Antidepressants are one of the most difficult groups of drugs for pharmaceutical consultation. Often associated with very specific disorders and sold strictly by prescription, they are shrouded in many secrets and speculation. Some patients are afraid of antidepressants, others have too high hopes for them. But both the former and the latter have many questions about how these medications will affect their lives. They ask these questions not only to the attending physician, but also to another person in a white coat - the head of the pharmacy. We have collected answers to the most popular of them in this material to help our readers, if necessary, build a capacious and correct consultation.
Explain in simple terms - how do antidepressants work?
Antidepressants are a group of psychotropic medications that affect the levels of neurotransmitters (they transmit nerve impulses between cells in the human brain), thereby helping to treat depression. We are talking about three hormones: serotonin, dopamine and norepinephrine. According to the prevailing point of view in scientific circles, with depression their concentration noticeably decreases, which is why the interaction between neurons is disrupted. Modern antidepressants help reverse this process, returning the brain to normal functioning. Thanks to this, patients experience the following improvements: improved mood, improved vitality, decreased anxiety and apathy, and normalized sleep and appetite.
Nootropics and Metabolic Aids
The remedies in this group help to get out of a depressive state that has developed against the background of stress, overwork, encephalopathy, the consequences of injuries and poisoning. By improving the blood supply to neurons and energy metabolism within cells, they contribute to the activation of cognitive functions and memory. The most effective drugs in this group:
- Phenibut
- Mexidol
- Aminalon (GABA)
- Piracetam (nootropil)
- Picamilon
- Pyriditol (encephabol)
- B vitamins.
What happens if during treatment the patient stops taking the prescribed drug?
It all depends on the situation. If the withdrawal is abrupt, there is a high risk that the body will not have time to adapt to the new regime, and the side effects will increase exponentially. This is called withdrawal syndrome and can be expressed in different ways. Most often, patients complain of dizziness, headaches, sleep disorders, spasms and tremors in the limbs. There is also a rebound syndrome, in which untimely withdrawal from the drug provokes the return of all the negative symptoms of depression. With gradual withdrawal, such consequences do not occur, so it is extremely important to adhere to the dosage regimen prescribed by the doctor.
SSRI
Venlafaxine and duloxetine block the reuptake of both serotonin and norepinephrine, and both are substrates of CYP2D6.
Venlafaxine (dosage 75-300 mg per day, half-life - 5 hours, active metabolite - desmethylvenflaxine) is characterized by low bioavailability (less than 20%) when taken orally. At low dosages, it is able to inhibit the reuptake of serotonin, and at high doses, norepinephrine, which, however, does not in any way affect its antidepressant potential. Venlafaxine is also capable of partially inhibiting dopamine reuptake.
Duloxetine (dosage 30–90 mg per day) blocks the reuptake of both neurotransmitters equally. As you can already guess, acting only on the reuptake of neurotransmitters, selective inhibitors of this group do not have atropinergic and sedating effects, unlike tricyclic antidepressants. Sometimes patients begin to complain of difficulty urinating, sweating and impaired potency, but this rarely leads to refusal to take medications. These drugs are contraindicated for liver disease, severe hypertension, epilepsy and glaucoma.
Are antidepressants dangerous for the body?
As with any medicine, side effects may occur when taking antidepressants. Most often we are talking about drowsiness (and sometimes, on the contrary, insomnia), inhibition of reactions, hypotension. However, given that on the other side of the scale are often the patient’s thoughts about leaving life or causing other harm to himself, this is not regarded as a serious obstacle.
Some antidepressants are contraindicated for heart diseases (arrhythmia, conduction disorders in the myocardium), but there are drugs that are allowed to be taken even by people who have had a heart attack. A number of such drugs cannot be prescribed for pathologies of the kidneys and liver. Knowing the patient’s health characteristics, the doctor selects the most suitable option for him. Therefore, antidepressants can only pose a danger when self-medicated.
Neuroleptics
Despite the fact that most antipsychotic drugs depress the nervous system, among them there are drugs with antidepressant effects:
- Flupenthixol (fluanxol).
It has an antidepressant effect only when administered in small doses (less than 2 mg per day).
- Aripiprazole.
Effective for depression in bipolar affective disorder and schizitypal disorders.
- Levomepromazine (tizercin).
Prescribed for endogenous depression accompanied by insomnia.
Is it true that once started, depression medications will have to be taken for the rest of your life?
Treatment with antidepressants is not a quick process, and its duration largely depends on the severity of the person’s condition. Typically, the course of taking these drugs lasts at least six months. If no improvement is observed after six months, the doctor may extend the course or change the drug. Therefore, you need to be prepared for the fact that you will have to take antidepressants for quite a long time. However, there is no talk of lifelong treatment: the patient will either begin to recover, and the need for antidepressants will gradually disappear, or will demonstrate resistance to them, and the doctor will choose a different strategy. There is also a WHO recommendation that antidepressants should be taken for at least another 9 months after the symptoms of depression have disappeared.
Antipsychotics for depression and anxiety
Today, drugs such as antipsychotics are actively used in the treatment of depression and neuroses. They eliminate panic fears, anxiety, and normalize sleep patterns.
Doctors classify them depending on their chemical structure.
- Dibenzazepines are necessary to combat psychotic manifestations, they are perfectly combined with other medications, but they have a minimal sedative effect and have quite a few adverse reactions.
- Aliphatic phenothiazines have a greater sedative and calming effect and eliminate sleep problems.
- Phenothiazine derivatives are used in the presence of pain and problems with blood vessels.
- Butyrophenones are drugs that are used in medicine to combat delusional disorders and hallucinations; they have practically no sedative effect.
There are 2 types of antipsychotics: typical and atypical (as well as those with prolonged and non-prolonged action). In the first case, these are drugs that are already a thing of the past; they did a really good job with their main task - relieving psychotic symptoms, but had a fairly large number of undesirable side effects.
In the second case, the use of atypical antipsychotics is more modern. These are the latest generation drugs, antipsychotics, which have virtually no side effects. If drugs have a prolonged effect, this means that they have a long-term effect on the body, for example, for a month.
Does taking antidepressants guarantee a complete cure for depression?
Unfortunately no. Often, the causes of depressive disorders lie not in physiology, but in human psychology, so drug therapy has only a temporary effect, which gradually fades away after discontinuation of the drug. Knowing this, doctors usually use antidepressants as part of a comprehensive treatment that also includes psychotherapy sessions. However, some patients only need medication to recover. On the contrary, they don’t help some people. Depression is a very complex disorder, so doctors select their own treatment methods for each specific case.
“I heard that antidepressants change personality. Will they turn me into a “zombie”?
This is perhaps one of the most common and most ridiculous myths regarding antidepressants. They won't actually change your personality. You will remain the same person, you will be able to work normally, communicate with people around you, you will live a full life - your mood will simply stabilize and become normal. A far-fetched “side effect” in the form of personality changes is not something to be afraid of. You won't become a zombie.
The most important thing is to correctly determine whether you have indications for taking antidepressants and choose the appropriate drugs and dosages. Only a specialist can competently solve these problems. Trust an experienced doctor at the Cordia Clinic, contact us:
Do antidepressants affect your sex life?
Strong antidepressants may indeed not have a very good effect on this delicate area of life in both men and women. Among the side effects of some tricyclic drugs is priapism - a prolonged painful erection not associated with sexual desire. More modern medications (MAO inhibitors) in some cases lead to anorgasmia and decreased sexual desire. This effect of antidepressants is considered a side effect, does not occur in everyone and disappears when the drug is discontinued and treatment is adjusted. Therefore, any sexual disorders that occur should be reported to your doctor immediately.
Tranquilizers
- Bromodihydrochlorophenylbenzodiazepine (phenazepam).
The drug of choice for neurotic conditions with depression and post-stress conditions. That is, in cases where short-term treatment is required.
- Clonazepam.
Strong anti-anxiety and sedative effect. When taken for a long time it causes dependence.
- Alprazolam.
Prescribed for anxiety and depression. Recommended for short courses (no more than 10 days) due to the risk of developing addiction and dependence.
Are antidepressants compatible with alcohol?
During drug treatment of depression, alcohol consumption should be avoided. At the same time, different groups of antidepressants interact with alcohol in different ways. Mixing some (for example, tricyclic antidepressants) with alcohol can lead to serious consequences, including death. More modern drugs are not so dangerous in this regard. But MAO inhibitors, for example, can affect vasoconstriction (and therefore, indirectly, on erection), and can also enhance the effect of strong drinks and provoke, for example, damage to the liver or nervous system. Exactly how the drug interacts with alcohol is always written in the instructions. And in most cases this interaction is undesirable.
Sources
- Lacasse JR, Leo J. Serotonin and depression: a disconnect between the advertisements and the scientific literature // Florida State University College of Social Work, Tallahassee, Florida, United States of America PLoS Med. - 2005. - T. 2, No. 12.
- Rosenbaum JF, Fava M, Hoog SL, et al. Selective serotonin reuptake inhibitor discontinuation syndrome: a randomized clinical trial. Biol Psychiatry 1998 // https://www.uptodate.com/contents/discontinuing-antidepressant-medications-in-adults/abstract/17
- Haddad PM Antidepressant discontinuation syndromes // Drug Safety journal. - 2001. - Vol. 24, no. 3. - P. 183-197. - PMID 11347722.
- American Psychiatric Association. The Truth About Antidepressants // https://www.psychiatry.org/news-room/apa-blogs/apa-blog/2016/03/the-truth-about-antidepressants
- Tarasenko O. A. Side effects of antidepressants // Pharmacist. - 2003. - No. 14. https://www.provisor.com.ua/archive/2003/N14/art_33.php
- WHO Mental Health Program // https://www.who.int/mental_health/mhgap/evidence/depression/q2/ru/
- F Hieronymus et al., Efficacy of selective serotonin reuptake inhibitors in the absence of side effects: a mega-analysis of citalopram and paroxetine in adult depression // Molecular Psychiatry, 2017; doi:10.1038/mp.2017.147
- Rafael Gafoor. Antidepressant utilization and incidence of weight gain during 10 years' follow-up: population-based cohort study // BMJ 2018; 361 https://www.bmj.com/content/361/bmj.K1951
- Megan Brooks. Antidepressants Worsen Sexual Dysfunction and Depression? https://www.medscape.com/viewarticle/870660
- Kucher E. O., Shevchuk M. K., Sivak K. V. Experimental study of the influence of alcohol on the biological effects of antidepressants // Bulletin of St. Petersburg University. – 2010. – Series 11, issue 1. https://vestnik.spbu.ru/pdf10/s11/s11v1_10_S.pdf
Effective drugs for depression
Phenazepam
This is perhaps the most common drug in addiction medicine and psychiatry.
However, it is popular not only because it is highly effective in the treatment of anxiety disorders, but also because it is a dangerous pharmaceutical drug that causes addiction. That is why the duration of the course of treatment and dosage are controlled by the doctor. You cannot buy Phenazepam at a pharmacy without a doctor's prescription. This is a benzodiazepine that affects the central nervous system and is a potent drug. Today, the tranquilizer is used less and less, as it has a fairly large list of side effects, including drug addiction. It has a sedative and hypnotic effect.
Afobazole
An innovative modern drug is used for depression and neurosis. It eliminates anxiety, restlessness, relieves tension and stress, does not cause drowsiness, and has a minimum of side effects. The medication is a neuroprotector, protects nerve cells, stabilizes GABA receptors.
Mexidol
The purpose of antioxidants is to protect the body from dangerous substances that damage cells and adversely affect human health. The drug is prescribed to patients after a head injury, in the presence of abnormalities in the cerebral circulation, or stress. Mexidol is used in the treatment of encephalopathy, ischemic heart disease and VSD.
Magnesium
Our body cannot function normally without magnesium. This substance is involved not only in metabolic processes, but also affects the functioning of the central nervous system. That is why it is necessary to compensate for the existing magnesium deficiency in cases of depressive disorders.
Quetiapine
The drug affects serotonin receptors to a greater extent than dopamine receptors. Therefore, for depression it is prescribed quite rarely, or in minimal doses. Most often used for more severe illnesses, dementia, Alzheimer's or Parkinson's disease. Contraindications are oncology, hypotension, heart attack, diseases of the cardiovascular system and liver.
Amitriptyline
The drug increases the concentration of norepinephrine and serotonin and inhibits their reuptake. It is used in the presence of psycho-emotional disorders, psychosis, anxiety, insomnia, depression. It is not recommended to take if you have binge drinking and alcoholism, gastrointestinal diseases, or pregnancy.
Atarax
Inhibits the work of the central nervous system, is prescribed for mental disorders, psychomotor agitation, nervousness, anxiety, irritability. Do not use during pregnancy or individual intolerance to the components of the drug.
Global trends
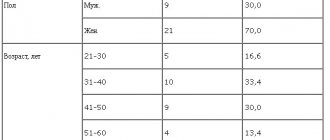
Since the early 2000s, the use of antidepressants has increased in almost all countries. In 2000, residents of Iceland were the most likely to use these drugs: 71 people out of a thousand admitted to regularly using them, and in 2011 this number increased to 106 people per thousand. In Canada and Australia, the figures are not much better: in 2011, 86 and 89 people out of a thousand, respectively, resorted to using medications against depression. The Scandinavians and other Europeans lagged behind, but not by much. Residents of Eastern European countries avoid taking antidepressants constantly, but often use them once (to be honest, this does not make much sense for health). Women are treated for depression more often than men, and bisexuals are treated more often than homosexuals and heterosexuals. For Russia, alas, there is no exact data.
Publications in the media
Depression (D) has many faces in its clinical manifestations, and along with affective, motor, autonomic, obligate, dyssomnia disorders are present, which makes the problem of sleep disorders one of the most pressing in this disease. The term “dyssomnic” reflects the diversity of these disorders, including both insomnic (85–90%) and hypersomnic (10–15%) manifestations. Statistics on the prevalence of sleep-wake cycle disorders in D ranges from 83% to 100%, which is determined by various methodological possibilities for their assessment; in polysomnographic studies this is always 100%.
This obligatory pattern of sleep-wake cycle disorders in D is based on common neurochemical processes. A special place in this regard is occupied by serotonin, disturbances in the mediation of which, on the one hand, play a crucial role in the genesis of D, and on the other, are of great importance in the organization of delta sleep and in the initiation of the rapid eye movement (REM) phase. This also applies to other biogenic amines, in particular norepinephrine and dopamine, the deficiency of which is important both in the development of depression and in the organization of the sleep-wake cycle. The state of the melatonergic system, which determines both the chronobiology of sleep and chronobiological disorders in D., is also important.
To date, there is no complete understanding of the characteristic features of sleep disorders in various forms of depression, although their great phenomenological diversity has long been pointed out. Sleep changes in endogenous depression are characterized by a reduction in delta sleep, a shortening of the latent period of the rapid eye movement (REM) phase, an increase in the density of rapid eye movements (REM) - one of the main phenomena characterizing FBS, and frequent awakenings. In psychogenic depression, the predominance of sleep disturbances with compensatory prolongation of morning sleep in the structure of insomnia is indicated, while in endogenous depression, frequent nighttime and final early awakenings are more often recorded. Patients D show a decrease in the depth of sleep, an increase in motor activity and frequent awakenings, a pronounced reduction in the 4th stage of sleep, against the background of which there is often an increase in the superficial (1st and 2nd) stages of the slow-wave sleep (SMS) phase. The number of transitions from stage to stage increases, which indicates instability in the functioning of the cerebral mechanisms for maintaining sleep stages. In addition, a characteristic feature was an increase in the number of awakenings in the last third of the night.
The phenomenon of “alpha-delta sleep” described in patients D indicates a significant change in the organization of the deepest stages of FMS. It is a combination of delta waves and high-amplitude alpha rhythm (lower in frequency by 1-2 vibrations than in wakefulness) and takes up to 1/5 of the total sleep time. In this case, the depth of sleep turns out to be greater than in stage 2, which is determined by a higher awakening threshold. It is believed that alpha activity in delta sleep is a reflection of the activity of activating cerebral systems, which do not allow somnogenic systems to fully perform their functions. Disruption of the regular distribution of delta activity, as well as a decrease in the amplitude of the delta rhythm and its power, indicate a relationship between the mechanisms of FMS and depression. The special relationship between D and delta sleep is also indicated by the fact that when leaving D, delta sleep is one of the first to be restored. Subsequently obtained facts showed, however, that delta sleep disturbances in depression are more typical for men and are not specific only to depression. Significant fluctuations in the duration of stage 4 sleep associated with age have been established, in particular its significant reduction in the period of maturity and especially in older people.
In depression, changes in the FBS are observed. According to various data, in patients with depression there is a significant variation in the duration of FBS - from 14% to 31%. The most important indicator reflecting the amount of need for FBS is its latent period (LP). The phenomenon of LA contraction in depression has long attracted the attention of researchers. A reduction in FBS latency was regarded by the authors as a sign of increased activity of the devices generating this phase of sleep, and was associated with an increased need for REM sleep. It has been shown that the more pronounced the depression, the more REM movements are collected into “packs”, between which there are long periods without any oculomotor activity. However, according to other data, there is simply an increase in REM density in the first sleep cycles. There are reports that the reduction of the FBS latency is not to the same extent characteristic of different types of depression - a short latency is characteristic only of all primary depressions and is absent in secondary ones. However, it is not determined in any way by other sleep parameters and does not depend on age and the effect of medications. Perhaps these data indicate desynchronization of circadian ri and their shift to an earlier time of day. It is also possible that the characteristic changes in sleep themselves play a role in the pathogenesis of D. Some authors emphasize the connection between the nature and severity of dreams with quantitative and qualitative changes in FBS in patients with D. However, it is quite possible that a decrease in FBS LP is secondary to to insufficient duration of delta sleep in the first sleep cycle, as mentioned earlier.
Since the discovery by Kupfer and Foster of the association of depression with a reduction in the interval between falling asleep and the first episode of FBS in comparison with healthy controls (
.), the relationship between mental disorders and sleep disorders is the subject of intense scientific research. In recent years, as a result of a large-scale meta-analysis, the following conclusions have been formulated. D is usually accompanied by a number of sleep disturbances in comparison with healthy control subjects: 1) an increase in sleep onset latency; 2)increasing the percentage share of FBS; 3) an increase in the density of the BDG; 4) deterioration in sleep continuity; 5) a decrease in the percentage of delta sleep and 6) a reduction in the latent period of FBS. Although the influence of age, gender, and severity of the depressive episode on sleep disturbances remains to be clarified, distinguishing depressed patients from healthy individuals based on sleep indicators does not present great difficulties. However, as shown in the aforementioned meta-analysis, none of the established sleep disorders can reliably differentiate depression from other mental disorders, such as panic disorder, generalized anxiety disorder, obsessive-compulsive disorder, schizophrenia, severe dementia or borderline personality disorder. Moreover, in polysomnography indicators it is not possible to identify clear differences between the subtypes of depression (primary, endogenous, atypical, etc.). Perhaps the most compelling differences concern the differentiation between psychotic and nonpsychotic depression. A few studies have attempted to take the opposite approach, i.e. group mental disorders or their subtypes based on biological markers, but the results do not support qualitative differences and common specific subtypes; only quantitative differences have been identified that support the concept of the “depressive spectrum.”
Several theories have been formulated to explain changes in sleep in untreated patients with major depressive disorder (MDD), the effects of medications on the sleep of such patients, and the effects of sleep manipulations, including total sleep deprivation or sleep deprivation.
There are a number of issues that are only partially resolved:
Are sleep disorders signs of a biological predisposition?
Do they reflect a depressive disorder and will they disappear after the clinical manifestations of a depressive episode are reduced?
Can effective antidepressants correct sleep disturbances found in untreated patients with MDD?
Can we assume that those sleep disorders that can be corrected in this way are primarily associated with depression?
Do drugs affect depression through sleep disturbances, or are the observed effects merely secondary effects?
Is it possible to predict in advance the effectiveness of this therapy 2 weeks after starting it?
Do they reflect the consequences of previous episodes?
Is it necessary to use sleeping pills or is it sufficient to use antidepressants to treat sleep disorders in patients with D?
The situation with neurotransmitters is no less complicated. For example, serotonin (5-hydroxytryptamine (5-HT)) is a major therapeutic target for depression and is important in sleep disorders. It would seem that selective serotonergic drugs can help clarify the relationship between these phenomena. However, the presence of several types of receptors (5-HT1A-D, 5-HT2A-C, 5-HT3 and 5-HT4), each of which has its own agonists and antagonists, not to mention their potential interactions with gamma-aminobutyric acid (GABA) ), norepinephrine (NA) or dopamine (DA), significantly complicates any scheme. Today, sleep research is an important part of the development of new psychotropic drugs, and almost every new drug is carefully studied for its effect on sleep.
Persistent insomnia is associated with a multiple-fold increased risk of developing MDD within 1–3 years, as well as an increased risk of recurrent depressive episode. Mood disorders have a high prevalence but often go unrecognized in people with chronic sleep disorders. Accordingly, today the development of optimal therapy for insomnia is becoming one of the most important health problems in industrialized countries. Because psychotropic medications can improve or impair sleep onset and sleep continuity, there is a need to consider insomnia in the development and selection of antidepressants. It is also known that antidepressants can provoke restless legs syndrome or periodic limb movements syndrome, which leads to worsening insomnia.
The effect of antidepressants on sleep
Monoamine oxidase inhibitors. Phenelzine, a monoamine oxidase inhibitor (MAOI), is able to almost completely suppress FBS after several weeks of therapy in both healthy individuals and patients with MDD. Other MAOIs, such as nialamide, pargylene, and mebanazine, have similar effects on sleep. This suppression of FBS coincides with the onset of the antidepressant effect, suggesting a physiological link between the suppression of FBS and the antidepressant effect. In most cases, MAOIs do not have a particularly pronounced effect on MBS, although these antidepressants are thought to reduce sleep efficiency.
The reversible MAOI moclobemide has polar effects: one study showed that its use increased sleep efficiency and shortened the latency period of FBS in patients with MDD; another study found almost completely the opposite results.
Tricyclic antidepressants . Tricyclic antidepressants (TCAs) differ from MAOIs in their ability to suppress FBS, since when using TCAs, suppression of FBS is observed immediately after the start of taking these drugs. Thus, clomipramine significantly suppresses FBS in control subjects. Imipramine and desipramine also have a significant suppressive effect on FBS, at least in healthy control subjects and animals. However, the effect of TCAs on FBS appears to be less consistent than the effect of MAOIs: long-term studies have documented normal and even elevated levels of FBS. One study in a group of patients with depression revealed an inhibitory effect of amitriptyline on FBS. After discontinuation of TCAs, the phenomenon of PBS rebound is often observed. It is interesting to note that not all TCAs have an inhibitory effect on FBS. For example, trimipramine, iprindole and viloxazine do not have a significant effect on FBS. As a group as a whole, TCAs increase the amount of delta sleep, with the exception of clomipramine. One study of clomipramine in a group of patients with MDD using spectral analysis showed a significant increase in delta waves corresponding to delta sleep. The use of desipramine in patients with MDD has been associated with difficulty falling asleep.
Tetracyclic antidepressants. Mianserin did not affect the duration of FBS in healthy control subjects and patients with MDD. Maprotiline suppresses FBS and increases the amount of stage 2 sleep in healthy control subjects. Both antidepressants can increase delta sleep rates.
Selective serotonin reuptake inhibitors . The selective serotonin reuptake inhibitor (SSRI) fluvoxamine suppresses FBS and increases latency in patients with MDD, but has no significant effect on delta sleep or delta waves as measured by spectral analysis. Paroxetine reduces total sleep time and reduces sleep efficiency in patients with MDD by decreasing FBS and increasing latency. In patients with MDD, the use of fluoxetine is accompanied by an increase in the frequency of awakenings, a decrease in sleep efficiency and a decrease in delta sleep, as well as an increase in the latency period and a reduction in FBS. Treatment of patients with MDD with sertraline is associated with an increase in sleep latency and a reduction in the duration of FBS. Citalopram persistently suppresses FBS, which is combined with the phenomenon of FBS rebound after drug withdrawal. According to spectral analysis, citalopram has no effect on delta waves. Trazodone at a dose of 100–150 mg/day suppresses FBS and increases delta sleep, and also improves subjective ratings of sleep quality, as shown in a group of middle-aged patients with insomnia. In high doses (400–600 mg/day), treatment with trazodone in patients with MDD is accompanied by an increase in total sleep time and delta sleep, but without significant changes in FBS and its latency. Nefazodone reduces arousals and increases sleep efficiency, and stabilizes or even increases FBS time in healthy subjects and patients with MDD; At the same time, a reduction in delta sleep was noted. SSRIs may cause periodic limb movement syndrome.
Serotonin and norepinephrine reuptake inhibitors. The serotonin norepinephrine reuptake inhibitor (SNRI) venlafaxine increases wake time and stages 1, 2, and 3 sleep in healthy subjects. There is a pronounced suppression of FBS and an increase in its latent period.
The noradrenergic and specific serotonergic antidepressant (NASSA) mirtazapine improves sleep in healthy subjects. Mirtazapine reduces the time it takes to fall asleep and increases the depth of sleep. There is also an increase in the latent period of FBS and a reduction in night awakenings. In patients with MDD, the use of mirtazapine improves sleep efficiency and increases total sleep time, while no effect on FBS was detected.
Other antidepressants . A study in young healthy subjects found no evidence of an effect of tianeptine at therapeutic doses (37.5 mg/day) on electroencephalographic (EEG) sleep parameters. Tianeptine has been shown to suppress FBS in healthy subjects and patients with comorbid depression and alcoholism. The same study showed improvement in sleep with tianeptine, as assessed by the Leeds Sleep Questionnaire.
Melatonin and melatonergic antidepressants . Almost all studies have identified certain hypnotic effects of melatonin and, first of all, acceleration of falling asleep. Regarding the antidepressant capabilities of melatonin, there are directly opposite points of view - from complete denial to confident confirmation. Without going into controversy, we emphasize that this new knowledge contributed to the creation of an absolutely new antidepressant in ideology and neurochemistry - agomelatine, which is an agonist of cerebral melatonin receptors of the 1st and 2nd subtypes (primarily in the suprachiasmatic nucleus) and an antagonist of 5-HT2C serotonin receptors. The uniqueness of this antidepressant lies in the fact that its hypnotic effect is not associated with the effect of sedation and occurs already on the 14th day. Of course, like any new pharmacological product, it requires further research, but theoretically its combined antidepressant and hypnotic effects seem to be very significant.
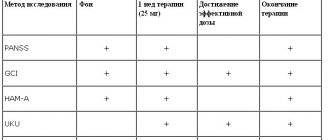
Possibility of using polysomnography to predict the effectiveness of antidepressants
By now, the significance of several such predictors can be debated.
- A short latency period of FBS before the start of therapy (baseline characteristic) correlates with a positive effect.
- For future responders, spectral analysis of electroencephalography (EEG) is characterized by high power of delta waves and low power of alpha, beta and theta waves throughout the night before the start of therapy.
- High REM density before therapy is associated with a poor prognosis, so it is important how quickly REM activity is suppressed during the initial period of therapy. Suppression of REM in the first two nights after starting TCAs has been shown to be associated with a high therapeutic effect. These data have not been confirmed in studies of SSRIs.
Despite their clear value, such prognostic strategies are rarely used in clinical practice.
Conclusion
A number of arguments have been put forward to support the hypothesis of a close connection between sleep dysregulation and the basic factors of depressive disorders:
- almost all patients suffer from sleep disorders (insomnia or hypersomnia);
- patients with chronic insomnia as a monosymptom are characterized by an increased risk of manifestation or relapse of depression;
- For the most part, pharmacological drugs effective for depression affect sleep, usually correcting the initial sleep disturbances in patients;
- Sleep deprivation is an effective therapy that provides relief from depressive symptoms in 50% of cases, although this effect is short-lived.
Most antidepressants suppress FBS quite quickly (TCAs, SSRIs, SNRIs and HASSA) or approximately 2 weeks (MAOIs) after initiation of therapy. However, there are a number of exceptions (trimipramine, iprindole, tianeptine, viloxazine, nefazodone). Sleep depth may increase (agomelatine, trazodone, nefazodone, mirtazapine), remain unchanged (most MAOIs, fluvoxamine), or decrease (clomipramine, desipramine, phenelzine, fluoxetine, paroxetine, sertraline, venlafaxine). The effects of long-term use of antidepressants are, in principle, poorly studied, although a tendency towards a gradual reduction of the initial effects has been found.
Here are some theories that help explain some facts.
The first theory is based on Borbely's general model of sleep regulation, in which the "S" process represents the delta wave EEG of sleep corresponding to deep sleep (roughly corresponding to stages 3 and 4 in hypnograms for visual assessment). One hypothesis is that depression leads to a decrease in slow wave sleep (SWS) or delta wave spectral power, which in turn frees up space for REM and stimulates a more rapid onset of REM at night with increased REM and decreased latency. One approach to confirm this hypothesis involves measuring the sleep EEG spectral power response in response to antidepressant therapy. A study using spectral analysis was performed in which a comparative assessment of the effects of trazodone and citalopram in patients with MDD was carried out. The aim of the study was to look for parallels between potential changes and timing of clinical improvement. This study shows that delta waves do not change significantly during the first 5 weeks of therapy, and the timing of changes in other waveforms does not correlate with clinical changes in patients' condition. Moreover, antidepressants varied significantly in their effect on sleep continuity, ranging from worse to better. Accordingly, the role of MVS restoration remains unclear.
The second theory is FBS pressure. It has been shown that almost all drugs that cause a pronounced and persistent reduction in the time of FBS and are characterized by the phenomenon of rebound of FBS after their withdrawal are effective means of treating endogenous depression. Antidepressant therapy, as well as sleep deprivation (partial, FBS-specific or complete), electroconvulsive therapy or psychotherapy act in parallel with the improvement or through the correction of pathological sleep disorders in patients with depression. It has been established that during depression, LP decreases and, regardless of the mechanism underlying this phenomenon, it must be increased; the percentage of FBS, on the contrary, increases with depression, so it should be reduced. However, it is obvious that the general rule for an effective antidepressant—reduction of FBS and increase in LP—has many exceptions. Therefore, it can be assumed that either more than one mechanism is involved and only some antidepressants are consistent with this rule, or changes in sleep parameters during antidepressant therapy are only indirectly related to their effectiveness against depression.
Although it is likely that sleep and its underlying neurophysiological mechanisms are closely related to the mechanisms of depression, these disorders do not appear to be identical, and we cannot argue that successful treatment of depression necessarily requires correction of sleep disturbances. At the same time, sleep cannot be considered as simply a concomitant phenomenon; this is contradicted by the frequent association of depression with sleep disturbances, changes in sleep structure, and modifications in sleep parameters during antidepressant therapy. However, sleep disturbances may not be a necessary component in the development of depression.
Thus, disturbances of the sleep-wake cycle in depression are diverse and include insomnia and hypersomnia. The “purer” the depression, the more likely it is to identify fairly characteristic changes in the structure of night sleep. Of great interest are not only the antidepressant effects, but also some non-pharmacological techniques that act on the depressive radical - sleep deprivation and phototherapy, which have proven to be quite effective and safe. The discovery of the commonality of some biochemical mechanisms of depression, sleep disorders and circadian rhythms further increases interest in this problem, especially since this opens up the possibility of new integrated approaches to the treatment of sleep disorders in depression.
Treatment for depression without a prescription
Don’t think that you can buy medications for stress and depression without prescriptions. Also, do not be mistaken about self-medication. Depression is not just a bad mood or blues, but a real mental disorder that can be treated not only with medications, but also with long-term work with psychologists, psychotherapists or psychiatrists. If you regularly have thoughts of suicide, have no appetite, or have disrupted sleep patterns, you should consult a specialist.
However, you can improve your mood and avoid illness if you use the following as preventative measures:
- sport;
- trips;
- breathing exercises;
- creative activities;
- bathing in hot baths;
- drinking green tea;
- aromatherapy;
- meditation.
Physical education and physical exercise help synthesize new neural connections that have a beneficial effect on the functioning of the nervous system and a person’s mood. Just 30 minutes of exercise a day and you won't be in a bad mood. Dancing is no less beneficial for the activity of brain cells. Art therapy helps to get rid of negative emotions, relieves stress, breathing exercises help to better supply the brain with oxygen. Green tea or tomato juice will help cope with stress. Inhaling essential oils also regulates mood. A hot bath will help you relax and normalize your emotional state before bed.
Indications for use
If you experience a bad mood and apathy, increased irritability and mood swings for several days, these are not signs of a disorder. We can talk about depression as a clinical disease when the described symptoms last continuously for at least 2 weeks in a row. Another important symptom is a lack of interest in life, a complete loss of joy and positive emotions.
Along with these symptoms, indications for the use of antidepressants are:
- increased anxiety;
- bulimia;
- anorexia;
- insomnia, severe sleep disturbances;
- somatoform disorders;
- compulsive overeating;
- loss of sexual desire.
Tricyclic antidepressants: list
These drugs have the most pronounced therapeutic effects. They were developed earlier than others, so they have been well studied for several decades. The list of tricyclics includes:
- "Amitriptyline" is a drug with a strong sedative effect. Used to treat both mild depression at the initial stage and severe disorders.
- "Anafranil" is a drug with a balanced effect and is better tolerated by patients compared to the previous one. It eliminates increased anxiety well and is used to treat clinical depression in mild, moderate and severe forms.
- Melipramine is a drug used to treat apathetic depression.