Polyoxidonium
Use the drug only according to the indications, method of administration and in the doses indicated in the instructions.
If there is no improvement after treatment, or symptoms worsen, or new symptoms appear, you should consult your doctor.
Orally and sublingually 20-30 minutes before meals every day, 2 times a day: children over 10 years old and adults - 1 tablet, children from 3 to 10 years old - ½ tablet (6 mg).
If necessary, repeated courses of therapy are possible after 3-4 months. When the drug is re-prescribed, its effectiveness does not decrease.
Recommended treatment regimens
Sublingual:
For treatment in adults:
influenza and acute respiratory infections - 1 tablet 2 times a day for 7 days; inflammatory processes of the oropharynx - 1 tablet 2 times a day for 10 days; exacerbations of chronic diseases of the upper respiratory tract, paranasal sinuses, chronic otitis media - 1 tablet 2 times a day for 10 days; allergic diseases (including hay fever, bronchial asthma), complicated by recurrent bacterial, fungal and viral infections - 1 tablet 2 times a day for 10 days.
For treatment in children aged 3 to 10 years:
influenza and acute respiratory infections – ½ tablet 2 times a day for 7 days; inflammatory processes of the oropharynx – ½ tablet 2 times a day for 7 days; allergic diseases (including hay fever, bronchial asthma), complicated by recurrent bacterial, fungal and viral infections - ½ tablet 2 times a day for 7 days.
For treatment in children over 10 years of age:
influenza and acute respiratory infections - 1 tablet 2 times a day for 7 days; inflammatory processes of the oropharynx - 1 tablet 2 times a day for 7 days; exacerbations of chronic diseases of the upper respiratory tract, paranasal sinuses, chronic otitis media - 1 tablet 2 times a day for 7 days; allergic diseases (including hay fever, bronchial asthma), complicated by recurrent bacterial, fungal and viral infections - 1 tablet 2 times a day for 7 days.
For prevention in adults:
influenza and acute respiratory infections in the pre-epidemic period - 1 tablet per day for 10 days; recurrent herpetic infection of the nasal and labial area - 1 tablet 2 times a day for 10 days; exacerbations of chronic foci of infections of the oropharynx, paranasal sinuses, upper respiratory tract, inner and middle ear - 1 tablet once a day for 10 days; secondary immunodeficiencies arising due to aging or exposure to adverse factors - 1 tablet once a day for 10 days.
For prevention in children aged 3 to 10 years:
influenza and acute respiratory infections in the pre-epidemic period - ½ tablet per day for 7 days; recurrent herpetic infection of the nasal and labial area - ½ tablet 2 times a day for 7 days; exacerbations of chronic foci of infections of the oropharynx, paranasal sinuses, upper respiratory tract, inner and middle ear - ½ tablet once a day for 10 days.
For prevention in children over 10 years of age:
influenza and acute respiratory infections in the pre-epidemic period - 1 tablet per day for 7 days; recurrent herpetic infection of the nasal and labial area - 1 tablet 2 times a day for 7 days; exacerbations of chronic foci of infections of the oropharynx, paranasal sinuses, upper respiratory tract, inner and middle ear, 1 tablet once a day for 10 days.
Orally
For treatment in adults:
diseases of the upper and lower respiratory tract - 1 tablet 2 times 10 days.
For treatment in children over 10 years of age:
diseases of the upper and lower respiratory tract - 1 tablet 2 times 10 days.
Experience of clinical use of Polyoxidonium in complex therapy of respiratory diseases
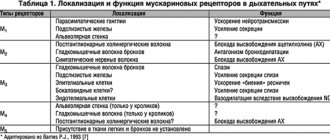
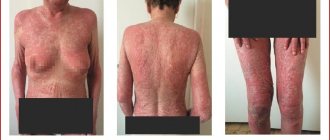
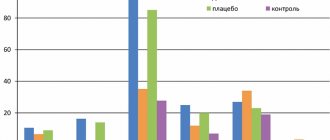
We chose the drug Polyoxidonium as an immunomodulatory agent. Its mechanism of action is based on direct activation of phagocytic cells and natural killer cells, increased interaction between T and B lymphocytes, and activation of antibody formation. At the same time, Polyoxidonium does not affect indicators that are within normal values, does not disrupt the natural mechanisms of inhibition of immune reactions, and does not deplete the reserve capabilities of the hematopoietic system. Polyoxidonium can be prescribed to patients with both identified and undiagnosed disorders of the immune status, based on clinical data. Along with immunomodulatory properties, Polyoxidonium also has detoxification and antioxidant properties, and also activates reparative and regenerative processes. An important feature of Polyoxidonium, which distinguishes it from other immunomodulators, is that it can be used both for the treatment of acute and chronic infectious processes of various etiologies, as well as for atopic diseases. These properties of the drug determined our choice of using it in patients with bronchopulmonary pathology. We used polyoxidonium in addition to complex therapy carried out in accordance with accepted standards of treatment. The study included 89 people. aged from 32 to 68 years, of which 60.7% were men, 39.3% were women. The study group of patients was represented by the following respiratory diseases: chronic obstructive pulmonary disease – 25 people. (28.1%), bronchial asthma – 38 people. (42.7%), bronchiectasis – 24 people. (27%), bronchopulmonary aspergillosis – 2 people. (2.2%). 22 people (35% of patients in the first two groups) fungal superinfection of the bronchi was detected. In 64% of cases, patients, in addition to bronchopulmonary diseases, had concomitant pathology, namely: duodenal ulcer, gastroesophageal reflux disease, intestinal dysbiosis, hypertension, myocardial dystrophy, fungal skin lesions. Methods of administration of Polyoxidonium were determined by the specific clinical situation. Patients received the drug intravenously, 6–12 mg, up to 5 injections per course (23 cases), intramuscularly, 6 mg up to 5–10 injections per course (13 cases), endobronchially, 6–12 mg, 1–2 procedures per course ( 53 cases). In 17 cases there was a combination of different methods of drug administration (intravenous and endobronchial). The endobronchial route of administration is possible due to the fact that Polyoxidonium is highly soluble in saline, quickly distributed in body tissues and does not cause local irritation. Endobronchial administration was carried out in the form of pouring a solution of the drug in a dose of 6 mg into the bronchi, as well as according to the well-known method of introducing 6 mg of Polyoxidonium, dissolved in 3 ml of saline solution into the carina of the trachea. For comparison, we took a group of patients comparable to the study group in terms of size, nosology, severity, age and gender. The dynamics of the patients' condition was assessed according to clinical indicators, data from laboratory, biochemical, radiological, bacteriological, endoscopic, and cytological research methods. The completeness of the therapeutic effect, the time of normalization of parameters, and the tolerability of treatment were compared in patients of the study and control groups. The assessment of the main clinical symptoms of exacerbation of the disease (cough, shortness of breath, volume and character of sputum, the presence of suffocation) was carried out in points (Table 1), by analogy with the criteria proposed by N. Anthonisen (1987). Patients in the study and control groups received standard therapy appropriate to the diagnosis and severity of the disease. The results of therapy were assessed according to the instrumental examination of patients, the severity of clinical symptoms (in points) and the rate of their regression (in days). Statistical data processing was carried out using variation statistics methods. As our observations showed, in the group of patients who received Polyoxidonium as part of complex therapy, there was a more rapid improvement in well-being, increased physical activity, and positive dynamics in the symptoms of the main and concomitant diseases. All patients tolerated the drug administration well. Only in three cases of endobronchial administration were short-term low-grade fever, tachycardia, and a transient increase in blood pressure noted, which we regarded as a general reaction of the body to the procedure; At the same time, bronchospasm was not recorded in any case of observation, with any method of drug administration. Tracking the clinical effects of Polyoxidonium in various nosologies, the following can be noted: the most clear result in our study was obtained when Polyoxidonium was prescribed to patients with exacerbation of bronchiectasis. The number of this group is 24 people, ages from 32 to 65 years, of which 66.7% are men, 33.3% are women. It should be noted that patients in the study and control groups had a long history of the disease, repeated exacerbations, requiring hospital treatment and the use of various antibiotics. Polyoxidonium in the study group of patients was prescribed at a dose of 6–12 mg in the form of intravenous infusions (5 procedures per course) in cases and (or) by endobronchial administration (1–2 procedures per course) in 20 cases; in 7 cases there was a combination of both methods of administration. Changes in the main clinical symptoms were assessed using a scoring system (according to Table 1) before the start of therapy, 1–2 days, 3–5 and 10–12 days from the start of treatment. The results of clinical observation are presented in Figure 1, where the columns of the chart reflect the severity of individual clinical symptoms (in points) in patients in the study group who received Polyoxidonium, and the graphs show the severity of the same symptoms (in points) in patients in the control group who did not receive this drug. As can be seen from the presented graphs and diagrams, patients in the study group experienced a more pronounced and rapid decrease in cough and “purulence” of sputum compared to the control group. The volume of sputum remains significant in the first days of treatment, and by days 10–12 it decreases significantly compared to the control group. Thus, in this case, the positive effects of Polyoxidonium include a faster and more pronounced reduction in the clinical symptoms of inflammation and improvement in bronchial drainage. This pattern was confirmed by the results of laboratory, bacteriological and endoscopic studies. The rapid detoxification effect was also noteworthy, literally from the first procedure of administering the drug. All this made it possible to reduce the dose of antibacterial drugs when carrying out the necessary sanitation of the bronchial tree. The indicated positive effects of Polyoxidonium with varying degrees of severity were observed in 100% of cases in the patients of the study group with bronchiectasis observed by us. The other study group consisted of patients with bronchial asthma (23 women, 15 men) aged from 38 to 60 years, all with polysensitization. The duration of the disease was 10 years or more. Moderate doses of systemic and inhaled glucocorticosteroids were used as basic anti-inflammatory therapy for 8 years or more. In addition, all patients in this group were characterized by a torpid course of the disease, with frequent exacerbations; the majority had side effects of glucocorticoid therapy (Cushingoid syndrome, osteoporosis). In 31.5% of cases, patients had mucosal and cutaneous candidiasis, requiring the addition of antifungal agents to therapy. Polyoxidonium was prescribed at a dose of 6 mg intravenously in 19 cases, intramuscularly in 6 cases, endobronchially (1-2 procedures per course) in 20 cases, in 7 cases there was a combination of different methods of administration. At the same time, no deterioration during the asthmatic process or manifestations of drug intolerance were recorded. In general, we observed a positive effect in 81.6% of cases. In 18.4% there were no significant clinical and functional changes. The dynamics of the main clinical symptoms before treatment and during observation were also assessed using a scoring system (Table 1). The results of clinical observation of the study group are summarized in a graph/diagram presented in Figure 2. Here, the columns of the chart reflect the indicators of the study group, and the graphs reflect the indicators of the control group (in points). As can be seen from Figure 2, with the introduction of Polyoxidonium, a more complete and rapid “effect of inflammation subsidence” is achieved, an increase in sputum production is observed due to improved bronchial drainage, and bronchial patency improves. More objectively, the improvement in bronchial obstruction during treatment is reflected by spirometry indicators (in particular, FEV1) in experimental bronchial asthma patients (who received Polyoxidonium) and control groups (Fig. 3). The rapid subsidence of inflammatory changes and a decrease in the phenomena of bronchial hyperactivity in patients of the study group led to the possibility of reducing the maintenance dose of glucocorticoids, reducing the need for b2-agonists without worsening the patients' condition. In the group of patients with chronic obstructive pulmonary disease who were prescribed Polyoxidonium, there were 25 people, of which 92% were men. This group is represented by patients with moderate and severe disease who have stage II respiratory failure. The disease occurred with frequent exacerbations requiring hospital treatment, with repeated courses of antibacterial, anti-inflammatory and constant bronchodilator therapy. In 40% of cases, the course of the disease was complicated by the addition of fungal superinfection of the bronchi (mucosal candidiasis). These patients, in combination with traditionally used medications, were prescribed Polyoxidonium in the form of intramuscular injections (7 cases), intravenous infusions (8 cases), and endoscopically (13 cases); in 3 cases there was a combined administration of the drug by different routes. To analyze the effectiveness of the drug in a scoring system (Table 1), the main clinical symptoms (cough, volume and character of sputum, shortness of breath and the number of asthma attacks) were assessed before the start and during treatment according to observation days: 1–2, 7–10, 12– 14th days. The results of clinical observations are summarized in graphs/diagrams (Fig. 4, 5). Assessing the results of the study (Fig. 4), it can be noted that when Polyoxidonium is prescribed in patients with COPD, the cough decreases faster and more clearly, literally on the 2-3rd day from the start of therapy the nature of the sputum changes from purulent, mucopurulent to mucous, and the volume of sputum even increases compared to the control group. Thus, the administration of Polyoxidonium leads to improved bronchial drainage, gives a more complete anti-inflammatory effect, leading to the possibility of sanitation of the bronchi without the use of antibiotics or with their short courses. As can be seen from Figure 5, symptoms reflecting respiratory disorders changed little over 12–14 days of observation. Patients in the study group noted an improvement in general well-being, an increase in resistance to habitual physical activity, but the objective functional indicators of spirometry practically remained the same (Fig. 6). In general, in the group of patients with chronic obstructive pulmonary disease, in 92% of observations, the effect of using Polyoxidonium was assessed as positive, of varying degrees of severity. Neither subjective nor objective deterioration in the condition of patients in this group was recorded when using Polyoxidonium. The dependence of the severity of the therapeutic effect of Polyoxidonium on the method of its administration into the body was studied (Table 2). The medicinal properties of the drug, namely anti-inflammatory effect, detoxification effect, enhancing the antimicrobial effect of antibacterial drugs, improving bronchial drainage, and the possibility of reducing the dose of other medications are assessed using a 5-point system: (–) – no effect. (+–) – questionable effect, (+) – significantly positive effect, (++) – significant effect, (+++) – maximally pronounced effect. The results are shown in Table 2. According to our observations, to achieve a clinically significant effect there is no need for long courses of use of the drug. Already with the first administrations of Polyoxidonium, changes in the clinical condition of patients are noted, and with the endobronchial method, 1–2 procedures are sufficient to obtain a significant result. With injection methods, 5–10 procedures per course are sufficient. No side effects were observed with all methods of administration, including in patients with atonic diseases. The speed of onset of the therapeutic effect, the multifunctionality of the effect on the state of the bronchopulmonary system and the body as a whole, the short duration of the course of administration, the absence of side effects when prescribing Polyoxidonium - all this significantly increases the effectiveness of standard therapy and reduces the patient’s time in the hospital (Fig. 7). Thus, the use of Polyoxidonium in the treatment of respiratory diseases is highly effective, expedient and allows optimizing anti-inflammatory treatment regimens for chronic nonspecific lung diseases.
What is Polyoxidonium used for?
The drug is prescribed in complex therapy and independently:
- for respiratory infections, including recurrent ones;
- acute or chronic infectious lesions of internal organs;
- to reduce the side effects of immunosuppressants in rheumatoid arthritis;
- for recovery after a course of potent drugs or operations;
- for fractures, burns, trophic ulcers;
- for the prevention of ARVI during epidemics.
The treatment regimen and dosage form are selected individually depending on the disease and physical condition of each patient.
What is Polyoxidonium used for?
This medicine corrects the body's immune defense against various infectious and systemic lesions. It alleviates physical condition, prevents intoxication by metabolic products, and shortens the acute period of illness. The active substance of Polyoxidonium is azoximer bromide.
The drug is produced in several forms:
- uncoated tablets containing 12 mg of active ingredient: yellow or orange, chamfered;
- suppositories: in a dosage of 6 or 12 mg, yellowish-waxy in color, torpedo-shaped;
- lyophilized powder for the preparation of nasal and parenteral solutions.
Polyoxidonium, 5 pcs., 1ml, 6 mg, solution for injection and topical use
Pills.
Orally
and
sublingually
, 20–30 minutes before meals, daily 1, 2 or 3 times a day.
Adults - in doses of 12 or 24 mg, adolescents - in doses of 12 mg. The method and dosage regimen is determined by the doctor, depending on the diagnosis, severity and severity of the process.
Sublingual:
- for inflammatory processes of the oropharynx (bacterial, viral and fungal in nature):
1 table each 2 times a day every 12 hours, for 10–14 days. For severe forms of herpetic and fungal infections of the oral cavity - 1 table. 3 times a day every 8 hours for 15 days;
- for chronic diseases of the paranasal sinuses and chronic otitis media:
1 table each 2 times a day every 12 hours, for 5–10 days;
- for chronic tonsillitis:
1 table each 3 times a day every 8 hours for 10–15 days;
- for chronic diseases of the upper respiratory tract:
adults - 2 tablets. (24 mg) 2 times a day, adolescents - 1 tablet. (12 mg) 2 times a day, every 12 hours, for 10–14 days;
- for the prevention of influenza and acute respiratory infections:
immunocompromised persons who suffer from acute respiratory infections more than 4 times a year; in the pre-epidemic period, adults - 2 tables. (24 mg), adolescents - 1 tablet. (12 mg) 2 times a day every 12 hours, for 10–15 days.
Orally:
— for chronic diseases of the upper respiratory tract:
adults - 2 tablets. (24 mg) 2 times a day after 12 hours, for adolescents - 1 tablet. (12 mg) 2 times a day, every 12 hours, for 10–14 days.
Lyophilisate for the preparation of solution for injection and topical use
Adults
Parenteral, intranasal
. Methods of application are selected by the doctor depending on the severity of the disease and the age of the patient.
IM or IV (drip):
the drug is prescribed to adults in doses of 6–12 mg 1 time per day, daily, every other day or 1–2 times a week, depending on the diagnosis and severity of the disease.
For intramuscular administration, the contents of the ampoule or bottle are dissolved in 1.5–2 ml of 0.9% sodium chloride solution or water for injection. For intravenous (drip) administration, the drug is dissolved in 2 ml of 0.9% sodium chloride solution, Hemodez-N, Reopoliglucin or 5% dextrose solution, then sterilely transferred into a bottle with the indicated solutions of 200–400 ml.
The prepared solution for parenteral administration cannot be stored.
Intranasally:
a dose of 6 mg is dissolved in 1 ml (20 drops) of distilled water, 0.9% sodium chloride solution or boiled water at room temperature.
Recommended treatment regimens for adults
Parenterally:
- for acute inflammatory diseases:
6 mg daily for 3 days, then every other day with a general course of 5–10 injections;
- for chronic inflammatory diseases:
6 mg every other day for 5 injections, then 2 times a week for a course of at least 10 injections;
- for tuberculosis:
6–12 mg 2 times a week for a course of 10–20 injections;
- in patients with acute and chronic urogenital diseases:
6 mg every other day for a course of 10 injections in combination with chemotherapy;
- for chronic recurrent herpes:
6 mg every other day for a course of 10 injections in combination with antiviral drugs, interferons and/or inducers of interferon synthesis;
- for the treatment of complicated forms of allergic diseases:
6 mg, course of 5 injections - the first 2 injections daily, then every other day. For acute allergic and toxic-allergic conditions, administer 6–12 mg intravenously in combination with other antiallergic drugs;
- for rheumatoid arthritis:
6 mg every other day - 5 injections, then 2 times a week for a course of at least 10 injections.
In cancer patients:
- before and during chemotherapy to reduce the immunosuppressive, hepato- and nephrotoxic effects of chemotherapy drugs - 6-12 mg every other day for a course of at least 10 injections, then the frequency of administration is determined by the doctor depending on the tolerability and duration of chemotherapy and radiation therapy;
— for the prevention of the immunosuppressive effect of the tumor, for the correction of immunodeficiency after chemotherapy and radiation therapy, after surgical removal of the tumor, long-term use of the drug Polyoxidonium® is indicated (from 2-3 months to 1 year) - 6-12 mg 1-2 times a week.
In patients with acute renal failure:
prescribed no more than 2 times a week.
Intranasally
6 mg/day is prescribed for the treatment of acute and chronic infections of the ENT organs, to enhance the regenerative processes of the mucous membranes, to prevent complications and relapses of diseases, to prevent influenza and acute respiratory infections. 3 drops in each nasal passage every 2–3 hours (3 times a day) for 5–10 days.
Children
Parenteral, intranasal, sublingual
. Methods of application are selected by the doctor depending on the diagnosis, severity of the disease, age and body weight of the patient.
Parenterally
the drug is prescribed to children from 6 months at a dose of 3 mg (im or intravenous drip 0.1–0.15 mg/kg) daily, every other day or 2 times a week in a course of 5–10 injections (dose calculation is indicated in the table ).
For intramuscular administration, the drug is dissolved in 1 ml of water for injection or 0.9% sodium chloride solution.
For intravenous drip administration, the drug is dissolved in 1.5–2 ml of a sterile 0.9% solution of sodium chloride, Reopoliglucin, Hemodez-N or 5% dextrose solution, sterilely transferred to a bottle with the indicated solutions with a volume of 150–250 ml.
Intranasal and sublingual:
daily at a daily dose of 0.15 mg/kg for 5–10 days. The drug is administered 1–3 drops into one nasal passage or under the tongue after 2–3 hours. To prepare a solution for intranasal and sublingual use, a dose of 3 mg is dissolved in 1 ml (20 drops), a dose of 6 mg is dissolved in 2 ml of distilled water, 0.9% sodium chloride solution or boiled water at room temperature. One drop of the prepared solution (50 μl) contains 0.15 mg of the drug Polyoxidonium®, which is prescribed per 1 kg of child’s body weight.
Store the solution for sublingual and intranasal use in the refrigerator for no more than 7 days. Before use, the pipette containing the solution must be warmed to room temperature (20–25 °C).
Recommended treatment regimens for children:
- for acute inflammatory diseases:
0.1 mg/kg every other day for a course of 5–7 injections;
- for chronic inflammatory diseases:
0.15 mg/kg 2 times a week for a course of up to 10 injections;
- for acute allergic and toxic-allergic conditions:
IV drip at a dose of 0.15 mg/kg in combination with antiallergic drugs;
— for the treatment of complicated forms of allergic diseases in combination with basic therapy:
IM 0.1 mg/kg in a course of 5 injections with an interval of 1–2 days.
Intranasally
administer 1–3 drops into one nasal passage every 2–3 hours (2–4 times a day). For intranasal and sublingual administration, the calculation of the daily dose for children is presented in the table.
| Child's body weight, kg | Number of drops per day | Volume of injected solution, ml |
| 5 | 5 | 0,25 |
| 10 | 10 | 0,5 |
| 15 | 15 | 0,75 |
| 20 | 20 | 1,0 |
Sublingual:
for all indications - daily at a daily dose of 0.15 mg/kg for 10 days, for the treatment of intestinal dysbiosis for 10-20 days. Place 1-3 drops under the tongue every 2-3 hours.
Suppositories
Rectally
or
vaginally
1 supp.
(6 and 12 mg) 1 time per day. The method and dosage regimen is determined by the doctor depending on the diagnosis, severity and severity of the process. Polyoxidonium® can be used rectally
or
vaginally
daily, every other day or 2 times a week.
Polyoxidonium®, suppositories 12 mg
used in adults rectally or vaginally.
Rectally:
1 time per day, 1 sup. (after bowel cleansing).
Vaginally:
for gynecological diseases, 1 supp. Once a day (at night) it is inserted into the vagina in a lying position.
Polyoxidonium®, suppositories 6 mg
used: in children over 6 years old rectally - 1 supp. 1 time per day (after cleansing the intestines), in adults - rectally (after cleansing the intestines) or vaginally (in the vagina in a lying position) as a maintenance dose - 1 supp. 1 time per day (at night).
Standard scheme
use of Polyoxidonium® - 1 supp. (6 or 12 mg) 1 time per day, daily for 3 days, then every other day with a course of 10–20 supp. If necessary, the course of treatment is repeated after 3–4 months.
For patients receiving long-term immunosuppressive therapy, cancer patients with an acquired defect of the immune system - HIV, who have been exposed to radiation, long-term maintenance therapy with Polyoxidonium® is indicated for 2-3 months to 1 year (adults - 12 mg, children over 6 years - 6 mg 1–2 times a week).
Recommended regimens for use as part of complex therapy:
— for chronic infectious and inflammatory diseases:
in the acute stage - according to the standard regimen, in the remission stage - 1 supp. after 1–2 days, the general course is 10–15 supp.;
— in acute infectious processes and to activate regenerative processes (fractures, burns, trophic ulcers):
1 sup. daily, course of treatment - 10–15 sup.;
- for tuberculosis
: according to the standard regimen, the course of treatment is at least 15 supp., then it is possible to use maintenance therapy - 2 supp. per week for a course of 2–3 months;
— against the background of chemotherapy and radiation therapy of tumors
: 1 sup. daily 2-3 days before the start of therapy, then the frequency of suppository administration is determined by the doctor depending on tolerability and duration of chemotherapy and radiation therapy;
— for rehabilitation of frequent (more than 4–5 times a year) and long-term ill persons and for rheumatoid arthritis
: 1 sup. every other day, course of treatment - 10–15 supp.
— for the correction of secondary immunodeficiencies, incl. arising due to aging
: 1 sup. (12 mg) 2 times a week, course - at least 10 supp. 2–3 times a year.
As monotherapy:
- for seasonal prevention of exacerbations of chronic foci of infection, prevention of recurrent herpes infection
: every other day for adults - 6–12 mg, for children - 6 mg. Course - 10 supp.
— for the correction of secondary immunodeficiencies, prevention of influenza and acute respiratory infections
: according to the standard scheme.
— for gynecological diseases
(rectal or vaginal)
: according to the standard regimen.