Inguinal hernia: symptoms, causes and treatment options
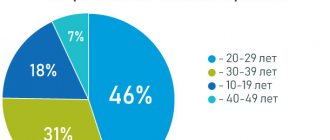
An inguinal hernia in men is a disease in which the walls of the abdominal cavity weaken and cannot hold the internal organs in place. In this case, an inguinal-scrotal hernia appears due to weakening of the inguinal muscles. As a result, protrusion of the organ under the skin is visible. Hernia occurs quite often, especially in older men.
The main factor in its occurrence is serious and regular stress on the abdominal cavity. In order to recognize the disease in time and prevent the development of complications, you need to know its symptoms. And for clarity, you can see what an inguinal hernia in men is in the photo. They will help present the overall picture of the disease.
Causes
An inguinal hernia can occur for a variety of reasons. The following factors are identified that can contribute to the appearance of this disease in men:
- Frequent (chronic) cough, which will put a lot of strain and pressure on weakened areas of the abdomen, which in turn can give rise to the formation of an inguinal hernia.
- A person's hereditary predisposition to an inguinal hernia is revealed in the anatomical weakness of the abdominal muscle tissue.
- Some diseases of the intestinal system can increase intra-abdominal pressure, especially when they cause constant constipation in the sick person.
- Excessive physical activity, which puts strong pressure on the abdominal cavity (and increases intra-abdominal pressure itself). Lifting heavy objects, holding something suspended, and carrying heavy things in front of you is considered especially dangerous.
- Previously suffered injuries to the groin area, which caused a sharp weakening of ligaments and muscles.
- Sudden weight loss leads to the formation of empty volumes in the human peritoneum, which can push outward into the abdominal cavity.
- Excess weight can put excessive stress on internal organs, which increases a person’s tendency to develop an inguinal hernia.
As can be understood from the above, several factors can contribute to the development of an inguinal hernia in men, but the most common cause of this disease is lifting heavy objects. It is most quickly capable of leading to an acute condition in a person, in which he will require immediate treatment.
Complication of scrotal hernia - strangulation
The most dangerous condition is when the hernia in the scrotum is strangulated. In this case, the part of the intestine that prolapses into the hole in the abdominal wall is compressed, preventing the intestine from returning to the abdominal cavity. Contents in this area cannot move further, resulting in a blockage.
The intestine itself is limited in blood supply and soon, due to ischemia, necrosis develops in this area. It is not difficult to detect pathology. The hernia, which was still soft, becomes hard and painful. The skin becomes red and hot. After a few hours, bloating, sharp abdominal pain, nausea, and sometimes vomiting appear.
Classification
Depending on the origin of the hernial sac, hernias are:
- Acquired - occur mainly in adults who experience severe physical exertion. They are both straight and oblique.
- Congenital - occur when the vaginal process of the peritoneum does not grow, when the testicles descend into the scrotum before birth. They are only oblique.
According to the anatomical classification, hernias are of the following types:
- Direct inguinal hernia is always acquired, never passes through the spermatic cord and does not descend into the scrotum; these are the signs that distinguish it from an indirect inguinal hernia. This hernia is very rarely strangulated. The sizes are usually not very large, on average 5-10 cm;
- Oblique PG - characterized by the passage of the hernial sac as part of the spermatic cord with the subsequent appearance of a protrusion under the skin of the groin area, and in advanced cases, in the scrotum. Has a tendency to infringe. Sizes vary from 4-5 cm to giant ones - 30-40 cm;
- Supravesical PG - occurs when there is weakness in the anatomical structures located immediately above the pubic bone. The protrusion is usually not very large;
- Sliding hernia – already from the name it can be assumed that this type of hernia is characterized by incomplete entry of the organ into the hernial sac, but only by one of its walls. Often, only part of the bladder and cecum ends up in the hernial sac. That is why, with this type of hernia, some difficulties arise when suturing the hernial sac during surgery;
- Combined inguinal hernia - with this type of hernia, the patient simultaneously experiences direct and oblique inguinal hernias, very rarely they are joined by a supravesical hernia.
Another important clinical classification on which the choice of treatment depends:
- Irreversible PG - occurs when there is a long-term presence of a hernia, when the hernial sac is connected by adhesions to the subcutaneous fatty tissue. In this case, it is not possible to reduce the hernia into the abdominal cavity, but its contents are not tense and may slightly decrease or increase;
- Reducible hernia - characterized by independent or manual reduction of the contents of the hernia into the abdominal cavity. Usually these are small hernias and at the initial stage of development, when adhesions between the tissues have not yet formed;
- Strangulated hernia - if it is strangulated, it is impossible, even with external help, to reduce the contents of the hernia into the abdominal cavity. In this case, the hernial sac is tense and painful.
You can determine whether an inguinal hernia is strangulated or not by performing a simple task - holding the hernia with your hand, you need to cough several times. If at the same time the hernial protrusion increases and decreases, then the hernia is reducible. Otherwise, if, when coughing, the protrusion does not change its size and continues to hurt, it is most likely that the hernia is strangulated!
Rehabilitation period
The duration of the recovery period after treatment of a hernia ranges from 3 to 10 days, which depends on the volume of the operation and the method of its implementation. With local anesthesia and removal of a small hernia, a person can go home a couple of hours after the operation. After general anesthesia, the patient can be released after 2 days; with laparotomy, the duration of inpatient treatment can be up to 10 days.
All patients, regardless of the type of operation, are prescribed a gentle diet with the exception of fatty, salty, spicy, fried foods and painkillers as needed. Physical activity must be avoided for at least 1 month. The sutures after surgery are removed on days 6–8. In the postoperative period, it is recommended to wear a bandage to relieve stress. Full restoration of functionality may take up to 5 months.
An inguinal hernia is not one of those diseases whose treatment can be shelved. Its progression, increase in size, in the absence of treatment, will ultimately lead to its infringement, and it is unlikely that it will be possible to get by with a small incision in the groin area. In addition, this complication is fraught with intestinal dysfunction and gangrene of loops that fall into the hernial sac. In this case, the dead areas will have to be removed.
Book a consultation 24 hours a day
+7+7+78
Symptoms
In men, the symptoms of an acquired inguinal hernia (see photo) are as follows:
- The formation can be straightened with regular pressure, and a characteristic rumbling sound can be heard.
- In a lying position, the protrusion usually either levels out or greatly decreases in size, and vice versa, in an upright position it increases and appears again.
- In the reduced state of the hernia, you can easily feel the enlarged inguinal ring through the skin.
- When the hernial sac descends into the scrotum, the corresponding half of the scrotum increases in size.
- With strong coughing, straining, or sneezing, the hernia increases in size and becomes tense; if you put your hand on it, you can easily feel it.
With a small inguinal hernia, there are no longer any symptoms that bother the patient. But with a significant increase in protrusion, the following ailments may appear:
- Pain in the lower back, lower abdomen - this occurs due to compression of other organs and intestines.
- Aching, prolonged pain in the area of the hernial formation.
- Other signs of indigestion, such as bloating, loud rumbling.
- Constipation, this is also caused by compression of the intestinal loops in the hernial sac.
- In rare cases, if part of the bladder gets into a hernial formation, problems with urination may occur.
The symptoms of an inguinal hernia are quite obvious upon visual examination; the formation has a dense elastic consistency and is easily palpable on its own. It can be round, and if the hernial sac descends into the scrotum, then the protrusion has an elongated shape. As a rule, with a genetic predisposition, the body’s tendency to develop a hernia, a hernial protrusion may occur after lifting weights and intense physical activity.
A hernia appeared in the groin. What to do?
You or your relative, father, husband, friend, colleague or just a loved one has an inguinal hernia. It always appears at the wrong time and unexpectedly for its new owner, sometimes on both sides at once (bilateral). The process of herniation begins. The scenario and first signs of the appearance of a hernia vary. Anything can happen against the background of complete well-being and good general condition. Unpleasant pulling sensations in the lower abdomen appear and disturb, or after strong physical activity (static tension, heavy lifting, repairs, sports) a sharp pain occurs in the groin. Unpleasant sensations and pain may subside and go away on their own, but then a characteristic tumor-like hernial formation (bulging, bulging) of an oval or round shape is discovered in the groin area.
Consultation with a surgeon, candidate of medical sciences
Make an initial appointment in Moscow by phone
An inguinal hernia comes in different sizes (from a pea or larger) and can enlarge with coughing, sneezing, straining and physical activity. Pain, discomfort and discomfort are usually periodic. The hernia is mobile, reducible, and over time, it can begin to descend into the scrotum, turning from just inguinal to inguinal-scrotal. In addition to pain and discomfort, there are often dysuric phenomena (impaired urination - frequent, difficult or involuntary, urinary retention, pain and discomfort in the urethra). Periodic chronic constipation and/or bloating may be a concern. If your close relatives (father, grandfather, great-grandfather and others) had a similar pathology, then the likelihood of it happening to you and your children is very high. The process, location and age at which the formation appears in the groin may be similar. The symptoms are often the same.
A hernia has appeared. It would seem that there is nothing wrong and you can continue to live with her. Especially if it is small in size and practically does not bother you. Yes, there is some discomfort, there are inconveniences, but it seems that you can put up with it. In this situation, some choose the “ostrich” tactic and try to avoid the problem and not pay attention to it. Others enter a mode of observation and watchful waiting. You know, indeed, you can live like this for some time, but you need to take into account that the hernia carrier’s quality of life will suffer and decrease. Taking this factor into account, you need to decide what to do next.
If nothing is done, the hernial protrusion, as a rule, gradually increases in size and becomes more and more disturbing. More and more new symptoms appear that make it difficult to live peacefully. The discomfort is growing. But most importantly, there is always a danger of complications (strangulation, coprostasis and others). An inguinal hernia is like a “bomb” in your pocket, which can suddenly explode at any moment (both day and night) (complicated - pinched). And then she will have to be operated on as an emergency, which means that the likelihood of postoperative complications increases many times over, even after a well-performed surgical intervention. Hernioplasty (surgery) in such a situation will be less reliable, and the likelihood of relapse is very high.
When an injury occurs, it will be a great success if there is a good hospital and a qualified surgeon nearby. And if not? What if you are far from home? Business trip? On a rest? Fishing? Abroad? In such a situation, everything is left to chance. You are taking a risk... The consequences can be unpredictable and sometimes disastrous. The hernia limits freedom of movement. You need to constantly remember it. Among other things, the condition of a person with a hernia negatively affects not only him, but also affects his family, relatives and friends. A man can quietly plunge into prolonged depression and frustration. It's no secret that behind the outer brutal shell, imperturbable character and iron will often hide fears that are not voiced even to oneself. The stronger sex can solve the most difficult problems, be a stone wall for their loved ones and friends, stand to death, but men also need help and support. Often, hernia carriers do not want to talk about their problems and show their weaknesses. Sometimes the mere mention of a visit to the doctor or the need for surgery puts you into a stupor. It seems that it is easier to die than to solve this problem.
No matter how difficult and scary it may be, it is necessary to face this problem head on. And here only really close people whom a man trusts can help. These are usually parents, wives, children or friends. We need to walk this path together, step by step. The path from the appearance of a hernia to surgery and successful rehabilitation. To make the right decisions, you need to find answers to the many questions that arise with your family and friends.
What is an inguinal hernia? How does she look? What are its reasons? Why did it appear specifically for me? What health risks does an inguinal hernia pose? Who is treating? Where to contact? How to cure a hernia? Is it possible not to contact a surgeon? Is it possible to do without surgical treatment (not undergo surgery)? Is it possible to cure a hernia with folk, home or alternative remedies? Is it dangerous not to have surgery? If I have surgery, where can I do it? Where is the best place to do this operation? How long does the operation take? Does it hurt? What anesthesia or anesthesia is used to perform the operation? What surgical procedures are used to remove an inguinal hernia? What is the best operation to do? Open cavity or laparoscopic? What are the differences between surgical interventions for inguinal hernia? Is it possible to cut out hernias from both sides at once? What is needed before surgery? What examinations are needed? How much does surgery to remove an inguinal hernia cost? Cost of surgery (hernia repair)? What are the complications? What to do if there is a complication? What kind of rehabilitation is necessary after surgery? For how long is sick leave issued? What to do? And many, many other very diverse questions...
No one prepares to answer these questions from childhood, and many will not even need it in life. But if you are faced with such a problem, then you cannot do without collecting information. You should not complain about fate, rely on miracles or traditional healers. You need to learn as much as possible and immediately and consistently act. If you go to any forum on inguinal hernias, to the questions and answers section or frequently asked questions (FAQ, Q&A), and type reviews in search engines, you will see a lot of different opinions and advice. Sometimes they can be contradictory or even mutually exclusive. In order to act, you need information and knowledge from different sources. Read, analyze, think, ask and make decisions, only for you. We will try to help you, tell you in detail about inguinal hernias in men and answer your questions...
Strangulated hernia
A strangulated inguinal hernia is accompanied by the following symptoms:
- weakness, tachycardia;
- nausea, vomiting;
- bloating, lack of stool;
- negative reaction to a cough impulse; when coughing, placing a finger on the inguinal ring, shocks are usually felt; if the hernia is strangulated, the impulse is not transmitted;
- the hernia stops being reduced;
- the hernial sac is very tense;
- sharp, acute pain in the hernia area and in the abdomen.
A strangulated inguinal hernia is a very dangerous complication, so medical care should be provided as soon as possible. The operation must be performed as quickly as possible, since serious complications may develop, such as:
- Necrosis is the necrosis of parts of the intestinal loops or omentum that have fallen into the hernial sac.
- Peritonitis - with prolonged strangulation of the groin hernia, inflammation of the abdominal cavity develops.
At the same time, irreducible and large hernias, even without complications, cause discomfort to patients: they limit their activity and are accompanied by unpleasant symptoms.
When is an ultrasound necessary?
First of all, an ultrasound is prescribed by a surgeon or urologist if it is necessary to confirm or clarify the diagnosis, which is of particular importance at the initial stage of development of the disease. Alarming signs that require an ultrasound diagnosis of the groin area may include: swelling of the scrotum (in infants), problems with urination, discomfort and pain in the groin area. Despite the similarity of symptoms, the pathogenesis of inguinal hernia occurs differently and largely depends not only on the age, but also on the gender of the patient, although, according to medical statistics, for every 5 patients seeking help, there is only 1 woman. It should be remembered that correct and timely diagnosis and treatment prescribed based on its results can completely relieve the patient from discomfort and relapses, as well as eliminate the risk of pinching and necrosis, which is fraught with surgical intervention and long-term treatment.
Treatment of inguinal hernia in men
The only treatment for inguinal hernia in men is surgery. During the operation, the doctor excises the hernial sac and performs plastic surgery of the hernial orifice, which prevents further relapses of the disease. Plastic surgery of the hernial orifice can be performed either using an aponeurosis (tension technique) or using a special mesh prosthesis (non-tension technique).
In most cases, removal of an inguinal hernia in men is performed with the subsequent use of a polypropylene mesh. It is installed in the hernial orifice and fixed. Subsequently, connective tissue fibers grow through its cells and form a reliable barrier for the abdominal organs on the way to the inguinal canal. Using this technique significantly reduces the likelihood of recurrence of the disease.
Surgeries for inguinal hernia in men can be performed either in the traditional open way with a skin incision, or laparoscopically - through a small puncture.
Diagnostics
If there are characteristic complaints, the pediatric surgeon conducts a careful but detailed examination of the child.
In case of strangulation, an inguinal hernia looks like a swelling localized in the groin, which in boys can descend into the scrotum, i.e. along the funicular spermatic tract. In girls, such hernias are usually small and hardly noticeable upon examination. However, a targeted examination allows us to identify this problem. In difficult clinical cases, an ultrasound scan of the abdominal organs, groin area, pelvis and scrotum is performed. For the greatest information content, ultrasound is supplemented with Doppler ultrasound, which allows assessing blood flow. Modern ultrasound scanners, which the SM-Doctor children's clinic is equipped with, make it possible to clearly distinguish the tissue structures and organs of the groin area and scrotum in order to assess the nature of their involvement in the pathological process. Doppler data is an objective assessment of the preservation of blood flow in the strangulated organs, which is necessary for planning the most rational extent of surgical intervention. If there are symptoms of intestinal obstruction, then a plain radiography is indicated.
Laboratory indicators in the first hours of infringement differ little from the norm. Some children may have a slight increase in the number of leukocytes and accelerated erythrocyte sedimentation in a general clinical blood test.
Laparoscopic surgery for inguinal hernia
Laparoscopic technology allows special manipulators to enter the patient's abdominal cavity through small punctures on the anterior abdominal wall. The advantage of the operation is that there are no scars left after it, and minor damage to the tissues is caused during the procedure.
- At the initial stage, the patient is given anesthesia. The intervention is performed under general anesthesia (anesthesia).
- Carbon dioxide is pumped into the abdominal cavity, due to which the anterior abdominal wall is raised like a dome, and conditions are created for surgeons to work.
- The hernial sac with its contents returns back to the abdominal cavity.
- A mesh is sutured from the inside to the abdominal wall. As a result of this, it more effectively holds the abdominal organs and prevents them from extending beyond its limits. Gradually it grows and is securely fixed in its place.
Due to a number of advantages, laparoscopic hernia treatment methods are gradually gaining popularity. However, if the protrusion is large, then surgeons prefer to work using traditional methods, since it is technically easier to perform the intervention. Therefore, it is necessary to contact doctors for help as early as possible and receive treatment using the most modern methods.
How long do you need to stay in hospital? Usually, after laparoscopy, a man can go home within 1 day after the operation, if no complications arise.
Definition
An inguinal hernia
is a pathological formation that should not exist normally. This is a tumor-like protrusion of a round or oval shape in the groin area (lower abdomen) on the right, left, or on both sides at once. An uncomplicated hernia is best detected in an upright position (standing) and can disappear (reduced) in a horizontal position (lying down).
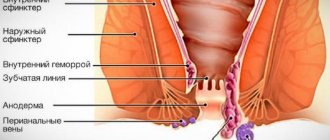
An inguinal hernia consists of the following elements:
- hernial orifice
(the place where the hernia emerges is weak spots or holes in the anterior abdominal wall in the groin area, inguinal rings)
- hernial sac
(a section of the peritoneum that exits through the hernial orifice along with the contents - the abdominal organs)
- hernial contents
(what is inside the hernia and hernial sac - omentum, intestine, bladder, etc.)
Complications after surgery
The most common consequences after surgery are:
- Seams coming apart.
- Hematomas. To prevent them, ice is applied immediately after surgery.
- Infection and suppuration of the wound. To avoid this, a course of antibiotics is prescribed.
- Dropsy of the testicles. Develops due to damage to the membranes of the testicle. A symptom of this complication is an enlargement of the scrotum on one or both sides. It can only be treated surgically.
- Damage to the spermatic cord. It occurs due to the fault of the doctor and is associated with the structural features of the inguinal canal. The spermatic cord passes close to the hernial sac, so if the doctor is insufficiently qualified, it can be damaged. This complication can lead to infertility.
- Damage to the hip joint. Occurs in case of rough sutures.
- Relapse. Recurrence of a hernia most often occurs due to patient non-compliance with the regimen.
- Damage to blood vessels. This is also a rather serious complication, as it leads to testicular atrophy.
Even an operation to remove an inguinal hernia in men that is considered easy and safe can be accompanied by complications. Most often, they arise through the fault of the patient himself, due to violation of restrictions during the rehabilitation period. Sometimes complications arise due to the fault of the surgeon, or arise as a result of the individual characteristics of the body.
Reasons for appearance
An inguinal hernia is a disease associated with prolapse or protrusion of abdominal organs in the groin area. In this case, a hernial sac is formed, which most often contains intestinal loops or part of the greater omentum. There are two main reasons for the formation of this defect: congenital changes in the structure of the inguinal canal and increased intra-abdominal pressure.
Birth defects appear in childhood, starting from the first year of life. In boys, they develop as a result of non-fusion of the testicular membranes or expansion of the inguinal canal. In adult men, hernias occur as a result of heavy physical exertion. In older people, the disease is associated with a decrease in the tone of muscle tissue and an increase in its extensibility.
General risk factors for the development of pathology, regardless of age and gender:
- Obesity.
- Chronic severe cough.
- Injuries to the groin area.
- Pathology of the gastrointestinal tract associated with increased intra-abdominal pressure (more often, this is an increase in the size of organs and tumors).
- BPH.
- Chronic constipation.
- Passive lifestyle.
- Heavy physical activity (especially for athletes involved in weightlifting, such as lifting weights).
- Playing wind instruments in combination with other risk factors.
- Women have multiple pregnancies.
Diet after hernia repair
A proper diet will speed up recovery. For the first few days, it is better to eat only liquid and pureed food in small portions. On day 4-5 you can go back to your normal diet.
You need to eat as many foods rich in protein and fiber as possible. The diet should include:
- lean boiled meat (chicken, beef);
- seasonal vegetables (raw or steamed);
- dairy products, especially cottage cheese;
- fruits and berries;
- various porridges (buckwheat, millet, oatmeal, pearl barley);
- Fish and seafood;
- nuts and dried fruits.
It is better to exclude alcohol and coffee from your diet, as well as smoking.
How to prepare for hernia surgery?
Scrotal hernia surgery is usually planned and has to wait for some time. At this time, the hernia can not only cause pain, but also increase significantly. Most types of hernias (not only abdominal, but also inguinal, umbilical, esophageal or incisional) do not pose an immediate threat to life, but if they are strangulated, serious problems can arise.
To prevent this from happening, you must follow certain rules of behavior and, in addition, you need to carefully prepare for the upcoming operation.
- Check if you are vaccinated against hepatitis B. To do this, you need to take an antibody test. If there are few of them, you need to get vaccinated.
- If you suffer from any chronic illness, take the recommended medications regularly to prevent your overall health from deteriorating.
- Avoid colds and any infections that may cause sneezing and coughing. These are situations in which abdominal pressure quickly increases, which can lead to the growth of the hernia or even strangulation.
- Don't overeat because after eating, the pressure in your stomach also increases. Before and after surgery, significantly reduce the amount of food you eat, but eat more often, 5-6 times a day.
- Avoid constipation. The pressure when attempting to defecate can be so intense that it will significantly enlarge the hernia. If you have a tendency to constipation and bloating, be sure to change your diet - eat more foods rich in fiber (vegetables, fruits, dark bread).
- Don't lift heavy objects. This is the main cause of strangulated hernias.
What are the options for treating an inguinal hernia without surgery?
Taking into account the pathogenesis of the disease, it is believed that treatment for inguinal hernias without surgery is impossible. It should be borne in mind that the bandage also does not cure, but only helps to keep a reducible inguinal hernia in men in the abdominal cavity.
According to some doctors, treating an inguinal hernia in men with physical exercise has no therapeutic effect. However, many experts advise using exercises to increase the strength of the abdominal muscles, but only while lying on your back or sitting.
For example, exercises such as:
- breathing with the stomach with a load (1-2 kg) on the abdominal wall;
- raising straight legs 30° relative to the horizontal position of the body;
- raising the shoulder girdle and shoulder blades from a horizontal position (with hands placed on head);
- squeezing a ball placed between the knees (lying on your back, with your knees bent), etc.
The most suitable yoga asanas for inguinal hernias are: uddiyana, pavanmuktasana, sarvangasana, etc. Uddiyana asana should be performed while sitting: exhale the air forcefully, “squeezing” it out of the lungs, drawing in the stomach as much as possible, hold for three seconds, and then take a deep breath through the nose. Repeat 5-6 times.
Scrotal hernia: treatment
A scrotal hernia, unlike, for example, an umbilical hernia, does not reduce or heal on its own, so surgery is necessary.
- In children, operations are performed when the child is one year old.
- A man should consult a urologist if he notices the above symptoms immediately. The operation must be done within the time frame specified by the doctor, without delay.
The traditional method of surgical treatment of hernias, including scrotal hernia, is hernioplasty using the Bassini method (using your own abdominal wall tissue). The recovery period lasts from 4 to 12 weeks.
Bassini hernioplasty carries a risk of recurrence of the hernia, so it is recommended to perform the Lichtenstein procedure, during which the doctor protects the operated area with a polypropylene mesh. After such an operation, the risk of hernia recurrence is significantly reduced. The recovery period is also shorter, lasting 1-3 weeks.
Endoprosthesis for hernioplasty
Invasive treatment also uses laparoscopic techniques, in which special guides are placed in the groin through which surgical instruments are inserted. Using mini instruments, the operation is performed and a protective mesh is sewn in.
Prevention
The disease can be prevented by avoiding excessive physical activity and lifting heavy weights. It is important to take care of the stable functioning of the gastrointestinal tract, because constipation provokes hernias. You need to lose excess weight and do physical therapy. You should strengthen your abdominal wall by performing abdominal exercises and “bicycle” exercises. Therapeutic gymnastics should be given at least 20-30 minutes a day.
It should be noted the importance of maintaining a competent diet. You need to eat often, but little by little, and no alcohol. Instead of fatty and spicy foods, flour and confectionery products, you need to eat vegetables, fish and meat, boiled or steamed.
Main predisposing factors for groin hernias
Hereditary predisposition is one of the most important reasons for the formation of an inguinal hernia. Of course, a hernia itself cannot be inherited - features of the anatomical structure of the abdominal wall, features of the tissue structure of muscles and aponeuroses (tendons) are inherited, which in one way or another can contribute to the formation of a hernial protrusion. Therefore, inguinal hernia often runs in families. On the other hand, one should not consider the hereditary factor as a kind of death sentence: the correct approach to the physical development of a child, a reasonable choice of profession, dosed physical work in adulthood play a big role and serve as an effective prevention of the development of a hernia in the inguinal region. Therefore, the fact of the presence of a hereditary predisposition should be considered as a warning and a reason for a more responsible attitude towards one’s own body.
Constitutional features . Doctors have long noticed the relationship between body type (hyper-, normal-, asthenic) and the likelihood of developing certain diseases. This pattern also applies to inguinal hernias. In particular, people of the hypersthenic type (with a wide chest, wide abdomen, relatively short limbs and developed muscles) more often develop direct inguinal hernias. On the contrary, asthenics (people with a narrow chest and long limbs) are more likely to develop indirect inguinal hernias. This circumstance is explained by the fact that different types of body structure and the abdominal wall in particular correspond to various specific nuances of the structure of the abdominal wall, its muscles, ligaments and aponeuroses. It is worth considering that a particular body type in itself is not a determining factor in the development of a certain type of hernia - it only indicates an increased likelihood of this.
On the other hand, there are a number of genetic pathologies that are associated both with a certain body type and with connective tissue weakness, which results in the development of hernias. For example, Marfan syndrome. However, in this case, we are not talking about a connection with the constitution of the body, but about the result of congenital underdevelopment of connective tissue formations. Often in such pathologies, hernias are accompanied by articular dysplasia, scoliosis, flat feet, malocclusion and other manifestations of connective tissue deficiency.
Connection with gender - numerous statistical observations indicate that in the vast majority of cases, representatives of the stronger half of humanity experience inguinal hernias. This circumstance is explained, as mentioned above, by the specific structure of the male inguinal canal, as well as by the peculiarities of the intrauterine formation of the male body.
Pregnancy is a condition in which there is a significant increase in intra-abdominal pressure. It is absolutely physiological and by nature a certain margin of safety is built into the body of the expectant mother, which allows her to go through the period of bearing a baby without serious harm to her health. However, with multiple pregnancies, polyhydramnios, and frequent births, compensatory mechanisms may not be enough and there is a possibility of developing a hernia. In addition, it should be taken into account that the state of pregnancy affects connective tissue at the biochemical level. This is necessary for subsequent childbirth: muscles, ligaments, and joints soften, become more mobile and elastic, which also contributes to the formation of abdominal wall hernias. However, pregnancy more often causes hernias of the white line of the abdomen; inguinal hernia develops relatively rarely.
Obesity is a common cause of hernias. A thick layer of subcutaneous fat in the abdominal wall, which is almost always observed with excess body weight, provokes sagging and atrophy of the underlying muscle tissue. In addition, in obesity, adipose tissue is usually located in the lower abdomen. A thick layer of skin and fat creates additional stress on the muscles and aponeuroses of the lower third of the anterior abdominal wall, which leads to their degeneration, weakening and also creates a significant predisposition to the formation of inguinal hernias.
Exhaustion is the opposite of obesity, which can also serve as a prerequisite for the occurrence of an inguinal hernia. A sharp decrease in body weight, on the one hand, may indicate diseases that themselves can contribute to the formation of a groin hernia. On the other hand, the lower part of the anterior abdominal wall, even in fairly slender people, contains a fairly noticeable layer of fat. The disappearance of such a layer inevitably weakens the abdominal muscles and can provoke inguinal hernias.
Publications in the media
Regarding the treatment of this disease, you can contact the Surgical Department No. 1 of the Clinic of Faculty Surgery named after. N.N. Burdenko
A congenital abdominal hernia occurs when the abdominal wall or diaphragm is underdeveloped • Congenital hernia is an anatomical concept. Its first manifestations can occur not only in early childhood, but also in adults (especially with a congenital inguinal hernia). This is explained by the fact that a weak spot in the abdominal wall becomes a hernial orifice only under the influence of a provoking factor - an increase in intra-abdominal pressure, often caused by heavy lifting, persistent cough, frequent anxiety (crying) or straining with chronic constipation or difficulty urinating • This group includes congenital inguinal and diaphragmatic hernias.
Congenital inguinal hernias in children are exclusively oblique. The viscera with them enter the inguinal canal outward from the lateral inguinal fold and pass obliquely through the inguinal canal.
• Frequency - 1-3% of children. In 35% of patients, the diagnosis is made before the age of 6 months •• Right-sided localization is 60% of cases, left-sided - about 30%, in 10-15% of cases the hernia is bilateral •• In boys it is registered 6 times more often •• In premature infants the incidence 1.5–2 times higher.
• Etiology: protrusion of internal organs into the lumen of the unopened processus vaginalis of the peritoneum (by the time of birth it is obliterated in 75% of newborns) •• Processus vaginalis of the peritoneum is a protrusion of the parietal peritoneum in the form of a blind sac descending into the scrotum, where the testicle moves from its original location in the lumbar areas •• Similar phenomena are observed in the female fetus. But normally the ovary remains in the pelvis. The inguinal canal in girls is much narrower and contains the round uterine ligament. The protruding vaginal process of the peritoneum closes. However, it may remain open after birth in the form of the so-called Nukki canal.
• Clinical picture •• History and physical examination ••• Round formation or swelling in the groin, scrotum or labia ••• Appears during an increase in intra-abdominal pressure (with screaming or straining) ••• Usually disappears after a decrease in intra-abdominal pressure, but in most cases, it easily recurs ••• Even if there is no hernial protrusion at the time of examination, in boys a compaction of the spermatic cord is found - a sign of an unstretched hernial sac (silk glove sign) •• Surgical findings in men ••• The hernial sac is covered with fascia of the levator muscle testicle ••• The tunica vaginalis of the testicle is absent ••• The testicle protrudes into the lumen of the hernial sac and is visible after opening the latter.
• Differential diagnosis •• Hydrocele of the testicle or spermatic cord: the tumor does not retract into the abdominal cavity and does not change its size when straining, gives a dull sound when percussed. It should be remembered that when hydrocele of the testicle communicates with the abdominal cavity, the tumor is reduced •• Inflammation of the inguinal lymph nodes: the formations are dense, limited from the external opening of the inguinal canal, and do not change when straining. Inguinal lymphadenitis is very painful, hot to the touch, the skin over it is swollen and reddish in color.
• Treatment is surgical. Even in the absence of a palpable hernia, but with a typical history, surgical intervention is usually performed. In children, hernia repair is used without opening the inguinal canal according to Roux-Krasnobaev. Stages of the operation: •• Isolation of the hernial sac •• Dissection of the hernial sac and revision of its contents. Reduction of the latter into the abdominal cavity •• Separation of the spermatic cord and testicle along with the peritoneum of the hernial sac covering them •• Applying a purse-string suture to the neck of the hernial sac (care must be taken not to damage the spermatic cord) •• Excision of the rest of the hernial sac •• Anterior plastic surgery the walls of the inguinal canal ••• First, the legs of the external inguinal ring are captured in the suture so that it has a sufficient opening for the passage of the spermatic cord ••• Then the formed fold of the aponeurosis of the external oblique abdominal muscle is strengthened with another 2-3 silk sutures.
Strangulated congenital inguinal hernia
• In boys, a strangulated hernia usually contains an intestinal loop •• There is a high probability of developing obstruction and ischemia of the intestine with necrosis of its wall •• Edematous strangulated intestine compresses the vessels of the spermatic cord, which leads to ischemia of the testicles with their necrosis and atrophy.
• In girls, as a rule, strangulation of the ovary occurs.
• Clinical picture •• Incarceration often occurs for no apparent reason or after some minor reason (coughing attack, straining during defecation) •• The child screams, complaining of pain in the hernia area, and sometimes throughout the abdomen •• The hernial swelling becomes dense, tense, very sensitive to palpation and irreducible •• Nausea and vomiting soon occur •• There may be an urge to defecate.
• Treatment •• Conservative ••• In children in the first months of life or with severe somatic pathology in the early stages (up to 12 hours), the following measures are indicated: warm bath - IM 1% trimeperidine solution and 0.1% solution atropine - position with a raised pelvic end ••• Forced attempts at reduction are unacceptable ••• If conservative treatment is ineffective within 2-3 hours, surgery is indicated •• Surgical. Stages of the operation: ••• Isolation and opening of the hernial sac ••• Fixation of the strangulated organ ••• Dissection of the strangulated ring. In case of an indirect inguinal hernia, it is unacceptable to dissect the ring downwards (danger of injury to the femoral vessels) and medially (danger of damage to the lower epigastric vessels) ••• Assessment of the viability of the strangulated organ with its subsequent removal or reduction ••• Plastic surgery of the anterior wall of the inguinal canal.
Congenital diaphragmatic hernias are caused by the presence of holes in the diaphragm, allowing the contents of the abdominal cavity to penetrate into the chest.
• Frequency - 1 in 1,700 births.
• Classification •• By localization of congenital defects of the diaphragm ••• Hernia of the dome of the diaphragm (66% of cases) ••• Hernia of the esophageal opening of the diaphragm (19%) ••• Hernia in the anterior part of the diaphragm (15%) •• Depending on the presence of a hernia sac ••• True (there is a hernial sac) ••• False (there is no hernial sac, the abdominal organs are in direct contact with the pleura).
• Clinical picture •• Soon after birth, cyanosis may occur, which differs from cardiac cyanosis in that it is intermittent in the form of attacks associated with eating or crying •• If the stomach is displaced into the pleural cavity and stretched by liquid and gases, then, in addition to shortness of breath, cyanosis and increased heart rate, coughing, vomiting and difficulty swallowing also occur •• On the affected side, respiratory sounds are weakened (or absent) •• Percussion is used to determine the displacement of the heart to the side opposite the hole in the diaphragm •• In the affected half of the chest, peristaltic noises are heard •• Due to the migration of contents into the chest cavity, the abdomen acquires a scaphoid shape •• When a diaphragmatic hernia is strangulated, intestinal obstruction develops, not accompanied by bloating •• Hiatal hernias in older children are characterized by the development of anemia: gastric bleeding occurs due to ulceration of the esophagus and stomach, which are constantly injured in the area of the hernial orifice •• Anterior hernias of the diaphragm are mostly detected only with age. The leading symptom is abdominal pain due to partial strangulation of displaced intestinal loops.
• Method of examination - X-ray of the chest while lying down and in an upright position of the body •• Gas bubbles with fluid levels (stomach or intestinal loops) in the affected half of the chest •• Displacement of the mediastinal organs to the side opposite to the affected side •• Collapse of the lung on the affected side • • After insertion of a nasogastric tube through the esophagus, it is found in the affected side of the chest.
• Treatment •• Indications for surgery ••• In case of severe breathing problems, children with large hernias of the diaphragm should be operated on in the first days of life ••• For hiatal hernias, surgery can be delayed until the age of 1 year ••• Emergency surgery is indicated for strangulated hernia and bleeding from the stomach •• Surgical treatment. Stages of the operation: ••• Transperitoneal access ••• Reduction of the hernia into the abdominal cavity ••• Closing the hernial orifice (plasty or alloplasty for large defects) ••• Revision of the abdominal organs to identify associated congenital anomalies (diaphragmatic hernia is often accompanied by incomplete intestinal rotation ) ••• Drainage of the affected half of the chest.
• The results of surgery in newborns with diaphragmatic hernias depend on the timing of their detection and the severity of clinical manifestations •• Mortality in the preoperative period reaches 50% •• Postoperative mortality - 12–20%. The cause of death in newborns and infants is most often pulmonary failure ••• With diaphragmatic hernias, the lung on the affected side is often hypoplastic due to compression by the hernia during intrauterine development ••• Relief of respiratory failure in the postoperative period depends on the compensatory capabilities of the healthy lung ••• If the outcome of the operation is favorable, a hypoplastic lung may develop with age.
ICD-10 • Q40.1 Congenital hiatal hernia • Q79.0 Congenital diaphragmatic hernia