Acute pyelonephritis is a nonspecific inflammatory pathology that affects the renal parenchyma. The disease is manifested by nausea, which often ends with vomiting, fever, pain, discomfort when emptying the bladder, and frequent urination. Lack of medical care can lead to sepsis, renal failure, nephrogenic arterial hypertension, interstitial pneumonia, meningitis and even death. Therefore, at the first signs of inflammation, you should consult a doctor. They will be diagnosed and treated immediately.
Description of the disease
Pathology develops as a result of the introduction of pathogenic bacteria into the body or a rapid increase in the population of opportunistic microorganisms already living in it. They either directly penetrate the renal structures or are transported by the blood stream from the primary infectious focus. A violent inflammatory process develops, affecting almost the entire pyelocaliceal system and interstitial tissues.
Most often, acute pyelonephritis is diagnosed in women due to anatomical features - a short and wide urethra. It is often detected in children, because their immune system has not yet fully formed and cannot adequately withstand the attack of infectious pathogens.
Stages of pyelonephritis
Despite the rapid course of the infectious-inflammatory process in the kidneys, separate stages of its development are distinguished. Each is characterized by fairly pronounced pathomorphological changes in the renal structures.
At the initial stage of pathology, abundant exudate accumulates in the tissues, consisting of a watery, slightly cloudy serous fluid saturated with proteins. This leads to a still insignificant increase, tension of paired organs, and perivascular infiltration. If the patient ignores the first discomfort of the initial stage and does not seek medical help, then the pathology progresses with subsequent purulent-destructive kidney damage.
At the next stage, apostematous pyelonephritis develops - an acute purulent-inflammatory process with the formation of multiple abscesses in the parenchyma, pronounced signs of general intoxication of the body. In the absence of adequate therapy, the size of small pustules increases, they merge to form a single large lesion, or carbuncle. The likelihood of an abscess caused by a breakthrough of the abscess and penetration of pathological exudate into nearby renal structures increases significantly. They are irreversibly damaged, and connective tissues devoid of any functional activity are formed in their places.
Risk factors
Doctors identify a number of factors that can predispose to kidney damage by acute pyelonephritis. The likelihood of its development increases in the presence of the following pathological conditions:
- congenital or acquired anomalies of the structure of the kidneys, urinary ducts, urethra, bladder;
- immunodeficiency conditions, including HIV;
- urolithiasis;
- diabetes mellitus, in which pathogens grow and multiply especially intensively due to the presence of glucose;
- previous traumatic injuries of the spinal cord, organs located in the abdominal cavity;
- any inflammatory chronic disease in which infectious foci form;
- prostatic hyperplasia, prostatitis.
Elderly people are predisposed to acute pyelonephritis, including due to the presence of a number of chronic diseases of internal organs at this age. Also, its development can be triggered by surgery or medical manipulation.
Ascending infection towards the kidneys
Most often, pathogenic and opportunistic microorganisms enter the kidneys from the urethra through the bladder and urinary ducts. With weakened immune defenses, this process occurs at a rapid pace.
Because of the wide, short urethra, women are much more likely to have kidney damage than men. It is located very close to the vagina, anorectal area. Therefore, even with proper intimate hygiene, the risk of infectious pathogens moving towards the kidneys in women is very high.
In men, the development of the inflammatory process is usually caused by the presence of some kind of formation in the urethra, which prevents the normal flow of urine. It stagnates, which becomes a favorable environment for the proliferation of pathogenic bacteria. Men with kidney stones, proliferation of prostate tissue, urethral stricture, benign or malignant neoplasms in the organs of the urinary system are predisposed to acute pyelonephritis. Tumors and other factors that lead to narrowing of the urethra become an impetus for stagnation of urine in women.
Vesico-ureteral reflux
Vesico-ureteral reflux is a pathological condition characterized by the backflow of a small amount of urine into the renal pelvis. It is caused by its obstructed outflow into the bladder through the ureters.
Vesico-ureteral reflux is most often diagnosed in childhood and adolescence. Its danger lies in an acute attack with painful symptoms and quickly occurring complications. It is in childhood that there is a high risk of rapid replacement of functionally active tissues with connective tissues with pathological scarring. A number of factors predispose to pyelonephritis, including anatomical features:
- lower hydrostatic pressure (the volume of blood flowing through the kidney);
- inability to control urination in early childhood;
- lack of intimate hygiene skills;
- predisposition to weakened immunity.
Young children do not inform their parents about the first uncomfortable sensations and do not know how to interpret them. Therefore, pyelonephritis is diagnosed in them not at an early stage, but at a late stage, when severe complications have already arisen.
Another feature of the development of the disease in childhood and adolescence is the descending route of infection. Pathogenic microorganisms are transported by the blood stream from inflammatory foci formed in the upper respiratory tract. There are known cases where the trigger for pathology was carious teeth and a common ARVI.
Causes of upper respiratory tract diseases
Despite the similarity of manifestations, acute respiratory infections differ in the nature of their origin. They can be caused by different pathogens.
1.Viruses
They are the culprits of the “cold” in the vast majority of cases3 and then it is called ARVI (acute respiratory viral infection). About 40% of all such infections are associated with rhinoviruses1, which mainly affect the mucous membrane of the nose, nasopharynx and pharynx. They are followed by human coronaviruses, which cause nasopharyngitis, and parainfluenza viruses, which are responsible, among other things, for the development of laryngitis - inflammation of the larynx1. Adenoviruses and respiratory syncytial viruses are less common, as are other almost 200 types of viruses that cause respiratory tract infections4.
In approximately 1-2% of cases, viruses “can contribute to the activation of bacterial microflora”: they penetrate into the cells of the mucosa, cause their death, disrupt the functioning of the ciliated epithelium and the mechanisms of cleansing the respiratory tract, reduce local immunity and thereby create favorable conditions for the development of bacteria. In this case, the inflammation becomes viral-bacterial4.
2.Bacteria
Sometimes acute respiratory infections are initially bacterial in nature. Infectious agents are usually streptococci, pneumococci, Haemophilus influenzae, and Moraxella2. Bacterial infections of the upper respiratory tract often “cling” to young children with undeveloped immunity, elderly people whose bodies are weakened by health problems, and patients with primary and secondary immunodeficiency.
3. Atypical pathogens of acute respiratory infections
This group includes chlamydia, mycoplasma, pneumocystis, legionella and other microorganisms. The respiratory diseases they cause are rare, so we will not dwell on them.
Up to contents
Infectious agents
The most common infectious agent of acute pyelonephritis is Escherichia coli. It is a gram-negative rod-shaped bacterium that lives in the lower intestine. The development of the inflammatory process can be provoked by the following microorganisms:
- staphylococci;
- Proteus;
- Klebsiella;
- enterococci;
- pseudomonas;
- streptococci;
- Pseudomonas aeruginosa.
A disease caused by the introduction of pathogenic or opportunistic fungi into the renal structures is diagnosed much less frequently.
In case of ascending infection in the urine, E. coli is especially often detected by biochemical methods or microscopy. But if surgical intervention, traumatic injury and medical manipulation led to pathology, then Klebsiella, Proteus, and Pseudomonas aeruginosa are detected.
Diagnosis of respiratory viral infections
If after a few days you cannot cope with the cold on your own, you should consult a doctor. Modern diagnostic methods make it possible to identify the type of virus at an early stage and prevent complications.
At the Anapa Diagnostic Center you can undergo examinations, undergo fluorography, and take sputum, blood and urine tests. If a bacterial infection is suspected, a bacteriological culture will be performed. Having identified the causative agent of the disease, effective treatment will be prescribed. Call and make an appointment; the earlier treatment is started, the lower the risk of complications.
Clinical picture in women
The nature and severity of symptoms of acute pyelonephritis varies depending on the stage of the infectious-inflammatory process. Its acute course is characterized by the following symptoms:
- thickening, darkening of urine, the presence of blood streaks and purulent impurities in it;
- body temperature above subfebrile values, its sharp decrease and subsequent rise during the day;
- burning sensation when emptying the bladder, pain, pain;
- nausea leading to vomiting;
- headaches.
With severe kidney damage, the pain radiates, is felt in the lumbar region, and intensifies with pressure.
How is the treatment carried out?
Acute respiratory viral diseases are treatable. The best results are achieved with an integrated approach and early exposure to the pathogen. In typical cases, the pathology begins with a feeling of discomfort, sore nose and throat, sneezing, and runny nose. Gradually, the intensity of symptoms increases, manifestations of intoxication occur, body temperature rises, and a nonproductive cough appears.
The basis for diagnosing acute respiratory infections is the clinical picture. To establish the type of inflammatory process and the nature of the pathogen, laboratory tests are used. If the pathology is of microbial origin, tests will confirm leukocytosis. With a viral infection, lymphocytosis appears. If there is severe wheezing in the lungs, a chest x-ray is indicated. It eliminates pneumonia.
Diagnosis and treatment of the disease is provided by a therapist, family doctor, pediatrician (if an acute respiratory infection occurs in a child). If complications develop from the ENT organs, consultation with an otolaryngologist is indicated. If conjunctivitis occurs, the help of an ophthalmologist is necessary. The duration of treatment is from 7 to 14 days. You should not resort to self-medication or use alternative medicine; such actions can lead to serious complications.
Treatment of acute respiratory infections consists of eliminating symptoms and increasing the body's immunity. The use of such means is shown:
- antipyretic drugs;
- anti-inflammatory drugs;
- sprays for sanitizing the nasal cavity and facilitating breathing;
- antitussives or expectorants;
- vitamins.
The dosage of medications and the regimen of use are determined by the doctor. Clinical recommendations for acute respiratory infections include bed rest, proper rest, and drinking plenty of fluids.
Symptoms of acute pyelonephritis in men
Since in men the pathology develops mainly due to narrowing of the urethra, tissue proliferation, and the presence of tumor-like formations, the symptoms of pyelonephritis are complicated by signs of the primary disease:
- suppression of appetite leading to weight loss;
- weakness, fatigue;
- difficulty urinating;
- soreness in the lower back;
- a feeling of incomplete emptying of the bladder, constant thirst;
- frequent urge to urinate.
As in women, in men acute pyelonephritis occurs with signs of general intoxication of the body. These include high fever, chills, and excessive sweating. If dark blood streaks or admixtures of fresh blood appear in the urine, this may indicate displacement of the stone.
Leading signs of the disease in childhood
Due to the imperfection of the immune system and the characteristics of blood circulation, the disease in childhood is especially severe. It is manifested by increased body temperature, chills, and fever. The child suffers from attacks of nausea and vomiting, girdle pain, weakness, drowsiness, and dehydration. Due to dyspeptic disorders, there is no appetite.
Any child’s complaint of discomfort in the kidney area should be a signal to immediately seek medical help. It is impossible to make a diagnosis and carry out proper treatment on your own. Using data from a number of laboratory tests, the doctor will determine the nature of the infectious pathogens and prescribe the appropriate antibiotics.
Prevention of respiratory diseases
Prevention of ARVI is aimed at increasing immunity. There are many known folk ways to increase the body's defenses: hardening, a diet rich in vitamins, and the use of natural phytoncides, for example, garlic.
In order not to become infected, it is necessary to take precautions: maintain a safe distance, reduce contact during periods of epidemics, wash your hands more often, ventilate the premises, dress according to the weather, avoiding hypothermia.
Vaccination provides the most effective protection against viruses. It is necessary to get vaccinated against influenza every year. You can get a pneumococcal vaccine to prevent severe pneumonia.
Clinical manifestations of pyelonephritis in pregnant women
During pregnancy, the female body is exposed to high stress. Due to the constantly growing uterus, the functioning of internal organs may be disrupted. In combination with hormonal fluctuations and weakened immune defenses, this often causes the development of acute pyelonephritis, especially in the second and third trimesters.
The main cause of infectious and inflammatory damage to the kidneys in pregnant women is strangulation of the ureters by the growing uterus. As a result of disruption of the full outflow of urine, favorable conditions are created for an increase in the population of pathogenic microorganisms. Often, pyelonephritis develops against the background of cystitis, an acute or chronic inflammatory lesion of the mucous layer of the bladder.
PNEUMONIA
Pneumonia
- an acute infectious disease characterized by focal damage to the respiratory parts of the lungs with intra-alveolar exudation, detected by objective and x-ray examination, expressed in varying degrees by a febrile reaction and intoxication.
Clinically significant is the division of pneumonia into community-acquired
and
nosocomial (hospital, in-hospital)
. This division of pneumonia has nothing to do with the severity of their course. The main and only criterion for differentiation is the environment in which pneumonia developed.
Nosocomial pneumonia
- pneumonia that develops in a patient no earlier than 48 hours after hospitalization and was not in the incubation period.
Main pathogens
Community-acquired pneumonia
Pneumococcus remains the most common causative agent of community-acquired pneumonia (Table 2). Two other microorganisms are M.pneumoniae
and
C.pneumoniae
- often occur in young and middle-aged people (up to 20-30%), and their etiological role in patients of older age groups is less significant (1-3%).
L.pneumophila
is a rare causative agent of community-acquired pneumonia, but legionella pneumonia ranks second (after pneumococcal) in terms of mortality.
H.influenzae more often causes pneumonia in smokers, as well as against the background of chronic bronchitis. E.coli
and
K.pneumoniae
(less commonly other representatives of the
Enterobacteriaceae
) are found, as a rule, in patients with risk factors (diabetes mellitus, congestive heart failure, etc.).
The likelihood of staph pneumonia ( S. aureus
) increases in older people or in people who have had the flu.
Table 2. Etiology of community-acquired pneumonia
| Pathogen | Detection rate, % |
| S. pneumoniae | 30,5 |
| M. pneumoniae | 12,5 |
| C. pneumoniae | 12,5 |
| L.pneumophila | 4,8 |
| H.influenzae | 4,5 |
| Family Enterobacteriaceae | 3,0 |
| S. aureus | 0,5 |
| Other pathogens | 2,0 |
| Pathogen not detected | 39,5 |
Nosocomial pneumonia
The etiology of nosocomial pneumonia is dominated by gram-negative microflora of the Enterobacteriaceae family, P.aeruginosa
(Table 3).
Table 3. Etiology of nosocomial pneumonia
| Pathogen | Detection rate, % |
| P. aeruginosa | 25-35 |
| Family Enterobacteriaceae | 25-35 |
| S. aureus | 15-35 |
| Anaerobes (usually in combination with gram-negative bacteria) | 10-30 |
| H.influenzae | 10-20 |
| S. pneumoniae | 10-20 |
There is a special type of nosocomial pneumonia - ventilator-associated pneumonia, the etiology of which depends on the length of the patient's stay on mechanical ventilation. With the so-called early VAP (development in the first 4 days of being on a ventilator), the most likely pathogens are S.pneumoniae, H.influenzae, S.aureus
(MSSA) and other representatives of the normal microflora of the oral cavity.
The development of late VAP (more than 4 days on mechanical ventilation) is associated with P.aeruginosa, Acinetobacter
spp., members of the
Enterobacteriaceae
, and less commonly MRSA.
Choice of antimicrobials
When treating patients with community-acquired pneumonia, a differentiated approach should be taken to the choice of antimicrobial agents, taking into account age, severity of the condition, the presence of concomitant diseases, location of the patient (at home, in the general ward of a hospital, in the ICU), previous antimicrobial therapy, use of glucocorticoids, etc. (Table . 4).
Table 4. Choice of antibiotics for community-acquired pneumonia
| Features of the nosological form | Main pathogens | Drugs of choice | Alternative drugs |
| Non-severe course, age up to 50 years without concomitant diseases. Treatment at home | S.pneumoniae M.pneumoniae H.influenzae C.pneumoniae | Amoxicillin Modern macrolides | Doxycycline Levofloxacin Moxifloxacin |
| Non-severe course in patients with risk factors for ARP or gram-negative microflora (age 65 years and older, cardiovascular or bronchopulmonary diseases, AMP therapy within the previous 3 months, etc.). Treatment at home | Cefuroxime axetil, amoxicillin/clavulanate + macrolide, doxycycline or monotherapy with a third-fourth generation fluoroquinolone (levofloxacin, moxifloxacin) | Ceftriaxone IM | |
| Non-severe course, age under 60 years and/or with concomitant diseases. Treatment in the general department | S.pneumoniae M.pneumoniae H.influenzae Enterobacteriaceae Legionella spp. C. pneumoniae | Benzylpenicillin, ampicillin + macrolide | II-III generation cephalosporins + macrolide Amoxicillin/clavulanate, ampicillin/sulbactam + macrolide Levofloxacin Moxifloxacin |
| Severe course regardless of age. Treatment in the ICU | S. pneumoniae Legionella spp. Enterobacteriaceae S.aureus C.pneumoniae | Amoxicillin/clavulanate, ampicillin/sulbactam + macrolide III-IV generation cephalosporins + macrolide Levofloxacin + cefotaxime or ceftriaxone | Fluoroquinolones (iv) Carbapenems |
Prognostically, the rapid initiation of antimicrobial therapy, no later than 4 hours after diagnosis, is very important.
When choosing AMPs in a patient with nosocomial pneumonia
the nature of the department in which he is located (general profile or ICU), the use of mechanical ventilation and the time of development of VAP are taken into account (Table 5). Empirical therapy is planned based on local data on the sensitivity of likely pathogens. Sputum examination is mandatory, and it is desirable to obtain material by invasive methods with quantitative assessment of the results, and blood culture.
Table 5. Choice of antibiotics for nosocomial pneumonia
| Features of the nosological form | Most common pathogens | Drugs of choice | Alternative drugs |
| Pneumonia that occurred in general wards, without risk factors or early VAP | S.pneumoniae Enterobacteriaceae H.influenzae Less common: Pseudomonas spp., S.aureus | Amoxicillin/clavulanate Ampicillin/sulbactam Cephalosporins II-III generation (except ceftazidime) | Fluoroquinolones Cefepime Cefoperazone/sulbactam |
| Late ventilation pneumonia or pneumonia that occurred in general departments, in the presence of risk factors | Enterobacteriaceae Pseudomonas spp. S. aureus (including MRSA) | Cefepime Ceftazidime, cefoperazone + aminoglycoside Imipenem + aminoglycoside | Fluoroquinolones Cefoperazone/sulbactam, ticarcillin/clavulanate or piperacillin/tazobactam + aminoglycoside Vancomycin |
Risk factors: recent abdominal surgery, aspiration - anaerobes; coma, head injury, diabetes, chronic renal failure, influenza, “IV drug addicts” - S.aureus
;
large doses of glucocorticoids, cytostatics, neutropenia - Legionella
spp.,
P.aeruginosa, Aspergillus
spp.;
long stay in the ICU, treatment with corticosteroids, antibiotics, bronchiectasis, cystic fibrosis - P.aeruginosa
,
Enterobacter
spp.,
Acinetobacter
spp.
Routes of administration of antimicrobial drugs
In the treatment of outpatient forms of community-acquired pneumonia, preference should be given to oral antibiotics. However, in severe infections, AMPs must be administered intravenously. In the latter case, stepwise therapy is also highly effective, which involves switching from parenteral to oral administration. The transition should be made when the course of the disease stabilizes or the clinical picture improves (on average 2-3 days from the start of treatment).
Duration of therapy
For uncomplicated community-acquired pneumonia, antibiotic therapy can be completed once stable normalization of body temperature is achieved. The duration of treatment is usually 7-10 days.
If there are clinical and/or epidemiological data on mycoplasma, chlamydial or legionella pneumonia, the duration of antibacterial therapy should be longer due to the risk of relapse of infection - 2-3 weeks.
Duration of AMP use for complicated community-acquired pneumonia
and
nosocomial pneumonia
are determined individually.
In any case, the persistence of individual clinical, laboratory and/or radiological signs is not an absolute indication for continuation of antibacterial therapy or its modification. In most cases, these signs resolve spontaneously over time.
Consequences and complications
The cause of complications is late seeking medical help, as well as improper treatment. Acute pyelonephritis is especially dangerous for pregnant women and people with diabetes. The disease develops rapidly in them, and many pharmacological drugs with antibacterial effects are contraindicated. In such cases, adequate therapy with gentle agents under close medical supervision is required.
The more severe the inflammation, the higher the likelihood of sepsis. Pathogenic microorganisms quickly grow and multiply, and the infectious process spreads to healthy kidney structures. Toxic products of their vital activity accumulate in the systemic bloodstream. Blood poisoning occurs - a life-threatening condition that, if not treated promptly, can result in death.
Complications of ARVI and their danger
In a person with good immunity, acute respiratory diseases go away within a few days, especially if the body is helped to cope with viruses. It is recommended to drink more water, rinse your nose, and gargle. Symptoms can be stopped - bringing down the temperature above 38 degrees, fighting a runny nose, treating the throat with emollients.
However, in some cases, severe viral intoxication or the addition of a bacterial infection can cause complications. Most often, complications arise in the respiratory system and lead to other diseases: tonsillitis, sinusitis, rhinitis, pharyngitis, laryngitis. Often, ARVI develops into bronchitis, otitis media, sinusitis, and pneumonia.
More serious consequences of ARVI threaten people with weakened immune systems. A respiratory infection may not be limited to the respiratory tract and spread to other organs. Severe complications include: pyelonephritis, nephritis, rheumatoid arthritis, neuroinfection.
Diagnosis of acute pyelonephritis
An experienced doctor will suspect a developed disease only based on the patient’s complaints. To confirm the diagnosis, the following measures are required:
- Collection of anamnestic data. The doctor asks the patient about what preceded the onset of symptoms, when pain and other discomfort are most common. The presence of chronic pathologies of the urinary system in the patient also helps to determine the diagnosis.
- Examination of the patient. An acute course of the infectious process is indicated by high fever, chills, and increased sweating.
- Studying the results of laboratory, including biochemical studies.
- Study of instrumental research data.
The patient is required to undergo general clinical tests, Zimnitsky's test, and urine examination using the Nechiporenko method.
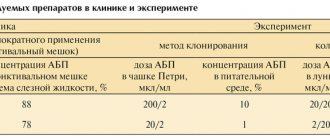
In a laboratory setting, urine is cultured into culture media. The shape, size, and number of formed colonies are used to judge the type of infectious agents, the severity of the inflammatory process, as well as the sensitivity of pathogenic bacteria to antibiotics, which are most often used in the complex therapy of acute pyelonephritis.
The information content and reliability of laboratory test data directly depends on the correct collection of urine. Be sure to pre-wash the genitals and dry them. The collection of biological material is carried out in a special sterile compact container with a tightly screwed lid.
The presence of an infectious kidney lesion is indicated by a high level of leukocytes and the presence of a large number of microorganisms. The erythrocyte sedimentation rate in blood tests is also increased. Indirect confirmation of the development of acute pyelonephritis is alkalinization of urine, increased quantitative content of proteins and glucose.
Acute respiratory viral infection (ARV)
This term refers to a symptom complex that includes such typical manifestations of a “cold” as nasal congestion, rhinorrhea, sneezing, sore throat and cough [1].
ARVI is caused by over 200 different viruses, most often rhinoviruses, of which there are more than 100 types. Other etiological factors include adeno-, coronaviruses, parainfluenza viruses, respiratory syncytial viruses (RS viruses), as well as influenza viruses A, B and C. A less common cause of the development of this symptom complex is enteroviruses, Epstein-Barr virus and herpes (hepressimplex ). In typical cases, the clinical picture is dominated by signs of catarrhal inflammation of the upper respiratory tract, while the phenomena of general intoxication are moderate and may even be absent. The incubation period for ARVI depends on the type of virus and usually lasts from 48 to 72 hours [1]. Clinical manifestations of the disease in most cases bother the patient for no more than one week, but in about a quarter of cases their duration increases to 2 weeks. If these symptoms persist beyond this period, a secondary bacterial infection may be suspected - most often sinusitis or pharyngitis. Complications also include acute bacterial otitis media (in approximately 2% of ARVI cases) and persistent cough due to bronchospasm [1].
In the acute period of ARVI, local manifestations of the disease include swelling of the nasal mucosa, exudation and signs of pharyngitis in the form of erythema of the pharynx and pharynx. Symptoms of exudative pharyngitis do not always occur and can be a manifestation, in particular, of adenoviral infection [1].
Most adults experience ARVI 2–4 times a year, while children usually experience symptoms of the disease 6–8 times a year. In smoking patients, the frequency of ARVI and the severity of its symptoms increase [2]. The disease is more common in the autumn and winter seasons, which helps to differentiate it from seasonal allergic diseases, which usually dominate in the spring and early autumn periods.
The mechanism of transmission of a viral infection from person to person is usually associated with the transfer of viral particles from the skin of the hands to the nasal mucosa (hand-nose-hand contact route). In some cases, viruses are transmitted through airborne droplets by sneezing and blowing your nose [3]. Treatment of ARVI is usually symptomatic, usually prescribed when complications occur (for example, signs of a secondary bacterial infection) and symptoms are poorly tolerated. The use of nasal decongestants, rinsing the throat and nose with a warm saline (mineral) aqueous solution, and antitussive drugs are recommended. Antipyretics are usually effective and are prescribed when symptoms are severe. The use of acetylsalicylic acid must be strictly regulated. The drug is used with caution not only in children, but also in adult patients due to the risk of Reye syndrome, especially in acute respiratory viral infections caused by influenza and herpes viruses. Antibiotic therapy for ARVI should not be considered as a standard treatment method even if signs of a bacterial infection appear, therefore the prescription of antibacterial agents should be justified. The use of large doses of ascorbic acid for acute respiratory viral infections has received the support of a number of practicing physicians, but scientific evidence of the effectiveness of such therapy has not yet been obtained. The use of drugs containing echinacea is not accompanied by a decrease in the incidence of the disease, nor a decrease in its duration and severity, i.e., their effectiveness is comparable to placebo [4]. To date, there is no convincing evidence that the use of antiviral drugs for this pathology (unlike influenza, see below) has a significant positive effect. A number of researchers indicate the effectiveness of pleconaril, however, despite the fact that the drug can reduce the duration of symptoms of the disease, it is not recommended for free clinical use [5]. Prevention of viral transmission is achieved primarily through sanitary and hygienic measures. Thorough hand washing throughout the day and after contact with sick patients is considered important. The effectiveness of using fabric masks treated with special antiviral agents, as well as intranasal instillation of interferon α-2, has been proven [5].
Today, the most popular drugs prescribed for symptomatic purposes for ARVI are antipyretics (usually paracetamol or ibuprofen), as well as decongestants (for example, phenylephrine). The release of combination drugs containing fairly high concentrations of paracetamol (0.6–1.0 g) and phenylephrine (10.0–12.2 mg) allows for effective symptomatic treatment of patients with both average and increased body weight. The drug Lemsip belongs to this category of medicines. The absence of antihistamines in its composition allows you to use Lemsip without the risk of developing unwanted reactions in the form of drowsiness and lethargy. The therapeutic effect after taking the drug appears within 15–20 minutes and lasts 4–6 hours. It is believed that the duration of the course of self-treatment is on average 5 days. Lemsip is effective as an antipyretic; it also reduces other main symptoms of the disease: rhinorrhea, nasal congestion, cough and sore throat, as well as pain.
Pharyngitis
Pharyngitis can accompany the symptoms of ARVI, but can also manifest itself independently [6]. Etiological factors for pharyngitis include viral or bacterial agents, the most important of which is considered to be group A β-hemolytic streptococcus (GABHS). It has been established that GABHS rarely causes an infectious disease in the first 2 years of life, however, among children 5–10 years old, their role in the development of such pathology increases significantly. In children, GABHS is responsible for a third of all cases of pharyngitis. Studies in groups of students showed that 25% of cases of pharyngitis were caused by streptococcus, and in 38% of cases the disease was of a viral nature [6]. Over the age of 35 years, streptococcal pharyngitis occurs in only 5% of all patients with pharyngitis [5].
Other causes of pharyngitis in children and adults include adenoviruses, RS viruses, rhinoviruses, coronaviruses, influenza and parainfluenza viruses, Epstein-Barr virus, human herpesvirus and Mycoplasma neumoniae. Relatively rarely, the pathogens are Neisseriagonorrhoeae, Neusseriameningitidis, Haemophilus. influenzae, Corynebacterium diphtheriae and various anaerobes.
Based on the clinical picture, it is quite difficult to talk about the supposed etiology of pharyngitis, however, the sudden onset of the disease with high fever, the appearance of signs of swelling of the mucous membrane of the pharynx and uvula are most often a manifestation of streptococcal infection [5]. Less commonly, such pharyngitis is caused by the Epstein-Barr virus, herpes, adeno- and enteroviruses.
Streptococcal pharyngitis requires antibiotics. The use of penicillin or aminopenicillins for 10 days is usually recommended [9]. In case of allergy to β-lactams, they are replaced with macrolides (erythromycin, azithromycin or clarithromycin). It is important to be sure that the disease is caused by streptococcus, since in rare cases, pharyngitis can be a manifestation of an anaerobic infection (usually initially localized in the oral cavity) and progress to Lemierre's syndrome (pharyngitis complicated by jugular vein thrombosis and anaerobic sepsis). In this case, macrolides are ineffective because, unlike penicillins, they do not act on anaerobes. Adequate antibiotic therapy helps reduce the duration of the disease, prevents the spread of the pathogen, the appearance of complications, such as peritonsillar and retropharyngeal abscesses, rheumatic fever, but is not able to prevent the development of glomerulonephritis.
False croup
The term “false croup” refers to acute laryngotracheobrochitis in children of early (usually from 3 months to 3 years) age. The peak of the disease occurs in the 2nd year of life. The usual cause of “false croup” is a viral infection. The disease occurs with varying degrees of severity and severity of clinical symptoms; in mild cases there may be only moderate signs of catarrhal inflammation. In some children, relapses of croup symptoms may occur whenever signs of ARVI appear [6].
The most common cause of this disease is parainfluenza virus type 1, but similar manifestations occur during infection with influenza virus, PC virus, adenovirus, mycoplasma, and rhinovirus [6]. In patients, the first signs of inflammation of the upper respiratory tract appear, a barking cough, then a hoarse voice with the rapid development of stridorous difficulty breathing. Shortness of breath may become severe. Symptoms of the disease sometimes appear in waves, usually improving during the day. It is believed that with “false croup,” swelling of the walls of the respiratory tract is accompanied by less severe respiratory disorders than with infectious epiglottitis, the development of which is associated with a high risk of sudden obstruction of the upper respiratory tract [6].
Treatment of “false croup” is usually supportive and includes inhalation of moist cold air, administration of drugs containing racemic adrenaline. Although data on the use of glucocorticosteroids are conflicting, their use is thought to be feasible. If the patient does not have signs of a bacterial infection, antibiotic therapy is not prescribed.
Bronchitis
Bronchitis is an acute infectious disease with inflammation localized in the walls of large-diameter airways, which is caused by both viruses and bacteria. Bronchitis can occur in initially healthy patients, in which case its manifestations may resemble mild pneumonia. In patients with chronic respiratory diseases (for example, chronic obstructive pulmonary disease, bronchiectasis), the etiology and clinical picture of acute bronchitis differ significantly from those observed during the development of bronchitis in healthy people. Issues of prevention and treatment of acute bronchitis in this category of patients require separate consideration.
In initially healthy people, the cause of acute bronchitis in 40% of cases is viruses (usually adenoviruses, influenza A and B viruses, coronavirus, rhinoviruses, herpes simplex viruses, RS viruses and parainfluenza viruses). The etiological role of bacteria in the development of bronchitis is difficult to establish due to the inability to draw a clear line between infection and colonization. Bacterial pathogens of acute bronchitis usually include Haemophilus influenzae and pneumococcus. M. pneumoniae can cause up to 10% of cases of acute bronchitis, and relatively recent studies have identified the etiological significance of Moraxella catarrhalis and Chlamydophilapneumoniae[7].
Patients with acute bronchitis complain of a cough with the release of mucopurulent sputum, low-grade fever, prolonged burning sensations in the chest, discomfort behind the sternum (the latter symptoms indicate the spread of inflammation in the distal direction). The patient may experience hemoptysis (acute bronchitis is considered the most common cause of mild hemoptysis in the population), shortness of breath is usually moderate, and dry rales are sometimes heard on auscultation in the lungs.
The diagnosis of acute bronchitis is based on the identification of the above clinical symptoms in the absence of radiological signs of pneumonia. Sputum analysis with Gram stain can detect many polymorphonuclear cells and, in some cases, identify bacteria.
Therapy is mainly supportive in nature. Cough suppressants (if it is excessive and poorly tolerated) and antipyretics are used; It is recommended to drink plenty of fluids. Despite many studies, there is currently no clear data on the effectiveness of antibiotics for this disease, and therefore their use should not be routine. It is recommended to conduct educational conversations with patients about methods of treating the disease and the possibility of developing antibiotic resistance with uncontrolled use of antibiotics.
Many patients with acute bronchitis may develop postinfectious bronchospasm, which is characterized by a persistent dry cough with wheezing and usually lasts 4–6 weeks after signs of acute infection have resolved. For diagnosed bronchospasm, brochodilators are used, and sometimes inhaled glucocorticosteroids are used. Such symptoms are accompanied by clinical and functional signs of airway hyperresponsiveness, and in some cases turn out to be the onset of bronchial asthma. Evidence has been obtained that children with a history of multiple episodes of acute viral bronchitis have an increased risk of developing various chronic respiratory diseases (including bronchial asthma) in adulthood [10].
Flu
Influenza is an acute respiratory infection caused by RNA viruses A and B types [8]. Compared with influenza B virus, infection with influenza A virus increases the risk of severe disease with high mortality. Annual changes in the surface antigens of viruses are accompanied by epidemic outbreaks, which usually begin in the second half of autumn and can continue until early spring. A decrease in the effectiveness of anti-infective immune mechanisms contributes to the severe course of the disease in patients with cardiac or respiratory pathology, in the elderly and during pregnancy.
The incubation period for influenza usually lasts 2 days. The spread of the virus occurs through airborne droplets, as well as through the transfer of infected secretions during household contacts.
The influenza A virus can cause the disease together with other pathogens, in particular the RS virus, and especially in older people - the parainfluenza virus. The virus exhibits affinity for the mucous membrane of the respiratory tract. Its infection leads to desquamation of the respiratory epithelium, cellular degeneration, edema and recruitment of mononuclear phagocytes to the area of inflammation.
In more than 50% of patients with influenza, the course is subclinical [8]. The typical clinical picture is characterized by the sudden onset of fever, runny nose, severe myalgia, weakness and headache. The duration of the acute period is usually 3 days. As the first symptoms subside, respiratory complaints begin to dominate: dry cough, burning sensations in the chest, which can persist for several weeks. Laboratory and physical findings are nonspecific, and diagnosis is made by the presence of typical clinical symptoms during epidemic outbreaks. The use of serological diagnostic methods (ELISA, determination of the level of antibodies to hemagglutinin, cultural virological method) helps to confirm the suspected diagnosis. The disease is more severe in smokers, elderly people, children of the first year of life, pregnant women and patients with diseases of the cardiovascular and respiratory systems.
Viral infection may be complicated by the development of secondary bacterial pneumonia. The influenza virus alters mucociliary clearance, which promotes bacterial colonization on the walls of the respiratory tract and affects the functional activity of immunocompetent cells (in particular, polymorphonuclear cells and macrophages). Respiratory complications of influenza include bronchiolitis obliterans, airway hypersensitivity, exacerbation of chronic bronchitis, primary viral pneumonia and secondary bacterial pneumonia. With the development of primary viral pneumonia, the clinical manifestations of the disease persist beyond the usual period (more than 3 days), and their progression is noted with the development of a dry or productive cough and severe shortness of breath. In this case, the appearance of bilateral infiltrative shadows on a radiograph is associated with the risk of a fatal outcome of the disease.
The development of secondary bacterial pneumonia follows a different scenario. 3-4 days after the disappearance of the main symptoms of influenza, the clinical picture of pneumonia develops (usually lobar). Its most common pathogens are pneumococcus, Haemophilus influenzae, intestinal gram-negative bacteria and Staphylococcus aureus.
Other complications of influenza include myocarditis and pericarditis, epilepsy, neuritis, coma, transverse myelitis, toxic shock and acute renal failure [8].
Treatment of influenza is mainly symptomatic and includes antipyretics, bed rest, and drinking plenty of fluids. Taking amantadine in the first 24–48 hours from the onset of an illness caused by the influenza A virus can lead to an improvement in its course. This drug is also recommended as a prophylactic agent during epidemics in patients at high risk of the disease (100 mg twice a day for the entire duration of the epidemic). In patients with renal failure, the dose of the drug should be reduced. Complications of this therapy include confusion (3–7% of cases). The amantadine derivative rimantadine is also effective for the treatment and prevention of disease caused by the influenza A virus. The drug has less effect on the functions of the central nervous system than amantadine and is prescribed once a day, because it has a long half-life. A new class of antiviral drugs, neuraminidase inhibitors, has begun to be used as a prophylactic and therapeutic agent for influenza A and B virus infections. Zanamivir or oseltamivir, prescribed within 36–48 hours of the onset of the disease, reduces the duration of the symptomatic period [11].
Annual influenza vaccination is indicated for elderly patients, as well as patients who are likely to have exacerbations or progression of existing chronic diseases. When choosing a vaccine, information about the strain of the virus that caused the epidemic is important. If an outbreak of influenza occurs in closed communities among non-immunized patients, preventive antiviral therapy and vaccination should be prescribed as early as possible. Prophylactic use of antiviral drugs should continue for 2 weeks after vaccination [11].
Instrumental studies
Instrumental diagnostics are necessary not only to detect kidney damage. It is carried out to determine the localization of the pathological process, the degree of its severity, as well as factors predisposing to the development of acute pyelonephritis. The most informative results are the following instrumental studies:
- Ultrasound. Using ultrasound, it is possible to accurately assess the density of paired organs, their shape and size. Acute inflammation is indicated by abnormal values of these diagnostic criteria and an uneven decrease in echogenicity.
- CT. Computed tomography allows you to obtain an x-ray picture in the form of thin layer-by-layer sections.
- Excretory urography. A diagnostic technique aimed at examining all organs of the urinary system. They are clearly visualized on photographs due to the preliminary intravenous administration of a contrast agent.
- Cystography. The study helps to identify vesicoureteral reflux, which provokes the reverse reflux of urine. It consists of an X-ray examination of the bladder, previously filled with a contrast agent.
Differential diagnosis is also carried out to exclude pathological conditions that manifest similar symptoms, such as renal failure.
Diagnostics
Diagnosis of acute respiratory infections is based mainly on clinical symptoms of inflammation of various parts of the respiratory tract and the results of a medical examination. Given the predominantly mild course of the cold, no additional research is required. Virological diagnosis is usually not carried out, the nature of the pathogen remains unspecified - acute respiratory tract infections do not require specific treatment4,5.
Bacteriological analysis of throat swabs and rapid tests for group A beta-hemolytic streptococcus make it possible to differentiate common viral sore throats and pharyngitis from dangerous bacterial diseases that require immediate antibiotic therapy4,5. Bacteriological examination is also indicated in case of complications development and lack of effect from the antibiotics used4.
Up to contents
Treatment methods for acute pyelonephritis
When determining individual therapeutic tactics, the doctor takes into account the nature and severity of the symptoms of acute pyelonephritis, the severity, age of the patient, and the presence of concomitant diseases.
Treatment is outpatient only for pathology detected at an early stage of development. In other cases, the patient is hospitalized for therapy under the supervision of medical personnel. This is also necessary if there are signs of general intoxication of the body - fever, chills, nausea, vomiting, and a dangerous drop in blood pressure.
The leading method of treatment is a course of antibiotics. To increase the effectiveness of therapy, you must adhere to the following medical recommendations:
- frequent consumption of water acidified with lemon juice, weakly brewed tea to force the elimination of pathogenic bacteria in the urine;
- compliance with bed rest to minimize the risk of spread of the infectious process to healthy tissues and organs;
- optimal temperature conditions, absence of drafts;
- emptying the bladder as often as possible, which often requires taking diuretic (diuretic) drugs.
Simultaneously with acute pyelonephritis, the pathology that caused its development is treated. Treatment of gynecological diseases, prostatitis, prostatic hyperplasia is performed. It is aimed at the rehabilitation of chronic infectious and inflammatory foci of any location and (or) restoration of optimal urine outflow.
When choosing the most effective antibiotic for a particular patient, the doctor is guided by the results of bacteriological urine culture. Its effect can be enhanced by drugs from other clinical and pharmacological groups, for example, antimicrobial agents, uroseptics, including those with herbal active ingredients. Self-selection of antibiotics is ineffective, since pathogenic bacteria gradually develop resistance (resistance) to such medications. And this will lead to the progression of the disease and the development of complications.
If conservative therapy is ineffective and a large purulent focus has formed in the renal structures, surgical treatment is performed. The doctor chooses the most gentle method, aimed at excision of the minimum possible amount of tissue. Only in emergency situations associated with irreversible damage to the organ is it completely removed.
The help of surgeons is often required to eliminate the cause of inflammatory kidney damage. For example, with a pronounced narrowing of the urethra, proliferation of prostate tissue, or the presence of a neoplasm.
EXacERBATION OF CHRONIC BRONCHITIS
Chronical bronchitis
- a disease associated with prolonged exposure to nonspecific irritants (tobacco smoke, etc.) on the respiratory tract, accompanied by hypersecretion of mucus and inflammatory and degenerative changes in the bronchi and lung tissue. The key symptom of the disease is a chronic productive cough observed for at least 3 months over 2 consecutive years, with the exclusion of other diseases/pathological conditions (tuberculosis, congestive heart failure, etc.).
Exacerbation of chronic bronchitis
is accompanied by increased cough, shortness of breath, an increase in the volume of sputum produced, its purulent nature and/or an increase in body temperature. Bacterial and viral infections are responsible for exacerbations of chronic bronchitis in 1/2-2/3 of cases. Other causes of exacerbation of the disease may be allergens, air pollutants, etc.
Main pathogens
Among the bacterial pathogens of exacerbations of chronic bronchitis
H.influenzae, S.pneumoniae
and
occupy a key position .
In special clinical situations (age over 65 years, concomitant diseases, severe bronchial obstruction - FEV1 less than 50% of the required values, constant separation of purulent sputum),
P.aeruginosa, S.aureus
, and enterobacteria acquire a certain etiological significance. About 30% of infectious exacerbations of the disease are caused by influenza/parainfluenza viruses, RSV, rhinoviruses, and coronaviruses.
Choice of antimicrobials
When choosing AMPs, it is necessary to take into account the patient’s age, the severity of bronchial obstruction syndrome, the frequency of exacerbations, the presence of concomitant diseases, the use of glucocorticoids and AMPs (Table 1).
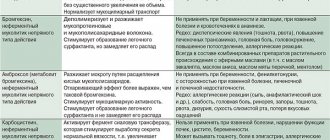
Table 1. Selection of antimicrobial drugs for exacerbation of chronic bronchitis
| Amoxicillin Doxycycline | Amoxicillin/clavulanate Azithromycin Clarithromycin Levofloxacin Moxifloxacin | ||
| Increased shortness of breath, increased volume and purulence of sputum. Age 65 years and older and/or severe bronchial obstruction (FEV1 < 50%), frequent exacerbations (from 4 times a year), concomitant diseases, exhaustion, long-term glucocorticoid therapy, disease duration more than 10 years | H.influenzae (the proportion of β-lactamase-positive strains increases) S.pneumoniae M.catarrhalis Sometimes Enterobacteriaceae | Amoxicillin/clavulanate Levofloxacin Moxifloxacin | |
| Constant separation of purulent sputum, frequent exacerbations | H.influenzae S.pneumoniae M.catarrhalis Enterobacteriaceae P.aeruginosa | Ciprofloxacin | Antipseudomonal β-lactams Aztreonam |
Due to the fact that exacerbation of chronic bronchitis in most cases is not severe, preference should be given to AMPs for oral administration. In cases of severe exacerbation in debilitated patients or those in hospital, parenteral administration of antimicrobial agents may be required. The duration of antibiotic therapy is 7-14 days.