Bronchodilators in the treatment of respiratory diseases
In the structure of respiratory diseases, chronic obstructive pulmonary disease (COPD) and bronchial asthma (BA) are the leading causes of morbidity and mortality.
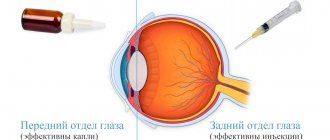
The pathophysiological basis of both nosological forms is bronchial obstruction, the relief or correction of which requires bronchodilator therapy. This provision is enshrined in international and national guidelines for the diagnosis and treatment of BA and COPD [1–6].
It should be noted that asthma and COPD are two independent diseases that have different etiologies, pathogenesis, prognosis, and also require different approaches to treatment. Thus, in particular, ventilation disorders in asthma are characterized by reversible bronchial obstruction and bronchial hyperreactivity, which makes it advisable to use bronchodilators used in this disease. On the contrary, bronchial obstruction in COPD steadily progresses and is only partially reversible. The latter circumstance argues for the feasibility of the clinical use of bronchodilators in this disease.
Naturally, these differences between asthma and COPD require a differentiated approach to both the selection of specific bronchodilators and the tactics of their administration. Thus, if patients with COPD are prescribed bronchodilators mainly on an ongoing basis, then patients with asthma are prescribed more often “on demand” and/or in combination with basic anti-inflammatory therapy (glucocorticosteroids or cromones).
Modern bronchodilators can be divided into three groups, listed below in the order in which they were introduced into clinical practice.
- Anticholinergic (cholinolytic) drugs. By duration of action: short-acting (ipratropium bromide, oxitropium bromide) and long-acting (tiotropium bromide); by route of administration: inhalation only.
- Methylxanthines. By duration of action: short-acting (aminophylline, diaphylline, aminophylline) and long-acting (teopek, theotard, etc.); by route of administration: mainly injection forms - intravenously, intramuscularly (aminophylline, diaphylline) and tablet forms, prolonged theophyllines (micronized forms).
- β2-agonists. By duration of action: short-acting (fenoterol, salbutamol, terbutaline) and long-acting (salbutamol, formoterol); by route of administration: inhalation (short-acting and long-acting β2-agonists), parenteral injection forms, oral tablet forms.
Anticholinergic drugs. For many millennia, traditional medicine has been used to treat respiratory diseases. References to the use of plants of the nightshade family were found in ancient Egyptian papyri. Hippocrates recommended that people with lung diseases use incense and smoke powders prepared from the dried roots and leaves of belladonna (Atropa belladonna), datura (Datura stramonium), and henbane (Hyoscyamus niger). Recent studies have found that the effect of smoking anti-asthmatic cigarettes containing Datura stramonium leaves is comparable to that of modern bronchodilators [7].
By the beginning of the 19th century. The anticholinergic effect of belladonna alkaloids was already known; a little later, scientists established the role of the parasympathetic nervous system in the development of bronchospasm, and since the mid-19th century, cholinergic blockers - atropine and platyphylline, soon synthesized - have become the “gold standard” in the treatment of asthma. The widespread use of anticholinergics for this indication continued until the 70s. XX century Only with the advent of powerful selective β2-agonists, as well as methylxanthines, atropine lost its importance in the treatment of patients with asthma. This was greatly facilitated by the presence of a large number of adverse events accompanying the administration of the drug: dry mouth, impaired mucociliary clearance, mydriasis, etc. [8].
In the 70s XX century Muscarinic receptors in the human respiratory tract were isolated and classified (M1-, M2-, M3 receptors). The establishment of the important role of the parasympathetic nervous system in the control of bronchial patency in asthma gave impetus to further development of anticholinergic drugs, which led to the creation of a fundamentally new drug - ipratropium bromide [8, 9]. However, during clinical trials in patients with asthma, its effectiveness turned out to be low. On the contrary, the drug demonstrated a clear clinical and, in some cases, bronchodilator effect in patients with COPD. Thus, it was possible to prove the partial reversibility of bronchial obstruction in COPD and subsequently establish its two pathophysiological components - reversible and irreversible.
The reversible (“bronchodilator”) component of bronchial obstruction is represented by inflammatory swelling of the mucous membrane of the respiratory tract, accumulation of inflammatory cells, mucus and plasma in the bronchial lumen, spasm of smooth muscles, which are mainly controlled by the parasympathetic part of the autonomic nervous system, the tone of which is naturally increased in COPD [10] .
The irreversible (“emphysematous”) component of bronchial obstruction is caused by the development and progression of pulmonary emphysema and the so-called disease of the small bronchi (decreased elastic traction of the lung tissue due to uneven, predominantly centriacinar emphysema, early expiratory collapse, deformation and narrowing of the small bronchi). It was assumed that these structural changes cannot serve as a point of application for bronchodilators and/or anti-inflammatory drugs. However, later it was possible to establish that it is these changes in the lung parenchyma that cause the formation of hyperinflation of the lungs with the development of an “air trap”, leading to impaired emptying of the alveoli during exhalation (this pathophysiological phenomenon can be most clearly demonstrated when performing physical activity). It is this mechanism that explains the development of such cardiac symptoms of COPD as severe shortness of breath and decreased exercise tolerance, which significantly worsen the quality of life of this category of patients [11].
The most well-known and widely used inhaled anticholinergic drug is currently ipratropium bromide. The drug is well tolerated, effective and safe with long-term use, does not cause the development of tachyphylaxis, and has no cardiotoxic effects. It is important to note that the sensitivity of M-cholinergic receptors does not decrease with age. That is why, in recommendations for the management of patients with COPD, approaches to prescribing this drug are defined as follows: treat “as long as the symptoms of the disease continue to cause inconvenience to the patient” [2].
The duration of action of ipratropium bromide is 4–6 hours, resulting in the need for repeated inhalations (4 times a day), so it is sometimes problematic to control possible deterioration of bronchial obstruction at night or in the early morning hours. Like atropine, ipratropium bromide is not a selective anticholinergic blocker and equally quickly blocks all three types of muscarinic receptors, so the patient should be closely monitored, since blockade of M2 receptors can sometimes lead to paradoxical bronchoconstriction [9].
A representative of the new generation of anticholinergic drugs is tiotropium bromide, registered in Russia in 2003. The peculiarities of the chemical structure of the drug explain the uniqueness of its interaction with muscarinic receptors, namely the unique kinetic selectivity, i.e., differences in the rate of blocking of the corresponding subtypes of muscarinic receptors, as well as increasing the duration of action [12, 13].
In the course of the studies, in particular, it was shown that long-term bronchodilation (~ 24 hours), recorded after a single inhalation of tiotropium bromide, persists even with long-term use (for 12 months) [14, 15]. Already 30 minutes after the first inhalation, the values of forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) increased, and did not subsequently decrease over the next 24 hours. The greatest bronchodilator effect was observed by the second week of treatment with tiotropium bromide.
Long-term therapy with tiotropium bromide (for 12 months) is accompanied by optimization of bronchial obstruction, regression of respiratory symptoms, and improvement in the quality of life of patients [16]. At the same time, the severity of shortness of breath clearly decreased. The famous pulmonologist P. Jones highly appreciated the possibilities of symptomatic control using inhaled tiotropium bromide, noting its sanogenetic effect: patients who took the drug for a long time no longer experienced shortness of breath during exercise and moved at a pace characteristic of their age [17]. Regression of shortness of breath is explained by a decrease in lung hyperinflation and the size of the “air trap”. Moreover, in the long-term treatment of patients with COPD, it was possible to demonstrate the therapeutic superiority of tiotropium bromide over ipratropium bromide [18].
An important advantage of inhaled anticholinergic drugs is the minimal frequency and severity of adverse events. The most common of these is dry mouth, which, as a rule, does not lead to discontinuation of medications [16, 18].
Methylxanthines. For many decades, methylxanthines (theophylline, etc.) have been used in the treatment of patients with asthma, although the mechanism of their action remained unclear for a long time. In 1859, Dr. Hyde Salter reported that a cup of strong coffee could stop an attack of asthma. In 1888, theophylline was isolated from tea leaves. For a long time, the approach to the use of theophylline was purely empirical and only after the mechanism of its action was clarified in the late 1930s. the drug became widespread. The bronchodilator effect of theophylline occurs through inhibition of phosphodiesterase isoforms with a subsequent increase in intracellular cAMP content and relaxation of smooth muscles of the respiratory tract. In addition, the immunomodulatory and anti-inflammatory effects of theophylline have been established, which allows this drug to be prescribed as monotherapy when it is impossible to use inhaled anti-inflammatory and/or bronchodilator drugs. Short-term use of long-acting theophyllines for 6–12 weeks is accompanied by improved indicators of symptomatic control of the disease and an increase in FEV1 [19, 20].
When discussing the possibilities of using theophylline in patients with broncho-obstructive diseases, it is important to take into account its extrapulmonary effects: improvement of peripheral ventilation, reduction of the development of “air traps”, improvement of diaphragm function, especially with hyperinflation of the lung, improvement (restoration) of mucociliary clearance, dilatation of the arteries of the pulmonary circulation, decreased pressure in the pulmonary artery and hemodynamic “unloading” of the right heart, increased physical performance.
At the same time, it is known that the metabolism of theophylline is subject to significant changes. Thus, in smokers, people suffering from chronic alcoholism, patients taking rifampicin or anticonvulsants, theophylline clearance is accelerated, which means that when using a standard dosage regimen, the plasma concentration of the drug may not reach therapeutic levels. On the contrary, with age, in the presence of arterial hypoxemia (PaO2 < 45 mm Hg), respiratory acidosis, in patients with congestive heart failure, liver cirrhosis, carrying a viral infection, taking macrolides (primarily clarithromycin and erythromycin), fluoroquinolones, cimetidine (but not ranitidine), there is a slowdown in the clearance of theophylline, which means that even with a standard dosage regimen there is a risk of creating toxic concentrations of the drug in the blood plasma.
However, the predictability of effects on the plasma concentration of theophylline makes it possible to either avoid them or change the dose (while monitoring the concentration of the drug in the blood). It has also been shown that when theophylline and salmeterol are used together, the “sum” of adverse events is comparable to the frequency of adverse events with monotherapy with each of these drugs [20].
The second no less serious circumstance limiting the widespread use of theophylline is its small therapeutic breadth, which requires determining the concentration of the drug in the blood plasma. It has been established that the optimal concentration of theophylline in blood plasma is 8–15 mg/l. An increase in concentration to 16–20 mg/l is accompanied by a more pronounced bronchodilator effect, but at the same time it is fraught with the development of a large number of adverse events, especially in patients of older age groups [21]. Meanwhile, recent studies have shown that the anti-inflammatory effect of theophylline is more pronounced when low concentrations of the drug are reached (5–10 mg/l) [22].
Currently, theophylline is usually classified as a second-line drug (in relation to anticholinergic blockers and β2-agonists). They represent a kind of reserve for those patients in whom other areas of bronchodilator therapy do not adequately control the symptoms of the disease. It is also possible to prescribe theophylline to those patients who cannot use inhaled delivery devices.
β2-agonists. Currently, it is difficult to imagine therapy for BA and COPD without β2-agonists. However, the history of the use of β-adrenergic receptor stimulants goes back a little over 100 years.
The basis for the first injection of adrenaline (epinephrine) to a patient with asthma was its vasoconstrictor effect, since it was assumed that bronchial obstruction was based on swelling of the mucous membrane of the respiratory tract. Subsequently, adrenaline was widely used to relieve attacks of bronchial obstruction, both parenterally and inhaled. The short duration of action (up to 1–1.5 hours), a large number of undesirable effects of adrenaline, as a non-selective stimulator of α- and β-adrenergic receptors, prompted scientists to search for new drugs [24].
One of them was isoproterenol, synthesized in 1940, a non-selective β-agonist. It was successfully used in inhalation form, allowing patients suffering from asthma to move freely - first with a glass nebulizer, and then (since 1956) with a metered dose aerosol inhaler. Unfortunately, the duration of action of isoproterenol also did not exceed 1.5–2 hours, and frequent inhalations of the drug contributed to the development of adverse events, in particular life-threatening cardiac arrhythmias.
Subsequent studies of the pharmacological properties of isoproterenol revealed the presence of two subtypes of β-adrenergic receptors: β1- and β2-adrenergic receptors, which made it possible to synthesize the first selective β2-agonist salbutamol soon (1970), and a little later - fenoterol and terbutaline [24] .
β2-agonists cause bronchodilation, this occurs primarily as a result of direct stimulation of β2-adrenergic receptors on airway smooth muscle. They are considered as functional antagonists, causing the reverse development of bronchospasm, regardless of the constrictor effect that has taken place. This property of the drugs is especially important since many proinflammatory mediators have a bronchoconstrictor effect.
β2-agonists are characterized by a rapid onset of bronchodilation (within 5 minutes) and a sufficient duration of action (up to 5–6 hours). However, they continue to be short-acting drugs and require repeated inhalations (usually 4 times a day). The drugs are used primarily by inhalation, although there are other dosage forms - injectable, intended to relieve severe exacerbation of asthma, and oral, to prevent/relieve nocturnal attacks of asthma.
In 1990, the first long-acting, highly selective β2-agonist salmeterol was synthesized, and a little later, formoterol. The duration of action of the drugs reached 12 hours, which made it possible to use them 2 times a day and reliably prevent night/pre-dawn attacks of asthma. Despite the same duration of action, there is a difference between these drugs in the timing of the onset of the bronchodilator effect. If salmeterol begins to act within 30–40 minutes, then formoterol is able to stop an attack of bronchial obstruction within 5 minutes after inhalation, similar to short-acting β2-agonists. Numerous studies evaluating the effectiveness of long-acting β2-agonists have shown that these drugs help reduce the frequency of asthma exacerbations, the number of hospitalizations, and also reduce the need for inhaled glucocorticosteroids (ICS) [3].
The long duration of action of salmeterol and formoterol makes it possible to prevent nocturnal attacks of bronchial obstruction. At the same time, monotherapy with long-acting β2-agonists is recommended only for the treatment of COPD [1, 2, 4]. Recent studies have shown that salmeterol and formoterol, like tiotropium bromide, can influence the size of the “air trap”, thereby increasing the exercise tolerance of COPD patients [25].
A study comparing the effectiveness of tiotropium bromide and formoterol [26] showed that tiotropium bromide is more effective on daytime symptoms of COPD, while formoterol improves pulmonary function parameters at night. This fact also indicates that in some cases it is advisable to combine long-acting anticholinergics and β2-agonists.
In the treatment of asthma, long-acting β2-agonists can only be used in combination with ICS [3]. This is also facilitated by the fact that the addition of long-acting β2-agonists is equivalent to doubling the dose of ICS. As a result of the use of a combination of ICS and long-acting β2-agonists, it was possible to reduce the incidence of adverse events that often develop during anti-inflammatory therapy with ICS. This fact gave rise to the creation of such combination drugs as seretide (a combination of salmeterol and fluticasone) and Symbicort turbuhaler (a combination of formoterol and budesonide). These drugs should be used in the treatment of asthma, but their short-term use in the treatment of COPD is also possible [1–5].
It should be noted that β2-agonists, both short-acting and long-acting, are not free from the development of adverse events. Frequent use of short-acting β2-agonists during the day (more than 4-5 times) and/or monotherapy with long-acting β2-agonists in asthma can mask progressive inflammation of the airways, which in the absence of ICS can cause the development of severe exacerbation of asthma.
Particular attention should be paid when prescribing β2-agonists to elderly patients suffering from concomitant diseases of the cardiovascular system. Firstly, with age, the number and sensitivity of β2-adrenergic receptors in the respiratory tract decrease, which causes a decrease in the therapeutic effectiveness of drugs. Secondly, the prescription of even therapeutic doses can aggravate hypokalemia, which naturally develops in the majority of elderly and old people, which, in turn, can lead to the development of severe, often life-threatening cardiac arrhythmias.
Combined bronchodilator therapy. The combination of an inhaled β2-agonist (short-acting or long-acting) and an anticholinergic blocker is accompanied by an improvement in bronchial obstruction to a greater extent than when prescribing either of these drugs as monotherapy [27]. It is possible to optimize the ventilation function of the lungs to an even greater extent with the simultaneous use of β2-agonists, anticholinergic blockers and theophylline [28]. However, according to popular belief, combination therapy should be used only if it is impossible to achieve an optimal therapeutic effect with any one class of bronchodilators.
In accordance with modern recommendations for the management of patients with COPD, in cases of inadequate control of the disease, combination therapy should be used, for example, Berodual (ipratropium bromide + fenoterol). The use of combination drugs promotes better compliance and significantly reduces the cost of treatment compared to the use of each drug separately.
BA is a disease based on inflammation of the airways, accompanied by reversible bronchial obstruction and changes in the sensitivity of the bronchi and manifested by an attack of suffocation, status asthmaticus, or in the absence of such symptoms of respiratory discomfort (paroxysmal cough, distant wheezing and shortness of breath) against the background of a hereditary predisposition to allergic diseases , extrapulmonary signs of allergy, blood and/or sputum eosinophilia.
The use of bronchodilators in patients with asthma due to the presence of transient bronchial obstruction is certainly justified. However, at present, when the leading role of inflammation in the pathogenesis of asthma is recognized, it is advisable to use anti-inflammatory drugs, and primarily ICS, as a basic therapy for the disease. Monotherapy with β2-agonists, as already noted, can mask progressive inflammation and contribute to the development of severe exacerbations of asthma.
According to the modern concept of stepwise therapy for BA, short-acting β2-agonists should be used as monotherapy only in patients with rare attacks (mild intermittent BA that does not require anti-inflammatory therapy) (see Fig. 1, under the heading “Under glass”). It is necessary to pay attention to the fact that if a β2-agonist is taken more than 4 times a day, both to relieve an attack and to prevent it, it is necessary to prescribe anti-inflammatory therapy corresponding to the next stage of treatment.
At stages II, III and IV, the use of short-acting β2-agonists should also not exceed 4 times a day. Thus, the frequency of administration
Short-acting β2-agonists are a marker of control over the symptoms of the disease, i.e., the adequacy of anti-inflammatory therapy.
Long-acting β2-agonists can be used already at the second stage of treatment, especially in patients with nocturnal or early morning asthma attacks/episodes of respiratory discomfort. It is natural to prescribe long-acting drugs at stages III and IV - in order to potentiate the effect of ICS and possibly reduce the dose of the latter.
As for anticholinergics, the role of tiotropium bromide in the treatment of asthma has not yet been determined. Ipratropium bromide, being inferior in the severity of the bronchodilator effect to β2-agonists, can be added to the complex therapy of severe asthma (IV stage) and/or used to relieve a severe asthmatic attack.
COPD is a disease characterized by chronic bronchial obstruction, which is only partially reversible and slowly progresses over the years. Bronchial obstruction naturally leads to the development of shortness of breath during physical activity, an increasing decrease in tolerance to physical activity - all this limits the activity of patients and leads to a sharp decrease in their quality of life [1, 2, 3].
The cornerstone in the treatment of patients with COPD is therapy aimed at reducing bronchial obstruction. For this purpose, short- and long-acting β2-agonists, anticholinergic drugs, and methylxanthines are used [1–6].
When prescribing bronchodilators to patients with COPD, every doctor must answer two key questions: which bronchodilator to choose and how to use the bronchodilator - “on demand” or on a regular basis?
It should be noted that the issues of choosing bronchodilators are not fully defined and are controversial. This is primarily due to the fact that both β2-agonists and anticholinergic drugs are almost equally effective in COPD: they reduce shortness of breath and improve quality of life. Thus, experts from the European Respiratory Society (ERS) recommend either β2-agonists or anticholinergic drugs, without providing clear criteria for choosing between them [6]. On the contrary, the recommendations of the American Thoracic Society (ATS) [6] and the French Pulmonary Society give preference to anticholinergic drugs (as the drugs of choice in patients with persistent symptoms), while β2-agonists are proposed to be used “on demand” in patients with paroxysmal shortness of breath [3 , 4]. Finally, according to experts from the British Thoracic Society (BTS), β2-agonists should be prescribed initially, and anticholinergic drugs should only be used if sympathomimetics are insufficiently effective or if there is a need to “intensify” bronchodilator therapy [5].
It should be noted that anticholinergics are still preferable for the regular treatment of COPD than β2-agonists. This is explained primarily by the fact that the reversible component of bronchial obstruction is controlled by the parasympathetic division of the autonomic nervous system.
In addition, patients with COPD are, as a rule, elderly and senile people, in whom β2-agonists can naturally cause undesirable effects, and the sensitivity of muscarinic receptors remains until old age.
At the same time, short-acting β2-agonists, characterized by an unsurpassed speed of onset of bronchodilator effect, are most suitable for on-demand therapy. If β2-agonists are poorly tolerated or in order to increase the power of the bronchodilator effect to relieve attacks, it is possible to use combination drugs (Berodual). The dose of β2-agonist in this drug is half that of standard inhalers; in this case, the combination of two drugs potentiates the effect of each other.
As for methylxanthines, as already mentioned, they are “second-line” drugs and are prescribed either for intolerance to inhaled drugs for one reason or another, or as an additive drug when β2-agonists, anticholinergics, or their combination are ineffective.
The preference for prescribing one or another bronchodilator is determined after an inhalation test, and the final decision remains with the patient.
In accordance with modern recommendations, the tactics of bronchodilator therapy for patients with COPD can be presented as follows (see Fig. 2, under the heading “Under glass”).
Stage I (mild) COPD involves the prescription of short-acting bronchodilators on demand. At stage II (moderate course), long-acting bronchodilators—tiotropium bromide or β2-agonists—are added to therapy, with the former being preferable (left side of the regimen), while the prescription of long-acting β2-agonists (right side of the regimen) is alternative. At stage III (severe course), it is advisable to combine one of the long-acting β2-agonists and tiotropium bromide. Stage IV is characterized as extremely severe: the course of the disease with frequent exacerbations - and involves, in addition to bronchodilator therapy, the administration of glucocorticosteroids (inhaled and/or oral).
Literature
- Chronic obstructive pulmonary disease: A practical guide for doctors. Federal program. M., 2004.
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. (Based on the April 1998 NHLBI/WHO Workshop). National Institutes of Healt, National Heart. Lung and Blood Institute. April 2001 (Updated 2003).
- Global Strategy for Asthma Management and Prevention. National Institutes of Health, National Heart, Lung, and Blood Institute REVISED 2002 Updated from: NHLBI/WHO Workshop Report: Global Strategy for Asthma Management and Prevention Issued January, 1995. NIH Publication. No. 2.
- Chronic Obstructive Pulmonary Disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax. 2004; 59; 1.
- British Guideline on the Management of Asthma. Thorax. 2003; 58; 1.
- Celli BR, McNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004; 23: 932-936.
- Trechsel K., Bachofen H., Scherre M. Die bronchodilatorische Wirkung der Asthmazigarette. Scweizerische Medizinische Wochenschrift 1973; 103:415-423.
- Gross NJ editor. Anticholinergic therapy in obstructive airway disease. London, Franklin Scientific Publications, 1993.
- Barnes PJ Muscarinic receptor subtypes in airways. Life Sci. 1993; 52:521-527.
- Barnes P. Tiotropium bromide: a new long-acting anticholinergic bronchodilator. In: Barnes P., Buist AS editors. The role of anticholinergics in chronic obstructive pulmonary disease and chronic asthma. Macclesfied Cheshire, UK: Gardiner-Caldwell Communications Limited; 1997; 126-136.
- Calverley HVA Breathlessness during exercise in COPD: how do the drugs work? Thorax. 2004; 59: 45-457.
- Barnes PJ The pharmacological properties of tiotropium. Chest. 2000; 117: 63-69.
- Disse B., Reichl R., Speck G. et al. DF 679 BR, a novel long acting anticholinergic bronchodilator. Life Sci 1993; 52(5-6): 537-544.
- van Noord JA, Bantje TA, Eland ME et al. A randomized controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. The Dutch Tiotropium Study Group. Thorax. 2000; 55: 289-294.
- O`Donnell DE, Fluge F., Gerken F. et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD/ Eur Respir J/ 2004; 23: 832-840.
- Casaburi R., Mahler DA, Jones PW et al. A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002; 19: 217-224.
- P. Personal communication. 10th European Respiratory Society Annual Conference (ERS), Florence, Italy, 30 August-3 September 2000. www.medscape.com/ConferenceSearchAll.ctm/.
- Wincken W., van Noord JA, Greefhorst APM et al. on behalf of the Dutch/Belgian Tiotropium Study Group. Improved health patients with COPD during 1-yr's treatment with tiotropium. Eur Respir J. 2002; 19: 209-216.
- Murciano D. et al. A randomized, controlled trial of theophylline in patients with severe chronic obstructive pulmonary disease. N Engl J Med. 1989; 320: 1521-1525.
- ZuWallak RL, Mahler DA, Reilly D. et al. Salmeterol Plus Theophilline Therapy in the Treatment of COPD. Chest. 2001; 119: 1661-1670.
- Shannon M. Life-threatening events after theophylline overdose: a 10-year-prospective analysis. Arch Intern Med. 1999; 159:989-994.
- Torphy TJ State of the art: Phosphodiesterase isozymes: Molecular targets for novel antiasthma agents. Am J Respir Crit Care Med. 1998; 157: 351-370.
- Tsukino M. et al. Effects of theophylline and ipratropium bromide on exercise performance pulmonary disease. Thorax. 1998; 53: 269-273.
- Lawrence D. R., Benitt P. N. Clinical pharmacology: In 2 vols. M.: Medicine, 1991.
- O`Donnell DE, Voduc N., Fizpatrick M., Webb KA Effect of salmeterol on tye ventilatory response to exercise in chronic obstructive pulmonary disease. Eur Respir J. 2004; 24: 86-94.
- Van Noord JA, Aumann J.-L., Jansens E. et al. Comparison of tiotropium once daily, formoterol twice daily and both combined once daily in patients with COPD. Eur Respir J. 2005; 26: 214-222.
- Van Noord JA et al. Long-term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J. 2000; 15: 878-885.
- Karpel JP et al. A comparison of inhaled ipratropium, oral theophylline plus inhaled beta-agonist, and the combination of all three in patients with COPD. 1994; 105: 1089-1094.
- Tashkin D, Cooper CB The role of long-acting bronchodilators in the management of stable COPD. Chest. 2004; 125: 249-259.
I. L. Klyachkina , Candidate of Medical Sciences, Associate Professor of the State Institute of Internal Medicine of the Ministry of Defense of the Russian Federation, Moscow
Bronchodilator therapy for patients with stable chronic obstructive pulmonary disease
TO
The cornerstone in the treatment of patients with chronic obstructive pulmonary disease (COPD) is therapy aimed at reducing bronchial obstruction. For this purpose, short- and long-acting b2-agonists, anticholinergic drugs, and methylxanthines are used. The position on the leading role of bronchodilator therapy in the complex treatment of patients with COPD is enshrined in both national and international consensus recommendations [1].
However, the criteria for choosing first-line bronchodilators in the clinical situation under discussion remain very uncertain.
, and often contradictory (given the fact that b2-agonists are usually as effective in COPD as anticholinergic drugs). Thus, experts from the European Respiratory Society (ERS) recommend either b2-agonists or anticholinergic drugs without clear criteria for choosing between them [2]. On the contrary, the recommendations of the American Thoracic Society (ATS), the French Pulmonological Society give preference to anticholinergic drugs (as the drugs of choice in patients with persistent symptoms), while b2-agonists are proposed to be used “on demand” in patients with paroxysmal dyspnea [3,4] . Finally, according to experts from the British Thoracic Society (BTS), b2-agonists should be prescribed initially, and anticholinergic drugs should only be used if sympathomimetics are insufficiently effective or if it is necessary to “strengthen” bronchodilator therapy [5].
Until relatively recently (1970–80s), the assumption about the possibility of using bronchodilators for COPD seemed, at least, controversial. Indeed, for many years, COPD was defined as a disease whose key pathophysiological feature was “fixed” or “irreversible” bronchial obstruction, developing as a result of inflammatory-degenerative changes in the airways and lung tissue. The irreversibility of bronchial obstruction has traditionally been considered as a reference point in the algorithm for the differential diagnosis of COPD and bronchial asthma (BA).
The belief in the irreversibility of bronchial obstruction was seriously shaken in the mid-70s of the twentieth century by the results of studies assessing the clinical effectiveness of the anticholinergic drug ipratropium bromide in patients with COPD.
Anticholinergics
First of all, it is obviously worth recalling that anticholinergic drugs (Atropa belladonna, Datura stramonium, etc.) have been used to treat respiratory diseases for several millennia. The anticholinergic effect of belladonna alkaloids, including atropine (daturine), isolated in 1833, was proven at the beginning of the 19th century. Since the mid-19th century, atropine has become the “gold standard” in the treatment of asthma. By the way, it was subsequently found that the effect of smoking cigarettes or inhaling the smoke of burning powder from belladonna leaves was comparable in severity of bronchodilation to modern bronchodilators [6].
However, over time, the use of atropine as a bronchodilator in the treatment of asthma has decreased markedly. On the one hand, this was explained by a significant number of adverse events (dry mouth, mydriasis, etc.), especially with systemic use of the drug. On the other hand, more effective and safe bronchodilator drugs appeared - sympathomimetics (1920s) and, with certain reservations, methylxanthines (1930s).
The renaissance of cholinergic blockers (anticholinergic drugs) occurred in the 1970s, when it was possible to prove the important role of the parasympathetic nervous system in the control of bronchial patency in asthma, as well as to isolate and classify muscarinic receptors (Table 1) [7,8].
As a result of numerous studies, by 1975 a fundamentally new drug was developed -
ipratropium bromide
. During clinical trials of the new drug, it turned out that its bronchodilator effect in asthma is small and is mainly additive to that of b2-agonists. At the same time, an unexpected but pleasant “surprise” was the clear bronchodilator effect of the drug in patients with COPD. Thus, perhaps for the first time, it was possible to demonstrate the reversibility of bronchial obstruction in this category of patients [8].
As a result of further research, two pathophysiological components of bronchial obstruction in COPD were finally established - reversible and irreversible.
Progressive pulmonary emphysema and the so-called small bronchi disease form an irreversible or “emphysematous” component of bronchial obstruction
. These structural changes, naturally, cannot be the point of application of drug therapy.
In turn, the reversible component of bronchial obstruction
develops as a result of processes described by the term “inflammatory remodeling of the bronchial wall” (edema, deposition of proteoglycan in the submucosa and adventitia of the bronchial wall, hypertrophy of the mucous glands and hyperplasia of goblet cells, an increase in the microvascular network of the bronchi, hypertrophy and hyperplasia of bronchial smooth muscle cells).
In this case, inflammatory swelling of the mucous membrane of the respiratory tract and excessive formation of viscous secretions, which significantly worsen the patency of the bronchi, become of particular importance. These processes are controlled by the parasympathetic nervous system, the tone of which is naturally increased in COPD. Stimulation of the vagus nerve branches by inflammatory mediators (eg, bradykinin) leads to the release of acetylcholine, which activates the corresponding muscarinic receptors in the airways (Table 1) [8]. Stimulation of M3 receptors has the greatest pathophysiological “consequences”: contraction of smooth muscle cells, hypersecretion of submucosal glands and goblet cells, swelling of the bronchial mucosa. Parasympathicotonia also causes a certain basal bronchomotor tone, as well as its slight variability.
Anticholinergic drugs (anticholinergic drugs or M-anticholinergics), which are competitive antagonists of acetylcholine, block muscarinic receptors and thereby eliminate the known effects of parasympathicotonia on postsynaptic smooth muscle receptors and mucus-forming elements of the bronchi. M1 receptors are localized in the parasympathetic ganglia and control the process of neurotransmission, and M2 receptors, located at the endings of postganglionic nerve fibers, are autoreceptors and control the release of acetylcholine into the synaptic cleft. In this regard, pharmacological blockade of M2 receptors leads to the release of significant amounts of acetylcholine and a possible worsening of bronchial obstruction.
The pathophysiological “contribution” of contraction of smooth muscles of the respiratory tract to the formation of bronchial obstruction in COPD turned out to be less certain. In the works of MS Dunnil et al., A. Nagai et al. [9,10] it has been shown that in COPD hyperplasia of airway smooth muscle occurs, although less pronounced than in asthma. in vitro studies
a clear relaxation of smooth muscle cells was found, the same in both asthmatics and those without asthma [11]. At the same time, when prescribing bronchodilators to patients with COPD, only restriction (“limiting”) of the shortening of bronchial smooth muscles occurs. This once again proves that bronchoconstriction itself has limited significance in the formation of bronchial obstruction in COPD.
Important for explaining the role and place of anticholinergic blockers in the treatment of COPD (and the disease mainly affects people in older age groups) is the fact that the sensitivity of muscarinic receptors does not decrease with age.
All of the above explains the current recognition of anticholinergic drugs as the drugs of choice in the treatment of COPD. Drugs in this group can be prescribed “on demand”, i.e. to relieve acute respiratory symptoms. However, their use on a regular basis is more justified, since anticholinergic drugs, acting on the reversible component of chronic bronchial obstruction, slow down the rate of progression of ventilation disorders and improve the quality of life of patients.
The most well-known and currently widely used inhaled anticholinergic drug is ipratropium bromide (IB).
. The drug is well tolerated, effective and safe with long-term use, does not cause the development of tachyphylaxis, and has no cardiotoxic effects. At the same time, it is important to recall once again that the sensitivity of M-cholinergic receptors does not decrease with age. That is why existing recommendations for the management of patients with COPD define approaches to prescribing IB as follows: treat “... as long as the symptoms of the disease continue to cause inconvenience to the patient” [3].
At the same time, information security is not free from known shortcomings. First of all, it has a short duration of action (4–6 hours), which results in the need for repeated inhalations (4 times a day), and the drug does not allow adequate control of possible deterioration of bronchial obstruction at night or in the early morning hours. In addition, like atropine, IB is not a selective anticholinergic blocker and dissociates equally quickly from all three types of muscarinic receptors. In this case, blockade of M2 receptors, as mentioned above, can lead to paradoxical bronchoconstriction [7].
A representative of a new generation of anticholinergic drugs is tiotropium bromide (TB)
.
The peculiarities of the chemical structure of TB explain the uniqueness of its interaction with muscarinic receptors, namely, its unique kinetic selectivity, i.e. differences in the rate of dissociation with the corresponding receptors (Table 2), as well as an increased duration of action [12,13]. In the course of the studies, in particular, it was shown that long-term bronchodilation (~ 24 hours), recorded after a single inhalation of TB, persists even after long-term use for 12 months [14,15,16].
Long-term TB therapy (for 12 months) is accompanied by optimization of bronchial obstruction, regression of respiratory symptoms, and improvement in the quality of life of patients [17]. At the same time, it was possible to demonstrate the therapeutic superiority of TB over IB in the long-term treatment of patients with COPD [18]. An important advantage of inhaled anticholinergic drugs is the minimal frequency and severity of adverse events. The most relevant of them is that dry mouth, as a rule, does not lead to discontinuation of medications [15,17,18].
b2-agonists
Along with anticholinergic drugs, b2-agonists, short-acting and long-acting, are also widely used for COPD.
The action of b2-agonists (stimulants of b2-adrenergic receptors) is mediated through an increase in the intracellular concentration of cAMP, which leads to a variety of biological and therapeutic effects (including relaxation of the smooth muscles of the respiratory tract and improvement of bronchial patency). The question of the therapeutic comparability of b2-agonists and anticholinergic drugs in COPD has been discussed for a long time, and the choice between these groups of drugs was (and is) often made empirically. However, it is currently proposed to choose one or another direction of bronchodilator therapy, taking into account the individual sensitivity of the patient (based on the results of the inhalation test).
Short-acting b2 agonists
can be used “on demand”, i.e. to relieve symptoms and on a regular basis. According to the results of a meta-analysis conducted by P. Sestini et al. [19], regular use of short-acting b2-agonists for 1–8 weeks leads to a slight increase in FEV1 (~ 0.14 L) and also reduces the severity of shortness of breath compared to placebo. However, the data do not provide clear evidence of a therapeutic superiority of regular use of inhaled b2-agonists compared with their on-demand use.
A retrospective analysis of studies devoted to the optimization of bronchodilator therapy for patients with COPD showed that the least number of exacerbations of the disease is observed with combination treatment (salbutamol + IB) compared with monotherapy with a b2-agonist or anticholinergic blocker [20].
The emergence of long-acting b2-agonists
(salmeterol, formoterol) has renewed the debate about the advantages of sympathomimetics over anticholinergic drugs. However, the results of the first controlled studies assessing the effectiveness of short-term administration (4–16 weeks) of the long-acting β2-agonist salmeterol in patients with stable COPD indicated a modest superiority of the bronchodilator over placebo (the increase in FEV1 was ~ 0.1 L) [21].
More recent studies have shown that long-term use of salmeterol is accompanied by a more pronounced bronchodilator effect [22], minimization of clinical symptoms [23], improvement in the quality of life of patients with COPD [24], and prolongation of the time interval from the moment the drug is prescribed to the development of the first exacerbation of the disease [ 25].
At the same time, in comparative studies - salmeterol vs
.
IB [26] and
formoterol vs. IB [27] – comparable therapeutic efficacy (regression of shortness of breath, increase in FEV1) of both directions of therapy was demonstrated.
Despite the limited pathogenetic contribution of bronchoconstriction to obstruction of the airways in patients with COPD and, accordingly, the insignificant effect of b2-agonists on the tone of bronchial smooth muscle cells, their use in the clinical situation under discussion has become almost textbook. Almost all researchers note a significant improvement in the condition of patients, regression of symptoms (especially in the morning), a decrease in the number of severe exacerbations and hospitalizations, which often do not correlate with the dynamics of FEV1.
In this regard, it should be noted that b2-agonists, in addition to their bronchodilator effect, also have other sanogenetic effects. The explanation for the latter should be sought primarily in the widespread localization of b2-adrenergic receptors not only in the smooth muscle cells of the bronchi, but also in skeletal muscles, myocardium, vascular wall, etc. And hence the multiplicity of therapeutic effects of b2-agonists: stimulation of the beating of the cilia of the ciliated epithelium of the bronchial mucosa and improvement of mucociliary clearance; increasing the strength and endurance of the respiratory muscles, incl. and diaphragm; increased myocardial contractility, decreased vascular resistance, decreased hemodynamic load on the heart and, as a consequence, increased physical performance [28].
Methylxanthines
For several decades, methylxanthines (theophylline, etc.) have been used in the treatment of asthma. Bronchodilator effect of theophylline (TF)
is carried out through inhibition of phosphodiesterase (blockade of phosphodiesterase receptors, mainly types III and IV) with a subsequent increase in the intracellular content of cAMP and relaxation of the smooth muscles of the respiratory tract. Recently, it has become known that type IV phosphodiesterase receptors are also localized on the surface of “inflammatory cells” (eosinophils, neutrophils, etc.), which explains the immunomodulatory and anti-inflammatory effects of TF.
The bronchodilator effect of TF is clearly manifested in the treatment of patients with COPD. Thus, in particular, short-term administration (6–12 weeks) of long-acting theophylline is accompanied by improved symptomatic control of the disease, especially in the morning, and an increase in FEV1 [29,30].
When discussing the possibilities of using TF in patients with COPD, one cannot ignore its extrapulmonary effects:
improvement of peripheral ventilation; reducing the development of “air traps”; improvement of diaphragm function, especially with hyperinflation of the lung; improvement (restoration) of mucociliary clearance; dilation of the arteries of the pulmonary circulation, decreased pressure in the pulmonary artery and hemodynamic “unloading” of the right heart, increased physical performance.
However, despite these and other evidence of the “therapeutic attractiveness” of TF, the role and place of the drug in the treatment of COPD has not yet been fully determined. This is partly due to the fact that TF metabolism is subject to significant changes. Thus, in smokers, people suffering from chronic alcoholism, patients taking rifampicin or anticonvulsants, the clearance of TF is accelerated, which means that when using a standard dosage regimen, the plasma concentration of the drug may not reach the therapeutic level. On the contrary, with age, in the presence of arterial hypoxemia (PaO2 < 45 mm Hg), respiratory acidosis, in patients with congestive heart failure, cirrhosis of the liver, carrying a viral infection, taking macrolides (primarily clarithromycin and erythromycin), fluoroquinolones, cimetidine (but not ranitidine), there is a slowdown in the clearance of TF, which means that even with a standard dosage regimen there is a risk of toxic concentrations of the drug appearing in the blood plasma.
However, the predictability of the effects on the plasma concentration of TF makes it possible to either avoid them or change the dose (while monitoring the concentration of the drug in the blood). It was also shown that when TF and salmeterol were used together, the amount of adverse events was comparable to the frequency of adverse events with monotherapy with each of them [31].
The second no less serious circumstance limiting the widespread use of TF is its small therapeutic latitude (proximity of therapeutic and toxic concentrations), which requires determining the concentration of the drug in the blood plasma. It has been established that the optimal concentration of TF in blood plasma is 8–15 mg/l. An increase in concentration to 16–20 mg/l is accompanied by a more pronounced bronchodilator effect, but at the same time it is fraught with a large number of adverse events, especially in patients of older age groups [32]. Meanwhile, recent studies have shown that the anti-inflammatory effect of TF is more pronounced when low drug concentrations are reached (5–10 mg/l) [33].
Currently, TF is usually classified as a second-line drug.
(i.e. after anticholinergics and b2-agonists), a kind of reserve for those patients in whom other areas of bronchodilator therapy do not adequately control the symptoms of the disease. It is also possible to prescribe TF to those patients who cannot use inhalation delivery devices.
Combined bronchodilator therapy
The combination of an inhaled b2-agonist (short-acting or long-acting) and an anticholinergic blocker is accompanied by an improvement in bronchial obstruction to a greater extent than when prescribing any of these drugs as monotherapy [34–37]. It is possible to optimize the ventilation function of the lungs to an even greater extent with the simultaneous use of b2-agonists, anticholinergic blockers and TF [38]. However, according to popular opinion, combination therapy should be used, as a rule, only if it is impossible to achieve an optimal therapeutic effect when prescribing any one class of bronchodilators.
In accordance with modern recommendations for the management of patients with COPD, in cases of inadequate control of the disease, combination therapy should be resorted to: Combivent
(IB + salbutamol) or
Berodual
(IB + fenoterol). The use of combination drugs promotes better compliance and significantly reduces the cost of treatment compared to using each drug separately.
Inhaled glucocorticoids
Currently, inhaled glucocorticoids (IGCs) deserve special attention in the treatment of COPD, taking into account the possible modification of bronchial patency when prescribed. Based on the recognition of the leading role of inflammation in the pathogenesis of bronchial obstruction in COPD ( "Chronic obstructive pulmonary disease is a disease characterized by partially irreversible airflow limitation. Airflow limitation, as a rule, has a steadily progressive nature and is caused by an abnormal inflammatory response of the lung tissue to irritation by various pathogens particles and gases" [1]
), it would be realistic to assume that the administration of anti-inflammatory drugs would lead to improved symptomatic and functional control of the disease.
Despite the fact that chronic inflammation plays a major role in the origin of COPD and asthma, the specific cellular and molecular mechanisms of inflammation in these diseases are different. Thus, in BA, the cytogram of inflammation of the bronchial mucosa is represented predominantly by eosinophilic leukocytes and CD4+ lymphocytes, and in cases of COPD, the dominant inflammatory cells are neutrophils, macrophages and CD8+ lymphocytes [39]. Hence the significant differences in response to treatment in asthma and COPD. Eosinophil cell inflammation is effectively controlled by glucocorticoids. On the contrary, these drugs have virtually no effect on the severity of neutrophil cell inflammation and the production of known inflammatory mediators and proteases by neutrophils. Moreover, in relation to eosinophilic and neutrophilic leukocytes, glucocorticoids demonstrate exactly the opposite effects - apoptosis of eosinophils and prolongation of neutrophil life.
All this explains the inconsistency of the results obtained during short-term use of IGCs in patients with COPD (including the dynamics of FEV1). Hence the well-known discrepancies in the interpretation of the role and place of IGK. Thus, according to the results of studies conducted in France, practitioners prescribe IGCs to patients with COPD in 76% of cases [40], which is comparable to the frequency of their prescription in the UK [3,41]. At the same time, the testimony that argued for this “therapeutic maximalism” was confirmed only in 10–30% of cases [1,5,40].
In turn, large-scale multicenter controlled studies (Copenhagen City Lung Study, EUROSCOP, ISOLDE, Lung Health Study II), aimed at assessing the clinical and functional effectiveness of long-term use of IGCs, yielded unexpected results (Table 3) [42]. Thus, it was shown that during the first 6 months, FEV1 values in COPD patients taking IGCs increased slightly, but by the end of the third year, bronchial patency indicators were comparable to those in groups of patients receiving placebo. However, it was found that long-term use of IGCs is accompanied by a reduction in the number of severe and moderate exacerbations of COPD by 25%
[43].
Currently, it is considered advisable to use IGCs only in patients with symptomatic COPD and positive results of the “inhalation test” ( The inhalation test is the administration of IGCs for 6 weeks - 3 months, and it is considered positive when FEV1 increases by 200 ml or more or by 15% or more compared to baseline values. In this case, FEV1 is determined 30-45 minutes after inhalation of the corresponding bronchodilator(s). It should be emphasized that monotherapy with IGCs in patients with COPD is unacceptable, and these drugs are prescribed in conjunction with bronchodilator therapy [1] .
), as well as with severe disturbances of bronchial obstruction (FEV1<50%) and repeated exacerbations of the disease, requiring the prescription of antibiotics and/or systemic glucocorticoids.
Long-term use of systemic glucocorticoids (> 2 weeks) in patients with stable COPD is not recommended due to the high risk of adverse events.
In conclusion, when characterizing bronchodilator therapy for patients with stable COPD, it is advisable to refer to the well-known provisions of the GOLD initiative [1]:
- Bronchodilators are central to the symptomatic treatment of COPD.
- Inhalation therapy is preferred.
- The choice of drug between b2-agonists, anticholinergics, theophylline, or a combination of these drugs depends on the availability and individual response to treatment in the form of relief of symptoms and absence of side effects.
- Bronchodilators are prescribed as needed or regularly to prevent or reduce the severity of symptoms.
- Long-acting bronchodilators are more suitable for regular use.
- Combination bronchodilators may increase effectiveness and reduce the risk of side effects compared with increasing the dose of a single drug.
- Currently, none of the areas of bronchodilator therapy is able to interrupt the progressive decline in bronchial patency (we can, obviously, only slow down the rate of this progression, when rational bronchodilator therapy “accompanies” the elimination of known risk factors for COPD).
- Unlike bronchial asthma, as adequate control of which is achieved in most patients it is possible to minimize therapy (“step down”), with COPD, taking into account the progressive course of the disease, over time we can only talk about intensifying treatment (“step up”) - picture 1.
Rice.
1. Modern approaches to the management of patients with COPD Literature:
1. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. NHLBI/WHO Workshop Report. Publication 2701, 2001.2. Siafakas NM, Vermeire P, Pride NB, et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). Eur Respir J 1995; 8:1398–1420.
3. American Thoracic Society. Standards for the diagnosis and care with chronic obstructive pulmonary disease. Am Rev Respir Dis 1995; 152:S77–S120.
4. Societe de Pneumologie de Langue de Francaise. Recommandations pour la price en charge des bronchopneumopaties chroniques obstructives. Comite d'organisation: Huchon G., Fournier M., Lebas FX, Pujet JC, Roche N. Rev Mal Respir 1997; 14:2S3–2S92.
5. The COPD Guidelines Group of the Standards of Care Committee of the BTS. BTS Guidelines for the management of chronic obstructive pulmonary disease. Thorax 1997; 52:S1–S28.
6. Trechsel K., Bachofen H., Scherre M. Die bronchodilatorische Wirkung der Asthmazigarette. Scweizerische Medizinische Wochenschrift 1973; 103:415–423.
7. Barnes PJ Muscarinic receptor subtypes in airways. Life Sci 1993; 52:521–527.
8. Gross NJ, editor. Anticholinergic therapy in obstructive airway disease. London, Franklin Scientific Publications, 1993.
9. Dunnil MS, Massarella GR, Anderson JA A comparison of the quantitative anatomy of the bronchi in normal subjects, in the status of asthmaticus in chronic bronchitis and in emphysema. Thorax 1969; 24: 176–179.
10. Nagai A., West WW, Paul JB, Thurbeck WM The National Institutes of Health intermittent positive–pressure breathing trial: pathology studies. Am Rev Respir Dis 1985; 132:937–945.
11. James A., Carroll N. Airway smooth muzcle in health and disease; methods of measurement and relation to function. Eur Respir J 2000; 15: 782–789.
12. Barnes PJ The pharmacological properties of tiotropium. Chest 2000; 117 suppl.: 63S–69S.
13. Disse B., Reichl R., Speck G., et al. DF 679 BR, a novel long acting anticholinergic bronchodilator. Life Sci 1993; 52(5–6): 537–544.
14. van Noord JA, Bantje TA, Eland ME et al. A randomized controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. The Dutch Tiotropium Study Group. Thorax 2000; 55:289–294.
15. Casaburi R, Briggs DD, Donohue JF et al. The spirometric efficacy of once–daily dosing with tiotropium in stable COPD. Chest 2000; 118:1294–1302.
16. Littner MR, Ilovite JS, Tashkin DP et al. Long-acting bronchodilation with once-daily dosing of tiotropium (Spiriva) in stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000; 161:1136–1142.
17. Casaburi R., Mahler DA, Jones PW et al. A long–term evaluation of once–daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J 2002; 19: 217–224.
18. Wincken W, van Noord JA, Greefhorst APM, et al. on behalf of the Dutch/Belgian Tiotropium Study Group. Improved health patients with COPD during 1–yr's treatment with tiotropium. Eur Respir J 2002; 19: 209–216.
19. Sestini P. et al. Short-acting ?2-agonists for stable COPD (Cochran Review). In: The Cochran Library. Issue 4, 2001. Oxford Update Software.
20. Friedman M, Serby CW, Menjoge SS et al. Pharmacoeconomic evaluation of a combination of ipratropium plus albuterol compared with ipratropium alone and albuterol alone in COPD. Chest 1999; 115:635–641.
21. Appleton S., Smith B., Veale A., Bara A. Longacting beta2-agonists for chronic obstructive pulmonary disease. (Cochran Review). In: The Cochran Library. Issue 4, 2001. Oxford Update Software.
22. van Noord JA, de Munck DR, Bantje TA et al. long–term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000; 15:878–885.
23. Ramirez-Venegas A., Ward J., Lentine T. Et al. Salmeterol reduces dyspnoea and improves lung function in patients with COPD. Chest 1997; 112:335–340.
24. Jones PW, Bush TK Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283–1289.
25. D'Urzo AD, De Salvo MC, Ramirez–Rivera A. et al. In patients with COPD, treatment with a combination of formoterol and ipratropium is more effective than a combination of salbutamol and ipratropium: a 3–week, randomized, double–blind, within–patient, multicenter study. Chest 2001; 119:1347–1356.
26. Mahler DA et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest 1999; 115:957–965.
27. Dahl R. et al. Inhaled formoterol dry powder versus ipratropium bromide in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001; 164:778–784
28. Jonson M., Rennard S. Alternative mechanisms for long-acting α2-adrenergic agonists in COPD. Chest 2001; 120: 258–270.
29. Murciano D. et al. A randomized, controlled trial of theophylline in patients with severe chronic obstructive pulmonary disease. N Engl J Med 1989; 320:1521–1525.
30. Tsukino M. et al. Effects of theophylline and ipratropium bromide on exercise performance pulmonary disease. Thorax 1998; 53:269–273.
31. ZuWallak RL, Mahler DA, Reilly D., et al. Salmeterol Plus Nheophilline Therapy in the Treatment of COPD. Chest. 2001; 119:1661–1670.
32. Shannon M. Life-threatening events after theophylline overdose: a 10-year-prispective analysis. Arch Intern Med 1999; 159:989–994.
33. Torphy TJ State of the art: Phosphodiesterase isozymes: Molecular targets for novel antiasthma agents. Am J Respir Crit Care Med 1998; 157:351–370.
34. COMBIVENT Inhalation Aerosol Study Group. In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85–day multicenter trial. Chest 1994; 105:1411–1419.
35. Ikeda A. et al. bronchodilating effects of combined therapy of ipratropium bromide and salbutamol for stable COPD: comparison with ipratropium bromide alone. Chest 1995; 107:401–405.
36. Wesseling G. et al. A comparison of the effects of anticholinergic and beta-2-agonist and combination therapy on respiratory impedance in COPD. Chest 1992; 101:166–173.
37. van Noord JA et al. long–term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000; 15:878–885.
38. Karpel JP et al. a comparison of inhaled ipratropium, oral theophylline plus inhaled beta–agonist, and the combination of all three in patients with COPD 1994; 105:1089–1094.
39. Barnes P. Mechanisms in COPD. Differences From Asthma. Chest 2000; 117:10S–14S.
40. Roche N., Lepage T., Bourcereau J., Terriox P. Guidelines versus clinical practice in the treatment of chronic obstructive pulmonary disease. Eur Respir J 2001; 18:903–908.
41. Siafakas NM, Vermeire P, Pride NB, et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). Eur Respir J 1995; 8:1398–1420.
42. Lazarus S. Update on Chronic Obstructive Pulmonary Disease. 96th International Conference of the American Thoracic Society, May 2000. https://www.medscape.com/medscape/cno/ConferenceSearchAll.cfm
43. Paggiaro PL et al. Multicentre randomized placebo–controlled trial of inhaled fluticasone propionate in patients with chronic obstructive pulmonary disease. Lancet 1998; 351:773–780.
Mucolytic and bronchodilator drugs in the treatment of bronchial obstruction during ARVI in children
In children with acute respiratory viral infections, the lower respiratory tract is often involved in the pathological process with the development of obstructive syndrome. The use of the combined drug Ascoril expectorant (bromhexine + salbutamol + guaifenesin), due to its combined bronchodilator and mucolytic action, leads to a rapid regression of the symptoms of the disease, preventing its transition to a more severe long-term course, and subsequently reduces the need for antibiotics. The clinical effectiveness and high safety profile of Ascoril expectorant allow us to recommend it as the drug of choice in children over 2 years of age with mild to moderate bronchial obstruction due to ARVI.
Rice. 1. Dynamics of symptoms of night cough in children during therapy with a combination drug (bromhexine + salbutamol + guaifenesin), compared with monotherapy with a mucolytic (bromhexine)
Rice. 2. Dynamics of symptoms of daytime cough in children during therapy with a combination drug (bromhexine + salbutamol + guaifenesin), compared with monotherapy with a mucolytic (bromhexine)
Rice. 3. The effectiveness of therapy with a combination drug (bromhexine + salbutamol + guaifenesin) in comparison with monotherapy with a mucolytic (bromhexine) according to the total symptom score, M ± m
Acute respiratory viral infections (ARVI) account for more than half of all acute infectious diseases in children, and during periods of epidemics the share of ARVI increases to 80–90%. The highest incidence rates of ARVI are observed in preschool children. Young children suffer from acute respiratory viral infections on average 3–4 times a year, while 30–40% of children in this age category suffer at least 6–8 acute respiratory viral infections per year. Children who begin to attend preschool institutions suffer from acute respiratory viral infections 1.5 times more often in the first year than their peers at home. The frequency of ARVI decreases with age, so schoolchildren suffer on average 2-3 ARVI per year.
ARVI is registered throughout the year, but the greatest number of diseases occurs from early autumn to late spring.
In children with respiratory diseases, especially at an early age, the lower respiratory tract is often involved in the pathological process with the development of obstructive syndrome (OS). There are several phenotypes of bronchial obstruction that have both clinical and prognostic significance. Transient obstruction is observed in children only in the first three years of life, persistent obstruction is observed mainly in the first 6 years of life. OS can develop in children after three years of life (late onset). In this case, atopic and non-atopic phenotypes of obstructive syndrome are distinguished, that is, OS in combination with and without atopy. Information obtained from long-term observation shows that in children with transient obstruction, pulmonary function is altered from birth, even before the first episode of obstruction. On the contrary, children with persistent obstruction and a high risk of developing bronchial asthma (BA) have normal lung function at birth, and obstructive disorders develop by the age of 4–6 years. Probably one of the significant factors predisposing to virus-induced obstructive symptoms in the first years of life is a decrease in airway lumen due to impaired fetal development in the antenatal period.
Obstructive pulmonary disease in preterm infants is usually associated with a combination of pulmonary immaturity, oxygen therapy, and ventilatory support. This primarily concerns children with low birth weight and severe neonatal respiratory disease. However, even in premature infants with an initial absence of diseases of the neonatal period, when examined at a later age, reduced respiratory function is diagnosed. It has been suggested that in prematurity, infants may be prone to an obstructive pattern. Testing of healthy premature babies in the second year of life shows that their lung function does not normalize during the period of greatest lung growth. The mechanism of persistent decline in pulmonary function in children born prematurely is not determined. This process may be the result of a narrower airway lumen and decreased elasticity of the lung tissue, which secondarily leads to changes in the alveolarization of the lung parenchyma.
Early respiratory viral infections may be a more important risk factor for bronchial obstruction than atopy. In the autumn-winter period, severe cases of bronchiolitis in children of the first two years of life are often caused by respiratory syncytial virus (RSV) and are of a typical seasonal nature. It has been established that severe bronchiolitis in 30–40% of cases is combined with the likelihood of developing asthma. RSV, when combined with human bocavirus, causes a more severe course of the disease.
The second most common etiological factor for bronchiolitis is rhinovirus (RV). In moderate to severe cases, it increases the risk of developing asthma. It should be noted: many other viral infections - influenza, parainfluenza, coronavirus infection, enterovirus, adenovirus, as well as infections caused by human metapneumovirus and bocavirus - affecting small bronchi and bronchioles, occur with the clinic of bronchiolitis. In newborns at risk of atopy, it has been shown that moderate/severe obstruction in RV disease is a more significant risk factor not only for the development of repeated episodes of obstruction by 3 years, but also the development of asthma by 6 years. Data from a number of studies have shown that the leading risk factors for recurrent bronchial obstruction after acute bronchiolitis were RV infection and a family history of asthma. Children with RV infection who received oral corticosteroid therapy were significantly less likely to develop subsequent recurrent obstruction. A study of the balance between Th1 and Th2 types of immune response showed that in children with atopy, peripheral mononuclear cells incubated with the RV virus produce interleukin-10 (IL-10), while in patients without atopy - gamma interferon and IL -12. The reduced ability of blood mononuclear cells to produce interferon gamma and IL-12 reduces viral clearance and may lead to asthma exacerbation by promoting Th2 inflammation and a deficiency of the Th1 antiviral immune response. It is currently debated whether recurrent airway infection leads to damage and thus to asthma or whether children are predisposed to asthma because they have altered interferon levels or a different cytokine response.
For a better understanding of postnatal processes, information about the antenatal period of development is important. Branching of the respiratory tract occurs in the first half of pregnancy, therefore, the characteristics of the antenatal period can affect their caliber. The ADAM33 gene plays an important role in antenatal lung development, especially in the morphogenesis of airway branching at 3–5 years of age. This gene also determines the size of the airways.
A combination of atopy in the mother with deterioration of pulmonary function in newborns has been noted, but the mechanism of this process has not been studied. Children born to mothers with preeclampsia, hypertension, and diabetes have an increased risk of developing early transient, persistent, and later obstruction. Prescription of antibiotics during labor can cause both early transient and persistent obstruction.
Maternal smoking has a direct negative effect on fetal lung development, as it leads to a decrease in IL-4 and interferon gamma and increases the proliferation of mononuclear cells in umbilical cord blood on house dust. Other studies of cord blood cells show that maternal smoking is associated with increased IL-13 and decreased interferon-gamma mRNA response after stimulation, as well as TNF-alpha production. Epidemiological studies have confirmed that maternal smoking and atopy are combined with subsequent bronchiolitis in children in the first year of life. Thus, maternal smoking significantly affects the nature of the immune response in newborns, as well as the anatomical features of the structure of the lower respiratory tract (underdevelopment of the alveoli).
RSV bronchiolitis is combined with an increase in the expression of Th2-pattern cytokines or a decrease in Th1. This makes the hypothesis that RSV causes asthma attractive. Bronchial hyperreactivity after bronchiolitis persists for a long time, this may explain the predisposition to bronchial obstruction in later life. However, the discovery of specific RSV IgE in children with bronchiolitis suggests that the result of early RSV infection in some patients may be a Th2-type immune response that predisposes these children to the development of asthma.
Genetic studies have established that polymorphism of the IL-8, IL-10 genes and toll-like receptor (TLR) genes is combined with the severity of RSV infection. It is assumed that the development of asthma in a normal child is not caused by RSV itself, but by previous exposure to unfavorable genetic and antenatal factors against the background of RSV bronchiolitis. This allows us to consider bronchiolitis as a marker of these problems, and not the cause of subsequent disorders. The addition of viral infections in such children will occur with complications and more severe manifestations of airway obstruction, which requires urgent and adequate treatment.
There is a hypothesis that early exposure to viral infections may prevent the onset of AD in later life. A connection has been established between the beginning of a child’s attendance at an organized institution at an early age and more frequent obstruction, while asthma in such children by the age of 6 develops less often than in “home” children. It is known that most asthma exacerbations are combined with viral infections. At an early age, diagnosing asthma is a difficult task due to the variability and nonspecificity of clinical manifestations, as well as the difficulties of performing functional diagnostics. In children of preschool and school age, there is an interaction between exposure to allergens, sensitization to them and viral infections.
The nonatopic phenotype of bronchial obstruction creates the greatest difficulties in diagnosing the disease. It is known that severe adenoviral infection can lead to long-term bronchial obstruction in a previously healthy child. Respiratory viruses (RV, RSV, metapneumovirus, influenza virus) affect the epithelium of the lower respiratory tract and provoke a local immunological reaction, as well as a protective antiviral response with the production of interferons, chemotaxis and activation of NK cells. The airway epithelium is a key component in respiratory disorders. Respiratory viruses damage the ciliated epithelium of the mucous membrane of the respiratory tract, increase its permeability to allergens and toxic substances, increase the sensitivity of the receptors of the submucosal layer of the bronchi, which causes their hyperreactivity and the occurrence of obstructive manifestations in children. The bronchial epithelium produces secretions containing nonspecific and specific anti-infective defense factors and responds to signals from immune cells that are involved in the initiation and maturation of the innate and adaptive immune response, including the inflammatory response to pathogens, the Th2-type immune response, structural changes in the airways and angiogenesis.
However, regardless of the predisposing factors, repeated episodes of respiratory diseases accompanied by bronchial obstruction form and/or aggravate bronchial hyperreactivity, which may likely contribute to the development of recurrent and chronic forms of bronchitis or the risk of asthma. The search for optimal diagnostic and treatment technologies that allow timely correction of bronchial obstruction is an important task for a pediatrician and pulmonologist.
Given the variety and severity of clinical symptoms, in the treatment of children with respiratory viral infections, drugs are used that act on various components of the pathological process. Mucoactive agents (ambroxol, acetylcysteine, carbocysteine) occupy a significant place in the treatment of cough during ARVI. They help to liquefy sputum, increase the secretion of its liquid part, stimulate the work of the ciliated epithelium, and promote the production of surfactant. The main direction of action of drugs in this group is to optimize the rheological properties of respiratory tract secretions, which can have a positive effect on the restoration of impaired mucociliary clearance.
The basis of complex drug therapy for bronchial obstruction during respiratory infections are bronchodilators. For mild manifestations of bronchial obstruction and the presence of difficult to separate sputum against the background of ARVI, the administration of combination drugs containing mucolytics and bronchodilators is effective. The combined drug Uskoril provides bronchodilator and expectorant effects, reduces the duration of cough, makes it productive, which helps to enhance mucociliary transport.
The components of the drug Ascoril - bromhexine + salbutamol + guaifenesin - have a bronchodilator, mucolytic and expectorant effect. Salbutamol, as a fast-acting beta-2 agonist, has a bronchodilator effect. Bromhexine hydrochloride with its active metabolite ambroxol has a pronounced mucolytic and expectorant effect due to the depolymerization and destruction of mucoproteins and mucopolysaccharides of sputum. It also stimulates the activity of secretory cells of the bronchial mucosa. Guaifenesin stimulates the secretion of the liquid part of bronchial mucus, reduces the surface tension and adhesive properties of sputum, reduces anxiety, reduces psychogenic and autonomic symptoms, and improves sleep. Menthol (racementhol) has a mild antispasmodic effect and has weak antiseptic properties. According to our data, the use of Ascoril expectorant in children aged 2 to 10 years with mild or moderate obstructive syndrome during ARVI has a pronounced positive effect on the course of the disease, both as assessed by doctors and according to the results of a parent survey. Acute respiratory diseases in the observed children occurred with a cough due to the involvement of various parts of the respiratory system in the inflammatory process (laryngotracheitis, bronchitis). In children under 6 years of age, Ascoril expectorant was prescribed 5 ml (1 teaspoon) 3 times a day, for children from 6 to 10 years old - 5–10 ml (1–2 teaspoons) 3 times a day. The best results of treatment were observed when it was started early - from the first day of the disease. The duration of therapy was 7–10 days, depending on the dynamics of symptom regression. The validity of the use of short-acting beta-2 agonists (salbutamol) as part of Ascoril is due to the presence of bronchial obstruction disorders in more than 60% of children according to bronchophonography. Oscillations in the high-frequency part of the spectrum (more than 5000 Hz), as well as deviations in the spirogram in the form of mild and moderate manifestations of bronchial obstruction were observed in more than 50% of children. Obvious clinical signs of bronchial obstruction were characterized by short-term episodes of shortness of breath, bouts of unproductive cough, and a small amount of wheezing in the lungs in only 15% of children. In patients receiving a combination drug (bromhexine + salbutamol + guaifenesin), compared with the control group of children receiving only a mucolytic (bromhexine), earlier positive dynamics were observed. By the 2–3rd day of treatment, the cough became wet, there was an improvement in sputum discharge; by the 6–7th day of treatment, the symptoms disappeared in most children (p
The presence of a short-acting bronchodilator in the drug, as well as the complementary effect of mucolytic, sedative, anti-inflammatory components, determined the pronounced clinical effectiveness and led to the disappearance of cough symptoms 3-4 days earlier than in patients in the comparison group (p
A decrease in the severity of cough symptoms was accompanied by improved sleep, increased activity in children, and normalization of their emotional state. The total score of clinical symptoms during treatment showed that the effectiveness of therapy with Ascoril expectorant was statistically significant (p
Three children (4%) of the Ascoril therapy group were given an antibacterial component due to the lack of effectiveness of treatment, but the need for its administration was significantly lower (2.5 times) than in the group of children receiving a mucolytic (in 3 children - 10%; p The positive dynamics of clinical symptoms was accompanied by a significant improvement in bronchophonography and spirography, which indicates the normalization of bronchial patency. One child had an allergic reaction to the drug in the form of a rash. The remaining children had no side effects or adverse reactions.
Thus, the combined drug Ascoril expectorant, providing a combined bronchodilator and mucolytic effect, potentiates the restoration of mucociliary clearance and leads to a more rapid regression of ARVI symptoms, preventing the transition of the disease to a more severe long-term course, and subsequently reduces the need for antibiotics. Clinical efficacy and high safety profile allow the use of Ascoril expectorant as the drug of choice in children over 2 years of age with mild to moderate bronchial obstruction due to ARVI.
When providing emergency care to children with severe broncho-obstructive syndrome, the basis of drug treatment is short-acting bronchodilators. Bronchodilators are necessary for obstructive bronchitis, bronchiolitis, threat of exacerbation or exacerbation of asthma. In pediatrics, to relieve acute bronchial obstruction disorders, various groups of bronchodilators are used: beta-2 agonists, anticholinergic drugs, methylxanthines.
The action of beta-2 agonists is based on stimulation of adrenergic receptors and is associated with activation of adenylate cyclase coupled to the receptor, which leads to an increase in the formation of c-AMP and stimulation of the calcium pump. As a result of a decrease in calcium concentration in myofibrils, dilatation of the bronchi occurs. When used inhaled, they provide a rapid (within 3–5 minutes) bronchodilator effect and help improve mucociliary transport. The method of drug administration depends on the age of the child and the severity of the disease: using metered-dose aerosol inhalers (MDIs), MDIs with a spacer, in the form of solutions for inhalation through a nebulizer and/or enterally.
To relieve bronchial obstruction in children, a combination of short-acting beta-2 agonists with cholinergic drugs is used. According to the international recommendations of the Global Initiative for Asthma (GINA, 2010) and the Russian national program “Bronchial asthma in children. Treatment strategy and prevention" (2008), a fixed combination of fenoterol and ipratropium bromide (Berodual®) is the first line of treatment for exacerbations in children from an early age. The components of the drug have different points of application and mechanisms of action. Due to the synergistic effect, the fixed combination drug uses a lower dose of the beta-2 agonist (fenoterol), which reduces the risk of side effects. Inhalations of Berodual solution through a nebulizer are carried out up to 3-4 times a day in a dosage appropriate to the child’s age (for 1 inhalation): newborns and infants - 1 drop/kg body weight; children from 1 to 6 years old – 10 drops; children over 6 years old – 10–20 drops. After inhalation, the child must be observed for 30–40 minutes.
For bronchial obstruction with severe symptoms of respiratory failure, inhaled corticosteroids (budesonide) are prescribed. The use of budesonide suspension (Pulmicort®) for nebulizer therapy in children has been well studied. Currently, more than 15 randomized controlled clinical studies of the effectiveness and safety of this drug have been published involving children aged 3 months to 18 years with varying degrees of severity of bronchial obstruction. Thus, an open study of the effectiveness of the Pulmicort® suspension was conducted at the emergency stage in Yekaterinburg and Nizhny Novgorod. The drug was used in children with moderate exacerbations of asthma at home in doses of 0.25–0.5 mg, which led to the normalization of the patients’ condition and made it possible to avoid hospitalization in all cases. In Nizhny Novgorod, doses of the drug 0.125–0.25 mg were used 2 times a day for 2 weeks in children with exacerbations, which made it possible to relieve all symptoms by the beginning of the second week of therapy. In young children at the children's clinical hospital of the First Moscow State Medical University named after. THEM. Sechenov used combination therapy (Pulmicort + Berodual + ambroxol). This combination had a faster positive effect than inhalation with Berodual solution alone or Berodual + ambroxol.
When treating exacerbations of asthma or relieving obstruction due to lower respiratory tract infections, the initial dose of Pulmicort® suspension is 0.5–1 mg 2 times a day for children from 6 months. Studies have also shown the effectiveness of administering the suspension once a day.
Currently, Pulmicort® suspension is the only inhaled glucocorticosteroid intended for use via a nebulizer, registered for the treatment of stenosing laryngotracheitis. For stenosing laryngotracheitis, Pulmicort inhalations are used to treat acute symptoms of croup at a dose of 1 mg 2 times every 30 minutes.
If inhaled steroids are ineffective or inhalations are impossible, systemic steroids (orally or parenterally) are prescribed. Indications for the use of systemic steroids for acute obstruction are:
- insufficient effect of bronchodilators (beta-2 agonists or anticholinergics);
- severe and life-threatening conditions;
- history of steroid use to relieve exacerbations.
The therapeutic effect of systemic steroids for severe obstruction lasts for 8–12 hours.
It should be remembered that these drugs have a delayed onset of action (4-6 hours), so if indicated, they should be administered as early as possible. The lowest dose that provides control of the symptoms of the disease is used (1 mg/kg body weight per day when administered orally). The duration of the course usually does not exceed 3–5 days. When conducting a short course of systemic steroids, they can be discontinued at once; a gradual dose reduction is not required. Since ARVI can provoke exacerbations in patients with asthma, the practicing physician must know the algorithm for relieving asthma exacerbations. In cases of mild exacerbation, therapy is started with inhaled short-acting beta-2 agonist using a pMDI with a spacer. If necessary, inhalations are repeated every 20–30 minutes for an hour. In young children, it is advisable to use a combined bronchodilator (beta-2 agonist and ipratropium bromide), and use a nebulizer as a delivery device. If there is no trend towards a decrease in the clinical symptoms of obstruction, the severity of the exacerbation should be reconsidered.
For moderate exacerbation of asthma, the administration of inhaled steroids (Pulmicort® suspension) in combination with bronchodilators through a nebulizer is indicated.
Severe exacerbation of asthma is an indication for hospitalization. At the outpatient stage, emergency care begins according to the previously stated principles. It should be remembered that inhaled bronchodilator therapy is carried out simultaneously with the administration of systemic steroids and oxygen therapy.
In young children with obstruction due to ARVI, a combination of an inhaled bronchodilator, a mucolytic, and an inhaled glucocorticosteroid is effective. The inclusion of mucoactive agents that have a multifactorial effect in the drug complex is advisable from 2–3 days. The drug of choice for inhalation therapy via a nebulizer is ambroxol. Mineral water should not be used for inhalation through a nebulizer. All bottled mineral waters (Essentuki, Narzan, etc.) are intended for the treatment of diseases of the gastrointestinal tract and kidneys and are not indicated for inhalation therapy, especially using a nebulizer.
Thus, only an integrated approach to the treatment of obstructive syndrome in ARVI, taking into account the clinical situation and the age of the child, can ensure high therapeutic effectiveness and have a positive impact on the patient’s quality of life.
For mild manifestations of bronchial obstruction and the presence of difficult to separate sputum against the background of ARVI, the administration of combination drugs containing mucolytics and bronchodilators is effective. The combined drug Ascoril provides bronchodilator and expectorant effects, reduces the duration of cough, makes it productive, which helps to enhance mucociliary transport.