One day hospital 3rd KO
Dadyev
Islam Arturovich
12 years of experience
Oncologist (OMC), surgical oncologist, candidate of medical sciences, member of the Russian Association of Oncologists, member of the Russian society of chemotherapists RUSSCO
Make an appointment
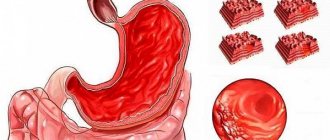
Esophageal cancer is a malignant pathology that involves the degeneration of cells in the mucous membrane of the esophagus and the subsequent formation of a tumor. Increasing in size, the neoplasm partially or completely blocks the lumen of the esophagus, grows through its wall and spreads to nearby organs. Without treatment, death is inevitable. The disease affects men four times more often than women. The main risk group is elderly people: the average age of male patients is 64 years, female patients – 70 years.
Kinds
According to histological characteristics, esophageal cancer is divided into:
- squamous - developing from epithelial squamous cells, in turn, can be superficial and deeply invasive;
- adenocarcinoma – developing from cells that produce protective mucus.
Tumors of the upper (10%), middle (35%) and lower (55%) parts of the esophagus are distinguished by location.
Squamous cell tumors in the superficial form respond well to treatment. An invasive tumor is prone to growing deep into tissue and forming metastases to nearby organs. Adenocarcinoma is much less common and has a severe course of the disease.
Symptoms
As a rule, the first symptoms of esophageal cancer appear too late, when the tumor has already acquired significant size, or accidentally, during examination for another disease. Typically the disease manifests itself through:
- difficulty swallowing food, especially solid food, due to which the patient is forced to reduce portions and give preference to liquid dishes;
- feeling of a constant lump in the throat;
- increased secretion of saliva, often even in the absence of food;
- a feeling of discomfort or even pain in the chest;
- weight loss due to eating problems;
- hiccups, cough, voice changes are rarer symptoms;
- bleeding in the esophagus, due to which the stool becomes dark, almost black;
- anemia, pale skin, constant weakness and drowsiness.
If these signs appear, you should consult a doctor as soon as possible for a thorough examination.
Why does cancer occur?
Esophageal cancer occurs in both young and old people.
Doctors consider risk factors for this disease:
- hereditary predisposition, if one of the parents suffered from esophageal cancer, the risk of the disease increases for children;
- smoking and alcohol abuse, especially if this occurs at a young age, with a fragile body. Those suffering from alcohol addiction get sick 10 times more often - strong drinks lead to chemical burns of the mucous membrane;
- errors in nutrition - eating too spicy, salty, pickled or fried foods;
- work in hazardous industries that use toxic gases;
- poor-quality drinking water containing heavy metals and other harmful impurities;
- chemical burn of the esophagus (alkali, acetic acid);
- bad air in the place of residence or work;
- male gender, the percentage of the disease in men in Russia is 10 times higher than in women, this is largely due to bad habits in men;
- age, most often a malignant tumor appears in people who are between 50 and 60 years old;
- drinking very cold or hot drinks, the drink should be at room temperature or not
- overweight, obesity. Scientists have conducted research and found that esophageal cancer is diagnosed in overweight patients twice as often as in people of normal weight;
- keratoderma (impaired keratinization of the skin);
- mechanical injuries when a solid body enters an organ or constantly ingests solid food.
The cause of cancer can be Barrett's disease - when a hernia occurs, stomach contents reflux into the esophagus, this can lead to Barrett's disease, which is considered a precancerous condition.
Also at risk are people suffering from esophageal achalasia, a neuromuscular disease that impairs the motility of the esophageal walls and the ability of the lower esophageal sphincter to relax when swallowing. Food stays in the esophagus for a long time, which leads to the development of severe pathology.
Cicatricial stricture is a narrowing of the esophagus. Often occurs after a chemical burn. Also as a consequence of a chronic disease in which cells degenerate into cancerous
Causes and risk factors
The mechanism of occurrence and development of esophageal cancer has not yet been thoroughly studied. However, factors have been identified that increase the risk of tumor development:
- smoking and drinking strong alcoholic drinks that burn the esophageal mucosa;
- old age: at least 85% of patients are people over 55 lei;
- overweight, obesity;
- habit of drinking very hot food and drinks;
- the presence of “Barrett's esophagus” - pathological areas of the intestinal epithelium in the lower part of the esophagus, resulting from chronic burns from gastric juice;
- inflammatory diseases of the esophagus;
- decreased locking function of the sphincter between the esophagus and stomach;
- Plummer-Wilson syndrome (simultaneous dysfunction of swallowing, narrowing of the lumen of the esophagus and iron deficiency anemia);
- constant contact with fumes of carcinogenic substances, acids and other aggressive reagents;
- papillomavirus infection.
The increased incidence of men compared to women is explained by the fact that they are much more often exposed to the listed negative factors.
Classification
To correctly assess the extent of the process, select a treatment method and reliably assess the long-term results of treatment, the classification of esophageal cancer by stages is used.
- Stage I - a small tumor affecting the mucous membrane and submucosa of the esophageal wall, without invading its muscular layer. There is no narrowing of the lumen of the esophagus. There are no metastases.
- Stage II - the tumor also affects the muscular lining of the esophagus, but does not extend beyond the wall of the organ. There is a narrowing of the lumen of the esophagus. Single metastases are detected in regional lymph nodes.
- Stage III - the tumor grows through all layers of the esophageal wall, passing through the peri-esophageal tissue or serosa. There is no germination into neighboring organs. Narrowing of the esophagus. Multiple metastases in regional lymph nodes.
- Stage IV - the tumor grows through all layers of the esophageal wall, periesophageal tissue, and spreads to adjacent organs. There may be an esophageal-tracheal or esophageal-bronchial fistula, multiple metastases to regional and distant lymph nodes (classification adopted by the USSR Ministry of Health in 1956).
Stages
Oncologists distinguish the following stages of esophageal cancer.
- Zero. The neoplasm is located on the surface of the epithelial layer, without even growing deep into the epithelium, and is a cancer “in situ”, i.e. "on the spot." It can only be detected by chance during an endoscopic examination of the esophagus from the inside.
- First. Malignant cells spread to the entire epithelium, but do not yet affect muscle tissue. The lymph nodes are not affected, there are no metastases.
- Second. The tumor either grows through the entire wall of the esophagus, including muscle and connective tissue, but without affecting the lymph nodes, or spreads only to the muscle layer and metastasizes to several nearby lymph nodes.
- Third. The size of the tumor creates obstacles to swallowing. Malignant cells affect nearby organs and regional lymph nodes.
- Fourth. Regardless of the size of the tumor and the degree of its spread to neighboring tissues, metastases of esophageal cancer are detected in distant organs - liver, lungs, bone structures.
Clinical picture
There are physiological narrowings in the esophagus, where malignant growth primarily begins. These narrowings are caused by passing near other anatomical formations - the aorta and the forks of the trachea into the bronchi; at the junction of the pharynx into the esophagus and the esophagus into the stomach there is also a slight narrowing. It is believed that the mucous membrane here is more susceptible to minor injuries from rough food, which means inflammation occurs more often. However, in the cervical region the incidence of cancer is 10%, in the lower third of the esophagus - 30%, and 60% of cancers are formed in the middle segment.
Malignant cells not only grow into the thickness of the organ, as happens with most cancers, they also migrate through small lymphatic vessels. The vessels form a complete lymphatic network inside the esophageal wall, spreading the tumor inside, so the length of the tumor can be 5, 10, or 15 centimeters.
In the advanced stage, localization determines the symptoms, and the first signs are considered to be the feeling of food sticking to the same place or scratching the mucous membrane with a piece of food. As it progresses, it becomes difficult to pass first solid pieces, then porridge, then liquid. All this is called dysphagia. First, the patient washes down pieces of food with water, pushing them through, but after that this no longer helps, nutrition is disrupted, and the person loses weight. Contact of the tumor with food leads to inflammation, an unpleasant putrefactive odor appears, and with regular trauma, the loose mucous membrane of the tumor begins to bleed, and life-threatening bleeding can develop.
Pain occurs as the esophagus contracts with peristaltic waves, the pain is spastic in nature. The growth of the tumor through the entire thickness of the esophageal wall makes the pain constant; it is localized between the shoulder blades. Infiltration of the mediastinal tissue by the tumor involves the recurrent nerve, which is responsible for the movement of the vocal cords, in the process, hoarseness and choking when drinking appear. The nerve can be compressed by lymph nodes enlarged by metastases and the sonority of the voice will disappear.
As with achalasia, a tumor forms an expansion above the narrowing of the esophagus, where food accumulates. Nighttime reflux of accumulated food masses into the windpipe can also lead to pneumonia. And during the day I am worried about severe weakness and fever. If the respiratory tract is involved in the process, an anastomosis may form between the esophagus and the trachea or large bronchi - a fistula, through which food crumbs will enter the breathing tube, causing coughing and pneumonia. If such a fistula opens from the esophagus into the mediastinum, its inflammation will lead to death.
Get a treatment program
Diagnostics
If the patient's complaints are similar to those of esophageal cancer, the oncologist will prescribe a series of diagnostic tests to confirm or refute this suspicion.
- X-ray of the esophagus. The test is performed with a contrast agent, which the patient drinks to make the esophagus more visible on the image. The image shows a narrowing of the lumen, allows you to determine the thickness of the walls, and indicates the presence of an ulcer.
- Esophagoscopy. An endoscopic examination is carried out using a flexible probe with a video camera, which broadcasts an image of the internal walls on a screen. The endoscope allows not only to detect pathologies, but also to take samples of altered tissue for analysis.
- Ultrasound of the esophagus and abdominal cavity. It is carried out to determine the size of the tumor and to identify metastases in the lymph nodes and peritoneal organs.
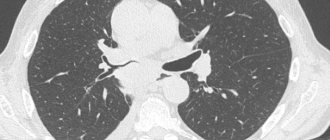
- MSCT of the chest cavity. The procedure allows not only to identify even a small tumor, but also to determine the extent of its spread to neighboring tissues, to identify metastases in the lymph nodes and other organs, including those developing in bone tissue.
- Laparoscopy. A probe is inserted into the abdominal cavity through a small puncture to examine the organs to detect secondary tumors and biopsy the affected tissue.
- Histological analysis of the biopsy specimen. Tissue samples taken are dissected and examined under a microscope to determine the type of tumor cells. This is one of the most important methods for diagnosing esophageal cancer.
Attention!
You can receive free medical care at JSC “Medicine” (clinic of Academician Roitberg) under the program of State guarantees of compulsory medical insurance (Compulsory health insurance) and high-tech medical care.
To find out more, please call +7, or you can read more details here...
Treatment
To ensure that the treatment of esophageal cancer is as successful as possible, oncologists use different methods and directions, building a therapeutic strategy in accordance with the degree of spread of the process, the patient’s condition, the stage of the disease, etc.
- Surgery. Surgery to remove pathological tissue is most effective when the tumor is localized in the middle or lower esophagus. In some cases, complete removal of the esophagus and lymph nodes affected by metastases is performed, followed by reconstruction of the organ from a segment of the small intestine. In the final stages, the intervention is performed to open the lumen of the esophagus in order to return the patient to the ability to eat in the usual way.
- Endoscopy. If cancer is detected at the zero or first stage, gentle endoscopic surgery is possible. A probe with a camera, surgical loop or laser emitter is inserted through the mouth and the diseased tissue is removed. In 70% of cases, such an operation returns the patient to his usual lifestyle.
- Radiation therapy. Radiation is often given before surgery to shrink the tumor. Postoperative therapy is carried out to reduce the risks of relapse and destroy residual malignant cells. For inoperable esophageal cancer, treatment can reduce the growth rate of malignant tissue and prolong the patient's life.
- Chemotherapy. Modern methods of combining cytostatic drugs with radiation therapy make it possible to achieve a significant reduction in tumors and reduce the risk of metastasis.
Statistics
This is one of the most aggressive malignant diseases. Esophageal cancer is the 8th leading cause of death worldwide. According to the International Agency for Research on Cancer, in 2018 the incidence was 7.49 cases per 100,000 people per year, and the mortality rate was 6.62. Calculations by Rosstat of the Russian Ministry of Health say that the incidence is 5.6 cases per 100,000 people. Among men – 9.43 per 100,000, among women – 2.29 per 100,000. The disease is most often diagnosed in the so-called “Asian belt”, that is, from the northern part of Iran, through Central Asia and to the central regions of Japan and China, also capturing Siberia. This is largely due to the peculiarities of the diet of people living in these areas.
Most often (up to 80% of cases), the neoplasm is located in the lower and middle thoracic sections of the esophagus. With a frequency of 10-15% of cases, cancer of the cervical esophagus is diagnosed.
Rehabilitation
In the first few days after surgery, the patient is usually prescribed intravenous nutrition, or nutritional mixtures are introduced into the stomach through a thin tube. Routine pain relief is performed to facilitate the recovery process. An important element of clinical recommendations after esophageal cancer is therapeutic and breathing exercises, which are first performed in bed, and then in a sitting and upright position. A bed with a raised headboard prevents the development of reflux. As the patient recovers, he is allowed to eat normally while following a special diet.
List of sources
- Kirkilevsky S.I. Esophageal cancer: current state of the problem/Oncology. Hematology. Chemotherapy. - 2015. - No. 2/1.
- Clinical recommendations Cancer of the esophagus and cardia. All-Russian National Union "Association of Oncologists of Russia" 2020, 62 p.
- Davydov M.I., Ter-Ovanesov M.D., Stilidi I.S. and others. Barrett's esophagus: from theoretical foundations to practical recommendations. Practical oncology. − 2003. − T. 4. − No. 2. − P. 109–119.
- Khalikova E.Yu. Individualization of parenteral nutrition in surgical oncological practice/Difficult patient. 2014. - No. 6. - With. 15-19.
- Mamontov AS. Combined treatment of esophageal cancer / Practical Oncology 2003; 4 (2): 76–82.
Diagnosis and treatment of esophageal cancer in Moscow
If signs of esophageal cancer appear, contact the Medicine clinic and undergo diagnostics using modern, highly informative medical equipment. Consultations and subsequent treatment are carried out by oncologists and gastroenterologists of the highest category with many years of experience in the treatment of diseases of the esophagus, including oncopathologies. The clinic's laboratory performs all types of tests that are necessary during the treatment process. The inpatient department has all the conditions for a comfortable stay during the treatment and rehabilitation period.
Questions and answers
How long do people live with esophageal cancer?
In the absence of medical care, the patient’s life expectancy is no more than 5-9 months from the moment the tumor is detected. Even in the most advanced cases, life expectancy as a result of competent treatment increases to several years, and with early detection of the disease, the chances of a complete cure range from 85 to 100%.
What does esophageal cancer look like?
With esophageal cancer, there are no obvious changes in the patient’s appearance even at a late stage. It is impossible to independently determine this disease, as special laboratory tests and diagnostic studies are required. If you suspect the presence of cancer, you must contact an oncologist as soon as possible for examination and qualified diagnosis.
Is there a cure for esophageal cancer?
The earlier a tumor is detected, the higher the chances of a complete cure, so if you have the slightest ailment, you should visit a gastroenterologist or oncologist. This is especially important for people at risk. To prevent the disease from progressing to an inoperable stage, you should undergo an annual screening examination.
Attention! You can cure this disease for free and receive medical care at JSC "Medicine" (clinic of Academician Roitberg) under the State Guarantees program of Compulsory Medical Insurance (Compulsory Medical Insurance) and High-Tech Medical Care. To find out more, please call +7(495) 775-73-60, or on the VMP page for compulsory medical insurance
Observation
Active surveillance is indicated for patients for early detection of relapse in the esophagus for the purpose of surgical intervention or relapse in the mediastinum for the purpose of chemoradiotherapy. The scope of the examination depends on the stage of the disease and previous treatment:
Stage I (after endoscopic mucosal/submucosal resections) and stages II–III (after chemoradiotherapy, with prospect of esophagectomy in case of recurrence):
- EGDS – every 3–4 months. during the first two years, every 6 months. – during the third year, then annually until the total observation period is 5 years.
- CT scan of the chest and abdominal organs – every 6 months. during the first 2 years, then annually until a total observation period of 5 years;
Stage I–III (after surgical treatment):
- CT scan of the chest and abdominal organs – every 6 months. during the first 2 years, then annually until a total duration of 5 years.
Other examination methods are recommended for other categories of patients if clinically indicated. Performing PET/CT and determination of serum markers for monitoring patients is not recommended.