Buy Buserelin-depot lyophilisate for the preparation of suspension intramuscularly 3.75 mg in pharmacies
Buserelin-depot Buy Buserelin-depot in pharmacies DOSAGE FORMS lyophilisate for preparing a suspension for intramuscular injection. entered prolong. active 3.75 mg lyophilized powder for the preparation of intramuscular solution 3.75 mg
MANUFACTURERS Deco Company (Russia) Pharm-Sintez (Russia)
GROUP Antiandrogens
COMPOSITION Active ingredient: buserelin acetate 3.75 mg in the form of a free peptide.
INTERNATIONAL NON-PROPENTED NAME Buserelin
SYNONYMS Buserelin, Buserelin FSintez, Buserelin-long FS, Buserelin acetate solution
PHARMACOLOGICAL ACTION Pharmacodynamics. A synthetic analogue of natural gonadotropin-releasing hormone (GnRH). Buserelin competitively binds to the receptors of the cells of the anterior pituitary gland, causing a short-term increase in the level of sex hormones in the blood plasma. Further use of therapeutic doses of the drug leads (on average after 12-14 days) to a complete blockade of the gonadotropic function of the pituitary gland, thus inhibiting the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). As a result, there is a suppression of the synthesis of sex hormones in the gonads, which is manifested by a decrease in the concentration of estradiol in the blood plasma to post-menopausal values in women and a decrease in testosterone content to a post-castration level in men. The concentration of testosterone with continuous treatment for 2-3 weeks decreases to the level characteristic of the orchiectomy state, i.e. pharmacological castration is caused. Pharmacokinetics. Bioavailability is high. The maximum plasma concentration is reached approximately 2-3 hours after intramuscular administration and remains at a level sufficient to inhibit the synthesis of gonadotropins by the pituitary gland for at least 4 weeks.
INDICATIONS FOR USE Hormone -dependent prostate cancer, breast cancer, endometriosis (pre- and postoperative periods), uterine fibroids, endometrial hyperplastic processes, infertility treatment (during an in vitro fertilization (IVF) program.
CONTRAINDICATIONS Pregnancy, breastfeeding, hypersensitivity to the components of the drug.
SIDE EFFECTS Allergic reactions: urticaria, skin hyperemia, rarely - angioedema. In women, typical adverse reactions are a manifestation of the achieved hypoestrogenic state - “pharmacological menopause”: From the central nervous system: frequent mood swings, sleep disturbances, depression, headache. From the endocrinological status: hot flashes, increased sweating, vaginal dryness, decreased libido, pain in the lower abdomen, demineralization of bones, rarely - menstrual-like bleeding (usually during the first weeks of treatment). In men, during the treatment of prostate cancer - during the first 2-3 weeks after the first injection, it can cause exacerbation and progression of the underlying disease, which is associated with stimulation of the synthesis of gonadotropins and, accordingly, testosterone, gynecomastia, a transient increase in the concentration of androgens in the blood (rarely - ossalgia , urinary retention, renal edema, muscle weakness in the lower extremities, lymphostasis). Other: in isolated cases (the cause-and-effect relationship has not been clearly established) - pulmonary embolism, dyspeptic disorders.
INTERACTION The simultaneous use of Buserelin with drugs containing sex hormones (for example, in the mode of ovulation induction) may contribute to the occurrence of ovarian hyperstimulation syndrome. With simultaneous use, Buserelin may reduce the effectiveness of hypoglycemic agents.
DOSAGE AND ADMINISTRATION For hormone-dependent prostate cancer: 3.75 mg intramuscularly (IM) every 4 weeks; In the treatment of endometriosis, endometrial hyperplastic processes: 3.75 mg IM once every 4 weeks. Treatment begins in the first five days of the menstrual cycle. Duration of treatment - 4-6 months; For the treatment of uterine fibroids: 3.75 mg IM once every 4 weeks. Treatment begins in the first five days of the menstrual cycle. Duration of treatment - 3 months before surgery, in other cases - 6 months; When treating infertility using in vitro fertilization (IVF): 3.75 mg IM once on the 2nd day of the menstrual cycle.
OVERDOSE Currently, no cases of overdose with Buserelin have been reported.
SPECIAL INSTRUCTIONS For women. Patients with any form of depression during treatment with the drug should be under close medical supervision. Ovulation induction should be performed under strict medical supervision. In the initial stage of treatment with the drug, the development of ovarian cysts is possible. Before starting treatment with the drug, it is recommended to exclude pregnancy and stop taking hormonal contraceptives, however, during the first two months of using the drug, it is necessary to use other (non-hormonal) methods of contraception. In men. In order to effectively prevent possible side effects in the first phase of the drug’s action, it is necessary to use antiandrogens two weeks before the first injection of buserelin depot and for two weeks after the first injection. Influence on the ability to drive a car and other mechanisms. Caution should be exercised when prescribing the drug to patients engaged in potentially hazardous activities that require increased attention and speed of mental and motor reactions.
STORAGE CONDITIONS Store in a place protected from light and out of reach of children, at a temperature of 8 to 20
Buserelin depot in the treatment of prostate cancer
G.P. Kolesnikov
GAUZ "Moscow City Oncology Hospital No. 62" of the Moscow Department of Health Russia, 143423, Moscow region, Krasnogorsky district, Stepanovskoye p/o, pos. Istra, 27
Contacts:
Gennady Petrovich Kolesnikov, e-mail: .
Print version
The high incidence of prostate cancer (PCa) and the very widespread use of hormonal therapy for its treatment as an independent method for common forms (T3-T4, N1, M1), relapses and progression of the disease after local treatment methods (radical prostatectomy, radiation therapy), as well as in combined treatment as neoadjuvant and adjuvant therapy, they determine the importance of a sufficient set of hormonal drugs in the urologist’s arsenal. Among the luteinizing hormone releasing hormone (LHRH) agonists, buserelin has been known for a long time, which is produced in Russia and whose clinical effectiveness is not inferior to imported analogues. The results of a study of the effectiveness and safety of treatment with buserelin depot in 20 patients with morphologically verified prostate cancer aged from 53 to 87 years are presented; the duration of the study was 3 months. During therapy with buserelin depot in patients with prostate cancer, a consistent decrease in the average values of prostate-specific antigen (PSA) was revealed from 81.2 to 27.8 ng/ml after 2 months and to 23.0 ng/ml after 3 months. During the therapy, a decrease in testosterone levels to post-castration values was achieved from the initial 168 to 21 ng/dl after 1 month and to 19.8 ng/dl after 3 months of treatment. All patients underwent treatment with buserelin depot without clinically significant adverse reactions. The most common complaints were increased sweating and hot flashes, characteristic of all drugs of the LHRH agonist group, no more pronounced than in treatment with other drugs of this group.
Conclusions.
Buserelin-depot at a dose of 3.75 mg is a highly effective domestic drug for the treatment of hormone-dependent prostate cancer. The use of buserelin depot leads to a decrease in PSA levels and ensures a stable decrease in serum testosterone levels to post-castration levels in the absence of serious side effects. The results obtained do not differ from similar indicators when using imported analogues of LHRH.
Keywords:
prostate cancer, hormonal therapy, luteinizing hormone-releasing hormone agonists, buserelin, prostate-specific antigen, testosterone, effectiveness and safety of therapy
DOI: 10.17 650/1726-9776-2015-11-3-&-&
GP Kolesnikov
Moscow City Cancer Hospital Sixty-Two, Moscow Healthcare Department; Stepanovskoe, 27, Istra Settlement, Krasnorgorsky District, Moscow Region 143423, Russia
The high incidence of prostate cancer (PC) and considerably the wide use of hormone therapy for its treatment as an individual modality for its advanced forms (T3-T4, N1, M1), recurrences, and progression after local treatments (radical prostatectomy, radiation therapy) and for combined treatment as neoadjuvant and adjuvant therapies determine the importance of a sufficient range of hormonal drugs at an urologic oncologist's disposal. Among the luteinizing hormone-releasing hormone (LHRH) agonists, there is rather long-known buserelin made in Russia, the clinical efficacy of which is highly competitive with foreign analogs.
The paper presents the results of a 3-month trial of the effectiveness and safety of buserelin depot treatment in 20 patients aged 53 to 87 years with morphologically verified PC. The patients with PC showed a gradual decrease in the mean values of prostate-specific antigen (PCA) from 81.2 to 27.8 and 23.0 ng/ml at 2 and 3 months of buserelin depot therapy, respectively. The performed therapy could achieve reductions in testosterone levels from 168 ng/dl at baseline to 21 and 19.8 ng/dl postcastration at 1 and 3 months of the therapy.
All the patients tolerated buserelin depot therapy without having clinically significant adverse reactions. The most common complaints were hyperhidrosis and hot flushes, which are typical of all LHRH agonists and which are not marked in the treatment with other drugs of this group.
Conclusion.
Buserelin depot 3.75 mg is a highly effective Russian drug to treat hormone-dependent PC. Its administration causes a reduction in PSA levels and ensures a steady decline in serum testosterone concentrations to the postcastration level without causing serious side effects. The findings do not differ from those when foreign LHRH analogues are used.
Key words:
prostate cancer, hormone therapy, luteinizing hormone-releasing hormone agonists, buserelin, prostate-specific antigen, testosterone, efficiency and safety of therapy
Introduction
Prostate cancer (PCa) is a common malignancy in men. In Europe, it is the most common solid cancer, with an incidence of 214 cases per 1000 men. Every year, more than 800 thousand new cases of prostate cancer are detected worldwide [1, 2].
The incidence of cancer of this localization in Russia has been rapidly increasing over the past 2 decades. In 2011, 28,552 new cases of prostate cancer were registered, in 2012 – more than 29,000. In the structure of cancer incidence, prostate cancer took 2nd place. In terms of growth rate, it is significantly ahead of malignant tumors of other localizations. The mortality rate also remains high [3, 4].
In Russia, there has been a trend towards an increase in the identification of patients with a localized form of prostate cancer. However, despite this, half of the patients are initially diagnosed with locally advanced and metastatic forms of prostate cancer [5]. Hormone therapy for prostate cancer, aimed at blocking testosterone synthesis, is widely used to treat primary advanced forms of prostate cancer, as well as relapses after local treatment methods (radical prostatectomy and radiation therapy) [4, 6, 7].
The main types of hormone therapy (androgen deprivation) today are surgical castration (bilateral orchiectomy) and medical castration - luteinizing hormone releasing hormone agonists (LHRH) and antagonists (firmagon) [4, 7]. Surgical castration has not been canceled or prohibited, but medical castration is more often used in practice due to the choice of the patient and the availability of drugs for its implementation, as well as the possibility of having a reversible effect upon cancellation. Currently, there are 4 main classes of substances that can be classified as LHRH agonists: goserelin, triptorelin, buserelin and leuprolide [7].
All drugs of the LHRH agonist group have approximately the same effectiveness in the treatment of prostate cancer, similar adverse events associated with low testosterone levels (hot flashes, sweating, decreased libido and potency, etc.) [4, 7]. But to date, only buserelin is produced in Russia, although it was synthesized as one of the first agonists [8]. Studies of Russian-made buserelin presented in the literature have shown its effectiveness and tolerability to be the same as that of imported analogues [4, 8-10].
The purpose of the study was to evaluate the effectiveness and safety of treatment of patients with prostate cancer with the drug buserelin-depot (ZAO Pharm-Sintez, Russia).
Materials and methods
From February to May 2014, at the clinic of the Moscow City Oncology Hospital No. 62, 20 patients with morphologically diagnosed prostate cancer were treated with buserelin depot. The age of the patients ranged from 53 to 87 years, the average age was 69.8 years.
Buserelin depot at a dose of 3.75 mg was used for 3 cycles with intramuscular administration once every 28 days.
In all patients, the diagnosis of prostate adenocarcinoma with varying degrees of differentiation according to the Gleason score (Gleason index) was previously morphologically confirmed. During histological verification of the diagnosis, moderate and poorly differentiated forms of PCa predominated (Gleason index 6–10).
All patients at the start of treatment had a prostate-specific antigen (PSA) level above normal. Before treatment with buserelin depot, the average PSA value was 81.2 (4.2–679) ng/ml. Half of the patients (n = 10) had distant metastases, represented mainly by bone deposits confirmed by bone scintigraphy, X-ray or magnetic resonance imaging (MRI). The number of bone metastases ranged from 2 to total damage to the bone skeleton. The distribution of patients by disease stage was as follows: T2N1M0 – 1, T3N0M0 – 9, T3N0M1 – 7, T3N1M1 – 2, T4N1M1 – 1 patient.
Based on the extent of the tumor, hormone therapy was prescribed to all. In some patients with bone metastases, in addition to hormonal treatment, other types of specialized treatment were used: palliative external beam radiation therapy for bone metastases, treatment with zoledronic acid, etc.
11 patients had pain, 9 did not require pain relief.
The effectiveness of drug treatment was assessed once a month. The examination included determination of PSA levels, serum testosterone, assessment of general condition according to the Karnofsky scale and pain syndrome according to the World Health Organization scale (clinical response).
Results and discussion
When analyzing the results obtained, it was found that the majority of patients receiving buserelin depot had positive PSA dynamics, characterized by a sharp decrease in the first 2 months of treatment, after which a gradual regression and stabilization of indicators occurred.
During therapy with buserelin depot in patients with prostate cancer, a consistent decrease in mean PSA values was revealed from 81.2 to 27.8 ng/ml after 2 months, to 23.0 ng/ml after 3 months.
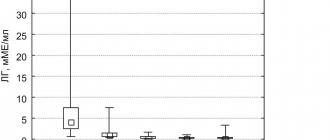
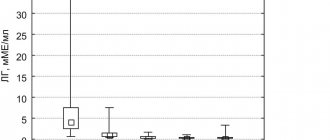
During the therapy, a decrease in testosterone levels to post-castration values was achieved from the initial average of 168 to 21 ng/dl after 1 month and 19.8 (3–29) ng/dl after 3 months of treatment.
A decrease in the level of pain was clinically noted in 4 (36.3%) patients out of 11 who had pain, which allowed 2 of them to stop using narcotic analgesics.
Since the group of elderly patients under observation (average age about 70 years), in half of the cases with metastatic prostate cancer, the severity of their condition, in addition to the underlying cancer, was due to concomitant age-related pathology. The choice of a drug for long-term therapy dictates the need not only for its effectiveness, but also for a minimum number of side effects and good tolerability.
All patients underwent treatment with buserelin depot without clinically significant adverse reactions. The most common complaints were increased sweating and hot flashes, characteristic of all drugs of the LHRH agonist group, no more pronounced than with treatment with other drugs of this group. No allergic reactions were registered. There were no cases of urinary retention, muscle weakness in the lower extremities, edema or lymphostasis. No local reaction to the administration of the drug was observed. Not a single patient refused treatment due to poor tolerance.
It should be noted that the majority of patients, after completing the 3-month study, the results of which are presented here, remain on hormone therapy with buserelin depot in a constant or intermittent mode, with good tolerability and response observed according to clinical data and PSA levels with varying durations.
conclusions
- Buserelin-depot is a highly effective domestic drug for the treatment of hormone-dependent prostate cancer.
- The use of buserelin depot leads to a decrease in PSA levels and ensures a stable decrease in serum testosterone levels to post-castration levels in the absence of serious side effects. The results obtained do not differ from similar indicators when using imported analogues of LHRH.
- Buserelin depot can be recommended for use as independent therapy or in combination with other treatment methods in patients with prostate cancer.
Literature
- Anderson J., Abrahamsson PA., Crawford D. et al. Management of advanced prostate cancer: can we improve on androgen deprivation therapy. BJU Int 2008;101:1497-501.
- Heidenreich A., Pfister D., Ohlamann CH et al. Androgen deprivation for advanced prostate cancer. Urologe 2008;47:270-83.
- Malignant neoplasms in Russia in 2012 (morbidity and mortality). Ed. HELL. Kaprina, V.V. Starinsky, G.A. Petrova. M.: FSBI “MNIOI im. P.A. Herzen" Ministry of Health of Russia, 2014. .
- Mishugin S.V., Mordovin A.A., Gritskevich A.A., Rusakov I.G. Medical castration in the treatment of common forms of prostate cancer. The role of buserelin. Medical Council 2014;8:3-6.
- Kaprin A.D., Starinsky V.V., Petrova G.V. The state of cancer care for the population of Russia in 2012. M., 2013.
- Babaev R., Matveev V.B., Volkova M.I. Predictive factors for survival in patients with advanced prostate cancer receiving hormone therapy. Oncourology 2011;2:78-83.
- Nyushko K.M., Alekseev B.Ya., Kalpinsky A.S., Kaprin A.D. Antagonists of luteinizing hormone-releasing hormone in patients with prostate cancer. Standard approach and results of innovative research. Oncourology 2014;4:70-4. [Nyushko KM, Alexeev BY, Kalpinsky AS, Kaprin AD Luteinizing hormone-releasing hormone antagonists in patients with prostate cancer. Standard approach and results of innovational studies. Onkourologiya = Oncourology 2014;4:70-4. (In Russ.)].
- Rapoport L.M., Demidko Yu.L. Use of buserelin depot, a gonadotropin-releasing hormone agonist, in the treatment of prostate cancer. Andrology and Genital Surgery 2014;3:2-7.
- Sivkov A.V., Matveev V.B., Bukharkin B.V. and others. Results of long-term use of the gonadotropin-releasing hormone agonist buserelin-depot in patients with prostate cancer. Consilium Medicum 2005;7(7):591-5.
- Kopyltsov E.I., Leonov O.V., Krivonogov I.I. and others. Domestic deposited drug in the treatment of patients with prostate cancer. Oncourology 2005. Abstracts of the 6th All-Russian. scientific-practical conference “Current issues in the treatment of urological cancer diseases”. pp. 94-5.
Contacts
: Kolesnikov Gennady Petrovich, MD, professor, head of the department of oncourology of the polyclinic of the Moscow City Oncology Hospital No. 62. Tel., email: .
Buserelin-depot lyof d/susp for IM injection, long-acting 3.75 mg N1
Registration Certificate Holder
PHARM-SYNTHESIS (Russia)
Dosage form
Medicine - Buserelin-depo (Buserelin-depo)
Description
Lyophilisate for the preparation of a suspension for intramuscular administration
of prolonged action
in the form of a white or white powder with a slight yellowish tint; the attached solvent is a colorless transparent liquid; the reconstituted suspension is homogeneous, white or white with a slight yellowish tint.
1 fl.
buserelin acetate 3.93 mg, which corresponds to the content of buserelin 3.75 mg
Excipients
: copolymer of DL-lactic and glycolic acids - 200 mg, mannitol - 85 mg, carmellose sodium - 30 mg, polysorbate 80 - 2 mg.
Solvent:
solution of mannitol 0.8% d/i - 2 ml.
dark glass bottles (1) complete with solvent (amp), syringe, needles (2 pcs.) and alcohol swabs (2 pcs.) - contour cell packaging (1) - cardboard packs.
Indications
- hormone-dependent prostate cancer;
- mammary cancer;
- endometriosis (pre- and postoperative periods);
- uterine fibroids;
- hyperplastic processes of the endometrium;
- infertility treatment (during an in vitro fertilization program).
Contraindications for use
- pregnancy;
- lactation period;
- hypersensitivity to the components of the drug.
pharmachologic effect
Antitumor drug, synthetic analogue of GnRH. Buserelin competitively binds to the receptors of the cells of the anterior pituitary gland, causing a short-term increase in the level of sex hormones in the blood plasma. On average, after 12-14 days, use of the drug in therapeutic doses leads to a complete blockade of the gonadotropic function of the pituitary gland, thus inhibiting the release of LH and FSH. As a result, there is a suppression of the synthesis of sex hormones in the gonads, which is manifested by a decrease in the concentration of estradiol in the blood plasma to post-menopausal values in women and a decrease in testosterone content to a post-castration level in men.
The concentration of testosterone with continuous treatment for 2-3 weeks decreases to the level characteristic of the orchiectomy state, i.e. the drug causes pharmacological castration.
Drug interactions
The simultaneous use of Buserelin-depot with drugs containing sex hormones (for example, in the mode of ovulation induction) may contribute to the occurrence of ovarian hyperstimulation syndrome.
With simultaneous use, buserelin may reduce the effectiveness of hypoglycemic agents.
Dosage regimen
For hormone-dependent prostate cancer -
3.75 mg IM every 4 weeks.
In the treatment of endometriosis, endometrial hyperplastic processes
- 3.75 mg IM once every 4 weeks. Treatment should begin in the first five days of the menstrual cycle. Duration of treatment is 4-6 months.
In the treatment of uterine fibroids
- 3.75 mg IM once every 4 weeks. Treatment should begin in the first five days of the menstrual cycle. The duration of treatment is 3 months before surgery, in other cases - 6 months.
When treating infertility using in vitro fertilization -
3.75 mg IM once at the beginning of the follicular phase (on the 2nd day of the menstrual cycle) or in the middle of the luteal phase (21-24 days) of the menstrual cycle preceding stimulation. After blockade of pituitary function, confirmed by a decrease in the concentration of estrogen in the blood serum by at least 50% of the initial level (usually determined 12-15 days after injection of Buserelin-depot), in the absence of cysts in the ovaries (according to ultrasound), endometrial thickness no more than 5 mm, stimulation of superovulation begins with gonadotropic hormones under ultrasound monitoring and control of the level of estradiol in the blood serum.
Rules for preparing the suspension and administering the drug
The drug is administered only intramuscularly. A suspension for intramuscular injection is prepared using the supplied solvent immediately before administration. The drug should be prepared and administered only by specially trained medical personnel.
The bottle with Buserelin-depot should be kept strictly vertical. By lightly tapping the bottle, you need to ensure that all the lyophilisate is at the bottom of the bottle.
Open the syringe, attach a needle with a pink pavilion (1.2 × 50 mm) to it to withdraw the solvent.
Open the ampoule and draw the entire contents of the ampoule with solvent into the syringe, set the syringe to a dose of 2 ml.
Remove the plastic cap from the bottle containing the lyophilisate. Disinfect the rubber stopper of the bottle with an alcohol swab. Insert the needle into the bottle with the lyophilisate through the center of the rubber stopper and carefully introduce the solvent along the inner wall of the bottle, without touching the contents of the bottle with the needle. Remove the syringe from the bottle.
The bottle should remain motionless until the lyophilisate solvent is completely saturated with the solvent and a suspension is formed (approximately 3-5 minutes). After which, without turning the bottle over, you should check the presence of dry lyophilisate at the walls and bottom of the bottle. If dry residues of the lyophilisate are detected, leave the bottle until completely saturated.
Once there is no remaining dry lyophilisate left, the contents of the bottle should be carefully mixed in a circular motion for 30-60 seconds until a homogeneous suspension is formed. Do not invert or shake the bottle, as this may cause flakes to fall out and the suspension to become unusable.
You need to quickly insert the needle through the rubber stopper into the bottle. Then lower the cut of the needle down and, tilting the bottle at an angle of 45°, slowly draw the entire suspension into the syringe. Do not invert the bottle when taking it. A small amount of the drug may remain on the walls and bottom of the bottle. Consumption for the residue on the walls and bottom of the bottle is taken into account.
Immediately replace the needle with a pink pavilion with a needle with a green pavilion (0.8x40 mm), carefully turn the syringe over and remove air from the syringe.
Buserelin-depot suspension should be administered immediately after preparation.
Using an alcohol swab, you need to disinfect the injection site. Insert the needle deep into the gluteal muscle, then pull the syringe plunger back slightly to ensure that there is no damage to the vessel. Inject the suspension intramuscularly slowly with constant pressure on the syringe plunger. If the needle becomes clogged, it is replaced with another needle of the same diameter.
Overdose
Currently, no cases of overdose with Buserelin-depot have been reported.
Side effect
Allergic reactions:
urticaria, skin hyperemia; rarely - angioedema.
From the side of the central nervous system:
frequent mood swings, sleep disturbances, depression, headache.
From the musculoskeletal system:
demineralization of bones, which is a risk of developing osteoporosis.
Among women
- headache, depression, sweating and changes in libido, dryness of the vaginal mucosa, pain in the lower abdomen;
rarely - menstrual-like bleeding (usually during the first weeks of treatment). In men
during the treatment of prostate cancer, during the first 2-3 weeks after the first injection, exacerbation and progression of the underlying disease (which is associated with stimulation of the synthesis of gonadotropins and, accordingly, testosterone), gynecomastia, possible “hot flashes”, increased sweating and decreased potency ( rarely requires a change in therapy), a transient increase in the concentration of androgens in the blood, urinary retention, “renal” edema (swelling of the face, eyelids, legs), muscle weakness in the lower extremities. When patients with prostate cancer begin treatment, they may experience a temporary increase in bone pain; in this case, symptomatic therapy should be carried out. Isolated cases of ureteral obstruction and spinal cord compression have been noted.
Other:
in isolated cases (the cause-and-effect relationship has not been clearly established) - pulmonary embolism, dyspeptic symptoms.
special instructions
Women.
Patients with any form of depression during treatment with Buserelin-depot should be under close medical supervision. Ovulation induction should be performed under strict medical supervision. In the initial stage of treatment with the drug, the development of ovarian cysts is possible.
Before starting treatment with the drug, it is recommended to exclude pregnancy and stop taking hormonal contraceptives, however, during the first two months of using the drug, it is necessary to use other (non-hormonal) methods of contraception.
Men.
In order to effectively prevent possible side effects in the first phase of the drug's action, it is necessary to use antiandrogens 2 weeks before the first injection of Buserelin-depot and for 2 weeks after the first injection.
Effect on the ability to drive vehicles and operate machinery
Care should be taken when prescribing the drug to patients engaged in potentially hazardous activities that require increased attention and speed of psychomotor reactions.
Storage conditions
The drug should be stored out of the reach of children, protected from light at a temperature of 8° to 25°C.
Best before date
The shelf life of the lyophilisate is 3 years, the solvent is 5 years.
Use during pregnancy and breastfeeding
Restrictions during pregnancy - Contraindicated. Restrictions when breastfeeding - Contraindicated. Use during pregnancy and lactation is contraindicated.
Terms of sale
The drug is available with a prescription.
Contacts for inquiries
PHARM-SYNTHEZ CJSC (Russia)
115419 Moscow, 2nd Roshchinsky pr-d 8 Tel.; Fax
Side effects of Buserelin
It is worth noting that “Buserelin” for fibroids and other diseases has a number of side effects:
- From the gastrointestinal tract: thirst, nausea and vomiting, weight gain or loss;
- From the central nervous system: headaches and dizziness, insomnia, constant feeling of weakness and fatigue, depression, anxiety;
- From the cardiovascular system: strong heartbeats, increased blood pressure;
- From the senses: visual impairment, hearing impairment, tinnitus;
- From the endocrine system: hot flashes, severe sweating, decreased libido, pain in the lower abdomen;
- Allergic reactions of varying intensity.
BUSERELIN-LONG FS
Directions for use and doses
For breast cancer and hormone-dependent prostate cancer,
Buserelin-long FS is administered at a dose of 3.75 mg (1 injection) intramuscularly (IM) every 4 weeks for a long time under the supervision of a physician.
In the treatment of endometriosis, endometrial hyperplastic processes
the drug is administered at a dose of 3.75 mg intramuscularly once every 4 weeks. Treatment should begin in the first five days of the menstrual cycle. Duration of treatment is 4-6 months.
In the treatment of uterine fibroids
Buserelin-long FS is administered at a dose of 3.75 mg IM once every 4 weeks. Treatment should begin in the first five days of the menstrual cycle. The duration of treatment is 3 months before surgery, in other cases - 6 months.
In the treatment of infertility using in vitro fertilization (IVF)
Buserelin-long FS is administered in a dose of 3.75 mg (1 injection) intramuscularly once at the beginning of the follicular phase (on the 2nd day of the menstrual cycle) or in the middle of the luteal phase (21-24 days) of the menstrual cycle preceding stimulation. After blockade of pituitary function, confirmed by a decrease in the concentration of estrogen in the blood serum by at least 50% of the initial value (usually determined 12 - 15 days after injection of Buserelin-long FS), in the absence of ovarian cysts (according to ultrasound), endometrial thickness no more than 5 mm, stimulation of superovulation begins with gonadotropic hormones under ultrasound monitoring and control of the concentration of estradiol in the blood serum.
Rules for preparing the suspension and administering the drug
— The drug is administered only intramuscularly
— A suspension for intramuscular injection is prepared immediately before administration using the supplied solvent.
— The drug should be prepared and administered only by specially trained medical personnel.
— Keep the bottle with Buserelin-long FS strictly vertically. By lightly tapping the bottle, ensure that all the lyophilisate is at the bottom of the bottle.
— Open the syringe, attach a needle measuring 1.2 mm x 50 mm to it to withdraw the solvent.
— Open the ampoule with the solvent and draw the entire contents of the ampoule into the syringe, set the syringe to a dose of 2 ml.
— Remove the plastic cap from the bottle containing the lyophilisate. Disinfect the rubber stopper of the bottle with an alcohol swab. Insert the needle into the lyophilisate vial through the center of the rubber stopper and carefully inject the solvent along the inner wall of the vial, without touching the contents of the vial with the needle. Remove the syringe from the vial.
— The bottle must remain motionless until the lyophilisate solvent is completely saturated with the solvent and a suspension is formed (approximately 3–5 minutes). Then, without turning the bottle over, check the presence of dry lyophilisate at the walls and bottom of the bottle. If you find dry residues of the lyophilisate, leave the bottle until completely saturated.
— After you have ensured that there are no residues of dry lyophilisate, carefully mix the contents of the bottle in a circular motion for 30-60 seconds until a homogeneous suspension is formed. Do not invert or shake the bottle.
— Quickly insert the needle through the rubber stopper into the bottle. Then lower the cut of the needle down and, tilting the bottle at an angle of 45 degrees, slowly draw the entire suspension into the syringe. Do not invert the bottle when drawing.
A small amount of the drug may remain on the walls and bottom of the bottle. Consumption for the residue on the walls and bottom of the bottle is taken into account.
Immediately after drawing up the solution, remove the needle. Replace with a 0.8mm x 40mm needle, carefully invert the syringe and remove any air from the syringe.
— Administer Buserelin-long FS suspension immediately after preparation.
— Use an alcohol swab to disinfect the injection site.
Insert the needle deep into the gluteal muscle, then pull the syringe plunger back slightly to make sure there is no damage to the vessel.
Inject the suspension slowly with constant pressure on the syringe plunger.
If the needle becomes clogged, replace it with another needle of the same diameter.
— For repeated injections, the left and right sides should be alternated.
The effect of "Buserelin" on the female body
The effect of “Buserelin” for uterine fibroids depends on the type of myomatous nodes and the individual characteristics of the patient’s body. It is worth noting that reviews of taking this drug are not always positive, since it causes a number of side effects. At the same time, it is worth noting that when using Buserelin in the form of a nasal spray. Negative manifestations were practically not noticed. Numerous studies show that after therapy with Buserelin, many women develop early menopause. The drug has found wide use in the postoperative period to eliminate the risk of fibroid recurrence.
Contraindications:
- Allergic reaction to buserelin acetate or additional substances;
- Pregnancy and lactation;
- Kidney failure;
- Depression;
- Diabetes mellitus along with two or more complications.
Mode of application
Side effects can be minimized and positive results can be achieved from taking Buserelin by strictly following the dosage and dosage regimen recommended by your doctor. They directly depend on the form of release of the drug. Thus, a nasal spray is usually used three times a day at equal intervals at a rate of 0.9 mg per day. During treatment, oral contraceptives cannot be used, so it is recommended to replace them with other methods of contraception. Intramuscular injections of Buserelin are given every 28 days, starting 5 days before the start of the cycle. If the product is used as preoperative preparation, then injections are given within three months. As for conservative therapy, its course lasts six months.
What is "Buserelin"?
“Buserelin” for the treatment of fibroids is a hormonal drug (antiandrogen, antigonadotropin, antiestrogen), which is produced in various forms:
- nasal spray;
- implants;
- lyophilisate for the preparation of suspension for injection;
- injection;
- drops.
Its active ingredient is buserelin acetate - a substance from the groups of hormones of the hypothalamus and pituitary gland, antagonists and gonadotropins, as well as antitumor hormonal agents. The substance is able to bind to the receptors of pituitary cells and stimulate a short-term increase in the level of sex hormones in the blood plasma. Use of the drug for two weeks leads to a blockade of the gonadotropic function of the pituitary gland (the process resumes after stopping the drug) and, as a result, a decrease in the level of estradiol in the blood. As a result, this makes it possible to stop the development of myomatous nodes.