Qatar of the upper respiratory tract
is the medical term for a buildup of mucus in the back of the nose, throat, and sinuses.
Doctors sometimes call catarrh of the upper respiratory tract postnasal drip
. Often, catarrh of the upper respiratory tract is the result of diseases such as allergies or acute respiratory viral infections. It usually goes away once the person is cured. However, some patients may have symptoms of chronic catarrhal inflammation that persist for months or even years. This is usually not a cause for concern, but it can be unpleasant to live with.
Qatar of the upper respiratory tract
Upper respiratory tract catarrh (URRT) is the most common disease that is caused by viruses and affects the respiratory tract. Acute respiratory infection (ARVI) is popularly called a cold.
Causes
There are many causative agents of CVDP. The most common groups of viruses:
- rhinoviruses;
- reoviruses;
- influenza and parainfluenza;
- adenoviruses, etc.
The wide distribution of respiratory viruses is explained by the methods of their transmission:
- by contact - for example, you can become infected with the virus by shaking hands (direct route of infection) or using shared household appliances (indirect route of infection);
- by airborne droplets - when talking, coughing or being in a room with a sick person.
Causes
There are many potential causes of postnasal drip. They include:
- change in weather conditions
- eating spicy food
- hay fever or allergic rhinitis
- non-allergic rhinitis
- viruses
- sinus infections
- nasal polyp
- gastroesophageal reflux (GER)
- gastroesophageal reflux disease (GERD)
- hormonal changes during pregnancy
- some medications
Symptoms
From the moment the virus enters the gate of infection - the mucous membrane of the nasopharynx and larynx - until the development of acute catarrh of the upper respiratory tract, 1-3 days pass. During the incubation period, symptoms usually manifest as a sore throat and pain, as well as a dry cough. Body temperature rarely exceeds normal.
As the virus multiplies, it enters the blood and causes symptoms of general intoxication:
- headache;
- muscle and joint pain;
- fever;
- fatigue and weakness;
- dry or wet cough;
- sneezing.
When the virus enters the body, the immune system forms a response with the production of antibodies. Their work begins with cleansing the blood of the virus and reducing symptoms. The epithelium of the upper respiratory tract is the last to be freed from the influence of viruses.
Uncomplicated catarrh of the upper respiratory tract in adults is manifested by a runny nose and expectoration (wet cough). After 10–14 days, symptoms usually disappear.
Sputum with a purulent-mucous admixture is a sign of a bacterial infection.
How does infection and development of acute respiratory infections occur?
The source of infection is always people sick with ARVI, who pose the maximum danger to others on the 3-4th day of illness, when the release of viruses into the environment is especially intense5.
The main routes of transmission of respiratory tract infections are airborne droplets and contact4.
- Airborne
Viruses and pathogenic bacteria are contained in the saliva and sputum of the patient. When coughing and sneezing, droplets of nasal mucus and sputum quickly spread in the environment and, together with the air, enter the respiratory system of a healthy person. In confined spaces and public transport, the infection spreads especially quickly, so limiting visits to public places significantly reduces the likelihood of catching ARVI4.
- Contact
The mucus released when the patient sneezes and blows his nose ends up on his hands surrounding household items. Viruses settle on dishes, the patient’s desk, door handles, handrails of public transport, books, and furniture used by an infected person. From these objects, pathogenic microorganisms fall onto the hands of healthy people, and then when they touch the face they are carried into the nose and mouth. It has been proven that contact transmission of viruses is more important than airborne transmission5. Therefore, frequent hand washing can be called one of the main ways to prevent respiratory tract infections5.
How does the disease develop? Once on the mucous membrane of the nasal cavity, viruses invade its cells and begin to multiply intensively. Their number reaches a critical level within 1-3 days (incubation period), after which the first symptoms of the disease begin to appear. In this list:
- Rhinitis is inflammation of the mucous membrane of the nasal cavity.
- Pharyngitis is an inflammation of the pharynx, soft palate, uvula and lymphoid tissue of the pharynx.
- Epiglottitis is an inflammation of the upper part of the larynx and epiglottis, which closes the entrance to the trachea during swallowing.
- Laryngitis is inflammation of the larynx.
Most often, colds are associated with viral nasopharyngitis - a combined inflammation of the mucous membrane of the nasal cavity and pharynx. If the disease is mild and does not lead to complications, doctors usually write “ARVI” or “acute upper respiratory tract infection” in the patient’s card, without specifying the localization of the inflammatory process2,3.
Up to contents
Diagnostics
Upper respiratory tract catarrh is treated by a family doctor or internist. At the appointment, he collects an anamnesis of the disease, examines the patient, auscultates (listens) the lungs, and also recommends a general blood test.
Differential diagnosis helps optimize treatment and prevent the development of complications. KVDP can be distinguished from a number of other diseases by the following characteristics:
- Influenza is characterized by a rapid onset of the disease, fever, and the development of a serious condition of the patient.
- Parainfluenza has a calmer course, but if the larynx is affected in small patients, there is a danger of swelling and suffocation.
- The adenovirus does not start as quickly as the flu and affects the lymphatic system and liver. The infection can cause conjunctivitis and runny nose.
Respiratory syncytial viruses attack the bronchi and lungs. If the trend is unfavorable, bronchopneumonia may develop.
In the summer, symptoms of stomach and intestinal disorders are common. In this case, the doctor diagnoses rotavirus infection.
In addition, the symptoms of upper respiratory tract catarrh are similar to the following diseases:
- infectious mononucleosis;
- sore throat;
- measles;
- AIDS.
Treatment
There is no specific therapy for viral infections. But treatment tactics are aimed at reducing and alleviating the patient’s condition:
- bed rest;
- frequent and abundant drinking of warm drinks;
- taking tableted vitamins and microelements (as prescribed by a doctor);
- vasoconstrictor nasal drops;
- antipyretic drugs (paracetamol, ibuprofen).
Antibiotics for viral infections are strictly contraindicated due to their negative effect on the immune system and intestinal microflora. Antibiotic therapy is prescribed by a doctor in case of a bacterial infection.
Features of treatment
Colds, especially during the off-season, are common. But if upper respiratory tract catarrh occurs in children more than 6–8 times a year, and an adult gets sick more than four times a year, this is a reason to consult an immunologist to determine the state of general immunity.
Viral infections in pregnant women always pose a potential threat to both the fetus and the woman herself. Therefore, if you become infected with the virus, you must consult not only a general practitioner, but also be observed by a gynecologist.
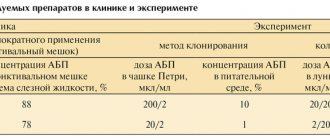
Publications in the media
Diseases caused by viruses of the Adenoviridae family are characterized by high body temperature, inflammation of the mucous membranes of the respiratory tract and eyes, as well as hyperplasia of the submucosa and regional lymph nodes. Adenovirus infection is highly contagious. The most commonly observed varieties • ARVI with severe fever (mostly affecting children) • ARVI in adults • Viral pneumonia • Acute adenoviral tonsillitis (develops in children, especially in the summer after swimming) • Acute follicular conjunctivitis • Epidemic keratoconjunctivitis (mainly in adults) • Intestinal infections ( enteritis), often complicated by mesenteric adenitis and invaginations. Frequency. A very commonly reported infection, it accounts for 2–5% of all respiratory tract infections. More often observed in newborns and children.
Etiology • Pathogens - DNA-containing viruses of the genus Mastadenovirus, 60–90 nm in size; about 80 serotypes (serovar) are known • The main causative agents of human lesions •• Infections of the lower respiratory tract (bronchiolitis, pneumonia) - serotypes 1, 2, 3, 5, 6, 7, 21 •• Pharyngoconjunctivitis - serotypes 1, 2, 3, 4, 6, 7, 14 •• ARVI - serotypes 3, 4, 7 •• Gastroenteritis - serotypes 2, 3, 5, 40, 41 •• Conjunctivitis - serotypes 2, 3, 5, 7, 8, 19, 21 • • Epidemic keratoconjunctivitis - serotypes 8, 19, 37 •• Hemorrhagic cystitis - serotypes 11, 21 •• Meningoencephalitis - serotypes 2, 6, 7, 12, 32 •• Disseminated lesions - serotypes 5, 34, 35, 39 •• Cervicitis and urethritis - serotype 37 •• Lesions associated with celiac disease - serotype 12.
Epidemiology. Human adenoviral infections are widespread and account for 5–10% of all viral diseases; most of the lesions occur in childhood (about 75%); while 35–40% are registered in children under 5 years of age, the rest - under the age of 14 years. The main routes of transmission are airborne and contact.
Pathomorphology • Varies among different serotypes, in severe pneumonia a large number of intranuclear inclusions can be identified • Bronchiolitis obliterans is possible.
Clinical forms • Qatar of the respiratory tract • Pharyngoconjunctival fever • Membranous conjunctivitis • Tonsillopharyngitis (adenoviral tonsillitis) • Intestinal form (viral diarrhea, gastroenteritis) • Mesadenitis • Viral pneumonia.
Clinical picture
• Qatar of the respiratory tract is the most common form, characterized by pronounced catarrhal changes in the respiratory tract (rhinopharyngitis, laryngitis, tracheitis, bronchitis) with moderate manifestations of general intoxication.
• Pharyngoconjunctival fever. It is characterized by a long-term temperature reaction (up to 2 weeks in the absence of intercurrent diseases and complications) and symptoms of pharyngitis: sore throat, rare cough, bright hyperemia of the tissues of the pharynx with large “grain” of the follicles of the mucous membrane; the respiratory tract is involved in the process to a small extent.
• Membranous conjunctivitis. Usually seen in adults and older children. Unilateral (less often bilateral) conjunctivitis with a fibrinous film on the surface of the mucous membrane (usually the lower eyelid), accompanied by severe swelling of the surrounding tissues, pain, hyperemia and injection of the vessels of the conjunctiva of the eye, fever. The respiratory tract is not involved in the process. This clinical form is characteristic only of adenoviral infection (an etiologically detailed diagnosis can be made without laboratory confirmation).
• Tonsillopharyngitis. Typical for preschool children. It is characterized by the development of inflammatory changes in the tissues of the pharynx and palatine tonsils with the formation of sore throat (catarrhal, fibrinous, less often [with the addition of a bacterial infection] purulent).
• Intestinal form (gastroenteritis, viral diarrhea). It is characterized by the development of moderately severe gastroenteritis, manifested by nausea, vomiting, loose stools without pathological impurities. Body temperature is subfebrile. Possible simultaneous involvement of the respiratory system in the process (catarrhal nasopharyngitis or laryngotracheitis).
• Mesadenitis. Characterized by the development of abdominal syndrome with abdominal pain and temperature reaction. Sometimes it is possible to palpate enlarged mesenteric lymph nodes. In rare cases, symptoms of an “acute abdomen” occur, simulating an attack of acute appendicitis.
• Viral pneumonia. An independent clinical form with typical symptoms of acute pneumonia (intoxication, signs of pulmonary heart failure). The exudative component is pronounced (multiple rales of various sizes throughout all pulmonary fields, cough with copious sputum, etc.). X-rays reveal widespread inflammatory changes in the lungs. This clinical form does not exclude possible bacterial superinfection, therefore antimicrobial therapy is necessary.
Research methods • Isolation of the pathogen by inoculation into cultures of human epithelial cells; the material being studied is discharge from the nose, pharynx, conjunctiva, feces, etc. • Detection of Ag viruses in cells by immunofluorescence microscopy, as well as staging of RSC, hemagglutination inhibition reaction (HRI) and reaction to neutralize the cytopathic effect in cell culture • X-ray diagnostics: bronchopneumonia in severe respiratory infection • In severe or atypical cases, a biopsy (of the lung or other tissue).
TREATMENT
Regime • Outpatient, with the exception of seriously ill young children, patients with epidemic keratoconjunctivitis and young children with severe pneumonia • Bed rest for the period of elevated body temperature.
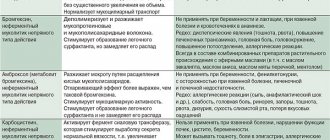
Drug therapy - symptomatic treatment • If necessary - paracetamol 0.2-0.4 g per dose 2-3 times / day (10-15 mg / kg / day). It is not recommended to take acetylsalicylic acid • Antitussives and expectorants • HA (topically) - for conjunctivitis (after consultation with an ophthalmologist).
Course and prognosis • The disease goes away on its own with virtually no complications • Severe course and death are possible among children and patients with impaired immunity.
Prevention • Live oral vaccines against adenovirus types 4 and 7, coated with a capsule that protects from digestion in the intestine, reduce the incidence of acute respiratory viral infections • Frequent hand washing is mandatory for staff of various institutions and family members of the patient.
ICD-10 • A08.2 Adenoviral enteritis • A85.1+ Adenoviral encephalitis (G05.1*) • A87.1+ Adenoviral meningitis (G02.0*) • B30.0+ Keratoconjunctivitis caused by adenovirus (H19.2*) • B30.1+ Conjunctivitis caused by adenovirus (H13.1*) • B34.0 Adenoviral infection, unspecified • J12.0 Adenoviral pneumonia • J02.8 Acute pharyngitis caused by other specified pathogens • J02.9 Acute pharyngitis, unspecified • J03.9 Acute tonsillitis, unspecified.
Application. Mesadenitis (acute mesenteric lymphadenitis) is inflammation of the lymph nodes located in the mesentery of the small intestine; observed mainly in children and adolescents; symptoms resemble acute appendicitis. Etiology: viral infection, as well as bacteria of the genus Yersinia. Clinical picture : abdominal pain (can be severe), nausea, vomiting and fever; some patients experience additional signs of viral infection (for example, pharyngitis and myalgia). The diagnosis is usually made by laparotomy for suspected appendicitis. Treatment: when Yersinia is isolated, antibiotics are prescribed. ICD-10. I88.0 Nonspecific mesenteric mesadenitis.
Frequently asked questions about upper respiratory tract catarrh
Why is upper respiratory tract catarrh dangerous?
If catarrh of the upper respiratory tract is carried on the legs, a person weakened by the virus can suffer complications in the form of serious diseases of the cardiovascular system, bronchi and lungs.
How long to treat upper respiratory tract catarrh?
Qatar of the upper respiratory tract usually heals on its own within 10–14 days and does not require special treatment. The doctor may prescribe symptomatic treatment: antipyretic, vasoconstrictor drops and herbal medicines to thin the sputum. If a bacterial infection occurs, the healing process is delayed. In this case, hospital treatment may be required.
Which doctor treats catarrh of the upper respiratory tract?
A cold is usually treated by a family doctor or general practitioner. But if complications arise, consultation with a specialist is required: an otolaryngologist - for sinusitis, sore throat and otitis media; pulmonologist - for complications of the bronchopulmonary system.