Classic symptoms of chronic heart failure (CHF) are shortness of breath, swelling, and fatigue/fatigue. Fluid retention in the body, volume overload and the formation of edema syndrome in most cases lead to hospitalization and death in patients with CHF (Fig. 1) [1, 2].
Dyspnea
is a manifestation of high pressure in the left ventricle (LV), stagnation of blood in the venous bed of the pulmonary circulation, leading to a decrease in gas exchange in the lungs and irritation of the respiratory center.
The appearance of shortness of breath is also facilitated by the accumulation of excess fluid in the serous cavities (abdominal, pleural), which complicates the excursion of the lungs. In some patients, shortness of breath may be paroxysmal in nature, turning into an attack of suffocation, especially at night ( paroxysmal nocturnal dyspnea
).
The reasons for its occurrence are a rapid and pronounced deterioration in the contractile function of the LV myocardium, an increase in venous blood flow to the heart and pronounced stagnation in the pulmonary circulation. Shortness of breath when bending the body forward (bendopnea)
during the first 30 s (usually when removing or putting on shoes) is a manifestation of increased venous return and filling of the left chambers of the heart, the right atrium, wedging of the pulmonary capillaries, especially in persons with initially high filling pressure of the heart chambers [ 3, 4].
Along with shortness of breath, patients with CHF are often bothered by a non-productive cough
that occurs in a horizontal position, mainly at night or after physical activity. Its occurrence is explained by prolonged stagnation of blood in the lungs, swelling of the bronchial mucosa and irritation of the corresponding cough receptors. Peripheral edema in the early stages of the disease is localized in the area of the feet, ankles and appears in the afternoon after a prolonged stay in an upright position, and as CHF progresses, it spreads to the area of the legs, thighs, lower back, and sacrum, increasing in the evening.
Possibilities for correcting edema syndrome
In order to alleviate symptoms and reduce the severity of signs of fluid stagnation, according to domestic and European recommendations, diuretics must be prescribed. These recommendations apply to absolutely all groups of patients, regardless of LV ejection fraction (LVEF) [1, 5, 6]. In cases of cardiac decompensation, mineralocorticoid receptor antagonists (MCRA) are added to complex diuretic therapy to increase diuresis and overcome refractoriness to thiazide and loop diuretics, which are prescribed in high doses (150–300 mg/day) for 1–3 weeks. until compensation is achieved. During the period of compensation of cardiac activity, AMKR is used in small doses (12.5–50.0 mg/day) as neurohumoral modulators, which more completely block the renin-angiotensin-aldosterone system (RAAS) and thereby improve the course of the disease and the prognosis of life of patients with CHF [1, 5, 7] (Fig. 2).
Espero, KS
Espero is an insecticide with a long protective period for reliable control of different types of pests on a wide range of crops. Reliable control of hidden, sucking and leaf-eating pests throughout the entire period of harmfulness
Mechanism of action: Espero insecticide contains two active ingredients:
- Alpha-cypermethrin - affects calcium metabolism in synapses and sodium-potassium channels, disrupts the function of the nervous system. This leads to a significant excess release of acetylcholine during the passage of a nerve impulse. Poisoning manifests itself in damage to the motor centers and in severe agitation. It has a long residual effect, as well as repellent and antifinding properties. Effective at all stages of insect development.
- Imidacloprid - has a contact and gastric effect. Blocks protein receptors of nerve cells of the central nervous system, which leads to the cessation of transmission of nerve impulses. The pest loses the ability to move, stops feeding and dies within 24 hours.
Advantages:
- The period of protective action is at least 14 days (depending on weather conditions and pest infestation).
- High initial speed of action of the drug
- Destruction of especially dangerous types of pests, incl. brown marmorated bug, bread ground beetle, meadow moth, polyphagous cutworm, moth and others
- Highly effective in conditions of outbreaks of mass reproduction of harmful insects
- Low application rates.
Instructions for using Espero insecticide:
| Application rate of the drug l/ha | Culture | Harmful object | Method, processing time | Waiting period (number of treatments) |
| 0,15-0,25 0.15-0.25 (A) | Winter wheat | Bread ground beetle | Spraying of seedlings The consumption of working fluid for ground application is 100-200 l/ha. when applied by air 25-50 l/ha | 20(2) 20(1-2)(A) |
| 0.1 0.1 (A) | Wheat | Bug bug, cereal aphids, wheat thrips, grain beetles, cereal flies | Spraying during the growing season. The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 20(2) 20(1-2)(A) |
| 0,1 | Wheat, barley | Bread fleas | Spraying of seedlings The consumption of working fluid for ground application is 100-200 l/ha. | 20(2) |
| 0.1 0.1 (A) | Barley | Cereal aphids, thrips, cereal flies, lechs | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 20(2) 20(1-2)(A) |
| 0,15-0,2 | Corn | Gnawing cutworms | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.15-0.2 0.15-0.2 (A) | Corn | Corn stem borer, bollworm, leafhoppers | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.15 0.1-0.15 (A) | Corn | Meadow moth, aphids | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.2 0.1-0.2 (A) | Corn | Brown marmorated bug | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.2 0.1-0.2 (A) | Sunflower | Cabbage bollworm, cotton bollworm | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.15 0.1-0.15 (A) | Sunflower | meadow moth | Spraying of seedlings The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.15-0.2 0.15-0.2 (A) | Peas | Pea moth | Spraying during the growing season The consumption of working fluid for ground application is 200-300 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.15 0.1-0.15 (A) | Peas | Pea weevil, pea aphid | Spraying during the growing season The consumption of working fluid for ground application is 200-300 l/ha. when applied by air 25-50 l/ha | |
| 0.15-0.2 0.15-0.2 (A) | Soybeans | Cotton bollworm, soybean moth | Spraying during the growing season The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0.1-0.15 0.1-0.15 (A) | Soybeans | Acacia (bean) moth, meadow moth | Spraying during the growing season The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | |
| 0,1-0,15 | Sugar beet | Beet weevils, beet flea beetles | Spraying seedlings. The consumption of working fluid for ground application is 200-400 l/ha. | 30(2) |
| 0.1-0.15 0.1-0.15 (A) | Sugar beet | Beet leaf aphid, meadow moth | Spraying during the growing season. The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 21(2) |
| 0.2-0.3 0.2-0.3 (A) | Sugar beet | Beet stem beetle | Spraying during the growing season. The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 21(2) |
| 0,1-0,15 | Spring and winter rape | Cruciferous flea beetles | Spraying seedlings. The consumption of working fluid for ground application is 200-400 l/ha. | 34(2) |
| 0.1-0.15 0.1-0.15(A) | Spring and winter rape | Rapeseed sawfly, rape seed beetle, rapeseed flower beetle | Spraying during the growing season. The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 34(2) |
| 0.15-0.2 0.15-0.2(A) | Spring and winter rape | Cabbage moth | Spraying during the growing season. The consumption of working fluid for ground application is 200-400 l/ha. when applied by air 25-50 l/ha | 34(2) |
| 0,1-0,2 | Chickpeas | Cotton bollworm, chickpea miner, meadow moth | Spraying during the growing season The consumption of working fluid for ground application is 200-400 l/ha. | 14(2) |
| 0.05-0.07 0.05-0.07(A) | Conifers | Pine-eating pests: Siberian cocoon moth, star weaver sawfly, red pine sawfly | Spraying during the development of caterpillars and larvae. The period of possible stay of people in areas treated with the drug is no earlier than 3 days after treatment. Collecting wild mushrooms and berries during the processing season is not permitted. Working fluid consumption: for ground use – 100-200 l/ha, for aviation – 3-25 l/ha | -(1) |
| 0,07 | Conifers | Pine-eating pests: Siberian cocoon moth, star weaver sawfly, red pine sawfly | Spraying during the development of caterpillars, larvae and adults using an aerosol generator of controlled dispersion "GARD". The period of possible stay of people in areas treated with the drug is no earlier than 3 days after treatment. Collecting wild mushrooms and berries during the processing season is not permitted. Effective working width – 140-480 m. Working fluid consumption – 1-3 l/ha | -(1) |
| 0.05-0.07 0.05-0.07(A) | Hardwood | Leaf-eating and sucking pests: oak flea beetle, oak lace bug | Spraying during the development of larvae and adults. The period of possible stay of people in areas treated with the drug is no earlier than 3 days after treatment. Collecting wild mushrooms and berries during the processing season is not permitted. Working fluid consumption: for ground use – 100-200 l/ha, for aviation – 3-25 l/ha | -(2) |
| 0,07 | Hardwood | Leaf-eating and sucking pests: oak flea beetle, oak lace bug | Spraying during the development of larvae and adults using an aerosol generator of controlled dispersion "GARD". The period of possible stay of people in areas treated with the drug is no earlier than 3 days after treatment. Collecting wild mushrooms and berries during the processing season is not permitted. Effective working width – 140-480 m. Working fluid consumption – 1-3 l/ha | -(1) |
Peculiarities:
- The drug can be mixed with most known insecticides, acaricides and fungicides. Check for miscibility before use.
- Spraying is carried out in calm weather, ensuring uniform wetting of the leaves. The interval between treatment and possible precipitation should be at least 4 hours.
Source : https://betaren.ru
Effects of Aldosterone
Aldosterone is secreted in the zona glomerulosa of the adrenal glands, stimulates sodium reabsorption and potassium excretion in the renal tubules, which allows it to be classified as a mineralocorticoid hormone. By reducing renal perfusion, increasing the activity of angiotensin II and adrenocorticotropic hormone, the release of aldosterone is stimulated. In CHF, the level of aldosterone in the blood plasma can reach 300 ng/dL, which is 60 times higher than the levels observed normally (5–15 ng/dL) [8]. Aldosterone promotes sodium and water retention in the body, the development of hypervolemia and fluid stagnation. In addition, aldosterone is a factor in the development of cardiac fibrosis, one of the most important elements of cardiac remodeling and the progression of CHF. The effects of aldosterone are realized through the modulation of gene expression in the cell upon binding to mineralocorticoid receptors located in the epithelial cells of the tubules of the kidneys and adrenal glands, as well as in non-epithelial cells of the hippocampus, endothelium and smooth muscle cells of the heart. The interaction of aldosterone with mineralocorticoid receptors contributes to endothelial dysfunction, increased thrombosis, decreased vascular compliance, baroreceptor function, myocardial and vascular fibrosis [9, 10]. The experiment showed that stimulation of mineralocorticoid receptors leads to an increase in the level of the matrix cellular protein osteopontin, which increases fibrosis and diastolic dysfunction of the myocardium [11]. In recent years, the pathophysiological mechanisms underlying the association of circulating aldosterone and lipid concentrations have attracted increasing attention. Adipose tissue stimulates the secretion of aldosterone, which in turn mediates adipocyte differentiation, promoting adipogenesis and inflammation [12]. In addition, there are studies indicating a damaging effect of high aldosterone concentrations on renal function with further proteinuria [13]. There is growing evidence that aldosterone may mediate and exacerbate the damaging effects of angiotensin II. Since angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor antagonists (ARBs) reduce plasma aldosterone concentrations, the so-called “aldosterone escape effect” is often observed with their use, regardless of the dose of ACEIs and ARBs. It is possible that this phenomenon is explained by the synthesis of aldosterone not only in the zona glomerulosa of the adrenal glands, but also by endothelial cells and cardiomyocytes, which are not affected by these groups of drugs. In this regard, it becomes quite obvious that a more complete blockade of aldosterone production is necessary to reduce the risk of progression of target organ damage in patients, in particular with CHF.
AMKR effects
According to recent studies, AMCRs reduce interstitial and perivascular myocardial fibrosis and its pathological remodeling, LV hypertrophy, oxidative stress and improve endothelial function. The beneficial effect of AMCR is a reduction in the risk of fatal ventricular and supraventricular arrhythmias, including atrial fibrillation. This effect may be due to both the prevention of hypokalemia and the antifibrotic effect [14]. A meta-analysis of 11 clinical studies assessing the effects of AMCR on the structure and function of the LV involving 942 patients with CHF, preserved LVEF and LV diastolic dysfunction revealed a significant decrease in the serum concentration of N-terminal propeptide of total procollagen type III (dynamics was -0.90 g/l, p<0.001). A similar decrease in the concentration of the C-terminal propeptide of total procollagen type I was observed in the group as a whole in the generalized analysis (dynamics was -17.6 ng/ml, p = 0.01). After 6 months after the start of AMCR treatment, there was an improvement in LV diastolic function in patients, which was expressed in a decrease in E/eʹ compared to the control group (dynamics was -1.68, p<0.001) [15]. Another meta-analysis confirmed the effect of AMCR on reducing the incidence of hospitalization (odds ratio 0.83) and improving LV diastolic function in patients with CHF and preserved LVEF after myocardial infarction [16]. The main representatives of AMKR - spironolactone and eplerenone (belong to the group of drugs for oral administration) have been studied in large controlled randomized trials. Another member of AMKR, potassium canrenoate, is administered both parenterally and enterally (in some countries). The anti-remodeling properties of potassium canrenoate were assessed in patients with mild CHF after myocardial infarction, but this drug was not studied in large randomized trials. In this regard, potassium canrenoate, unlike spironolactone and eplerenone, is less often used in the treatment of patients with CHF. A representative of the 3rd generation of non-steroidal AMCRs, finerenone is currently being studied in the FINESSE-HF study (Finerenone Trial to Investigate Efficacy and Safety to Eplerenone in Patients with Heart Failure) in comparison with eplerenone in more than 3600 patients with CHF and low LVEF, diabetes type 2 diabetes (DM) and/or chronic kidney disease [17, 18]. Currently, AMCRs are included in the main group of drugs and are used along with ACEIs and β-blockers (BAB) for the treatment of patients with CHF II–IV functional class (FC) in order to reduce the risk of hospitalization and death ( class I, degree of evidence A )
.
Place of selective AMCR eplerenone in CHF with low LVEF
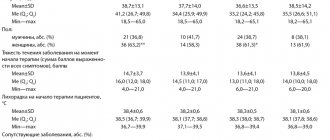
The international double-blind, placebo-controlled study EPHESUS (Epleronone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study) [19], which was conducted in 674 centers in 37 countries with the participation of 6632 patients (3319 - eplerenone group, 3313 - standard group). therapy) who have had myocardial infarction, with LVEF ≤40% and signs of congestion. The average age was 64 years, 71% were men, the average LVEF was 33%, the time from the onset of myocardial infarction was 7.3 days, the average follow-up period was 16 months. (from 0 to 33 months). Patients with creatinine levels greater than 2.5 mg/dL or potassium levels greater than 5 mmol/L were not included in the study. Eplerenone was added to standard therapy on days 3–14 of the disease at an average daily dose of 43 mg. An important component of this study was the administration of the study drug against the background of optimal therapy, which included ACEI or AR II (87%), beta blockers (75%), diuretics (60%) and, if possible, reperfusion therapy. The EPHESUS study showed that the use of the highly selective AMKR eplerenone in patients with LV systolic dysfunction and CHF after myocardial infarction contributed to a reduction in overall mortality by 15%, cardiovascular mortality by 17%, and sudden cardiac death by 21%. A 13% reduction in cumulative cardiovascular mortality and cardiovascular hospitalizations was achieved. The double-blind, randomized phase III study EMPHASIS-HF [20] included 2737 patients aged 55 years and older with CHF II class (according to NYHA) and LVEF not more than 35%. Eplerenone was recommended at an initial dose of 25 mg/day (group 1), titrated to 50 mg/day after 4 weeks. against the background of complex therapy with the use of ACE inhibitors, ARB II and beta blockers in the maximum tolerated dose. The control group consisted of patients receiving placebo. Interim analysis after 21 months. from the start of the study showed a significant decrease in mortality from cardiovascular causes and the number of hospitalizations, which served as the basis for premature termination of the study (Table 1).
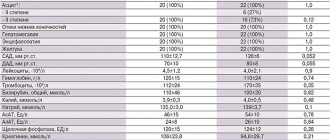
Spironolactone, unlike eplerenone, is a non-selective mineralocorticoid receptor antagonist (MCR) and has a high affinity for androgen and progesterone receptors, leading to undesirable effects such as gynecomastia and impotence in men, as well as menstrual irregularities in women. For example, in the RALES study, gynecomastia was reported in 10% of men taking spironolactone. Selective AMKR eplerenone (for example, the drug Espiro) has a greater tropism for aldosterone receptors, and its affinity for progesterone and androgen receptors is 100 and 1000 times lower than that of spironolactone, and therefore side effects when using this drug are recorded much less frequently. A number of drugs, such as ketoconazole, ritonavir, clarithromycin, erythromycin, verapamil, digoxin, cyclosporine, as well as grapefruit juice, can increase the concentration of eplerenone in the blood due to inhibition of the activity of CYP3A4 enzymes, which should be taken into account when prescribing this drug (Table 2).
The clinical effect of eplerenone is explained by favorable electrolyte changes, a decrease in myocardial interstitial fibrosis, oxidative stress, an improvement in endothelial function, a decrease in platelet aggregation, and an increase in the activity of metalloproteinases and the sympathoadrenal system. It is important to keep in mind that aldosterone binds not only to its specific receptors in the myocardium, macrophages, but also to fibroblasts. As a result of this interaction, the synthesis and accumulation of collagen type III is enhanced, which contributes to increased myocardial stiffness, the development of perivascular and interstitial fibrosis, and remodeling of the myocardium and arterial bed. Deterioration of the vasomotor reserve of the coronary vessels and blood supply to the myocardium leads to the death of cardiomyocytes, accelerating the process of fibrosis, diastolic and systolic dysfunction. Early administration of AMCRs is especially important for patients with CHF who have suffered a myocardial infarction, since AMCRs have a proven ability to slow down LV myocardial remodeling. In this situation, the use of eplerenone is preferable due to the less pronounced likelihood of side effects [21]. The most common side effect of eplerenone is hyperkalemia. According to the EPHESUS study, in patients with LV systolic dysfunction after myocardial infarction who used eplerenone, hyperkalemia (6 mmol/L or more) was detected in 1.6% of cases, while the frequency of hypokalemia (3.5 mmol/L or less) decreased by 4.9%. Hyperkalemia is the most common side effect of therapy with RAAS blockers, including AMKR. Significant risk factors for the development of clinically significant hyperkalemia are an estimated glomerular filtration rate (GFR) <45 ml/min/1.73 m2 and/or a potassium level >4.5 mmol/L while taking a diuretic dose that is optimal for a given renal function [22]. In such conditions, hyperkalemia is indeed a common complication of therapy with RAAS blockers and a frequent reason for discontinuation of treatment or the basis for the use of suboptimal doses of drugs. The situation is complicated by the fact that it is RAAS blockers that have proven their effect on reducing mortality (in particular, overall mortality by 15–30%), the frequency of hospitalizations and slowing the progression of renal dysfunction in patients with CHF [23–25]. Not all patients with CHF take ACE inhibitors/ARB II and only about 25–45% of them take the recommended drugs in optimal target doses, and 10% stop taking them. Patients with CHF and low LVEF also do not fully use AMCR, and treatment adherence reaches only 50%. According to T. Thorvaldsen et al., in 2012, 52% of patients took MACR, in contrast to 43% in 2002 (p <0.001), but despite the positive trend, adherence to treatment remains insufficient [26]. Low adherence to treatment is explained by the development of hyperkalemia and reduced renal function, especially in patients with concomitant diabetes and chronic kidney disease. Additional analysis of the EMPHASIS-HF study showed that MRAs, particularly eplerenone, remained effective at serum potassium levels up to 5.5 mmol/L. It is possible that the benefits of eplerenone therapy outweigh the risk of hyperkalemia [27]. These data formed the basis for recommendations to reduce the dose of AMCR in patients with GFR <30 ml/min/1.73 m2 or potassium levels >5.5 mmol/l and discontinue AMCR in patients with GFR <20 ml/min/1.73 m2 or potassium levels >6 mmol/L [1]. The above indicates the need to monitor the level of potassium in the blood and kidney function when prescribing AMCR, depending on the clinical condition, age of the patient and concomitant pathology. Analysis of a subgroup of patients with CHF, low LVEF, NYHA class II in the EMPHASIS-HF study revealed a group at risk for developing hyperkalemia, which includes patients over the age of 75 years with a GFR level <60 ml/min, diabetes and blood pressure >123 mm Hg . Art. In patients at risk, eplerenone increased potassium levels >5.5 mmol/L, but potassium levels >6.0 mmol/L were not observed in any of the patients, including those hospitalized for hyperkalemia, those who discontinued the drug due to hyperkalemia, and hospitalized for renal dysfunction [28]. The authors concluded that eplerenone is quite effective in reducing the frequency of hospitalizations for decompensated CHF and cardiovascular mortality not only in the studied patient population, but also in a group at high risk of developing hyperkalemia. In large randomized trials studying eplerenone (EPHESUS, EMPHASUS-HF), no deaths due to hyperkalemia were reported. Since eplerenone is a highly selective AMCR, gynecomastia occurs rarely (less than 1% of patients). According to the EPHESUS and EMPHASIS-HF studies, gynecomastia was reported in 0.5 and 0.7% of men taking eplerenone, respectively. The affinity of eplerenone for androgen receptors is 370 times lower than that of spironolactone, and even when taken in high doses, the drug does not bind to progesterone and glucocorticoid receptors. When identifying gynecomastia in a patient with CHF, it should be remembered that there are a number of diseases that increase the risk of its development, and most patients with CHF are comorbid older patients [29]. Inactivation of steroid hormones occurs mainly in the liver, kidneys and, less commonly, in the intestines. Impaired functioning of these organs can contribute to disruption of the metabolism of steroid hormones and increase their concentration in the blood. In addition, an increase in estrogen levels can be observed when taking drugs containing estrogens and having the effects of estrogens or antiandrogens: genistein, 8-prenylnaringenin, etc. The use of narcotic drugs, amphetamine, anticancer drugs, slow calcium channel blockers, diazepam, digitalis, human chorionic gonadotropin, ACE inhibitors, isoniazid, ketoconazole, methyldopa, metronidazole, tricyclic antidepressants can also cause the development of gynecomastia. These data support the choice of eplerenone in patients with complex comorbidities.
Espiro
Pharmacodynamic interactions
Potassium-sparing diuretics and potassium supplements: Given the increased risk of hyperkalemia, eplerenone should not be administered to patients receiving potassium-sparing diuretics and potassium supplements. Potassium-sparing diuretics may enhance the effects of antihypertensives and other diuretics.
Preparations containing lithium: the interaction of eilerenone with lithium preparations has not been studied. However, in patients receiving lithium preparations in combination with diuretics and AIF inhibitors. Cases of increased concentration and lithium intoxication have been described. If such a combination is necessary, it is advisable to monitor the lithium content in the blood plasma.
Cyclosporine, tacrolimus: Cyclosporine and tacrolimus may cause disturbances in nocturnal function and increase the risk of developing hyperkalemia. Concomitant use of eplerenoid and cyclosporine or tacrolimus should be avoided. If cyclosporine or tacrolimus is required during treatment of eplerenomas, it is recommended to regularly monitor serum potassium levels and renal function. Nonsteroidal anti-inflammatory drugs (NSAIDs): Treatment with III1VP may lead to acute renal failure due to direct suppression of glomerular filtration, especially in patients at risk (elderly patients and/or patients with dehydration). When using these drugs together, it is necessary to ensure adequate fluid intake and monitor renal function before and during treatment.
Trimethoprim: Concomitant use of trimethoprim with eplerenoid increases the risk of developing hyperkalemia. It is recommended to monitor serum stone levels and renal function, especially in patients with renal failure and in elderly patients.
AIF inhibitors and angiotensin II receptor antagonists: When using eplerenone with ACE inhibitors or angiotensin II receptor antagonists, serum potassium levels should be regularly monitored. Such a combination may lead to an increased risk of developing hyperkalemia, especially in patients with impaired renal function, incl. in elderly patients.
The triple combination of an ACE inhibitor and an ARA II with enlereion should not be used.
Alpha1-adrenergic blockers (prazoznn, alfuzoznn): with simultaneous use of alpha1-adrenoblockers with eplerenone, the antihypertensive effect may be enhanced and/or the risk of developing orthostatic hypotension may increase, and therefore it is recommended to monitor blood pressure when changing body position.
Tricyclic antidepressants, antipsychotics, amnphostin, baclofen: with simultaneous use of these drugs with eplerenone, the antihypertensive effect may be enhanced or the risk of developing orthostatic hypotension may increase.
Glucocorticosteroids, tetracosactide: simultaneous use of these drugs with eplerenone may lead to sodium and fluid retention.
Pharmacokinetic interactions
In vitro studies indicate that eplerenone does not inhibit CYP1A2 isoenzymes. CYP2C19, CYP2C9, CYP2D6 and CYP3A4. Eplerenone is not a substrate or inhibitor of P glycoprotein.
Digoxin: The AUC of digoxin when administered concomitantly with eplerenone increased by 16% (90% CI: 4-30%). Caution must be exercised if digoxin is used in doses close to the maximum therapeutic dose.
Warfarin: No clinically significant pharmacokinetic interaction with warfarin has been identified. Caution must be exercised if warfarin is used in doses close to the maximum therapeutic dose.
CYP3A4 substrates: In specific studies, no evidence of pharmacokinetic interaction of eplerenone with CYP3A4 substrates, such as midazolam and cisapride, was identified.
CYP3A4 isoenzyme inhibitors
Strong inhibitors of the CYP3A4 isoenzyme: when using eplersion with drugs that inhibit the CYP3A4 isoenzyme, significant pharmacokinetic interaction is possible. A strong CYP3A4 inhibitor (ketoconazole 200 mg twice daily) caused a 441% increase in the AIJC of eplercion. Concomitant use of eplerenone with strong inhibitors of the CYP3A4 isoenzyme, such as ketoconazole, itraconazole, ritonavir, nelfinavir, clarithromycin, telithrominine and nefazadone, is contraindicated (see section "Contraindications").
Weak and moderate inhibitors of the CYP3A4 isoenzyme: simultaneous use with erythromycin, saquinavir, amiodarone, diltiazem. verapamil and fluconazole were accompanied by a significant pharmacokinetic interaction (the degree of increase in AUC ranged from 98% to 187%). When using these drugs simultaneously with eplerenone, the dose of the latter should not exceed 25 mg (see section “Dosage and Administration”).
Inducers of the CYP3A4 isoenzyme: simultaneous use of drugs containing St. John's wort (a strong CYP3A4 inducer) with eplerenone caused a decrease in the AUC of the latter by 30%. When using stronger CYP3A4 inducers, such as rifampicants, a more pronounced decrease in the AUC of eplersion is possible. Given the possible decrease in the effectiveness of eplerenone, the simultaneous use of strong CYP3A4 inducers (rifampicin, carbamazepine, phenytoin, phenobarbital, drugs containing St. John's wort) is not recommended.
Lntacids: based on pharmacokinetic clinical study
There is no significant interaction between antacids and eplerenone when used concomitantly.
Place of eplerenone in CHF with preserved LVEF
Since there is evidence of the high effectiveness of eplerenone in patients with CHF and low LVEF, the question naturally arises about the possibility of using this drug in people with CHF and preserved LVEF. In the modern understanding, CHF with preserved LVEF is a complex of diseases in which it is often difficult to identify the leading cause of progression and decompensation of cardiac activity. All sorts of factors and diseases can shape and change the clinical picture, contributing to the development of various phenotypes. Several physiological mechanisms are involved in the pathogenesis of CHF with preserved LVEF. Systemic inflammation, fibrosis and oxidative stress play an important role. In many patients, LV diastolic function is impaired, LV stiffness increases due to increased deposition of extracellular collagen and changes in cardiomyocyte cytoskeletal proteins, the degree of myocardial relaxation and its energy reserve decreases, and neurohumoral activity increases [30]. Since aldosterone is involved in many of the listed processes, the use of eplerenone seems promising in this category of patients, which is confirmed by a number of studies [31]. Within 24 months. 303 patients (249 men) with preserved LVEF aged 58±11 years were observed, in whom the level of matrix metalloproteinase-9 (MMP-9) was assessed on the 7th day after myocardial infarction. Patients were divided into 2 groups: those taking eplerenone (n=201) at a dose of 25 mg/day and the control group (n=102). The use of eplerenone was not associated with improved survival in the overall group (p = 0.132), however, in the group of patients with initially lower MMP-9 levels (p = 0.005), the prognosis was better, which allowed us to consider low MMP-9 levels in patients after a heart attack myocardium with preserved LVEF as an identifier of that part of patients in whom eplerenone is associated with a favorable prognosis [32–37]. Since there is currently no convincing evidence of the high effectiveness of certain classes of drugs used in CHF with preserved LVEF, it is hoped that targeting the fibrosis process will help improve cardiomyocyte function and the clinical condition of patients.
Answers on questions
00:00
Arutyunov Grigory Pavlovich , Doctor of Medical Sciences, Professor:
— Based on the scenario of our event today, I have questions that I will now briefly try to answer. I will read the question and give a short answer to it.
Question: Is Torasemide effective in all patients?
- Yes. Prospective studies have shown that it is much more effective than Furosemide. Transferring patients who received Furosemide to Torasemide gave a greater diuretic effect.
Question: Are there patients in whom Furosemide should be preferred?
— When choosing one or another diuretic drug, you should focus, first of all, on the indicators of this drug, on the half-life. Remember firmly that the longer the half-life of the drug, the less the toxic effect. The second indicator is whether there are additional positive effects. In particular, does it affect mortality. Torasemide reduces mortality, especially sudden mortality.
Question: Does it have any additional effect?
- Please note that with equal potassium excretion, there is no peak-shaped potassium excretion on Torasemide. This means that the risk of ri violation does not increase.
Question: Another question related to Torasemide. From my own experience I know that Torasemide is less effective in some patients than Furosemide.
- This is not true, because I will once again refer to large prospective clinical studies. It is much more important to remember that 10 mg of Torasemide is equivalent to 40 mg of Furosemide.
Doctor Drachev asks a question.
Question: When is the combined use of Torasemide and Spironolactone indicated?
— Diuretics plus Spironolactone at a dose of 25 mg for life, starting from the third functional class, regardless of whether it is sinus rhythm or atrial fibrillation. Lifelong therapy.
Question: What is the fundamental difference between Veroshpiron and Eplerenone? What is the place of Eplerenone in the treatment of chronic heart failure?
— “Veroshpiron” differs from “Eplerenone” in only one thing - the removal of two radicals, which changed its sexual effect. Gynecomastia does not develop with long-term use. Currently, Eplerenone has been tested in patients who have survived myocardial infarction and has proven its effect on reducing the risk of death. First of all, by reducing sudden deaths.
02:22
Question: In urgent therapy, large doses of Furosemide are used. What is the maximum safe dose of Furosemide in urgent therapy?
— Such a dose does not exist. We must clearly remember that when starting therapy at 80 mg, you need to ask yourself the question: if you do not see a diuretic effect, what is happening. Or the wrong method of administration. For example, edema syndrome does not allow intramuscular and oral administration to be effective. Switch to intravenous administration.
If bolus administration is ineffective, switch to intravenous dosing. After this, do not strive to increase the dose. Instead, take the path of combination therapy. You have a way to add hydrochlorothiazide or potassium-sparing diuretics to diuretic therapy. It depends on the specific situation.
It is much more important to remember something else. Any increase in the dose of diuretics is toxic. It will always have a negative impact on the state of the glomeruli and will lead to a decrease in the glomerular filtration rate. Will affect electrolyte balance. Will increase the likelihood of rhythm disturbances. Forced diuresis (in large doses you should always think about forced diuresis) will lead to a change in the volume of circulating blood and create ideal conditions for deep vein thrombosis and embolism in the pulmonary artery.
Question: The numbers are 139/79 mmHg. Art. are they talking about normal blood pressure?
- But this is high normal.
Question: How can a practitioner determine blood pressure levels with an accuracy of 1 mm?
- By repeatedly measuring and finding the average figure, if your results always show borderline values.
Question: Any technical device produces an error. This error will be more than 1 mm. So again it is impossible to determine the level of blood pressure with such accuracy to 1 mm?
- If you are making a decision and it is really very important for you whether 140 or 139, try it on several times, find the average value. But it is a thousand times more important that you paid attention to the risk factors that the patient has and determined his true prognosis, the likelihood of his cardiovascular death. After that we would make that decision.
04:38
Question: Will there be changes in recommendations for the treatment of CHF? If yes, which ones?
- Yes, they will. Naturally. In the coming months, a new project will be posted on the Heart Failure Society website and will be discussed throughout the year. In particular, there will be a chapter related to chronic obstructive pulmonary diseases, and trophological additions will appear.
Large national studies have ended. These will probably be quite significant changes to the modern text.
Question: What place does Aliskiren occupy in the treatment of CHF?
— At the moment, there is no strictly defined place for Aliskiren in the treatment of CHF. But we must remember that in patients with CHF, the entire neurohormonal profile is disrupted, including increased renin activity. However, excessive blockade of neurohormones has never led to any significant success. On the contrary, it worsened the prognosis. Today, a blockade consisting of three components is considered safe. This influences the level of norepinephrine, angiotensin II and the level of aldosterone.
Question: Do approaches to the treatment of systolic and diastolic CHF differ?
- Yes, they will be fundamentally different. At the moment, there are no firm decisions regarding the treatment of diastolic circulatory failure. A number of studies (in particular “Ara”) have not shown any advantages in the treatment of diastolic circulatory failure.
Question: About the use of Torasemide in children.
— There is no such data. All patients who were included in the study were over 18 years of age. Thank you for your attention.
06:10
Oganov Rafael Gegamovich , President of the All-Russian Scientific Society of Cardiologists, Academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences, Professor:
Question: What are the statistics on cardiovascular mortality over the past 5 years? Is the average age of death from cardiovascular disease changing?
— The statistics are favorable. Since 2003, there has been a decrease in mortality from cardiovascular diseases. It is difficult to say how stable these statistics will be in the future, because various demographic processes are interfering. They do not depend on our actions and desires. But so far the statistics are favorable. There was a decrease of about 15 percent compared to 2003.
Question: Is the average age of death changing?
— It’s very difficult to say. We can say only if we compare the mortality rate at working age in our country and in the countries of the European Union, then it is somewhere 5-6 times higher than in the countries of the European Union.
Question: Question about risk factors. There is evidence that obese people do not live much shorter than people with normal body weight. How can this be explained?
— I have an article and lecture called “Paradoxes of Preventive Cardiology.” Yes, indeed there are quite a lot of studies that concern patients with coronary heart disease. They show that the prognosis for people with increased overweight and obesity is better than for people with normal body weight.
It is difficult to say what this is connected with. Although recently a study has emerged that shows that the criteria and methods of excess body weight that we use are not entirely suitable. Specifically, we use body mass index. In clinical studies, this index has been commonly used.
Compared how body mass index predicts the outcome, abdominal obesity, which is measured using waist circumference. It turned out that if we take abdominal obesity, it turns out very clearly, as we thought before. The larger the waist circumference, the higher the mortality rate. If you take the body mass index, you often get an inverse relationship. The higher the body mass index, the better the prognosis. Apparently, body mass index is simply not suitable for assessing prognosis in individuals who already have coronary heart disease.
08:39
Question: What are the acceptable minimum diastolic pressure numbers?
- Yuri Alexandrovich has already said. I won't.
Vladimir Trofimovich Ivashkin , academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences:
- Thank you. Please, Yuri Alexandrovich.
Yuri Aleksandrovich Karpov , Doctor of Medical Sciences, Professor:
— I have quite a lot of questions. I will try to answer briefly.
Question: One of the questions. The target pressure level (what I talked about in the recommendations) - is it office pressure, average daily pressure, or central pressure indicators?
— 130/139 is the so-called office pressure, that is, what was registered at the doctor’s appointment. We don't think the range is narrow. Moreover, this is an indicative level. If it turns out to be slightly lower, then this is allowed if the patient tolerates such a decrease well.
We have a lower limit for reducing blood pressure. I talked about her too. The only thing that is unacceptable is that the pressure is more than 140 mmHg. Art. This is the most important parameter.
Next point. Blood pressure control in people over 85 years of age who have not been controlled for a long time, and adapted to high numbers. In old age, the main principle is a gradual decrease in blood pressure. There is now evidence that in people over 80 years of age, controlling blood pressure provides patient benefits. This was shown in the Hyvet study. I mentioned him briefly.
Today we have no age restrictions for monitoring blood pressure levels, including those over 85 years of age. The optimal level for them is less than 150 mmHg. Art. (systolic).
10:24
Question: What is the clinical significance of reducing diastolic pressure to less than 60 mm in the effective control of isolated systolic arterial hypertension?
— This clinical significance is not entirely clear. But it is clear that the higher the pulse pressure, the worse the prognosis. There were no special studies. From my point of view, the most important indicator in this case is the controllability of systolic pressure. It is with the control of systolic blood pressure that the greatest problems are now encountered.
Question: From one of our listeners, from sixth-year student Ruchkin, I have a large number of questions regarding the methodology for measuring blood pressure and some other points.
- I can say the following. When measuring blood pressure, it is necessary to take into account the volume of the patient's arm. For overweight obese patients, larger cuffs should be used. There is a corresponding gradation of cuff sizes. Of course, an electronic tonometer has a greater degree of error compared to a mechanical one. We must take this into account. There is such a rule. Blood pressure must be measured with a device that is checked periodically. Accordingly, you must trust this device.
Blood pressure numbers given here by our listener. Of course, in many ways there is a certain degree of convention in the definition of what is called arterial hypertension, which we refer to as arterial hypertension. Moreover, in recent years we have changed the boundaries of normal and pathological conditions with increased blood pressure.
The diagnosis of arterial hypertension, of course, is determined by the blood pressure numbers, which have been recorded as elevated several times (more than 140 mm Hg). But the second very important point - this, of course, must be supported by an assessment of the state of target organs and risk factors. Everything must be considered in its entirety.
On the one hand, the diagnosis is simple. On the other hand, of course, assessing the patient requires certain diagnostic efforts. This is all very clearly stated in our recommendations.
12:55
Vladimir Ivashkin : Yuri Alexandrovich, I also read the questions of this inquisitive student. I think that the trend of changes in blood pressure during observation of the patient and during treatment is very important. Not just the baseline, the trend, where it's all going.
Yuri Karpov: Yes, of course, Vladimir Trofimovich. This is a very important point because for us, optimal control is extremely important in our end goal. Here, of course, we need to achieve an optimal result, use all the possibilities of drug therapy and what Rafael Gegamovich spoke about. We must not forget the non-drug effects on blood pressure.
Question: Another very interesting point is asked by a student. Is it possible to develop atherosclerosis with normal cholesterol levels?
- In general, yes. As well as the opposite. With high cholesterol, we may not detect signs of atherosclerosis. Everything will depend on what technique we use for diagnosis. This is a question that is, of course, very big. Maybe someday we will have a separate meeting that we will devote to this.
Question: How does pulse pressure differ from central pressure? Which is worse prognostically?
— If there is data on the value of pulse pressure in terms of prognosis, then central pressure is a relatively new indicator. It has not yet (to my knowledge) been used as a prognostic factor. Although this is very interesting and could expand our ability to clarify the prognosis of a patient with arterial hypertension, which, by the way, is not as simple as we sometimes think.
14:40
Question: Which group of drugs is more appropriate to start therapy with in elderly patients?
— Priority is given to two classes of medicines. These are diuretics and calcium antagonists. But in general, we do not have any ban on the use of other antihypertensive drugs. We can use the full range of antihypertensive medications.
Question: What place do renin inhibitors occupy in antihypertensive therapy? Why are they not included in the combination therapy regimen?
— Direct renin inhibitors (primarily the drug Aliskiren, which is registered and used for the treatment of arterial hypertension) occupy the position of additional classes of antihypertensive drugs.
This is due to the fact that to date we do not have data regarding the effect of Aliskiren on long-term outcomes of arterial hypertension. We have data on blood pressure control, on the effect on certain organ lesions, on the combination of Aliskiren with various drugs. But there are no data on long-term outcomes.
In terms of combination therapy, Aliskiren, as well as other drugs belonging to the class of blocking the activity of the renin-angiotensin system, are most beneficial in combination with diuretics and calcium antagonists. Today this is an interesting promising direction.
Question: Please tell us more about the Strong study.
— The “Strong” study is a large study, which we classify as research into real clinical practice. More than a thousand patients whose blood pressure was not controlled on either one, two, or more classes of antihypertensive drugs. Or untreated patients. Therapy was discontinued, and patients were transferred to a combination of Perindopril and Amlodipine.
This study showed that this combination has a huge benefit in improving blood pressure control.
Question: Which term is correct: antihypertensive therapy (or drug) or antihypertensive?
— For us, of course, the most important point is antihypertensive treatment. We must prevent blood pressure from rising. Do not be surprised that a patient with arterial hypertension takes a drug that lowers blood pressure when his blood pressure is normal. It is important that your blood pressure does not increase.
Antihypertensive therapy is applied to a situation where you have high blood pressure and you need to reduce this blood pressure. This is quite appropriate. But in general, it is better to use the terminology “antihypertensive therapy” and address this issue accordingly.
17:33
Question: A very important question. Isn't the combination of Trandelapril and Verapamil better?
- Apparently, doctors compare them with a combination of Perindopril and Amlodipine. I can say that it is not better, at least. I can back this up with the results of Ascot comparative research. There, the combination of Amlodipine with the addition of Perindopril was significantly more effective in reducing mortality compared to a beta blocker and a diuretic.
The counterbalance to this study is “INVEST”. There, the combination based on Verapamil with the addition of Trandelapril turned out to be the same for many patients as therapy based on Atenolol with the addition of a diuretic.
A comparison of the two studies allows us to say that the combination of Trandelapril with Verapamil is no better. If we still extrapolate the results, then it was no more effective than a beta blocker and a diuretic.
Question: What drugs are optimal for stopping a hypertensive crisis?
— If we are talking about oral drugs, then today we most widely use fast-acting drugs. This is one of the ACE inhibitors - Captopril. It is not very good for long-term treatment because it must be taken several times a day. But it works quickly. Taken under the tongue, it reduces elevated blood pressure levels within half an hour.
Then we use short-acting nifedipine drugs, calcium antagonists. They are also not suitable for long-term treatment, but are good for stopping a hypertensive crisis that is not severe. Clonidine in general can also be used in situations of rapid lowering of blood pressure. But it is not very good for long-term treatment due to the fact that it has some undesirable effects.
19:47
The last question, dear colleagues, that I have.
Question: What new did the cardio congress bring in Paris?
— Of course, it’s difficult to put it in a nutshell, but I’ll still try to express my personal opinion on the results of the Paris Congress of European Cardiologists. It was a huge event. A huge number of participants.
In recent years, European congresses have become larger in number of participants and in scale than American ones, which for many years have been for us a kind of standard for the mass nature of the event and the interestingness in terms of the results.
The main slogan of this congress was the analysis of controversial situations in cardiology. A huge number of events were associated with expressing an opposing point of view on diagnosis, treatment, and the use of different methodological approaches. It was certainly interesting. Especially young cardiologists, because a lot has been done.
It is important to analyze the studies conducted and understand the values of a particular diagnostic and treatment method. This year, perhaps, for the first time, registers were discussed so actively. Apparently, in the coming years, registers will be the main sources of information for assessing the situation in cardiology. This is due, first of all, to the fact that the number of studies in cardiology has decreased significantly in recent years.
What is important to us now is the results of how effectively we are applying everything that has been developed in recent years.
21:28
Another fundamentally important question regarding the results of the congress. It was made in a report by Professor Salem Yusuf, a very famous figure who is involved in clinical research. He presented data from one of the registers, which analyzed the frequency of use of different drugs to reduce the risk of complications in patients in different countries. High income, middle income and low income.
He expressed a very important point of view that today it is much more important for us to use everything that has already been developed and created to reduce the risk of complications. This includes cheap drugs that are absolutely accessible to the vast majority of patients than, for example, the creation of new drugs, the effectiveness of which requires great effort in terms of improving the prognosis. We need to implement everything that has already been achieved today.
From the point of view of the actual clinical studies that took place, I was most impressed by the results of the Aristotle study. This is the treatment of patients with atrial fibrillation using the anticoagulant pexoban.
For the first time, an advantage over warfarin therapy was shown not only in terms of reducing the risk of complications, but also a significant reduction in mortality in the group of patients who received pexoban. But perhaps the most important thing is the high degree of safety of such therapy. The risk of bleeding was significantly lower than in the Warfarin group. These are the most important impressions, the results of the last European Congress of Cardiologists.
Vladimir Ivashkin : Thank you, Yuri Alexandrovich.
Now I will answer my questions very briefly.
Question: How long can I take Trimedat (Trimebutin)? This refers to patients with chronic abdominal pain.
- Trimedat (Trimebutin) is an opioid receptor agonist. Moreover, it is an agonist of non-central opioid receptors, therefore, it is not addictive and does not cause certain changes in mood and behavior. The main target of this drug is peripheral opioid receptors. The gastrointestinal tract is characterized by a very dense distribution of opioid receptors. Activation of peripheral opioid receptors underlies the mechanism of action of Trimebutine (Trimedate).
It should be used depending on the patient’s response or the response of his pain. The drug gradually develops its effect and exhibits its analgesic effect, so it must be prescribed for at least a month. Then, if the effect is achieved, if good results are obtained, then treatment must be continued. You can continue treatment indefinitely or in long courses.
24:52
Question: Should patients with chronic abdominal pain be advised to consult a psychotherapist?
- Necessarily. This is a prerequisite in order to understand the essence of the patient's complaints. But what should come first: the attending physician or the psychotherapist. Of course, the attending physician should come first. First of all, he must evaluate the clinical symptoms, whether the patient has any symptoms of so-called anxiety.
What are the symptoms of anxiety? This is a fever (in the range of 37.5 - 38.5 ° C). This is weight loss. Especially when it comes to progressive weight loss. This is the appearance of blood in the stool (hidden or obvious). Such symptoms indicate that the patient needs to receive very close attention.
After this, it is necessary to perform essentially routine studies at the moment. Perform an endoscopy of the upper gastrointestinal tract. Perform an endoscopy of the large intestine, and, if possible, the distal parts of the small intestine. Do an ultrasound examination. View general clinical and general biochemical blood tests.
In the vast majority of cases, this is enough to get an idea of a possible (if any) organic pathology and prescribe treatment. Typically, if a specific cause is identified, abdominal pain subsides within a week after we prescribe treatment. If during such an examination and during the prescribed treatment there is no improvement, then a consultation with a psychotherapist can serve a good purpose.
26:56
What you need to pay attention to in patients with chronic abdominal pain. Clinical symptoms - firstly. Secondly, a very thorough examination of the abdominal organs. Mandatory superficial and deep palpation. Do not forget that the stomach must be listened to and auscultated. Often symptoms are revealed during auscultation. Intestinal paresis. Silent belly.
It is imperative to investigate the possibility of identifying a pain symptom by changing the spine. Most often this is spondylitis.
Finally, mental status is a very important factor.
Here's an interesting question.
Question: Does educational level influence pain perception?
— I think there is no direct correlation. Often highly educated people, if they find out about the diagnosis (they say: “You have a duodenal ulcer”), calm down. They may have pain for years. They won't come to you anymore. They got the answer to their question. They know that duodenal ulcers in the vast majority of cases do not cause any serious complications.
A poorly educated person, due to a lack of understanding of what is happening to him, can endure for a long time. Moreover, he begins to be treated with folk remedies. What folk remedies, first of all. This is alcohol. Vodka. After this, contact your friends and so on for a possible recommendation. Sometimes we see such poorly educated patients coming to the clinic with an extremely advanced situation.
It is probably impossible to say that education and attitude to pain have a direct correlation. But still, of course, an educated person is a person who is able to be critical of himself and be critical of what the doctor recommends to him. An educated person will follow the doctor’s recommendations and carry out self-analysis with greater responsibility and with unconditionally greater constancy.
The principle is simple. The principle applies to all cases in medical practice. This principle was once expressed by Bernard Shaw. He said that gentlemen who wear top hats and smoke cigars live longer than gentlemen who wear caps and smoke cigarettes. This is a social gradation. This is a social stratification in which the level of education plays a decisive role. Of course it matters a lot.
Thank you, colleagues, for all of you for the very interesting messages and for the discussion. I noticed one pattern. Oksana Mikhailovna and I will probably formulate a law. It is not easy to invite well-known and experienced professors to this studio. But when they see the response from the audience, the attention that the audience gives them, they light up and promise that they will come next time for the next session.
So prepare new lectures. I think the audience will also be happy to wait, just like Oksana Mikhailovna and I.