some patients, malabsorption syndrome may occur with formed stool, which is explained by good absorption of water by the unchanged mucosa of the small intestine and a small amount of water in the stool. Sometimes patients note greasy spots on the surface of the water in the toilet, “greasy”, shiny feces that are difficult to wash off from the walls of the toilet, which usually indicates pancreatic steatorrhea. The absorption of fat-soluble vitamins A, D, E, K suffers little; significant deficiency is rarely detected in pancreatic insufficiency.
Although impaired glucose tolerance is common and presents early in chronic pancreatitis, clinically apparent diabetes mellitus occurs relatively late. In most patients, the diagnosis of chronic pancreatitis is established long before the development of hyperglycemia, however, in some of them suffering from a painless form of pancreatitis, diabetes mellitus may be the first and only manifestation of the disease. A feature of the course of diabetes mellitus in chronic pancreatitis should be considered the rare development of ketoacidosis, diabetic nephropathy and good tolerance of hyperglycemia levels up to 200 mg/dl, however, with long-term diabetes, retinopathy and polyneuropathy occur with the same frequency for different types of diabetes.
Other clinical manifestations of chronic pancreatitis include jaundice due to compression of the common bile duct by the enlarged head of the pancreas, ascites or pleural effusion due to leakage of pancreatic secretions from destroyed ducts; pseudocysts. Atypical variants of chronic pancreatitis with the development of liponecrosis of the subcutaneous tissue or “chemical” polyarthritis of small joints of the hands are rare.
The mortality rate for chronic pancreatitis reaches 50% with a 20-25 year duration of the disease. 15–20% of patients die from complications associated with exacerbations of pancreatitis; other deaths are caused by trauma, malnutrition, infection, smoking, which are often observed in patients with chronic pancreatitis.
Complications of chronic pancreatitis include malabsorption syndrome, diabetes mellitus, pseudocysts, portal or splenic vein thrombosis, pyloric stenosis, common bile duct obstruction, and tumor. Pancreatic adenocarcinoma develops in 4% of cases in individuals with more than a 20-year history of chronic pancreatitis.
Diagnosis of chronic pancreatitis is quite complex and is based on 3 main signs: a characteristic history (pain attacks, alcohol abuse), the presence of exocrine and/or endocrine insufficiency and identification of structural changes in the pancreas.
The level of amylase and serum lipase often remains normal or reduced during an attack of pancreatitis, which is explained by a decrease in the number of acinar cells producing these enzymes. When alcoholic pancreatitis is combined with alcoholic liver disease, abnormal liver function tests may be detected. In 5–10% of cases of chronic pancreatitis, there are signs of compression of the intrapancreatic part of the bile duct caused by edema or fibrosis of the head of the pancreas, which is accompanied by jaundice, increased levels of direct bilirubin and serum alkaline phosphatase.
Impaired glucose tolerance develops in 2/3 of patients, diabetes mellitus in 30% of patients with chronic pancreatitis.
Exocrine insufficiency becomes obvious and easily detected with the development of malabsorption syndrome, in which fat in the feces can be determined qualitatively (Sudan stain) or quantitatively. Secretory insufficiency is detected at earlier stages using pancreatic functional tests.
In recent years, an enzyme-linked immunosorbent method for determining elastase-1 in the blood serum and feces of patients has been introduced into clinical practice for the diagnosis of chronic pancreatitis, which makes it possible to assess the exocrine function of the pancreas [4].
Instrumental data to confirm the assumption of the presence of chronic pancreatitis can be considered quite informative. Ultrasound examination of the abdominal organs is used; endoscopic ultrasound, spiral computed tomography and magnetic resonance imaging of the pancreas. ERCP can detect duct stenosis, localization of obstruction, structural changes in small ducts, intraductal calcifications and protein plugs, but there is a high risk of developing acute pancreatitis [5, 6].
The goal of treatment of chronic pancreatitis can be considered to solve several problems: eliminating provoking factors (alcohol, drugs, obstruction); pain relief; correction of exo- and endocrine insufficiency; treatment of associated disorders. The main goals of conservative treatment are to stop or slow the progression of chronic pancreatitis and combat its complications. Depending on the severity of abdominal pain, a step-by-step treatment of chronic pancreatitis is used, including the following components (modified by Ihse et al., 1993).
- Diet, fractional meals, fats less than 60 g/day.
- Pancreatic enzymes (Pancreatin, Creon, Mezim, Panzinorm, Festal, Pensital, Enzistal) + H2 blockers (famotidine, ranitidine, cimetidine, nizatidine).
- Non-narcotic analgesics (acetylsalicylic acid, diclofenac, ibuprofen, piroxicam).
- Octreotide (Sandostatin).
- Endoscopic drainage (Olimpus, LOMO, Pentax, Fujinon).
- Narcotic analgesics (butorphanol, antaxone, fortal, tramadol, sedalgin-neo).
- Solar plexus block.
- Surgical intervention.
With mild pain syndrome, success can be achieved through a strict diet, small meals (every 3 hours) and limiting fat to 60 g per day, which helps reduce pancreatic secretion with a low-calorie diet. Given the fact that the main cause of pain is intraductal hypertension, it is advisable to use drugs that block stimulated pancreatic secretion. Normally, the release of cholecystokinin, the main stimulator of exogenous pancreatic function, is regulated by cholecystokinin-releasing peptide in the proximal small intestine, which is sensitive to trypsin and active in the intestinal lumen. The administration of pancreatic enzymes (mezim forte, pancreatin, panzinorm, pancitrate lycrease) provides significant relief of pain in some patients due to the inclusion of a feedback mechanism: an increase in the level of proteases in the lumen of the duodenum reduces the release and synthesis of gastrointestinal hormones (cholecystokinin), which leads to a decrease stimulation of exocrine pancreatic function, reduction of intraductal and tissue pressure and pain relief [7, 8].
One should be aware of the possibility of inactivation of exogenous digestive enzymes by stomach acid and pancreatic proteases. To prevent this effect, a combination of enzymes (Pancreatin, Creon, Mezim, Panzinorm, Festal, Penzital, Enzistal) with H2-histamine blockers (famotidine, ranitidine, cimetidine, nizatidine) is widely used. Doses of enzyme preparations for pain relief must be adequate; in a placebo-controlled, double-blind study, pancreolipase at a dose of 6 tablets 4 times a day for 1 month significantly reduced pain in 75% of patients with moderate to severe pancreatitis. Pancreatic enzymes in encapsulated form containing acid-resistant mini-microspheres (Creon) are currently the first choice drugs in the treatment of abdominal pain in exocrine pancreatic insufficiency. Microgranular dosage forms (Creon 10,000 or 25,000) are characterized by rapid (after 45 minutes) release of more than 90% of enzymes at a pH of duodenal and small intestinal contents of 5.5 and above. At very low pH values in the gastrointestinal tract, adjuvant therapy with H2 antagonists or proton pump inhibitors (lansoprazole, omeprazole, pantoprazole, rabeprozole) is used. In addition, enzyme replacement therapy has been shown to improve the transit of food through the gastrointestinal tract, affecting the motor function of the gastrointestinal tract and thereby helping to reduce malabsorption. Pancreatic enzymes are prescribed in all cases of chronic pancreatitis to correct the exocrine function of the pancreas. Taking these drugs reduces intestinal distension and diarrhea caused by malabsorption of fats, and therefore reduces pain. Enzyme preparations reduce the intensity of pain in moderate chronic pancreatitis, especially in women with obstructive pancreatitis; against the background of pancreas divisum. In men with alcoholic calcific pancreatitis, these drugs are significantly less effective. To relieve steatorrhea in chronic pancreatitis, film-coated drugs with a high lipase content are indicated; for pain relief - drugs with a high content of proteases without a coating.
If there is no effect of enzyme replacement therapy in combination with H2-histamine blockers, it is necessary to prescribe analgesics; for this purpose, paracetamol (daleron, prodol, efferalgan), non-steroidal anti-inflammatory drugs: diclofenac (apo-diclo, voltaren, diclofenac, ortofen), ibuprofen (apo -ibuprofen, ibuprofen, ibufen, solpaflex), piroxicam (piroxicam, piroxifer, felden, erazon), celecoxib (celebrex), lornoxicam (xefocam), meloxicam (meloxicam, movalis), nimesulide (mesulide, nise, niculid), naproxen (apo -naproxen, nalgesin, naproxen). To relieve pain in chronic pancreatitis, octreotide (Sandostatin) is prescribed. As a potent inhibitor of neuroendocrine hormones of the gastrointestinal tract, sandostatin inhibits exogenously stimulated and endogenously stimulated exocrine pancreatic secretion by direct action on exocrine tissue and reduces the release of secretin and cholecystokinin. In a multicenter study, sandostatin at a dose of 200 mcg subcutaneously 3 times a day for 4 weeks reduced the severity of pain in 65% of patients with chronic pancreatitis. The drug is also effective in the treatment of pseudocysts, pancreatic ascites and pleurisy. We use small doses: 50–100 mcg subcutaneously 2 times a day for 1 week to treat painful chronic pancreatitis.
If the pain syndrome persists, it is necessary to perform ERCP to morphologically clarify the nature of the lesion of the ducts and exclude dysfunction of the sphincter of Oddi. In this case, the possibility of using invasive treatment methods is discussed: endoscopic drainage and bypass, solar plexus blockade with steroids, pancreaticojejunostomy and pancreatic resection.
The greatest difficulties are associated with the treatment of dysfunction of the sphincter of Oddi, one of the causes of the development of chronic pancreatitis, which is difficult to diagnose. With dysfunction of the sphincter of Oddi, there is increased sensitivity of the wall of the pancreatic and bile ducts to changes in volume and pressure. It is necessary to exclude drugs that have a choleretic effect (bile acids, including those contained in enzyme preparations - festal, enzistal, etc.; decoctions of choleretic herbs, synthetic choleretic agents). To relieve spasm of the smooth muscles of the sphincters of Oddi and the cystic duct, nitrates are used: nitroglycerin for quick pain relief, nitrosorbitol for a course of treatment (under drug tolerance monitoring).
Myotropic antispasmodics (bendazole, bencyclane, drotaverine, mebeverine, papaverine) reduce the tone and motor activity of smooth muscles. The main representatives of this group are papaverine, drotaverine (no-shpa, no-shpa forte, vero-drotaverine, spasmol, spakovin), bencyclane (halidor).
The most effective myotropic antispasmodic is duspatalin (mebeverine) - a muscletropic, antispastic drug that has a direct effect on smooth muscles. By selectively acting on the sphincter of Oddi, it is 20-40 times more effective than papaverine in terms of its ability to relax the sphincter of Oddi.
It is important that duspatalin does not affect the cholinergic system and therefore does not cause side effects such as dry mouth, blurred vision, tachycardia, urinary retention, constipation and weakness. It is actively metabolized when passing through the liver, all metabolites are quickly excreted in the urine. Complete excretion of the drug occurs within 24 hours after taking a single dose; as a result, it does not accumulate in the body; even elderly patients do not require dose adjustment. Duspatalin is prescribed 1 capsule (200 mg) 2 times a day, it is better to take it 20 minutes before meals.
Another myotropic antispasmodic with selective properties is hymecromone (odeston), a phenolic derivative of coumarin that does not have anticoagulant properties and has a pronounced antispasmodic and choleretic effect. Hymecromone is a synthetic analogue of umbelliferone, found in anise and fennel fruits, which were used as antispasmodics. The drug provides one or another effect depending on the characteristics of its action at various levels of the biliary tract. Odeston causes dilatation of the gallbladder, reduces intraductal pressure and, thus, is an antagonist of cholecystokinin. At the level of the sphincter of Oddi, it acts synergistically with cholecystokinin, reduces basal pressure and increases the duration of opening of the sphincter of Oddi, thereby increasing the passage of bile through the bile ducts. Being a highly selective antispasmodic, odeston also has choleretic properties. Its choleretic effect is due to the acceleration and increase in the flow of bile into the small intestine. An increase in the flow of bile into the lumen of the duodenum helps to improve digestion processes, activate intestinal motility and normalize stool.
Odeston is prescribed 400 mg (2 tablets) 3 times a day 30 minutes before meals, which ensures a relatively constant drug concentration in the serum exceeding 1.0 mcg/ml. The duration of treatment is individual - from 1 to 3 weeks. Odeston is low-toxic and is usually well tolerated.
If there is no effect from conservative therapy for sphincter of Oddi dysfunction and there is evidence of its stenosis, restoration of the patency of the sphincter of Oddi is carried out surgically (sphincterotomy).
Replacement therapy for exocrine pancreatic insufficiency as a result of chronic pancreatitis is carried out in the presence of steatorrhea of more than 15 g of fat per day, progressive loss of body weight and dyspeptic disorders. A single dose of enzymes must contain at least 20,000–40,000 units of lipase, so it is prescribed 2–4 capsules with main meals and 1–2 capsules with additional small amounts of food. With clinically significant pancreatic insufficiency, it is often not possible to eliminate steatorrhea completely. An increase in body weight, normalization of stool, and a decrease in flatulence indicate the adequacy of the selected dose of digestive enzymes. The ineffectiveness of replacement therapy requires the exclusion of other causes of malabsorption syndrome - Crohn's disease, celiac disease, thyrotoxicosis. To correct nutritional deficiencies, medium chain triglycerides (trisorbon) and fat-soluble vitamins A, D, E, K are prescribed.
For questions regarding literature, please contact the editor.
T. N. Lopatkina , Candidate of Medical Sciences, Associate Professor of MMA named after. I. M. Sechenova, Moscow
Pancreatin analogues
Pharmacies offer analogues and substitutes of Pancreatin of several groups:
- synonyms – drugs of domestic or imported origin containing pancreatin;
- combination products – along with pancreatin, they contain other medicinal substances;
- analogues from other pharmacological groups, but having the same properties and indications.
Pancreatin substitute drugs with prices and country of origin
| Analogue | Price, in rubles | Manufacturer country |
| Pancreatin | 25-130 | Russia |
| Allohol | 10-90 | Russia |
| Holenzym | 200-320 | Russia, Belarus |
| Enzistal | 130-560 | India |
| Creon | 280-670 | Germany |
| Omeprazole | 25-160 | Russia, Hungary |
| Pangrol | 240-1230 | Germany or Italy |
| Unienzyme | 90-160 | India |
| Mezim | 80-320 | Germany |
| Festal | 90-840 | India |
| Penzital | 60-240 | India |
| Micrasim | 210-870 | Russia |
| Panzinorm | 140-310 | Slovenia |
| Hermital | 160-1090 | Germany |
Allohol
Manufacturer: Biosynthesis, Pharmstandard, etc., Russia
Release form: tablets
Active ingredient: activated carbon, bile, dry garlic, nettle extract
The cheap analog Allohol is designed for better functioning of the gastrointestinal tract:
- prevents fermentation and decay processes;
- has a choleretic effect;
- helps with atonic constipation.
It is used in courses depending on the patient’s indications and complaints - from 3–4 weeks to 3 months.
Holenzym
Manufacturer: Belmedpreparaty, Belarus or Biosintez, Russia
Release form: tablets
Active ingredient: bile, pancreas powder, small intestinal mucosa powder
The Cholenzym analogue combines several properties: it promotes the formation and secretion of bile, improves digestion, and facilitates the digestion of incoming proteins, fats and carbohydrates. The drug is suitable not only for diseases of the digestive tract, but also to facilitate digestion during a sedentary lifestyle, a change in diet, and overeating. Cholenzym is taken 1-3 times a day depending on the symptoms and severity of the condition.
Enzistal
Manufacturer: Torrent Pharmaceuticals, India
Release form: tablets
Active ingredient: pancreatin, bile components, hemicellulase
An analogue of Pancreatin in tablets is the combined drug Enzistal. Contains additional components, resulting in a wider range of therapeutic effects:
- promotes better digestion of food and breakdown of proteins, fats, carbohydrates;
- relieves or alleviates symptoms associated with digestive disorders - pain after eating in the abdominal area, increased gas formation, flatulence, shortness of breath, heaviness;
- reduces the formation of gases in the intestines;
- increases bile production;
- promotes better absorption of incoming vitamins and minerals.
Also available in pharmacies is the drug Enzistal-P - an analogue containing only pancreatin, without additional components. The advantage is that you don’t need special conditions for storage or refrigeration.
Omeprazole
Manufacturer: Ozone, Kanonpharma, Promed, AVVA RUS, Sintez, Russia or Teva, Hungary
Release form: capsules
Active ingredient: omeprazole
Synonyms: Omez, Gastrozol, Ultop, Losek, Ortanol, etc.
The prescription analogue Omeprazole acts on stomach cells and reduces the production of hydrochloric acid. As a result, heartburn, stomach pain, sour belching and other symptoms of dyspepsia and gastritis are reduced.
Pangrol
Manufacturer: Berlin-Chemie, Germany or Italy
Release form: capsules
Active ingredient: pancreatin
The drug Pangrol is an analogue of Pancreatin in capsules, which is more effective. The capsule contains mini-tablets. Pancreatin analogue 10,000 units enters the stomach, the gelatin shell of the capsule dissolves. The active substance itself begins to act exclusively in the intestines.
Other analogues of Pancreatin
You can learn about other substitutes in pharmacy windows, in advertising or from doctor's prescriptions.
- Unienzyme is a drug for better digestion, replenishes enzyme deficiency, eliminates heaviness in the abdomen, diarrhea and other symptoms of intestinal dysfunction.
- Wobenzym is an enzyme preparation that reduces inflammation in the gastrointestinal tract and the entire body, the disadvantage is its high cost.
- Karsil is a medicine for protecting and restoring the liver and eliminating associated symptoms (pain, heaviness, bitterness).
- No-Shpa is an antispasmodic drug for pain and colic.
- Trimedat is an imported analogue that regulates intestinal motility and eliminates problems with stool (diarrhea or constipation), flatulence, bloating, and a feeling of heaviness.
- Motilium - regular and dispersible tablets, the suspension has the same effect as Trimedat, additionally eliminating nausea and vomiting.
Pancreatin (Creon, Mezim, Panzinorm, Festal)
- Page content:
- Table of analogues and prices
- Answers from the site author to typical requests from page visitors
- Creon (pure Pancreatin): instructions for use
- Festal (combined drug): instructions for use
- Children's dosages in the instructions for enzyme preparations
There are contraindications. Consult your doctor.
Preparations containing Pancreatin (Pancreatin, ATC code A09AA02):
Common forms of release of pure PancreatinCommon forms of release of combined preparations of PancreatinCommon forms of release of enzyme preparations of plant originRare and discontinued forms of release of pure PancreatinRare and discontinued forms of release of combined preparations of Pancreatin
| Name, manufacturer | Release form | Pack, pcs. | Price, r |
| Kreon 10 thousand (Kreon 10.000); Germany, Abbott | capsules 150 mg, 10 thousand units | 20 | 230-350 |
| Kreon 25 thousand (Kreon 25,000); Germany, Abbott | capsules 300 mg, 25 thousand units | 20 | 480-700 |
| Mezim 20 thousand (Mezym 20,000); Germany, Berlin Hemi | tablets 20 thousand units | 20 | 200-320 |
| Mezim Forte; Germany, Berlin Hemi | tablets 137.5 mg, 10 thousand units | 20 | 60-290 |
| 80 | 230-360 | ||
| Mezim Forte 10 thousand (Mezym Forte); Germany, Berlin Hemi | tablets 137.5 mg, 10 thousand units | 20 | 160-225 |
| Mikrazym; Russia, ABVA RUS | capsules 10 thousand units | 20 | 165-297 |
| 50 | 380-535 | ||
| capsules 25 thousand units | 20 | 345-540 | |
| 50 | 700-870 | ||
| Pangrol 10 thousand (Pangrol 10,000); Italy, Aptalis | capsules | 20 | 210-570 |
| 50 | 455-715 | ||
| Pangrol 25 thousand (Pangrol 25,000); Italy, Aptalis | capsules | 20 | 405-630 |
| 50 | 870-1.230 | ||
| Panzinorm 10 thousand (Panzynorm 10.000); Slovenia, KRKA | capsules 10 thousand units | 21 | 105-160 |
| Panzynorm Forte 20 thousand (Panzynorm Forte 20,000); Slovenia, KRKA | tablets 20 thousand units | 10 | 80-270 |
| 30 | 200-300 | ||
| 100 | 360-370 | ||
| Penzital; India, Shreya | tablets 212.5 mg, 6 thousand units | 10 | 180-205 |
| 20 | 45-70 | ||
| 30 | 170-180 | ||
| 80 | 150-210 | ||
| 100 | 170-210 | ||
| Enzystal-P; India, Torrent | tablets 116mg | 20 | 60-170 |
| Ermytal; Germany, Nordmark | capsules 10 thousand units | 20 | 90-200 |
| 50 | 325-480 | ||
| capsules 25 thousand units | 20 | 305-410 | |
| 50 | 580-775 | ||
| capsules 36 thousand units | 20 | 400-510 | |
| 50 | 940-1.060 | ||
| Pancreatin; Russia, various | tablets 25 units | 20 and 60 | 15-75 |
| Pancreatin | tablets 30 units | 60 | 15-70 |
| Name, manufacturer, composition | Release form | Pack, pcs. | Price, r |
| Festal; India, Aventis; pancreatin 192 mg (6 thousand units), dry. extra ox bile 25 mg, hemicellulase 50 mg | dragee | 20 | 110-280 |
| 40 | 200-420 | ||
| 100 | 530-1.050 | ||
| Enzystal; India, Torrent; pancreatin 192 mg (6 thousand units), dry extra. ox bile 25 mg, hemicellulase 50 mg | pills | 20 | 65-220 |
| 80 | 220-590 | ||
| 100 | 340-440 | ||
| Cholenzym; different; bile + yellow powder glands + small intestinal mucous powder | pills | 50 | 170-380 |
| Name, manufacturer, composition | Release form | Pack, pcs. | Price, r |
| Unienzyme with MPS; India, Uniquem; fungal diastase 20 mg, papain 30 mg, simethicone (espumisan) 50 mg, carbon act. 75 mg, nicotinamide 25 mg | pills | 20 | 75-180 |
| Name, manufacturer | Release form | Pack, pcs. | Price, r |
| Kreon 40 thousand (Kreon 40,000); Germany, Abbott | capsules 400 mg, 40 thousand units | 50 | 1.290-1.550 |
| Vestal; Russia, ShchVZ | pills | 50 | No |
| Gastenorm Forte; India, Rusan | pills | 20 | No |
| Pankreazim, Ukraine | tablets 240mg | 20 | No |
| Pankreon 10 thousand, Germany, Cali | tablets 250mg | 50 and 100 | No |
| Pancitrate (Panzytrat); Germany, Nordmark | capsules 25,000 units | 20 | No |
| Forte Enzyme; India, Rusan | pills | 100 | No |
| Name, manufacturer, composition | Release form | Pack, pcs. | Price, r |
| Biofestal; Russia, Biopharma | dragee | 20 | 120-140 |
| Normoenzyme forte; Russia, Pharmstandard | pills | 30 | No |
- Other enzyme preparations
- All drugs used in gastroenterology
- or leave a review about the medicine
- Which generic is better?
- Where can I buy?
Pancreatin or Creon - which is better for the pancreas
Manufacturer: Abbott, Germany
Release form: capsules
Active ingredient: pancreatin
Creon 10000 and 25000 are several times more effective than Pancreatin for a number of reasons:
- this is an original drug with an evidence base;
- capsules contain minimicrospheres that are resistant to gastric juice due to the shell;
- safety and possibility of use by children of the first year of life and pregnant women;
- the therapeutic effect begins 15 minutes after entering the intestines;
- convenient storage in a jar, no need to put it in the refrigerator to preserve its properties;
- positive reviews from doctors and patients.
Another advantage of Creon is the ability to open capsules and add them to liquid or soft sour foods. This is especially important when treating children and patients with swallowing difficulties.
The cost of Creon is higher.
When choosing between Creon or Pancreatin for one-time use, you can choose the second drug. It is up to 6 times cheaper than its analogue.
What is the difference between Creon or Pancreatin according to doctors and pharmacists:
- Release form: the first is in capsules, the second in tablets.
- The place of action is in the intestines and stomach, respectively.
- Efficiency - Creon is stronger, since all enzymes reach the intestines and begin to act there; Some of the Pancreatin enzymes are destroyed in the stomach.
- Storage – Creon does not require special conditions; Pancreatin must be placed in the refrigerator.
What to choose depends on the indications, frequency of use and financial capabilities.
Application of Creon, Mezim and Festal, differences between drugs, instructions for use and analogues
Currently, on pharmacy shelves you can find a wide range of drugs to improve digestion. They differ in the components that are included in the composition, as well as in the mechanism of action on the gastrointestinal tract. The most popular include Creon, Mezim and Festal.
What is the difference between the drugs
Creon, Mezim and Festal do not differ much in parameters, but they should be taken into account before starting drug treatment. There is a definite difference between the drugs in the amount of essential enzymes.
Of the three medications, only Creon is approved for use in children over one year of age. Festal and Mezim are not suitable for such a young age.
The price of Creon differs significantly compared to other drugs, but at the same time it has a huge number of advantages. The German company guarantees the result, as well as the exact calculation and balance of active ingredients.
In analogues, the content of amylase, lipase and protease fluctuates, and there are no sufficient calculations based on enzyme data.
In addition, Creon dissolves in the small intestine, which expands the possibilities and increases the positive effect.
Festal has more contraindications compared to the other two drugs; the capsule shell of this medicine also dissolves under the influence of gastric juice. Therefore, not all enzymes reach the small intestine. This is a big drawback of the medication, since it has a reduced percentage of absorption in relation to the same Creon.
Mezim is more suitable for one-time use, since it has not been studied as thoroughly as Creon. Mezim is an analogue and belongs to medicines of lower quality, but affordable in the price range.
Doctors note that Creon has a higher speed of action and side effects are less common.
The price difference is also obvious. Creon is the most expensive drug of the above, since it is produced in Germany and is a brand name. It has certain advantages, which affect the price. A package of this medication with a dosage of 10,000 in 20 capsules costs 280 rubles. 20 tablets of Mezim in the same dosage will cost 170, and Festal - 130 rubles.
Pancreatin or Mezim – which is better?
Manufacturer: Berlin-Chemie, Germany
Release form: tablets
Active ingredient: pancreatin
Mezim Forte is an imported analogue based on pancreatin to improve the absorption of food, the breakdown of proteins, fats and carbohydrates and the treatment of diseases of the pancreas, stomach and intestines.
What is the difference between the drugs:
- manufacturer: Mezim forte is an imported medicine, Pancreatin is produced by domestic pharmaceutical companies;
- price – the cost of Mezim is higher than the price of Pancreatin;
- the enzyme activity of the analogue Mezim Forte is higher and it is accurately calculated; in the Russian preparation only an approximate range is indicated;
- domestic medicine requires special storage conditions - in the pharmacy and at home it must be placed in the refrigerator.
Thus, Mezim is more effective and has positive reviews from doctors. Pancreatin is cheaper and can replace expensive medicine for mild overeating or lifestyle changes. To preserve the therapeutic effect, the enzyme preparation should be placed on the refrigerator shelf immediately after purchase.
Symptoms
Pain in the epigastric region and left hypochondrium, dyspepsia, diarrhea, weight loss, diabetes mellitus. The pain is localized in the epigastric region on the right when the process is predominantly localized in the region of the head of the pancreas, when its body is involved in the inflammatory process - in the epigastric region on the left, when its tail is affected in the left hypochondrium; Often the pain radiates to the back and has a girdling character; it can radiate to the heart area, simulating angina pectoris. The pain can be constant or paroxysmal and appear some time after eating fatty or spicy foods. There is pain in the epigastric region and left hypochondrium. Often there is a painful point in the left costovertebral angle (Mayo-Robson symptom). Sometimes a zone of skin hyperesthesia is determined corresponding to the zone of innervation of the eighth thoracic segment on the left (Kach’s symptom) and some atrophy of the subcutaneous fatty tissue in the area of the projection of the pancreas onto the anterior wall of the abdomen.
Dyspeptic symptoms in chronic pancreatitis are almost constant. Complete loss of appetite and aversion to fatty foods are common. However, with the development of diabetes mellitus, on the contrary, patients may feel severe hunger and thirst. Increased salivation, belching, attacks of nausea, vomiting, flatulence, and rumbling in the stomach are often observed. In mild cases, stool is normal, in more severe cases there is diarrhea or alternating constipation and diarrhea. Characterized by pancreatic diarrhea with the release of copious, pasty, foul-smelling, greasy-looking burl; scatological examination reveals steatorrhea, creatorrhoea, kitarhinorrhea.
Pancreatin or Festal
Manufacturer: Sanofi India Limited
Release form: pills
Active ingredient: bile components, pancreatin, hemicellulase
Synonyms: Enzistal
Festal is a combined analogue of Pancreatin, which has three medicinal properties:
- breaks down proteins, fats and carbohydrates, promoting better digestion;
- eliminates seething;
- relieves bloating and heaviness in the abdomen.
For pancreatitis, it is better to give preference to pure Pancreatin or drugs containing exclusively this substance (Creon, Penzital, Panzinorm, etc.). Festal is better for the pancreas and gall bladder, eliminating the consequences of overeating and poor lifestyle. The Festal analogue reduces diarrhea, a feeling of heaviness and fullness. The cost is several times higher.
Causes of chronic pancreatitis
Chronic pancreatitis often develops gradually against the background of chronic cholecystitis, cholelithiasis or under the influence of unsystematic irregular nutrition, frequent consumption of spicy and fatty foods, chronic alcoholism, especially in combination with a systematic deficiency of proteins and vitamins in food, penetration of stomach or duodenal ulcers into the pancreas , atherosclerotic damage to the vessels of the pancreas, infectious diseases (especially with infectious mumps, typhoid and typhus, viral hepatitis), some heminthiasis, chronic intoxication with lead, mercury, phosphorus, arsenic.
Pancreatin or Panzinorm
Manufacturer: KRKA, Slovenia
Release form: capsules
Ingredients: pancreatin
Panzinorm is a Pancreatin substitute in capsules produced in Slovenia. The price of a cheap analogue of Pancreatin depends on the dosage - on average it varies from 140 to 310 rubles. The drug is available to the population and is effective.
Panzinorm is distinguished by its imported manufacturer, release form (capsules), indication of enzyme activity units and the absence of the need for storage in the refrigerator or other special conditions.
Pancreatin or Ermital – which is better according to doctors’ reviews
Manufacturer: Nordix Pharma, Germany
Release form: capsules
Active ingredient: pancreatin
Pancreatin analogue for children Ermital is more effective and safer. It is produced by a German pharmaceutical company in the form of enteric capsules. Another protection against dissolution in the stomach and better action is that the capsule contains microtablets of optimal size, which, after release, are distributed throughout the entire volume of food. It is convenient to divide them if the medicine is to be given to newborns or older children.
According to research, the most effective analogues of Pancreatin are drugs with the same composition in the form of capsules. Their action is 25% faster and stronger, since the component is protected from the effects of gastric juice and begins to act in the intestines. When selecting a substitute, read the instructions, in particular, properties, indications and contraindications.
Introduction
Chronic pancreatitis (CP) is an inflammatory, continuously persistent disease of the pancreas (PG), often associated with pain, which is characterized by the development of irreversible morphological changes in the parenchyma and ductal system of the pancreas and the progressive destruction of organ tissue, leading to disruption of exocrine and endocrine functions [1 , 2].
Several risk factors have been established and/or suspected, but in a small proportion of patients the disease is idiopathic. Clinically, the early phase of the disease is characterized by pain or recurrent exacerbations of pancreatitis and the development of complications, while in the later stages of the disease, symptoms are caused by the appearance of exocrine and/or endocrine insufficiency. Chronic pancreatitis in the late stages is considered a risk factor for the development of pancreatic cancer [3–5], and therefore treatment of CP with conservative, surgical, endoscopic methods, or a combination thereof, can be considered as a putative measure for the prevention of carcinogenesis in the pancreas.
Despite numerous attempts, an ideal system for the etiological classification of CP has not yet been created. An emphasis on the etiology of CP is necessary because it provides an attempt at etiotropic treatment (for example, obstructive pancreatitis) or a more accentuated pathogenetic one when the first option is impossible (for example, treatment with steroids for autoimmune pancreatitis). One of the latest options for systematizing the many etiological factors of CP is the M-ANNHEIM classification of CP risk factors (Multiple, Alcohol, Nicotine, Nutrition, Heredity, Efferent pancreatic duct factors, Immunological factors, Miscellaneous and Metabolic factors) [6].
Alcohol abuse. Alcohol is responsible for 60–70% of cases of CP in the Western world. The dose of daily alcohol consumption at which the risk of developing CP increases has not been established, but according to some estimates, it may be 60–80 ml/day (pure ethanol). Gender, genetic and other factors may play a major role, and as a result, the term “alcoholic pancreatitis” does not necessarily imply chronic alcoholism or the consequences of alcohol abuse. Smoking increases the risk of development and progression of CP [2].
Smoking. The odds ratio for developing CP for smokers compared with non-smokers ranges from 7.8–17.3; The risk increases with the number of cigarettes smoked and the length of smoking. Thus, smoking should be considered an independent risk factor for the development of CP [7, 8].
Nutritional factors. The relationship between protein-energy malnutrition, hypertriglyceridemia, other hyperlipidemias and CP is ambiguous [2].
Hereditary factors. Inherited factors are believed to play a role in hereditary pancreatitis, familial pancreatitis, idiopathic pancreatitis with early and late manifestations, and tropical pancreatitis. Mutations in the coding part of the cationic trypsinogen gene lead to the development of hereditary pancreatitis [9]. In affected individuals, symptoms usually begin before the age of 20 years, and the risk of developing pancreatic adenocarcinoma is markedly increased. Mutations in the coding portion of the cystic fibrosis transmembrane conductance regulatory (CFTR) [10] and trypsin inhibitor (PSTI or SPINK1) [11] gene have been identified in patients with idiopathic CP.
Factors affecting the outflow of pancreatic secretions. Conditions associated with the development of obstructive CP are trauma, the presence of stones, false cysts and tumors. It is not precisely established whether CP occurs against the background of a split pancreas (pancreas divisum) and dysfunction of the sphincter of Oddi [2].
Immunological factors. Autoimmune pancreatitis (AIP) can occur alone or in combination with Sjögren's syndrome, inflammatory bowel disease, and many other autoimmune disorders. Clinically relevant serum findings for the diagnosis of AIP include hypergammaglobulinemia, elevated levels of immunoglobulin G (IgG), especially IgG4, and the presence of certain autoantibodies (antinuclear antibodies, anti-lactoferrin antibodies, anti-carbonic anhydrase type II antibodies, and anti-smooth muscle antibodies) [12]. It is extremely important to identify the etiological form of AIP in patients, since this form of the disease can be treated with corticosteroids.
Other and rare metabolic factors. Chronic renal failure [13] and hyperparathyroidism [14] are established causes of CP, while the exact role of drugs and toxic substances remains completely unproven [2].
Thus, a detailed history is of paramount importance, since its analysis can identify the etiological factor. Particular attention should be paid to occupation, potential exposure to toxic substances, diet, alcohol consumption and smoking. It is appropriate to use validated measures to detect alcohol abuse. Kidney disease and hyperparathyroidism should be considered in the differential diagnosis, and a history of autoimmune disease may indicate the presence of AIP. A thorough family history should be collected, and if a hereditary disease is suspected, genetic counseling is required.